11a Peritoneal dialysis.ppt
39
Peritoneal dialysis Jana Fialová Martina Peiskerová Klinika nefrologie 1. LF a VFN Praha 10/2007
Transcript of 11a Peritoneal dialysis.ppt
Peritoneal dialysis
Jana FialováMartina Peiskerová
Klinika nefrologie 1. LF a VFN Praha
10/2007

Ramesh Khanna & Karl D. Nolph
Modalities of renal replacement therapy
Interchangeable, depends on residual renal function
Peritoneal dialysis - outline
• Principles of PD• PD solutions• PD catheter• Indication / contraindication of PD• PD schemes : CAPD, CCPD• Assessement of PD adequacy,
ultrafiltration• Assessement of peritoneal function• Complications • Perspectives – new dialysis solutions
Peritoneal dialysis – introduction
• method of RRT for 100.000 patients worldwide• complementary to hemodialysisPrinciples: • peritoneum (capillary endothelium, matrix,
mesothelium) = semipermeable dialysis membrane through which fluid and solute move from blood to dialysis solution via diffusion and convection
• effective peritoneal surface area = perfused capillaries closed to peritoneum (↓ in peritonitis)
• ultrafiltration (movement of water) enabled by osmotic gradient generated by glucose or glucose polymers (isodextrin)

Principles of peritoneal dialysis
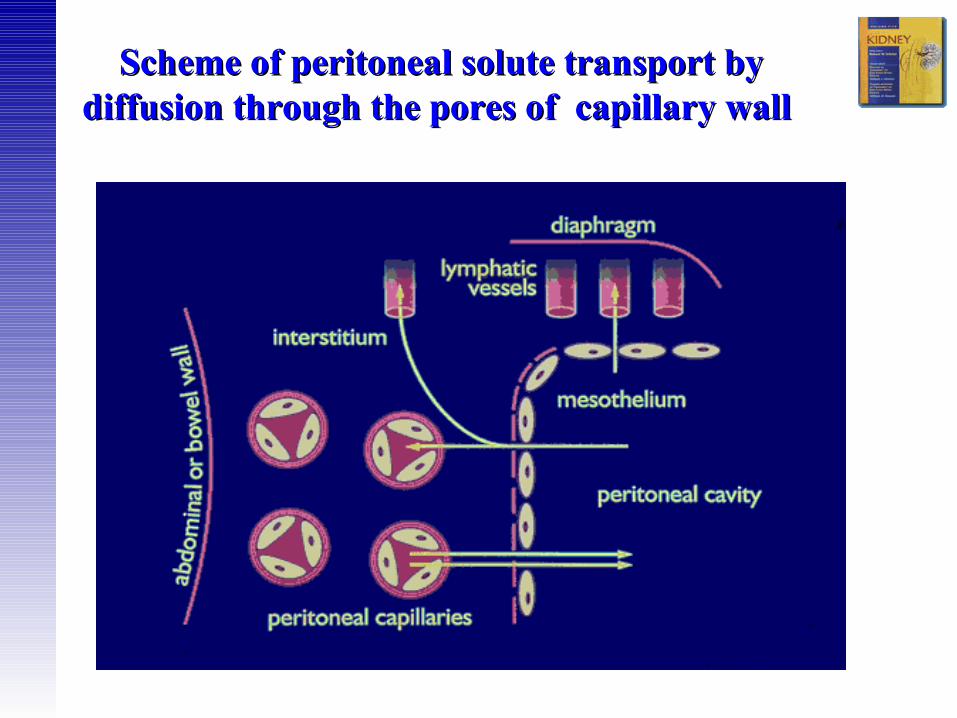
Scheme of peritoneal solute transport by Scheme of peritoneal solute transport by diffusion through the pores of capillary wall diffusion through the pores of capillary wall
Ramesh Khanna & Karl D. Nolph
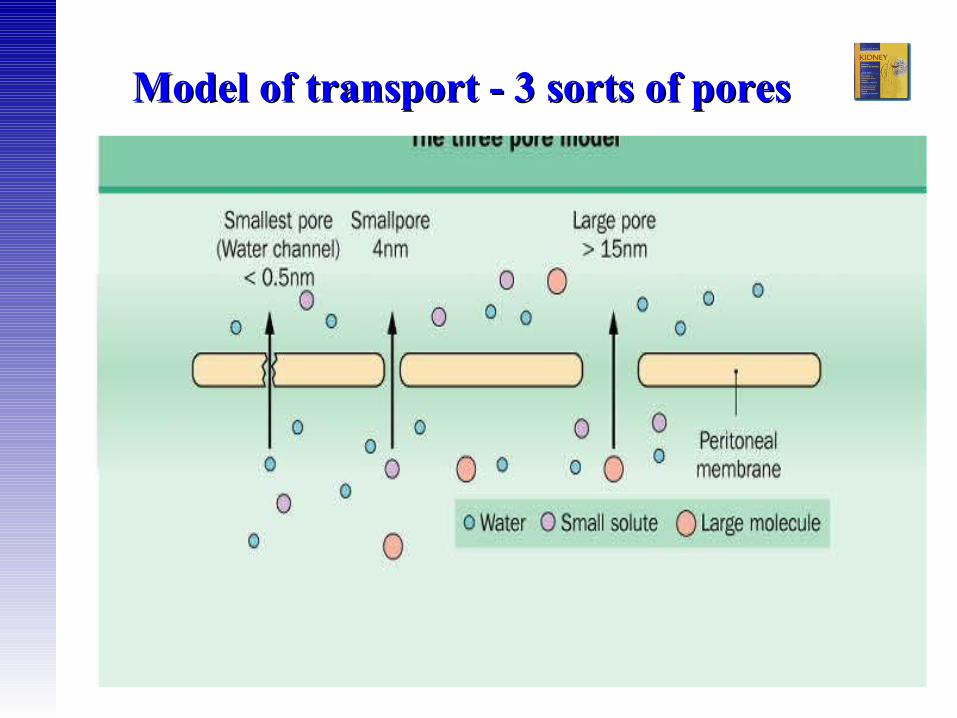
Model of transport - 3 sorts of pores Model of transport - 3 sorts of pores

Ramesh Khanna & Karl D. Nolph
Na 132 mmol/l
Ca 1,25mmol/l
Mg 0,5 mmol/l
Cl 100 mmol/l
lactate 35 mmol/l ev. lactate/bicarbonate
glukose 1,36-4,25 g/dl
osmolarity 347-486
pH 5,2
GDP (degradation products of glucose)
Composition of standard peritoneal Composition of standard peritoneal dialysis solutiondialysis solution
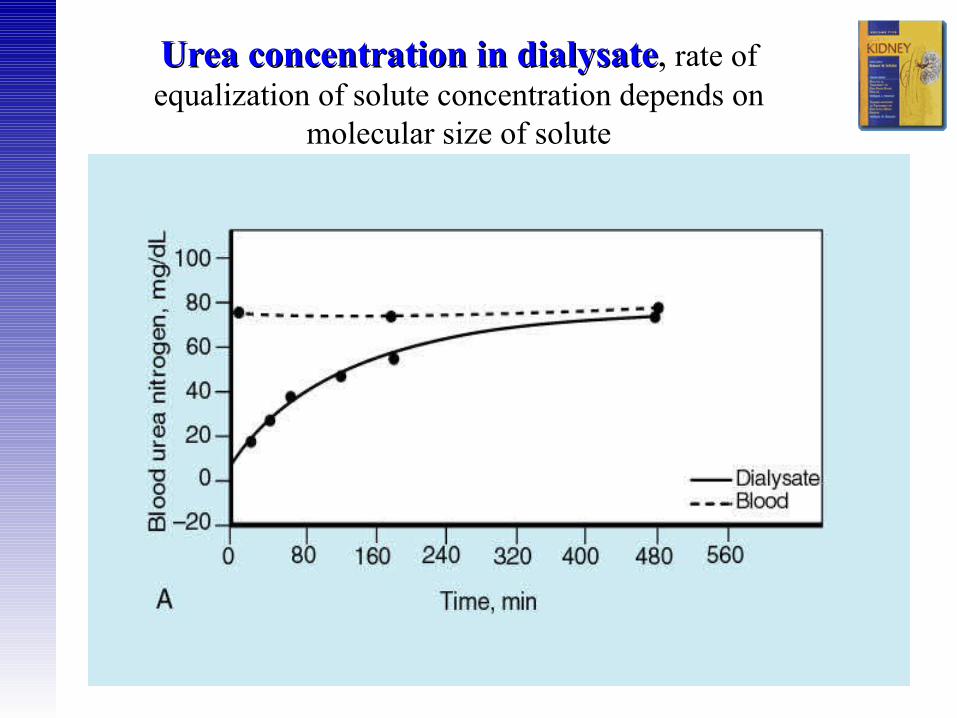
Urea concentration in dialysateUrea concentration in dialysate, rate of equalization of solute concentration depends on
molecular size of solute

Concentration of Creatinin in dialysate Concentration of Creatinin in dialysate equilibrium of concentrations between
dialysate and blood is slower than for urea
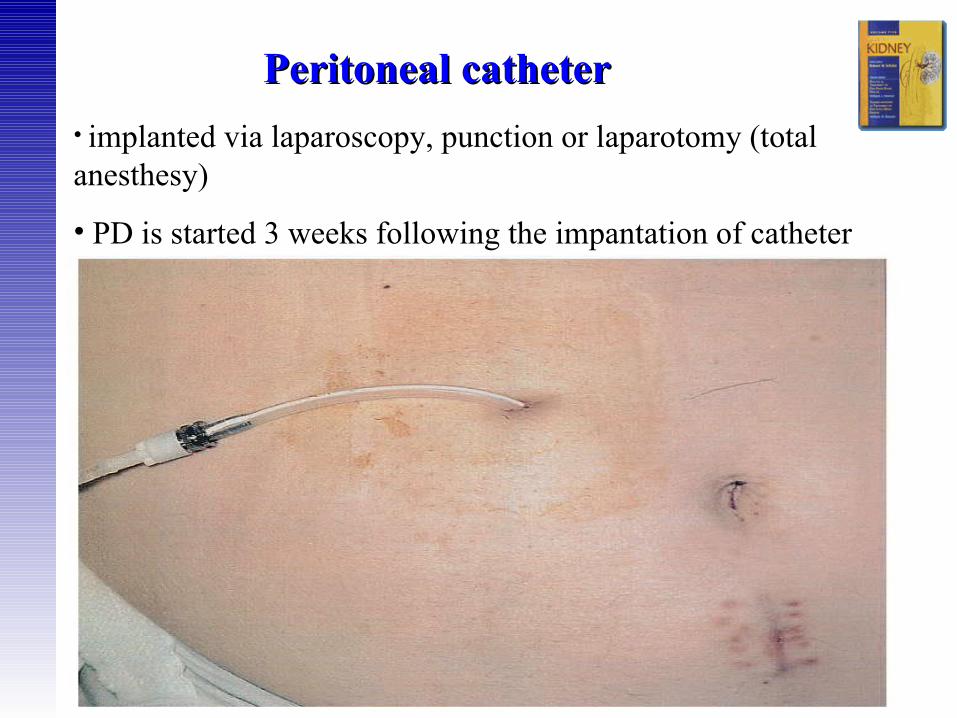
Peritoneal catheterPeritoneal catheter
• implanted via laparoscopy, punction or laparotomy (total anesthesy)
• PD is started 3 weeks following the impantation of catheter
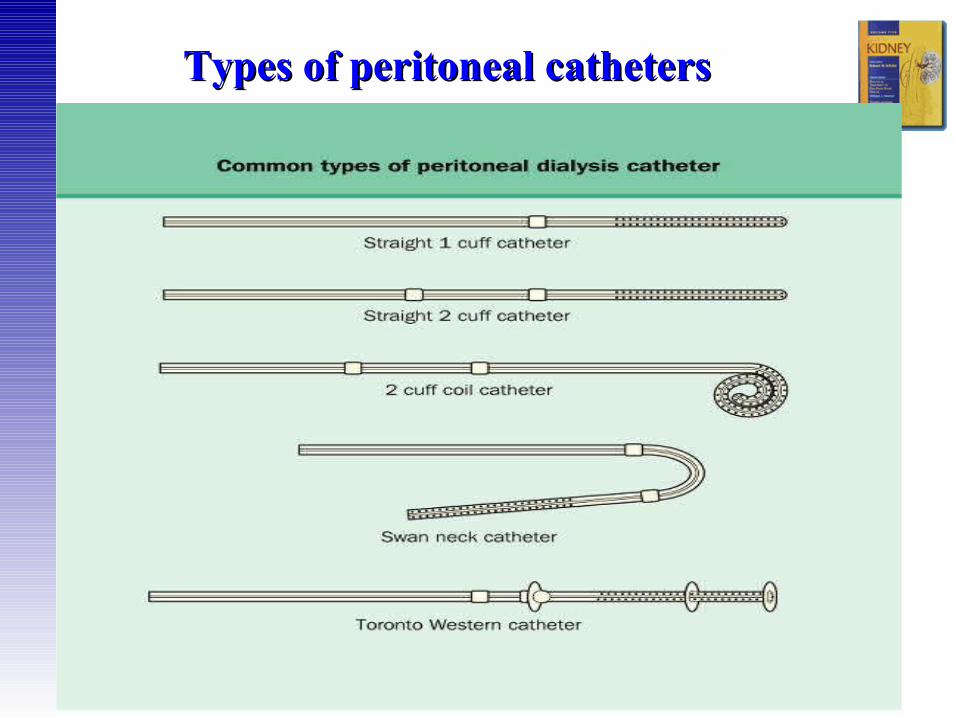
Types of peritoneal cathetersTypes of peritoneal catheters

Why to start with PD ?Why to start with PD ?
1. better maintenance of residual renal function
Why to start with PD ?Why to start with PD ?
• clinical outcomes comparable to HD, no difference in 2 year and 5 year mortality vs. HD (study NECOSAD)
• saves vascular access
• preferred for children (APD)
• modality choice is a lifestyle issue
Ramesh Khanna & Karl D. Nolph
80% of patients have no contra-indication to any of the dialysis methods and may choose according to their life style between HD a PD
Absolute contra-indications of PD:
1.peritoneal fibrosis and adhesions following intraabdominal operations
2.inflammatory gut diseases
Indication / Contraindications of PDIndication / Contraindications of PD
• pleuro-peritoneal leakage
• hernias• significant loin pain• big polycystic kidneys
Relative contraindications of PDRelative contraindications of PD
• severe deformant arthritis • psychosis• significant decrease of lung
functions
* diverticulosis
• colostomy • obesity
• blindness
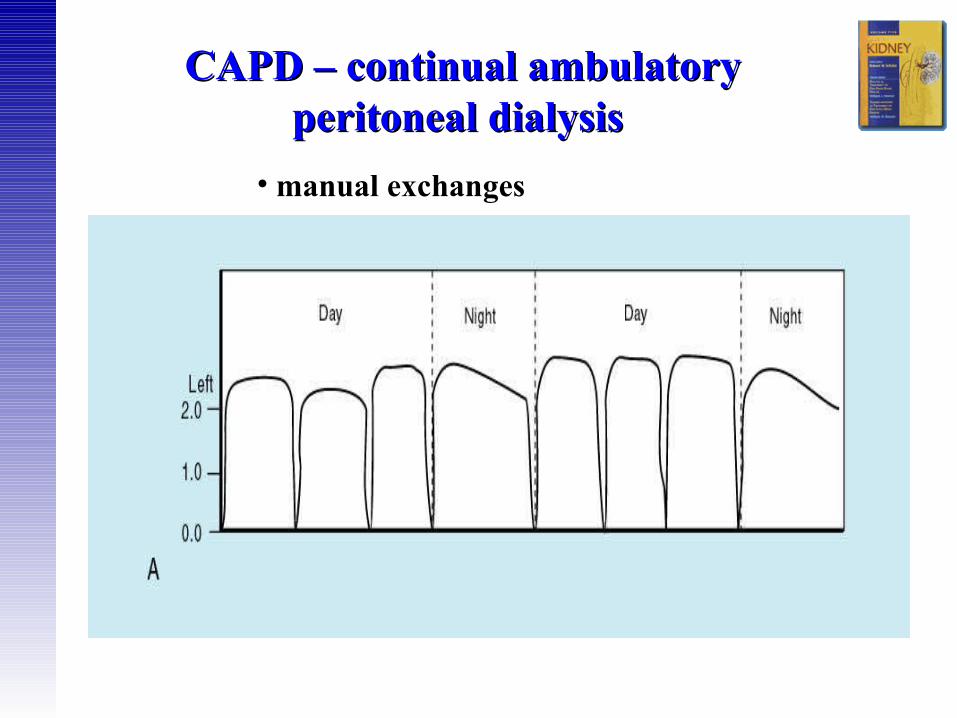
CAPD – continual ambulatory CAPD – continual ambulatory peritoneal dialysis peritoneal dialysis
• manual exchanges
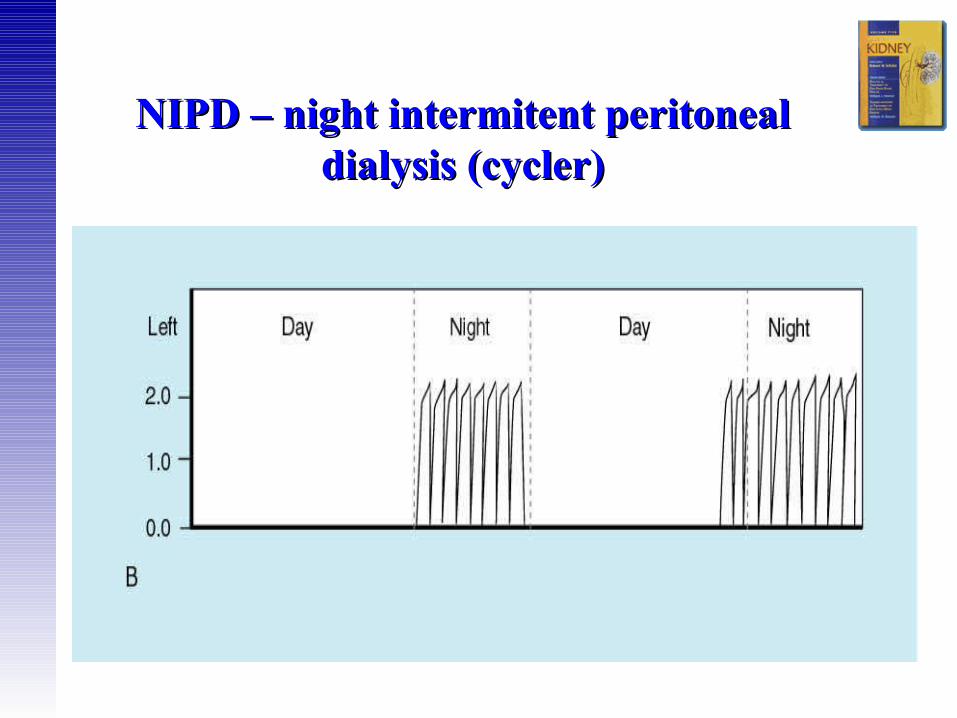
NIPD – night intermitent peritoneal NIPD – night intermitent peritoneal dialysis (cycler)dialysis (cycler)
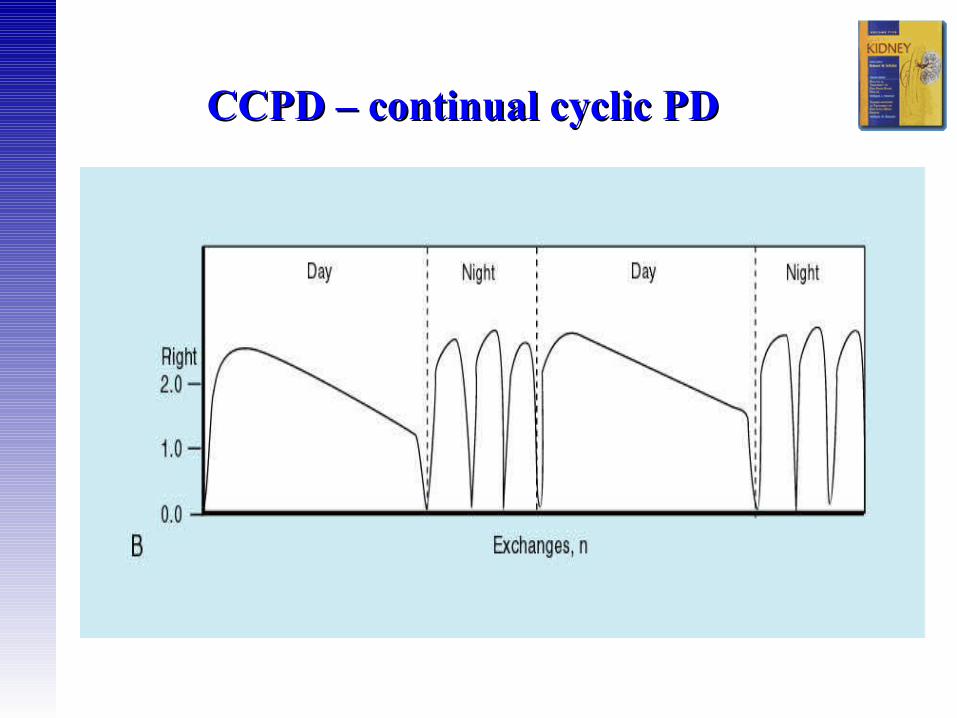
CCPD – continual cyclic PDCCPD – continual cyclic PD
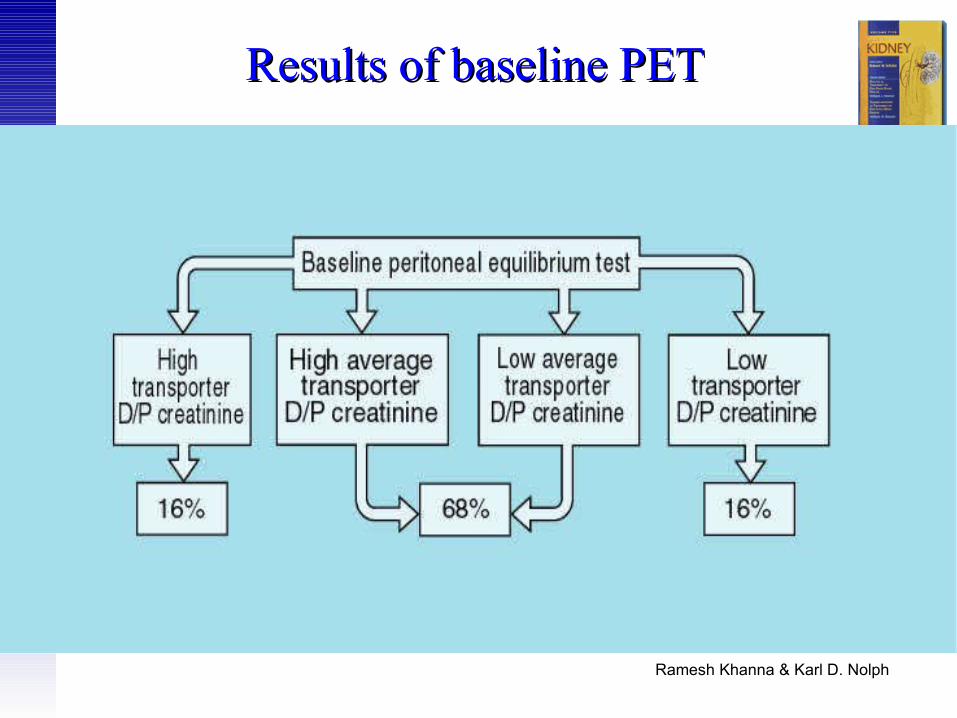
Assessement of PD adequacyPET (peritoneal equilibrium test) 1
• determines quick or slow passage of toxins from the blood into the dialysis fluid
• ‘high-fast transporters’ v.s. ‘low-slow transporters’
• helps to decide about the PD scheme (dwell duration and intervals, CAPD vs. CCPD)
• performed in hospital, takes 5 hours• involves doing a CAPD exchange using a 2.27%
G, samples of PD fluid and blood are taken at set times

PET (peritoneal equilibration test) 2
CAPD, 5 exchanges daily + 1 exchange at night
GoodSlowSlow
CAPD or APD
OKOKAverage
Frequent exchanges, short dwells – APD
Poor FastHigh
Best type of PD
Water removal
Waste removal
Transporter

Interpretation of peritonal Interpretation of peritonal equilibration test ??equilibration test ??
Ramesh Khanna & Karl D. Nolph
Results of baseline PETResults of baseline PET
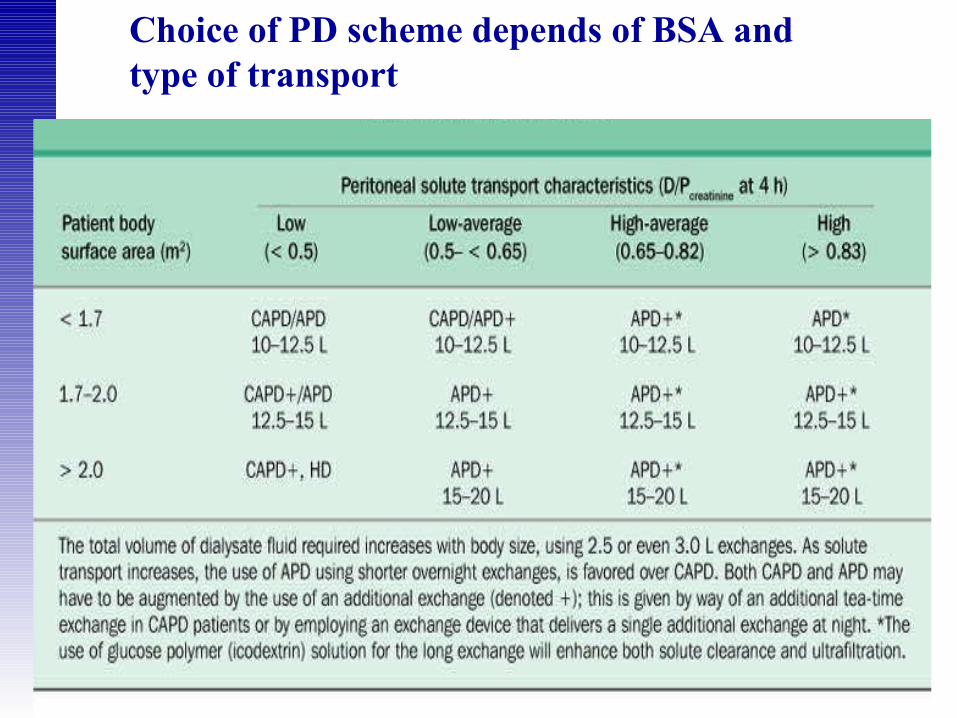
Choice of PD scheme depends of BSA and type of transport

2. PET- peritoneal equilibration test (type of transport and ultrafiltration after 4 hours)
3. weekly clearance of creatinine and urea
4. daily UF
5. dicrease of Na in dialysis fluid after 60 minutes using 3,8% G (test of aquaporines)
Assessement of peritoneal Assessement of peritoneal functionfunction
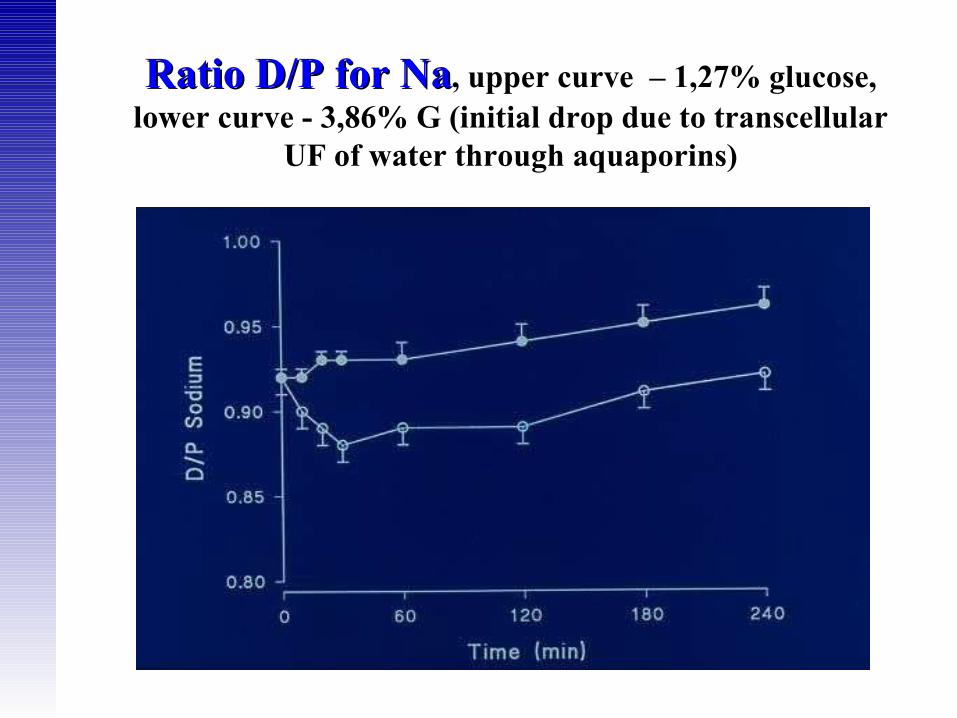
Ratio D/P for NaRatio D/P for Na, upper curve – 1,27% glucose, lower curve - 3,86% G (initial drop due to transcellular
UF of water through aquaporins)
Depends on:
- type of transporter – low transporters have better UF
- concentration and type of osmotic agent in PD fluid:
4. Fluids with glucosis (1,27%, 2,5% a 3,8% ), higher concentration – higher osmotic pressure and UF
5. Fluid with icodextrin (Extraneal) = glucose polymer with a large molecule, resorbs only 10-20%, offers longtime UF, suitable for long night exchanges, 8-12 hours)
- time between exchanges, using glucose-based fluids, maximal UF obtained after 2-3 hours, using longer spaces UF dicreases.
Ultrafiltration during PD Ultrafiltration during PD
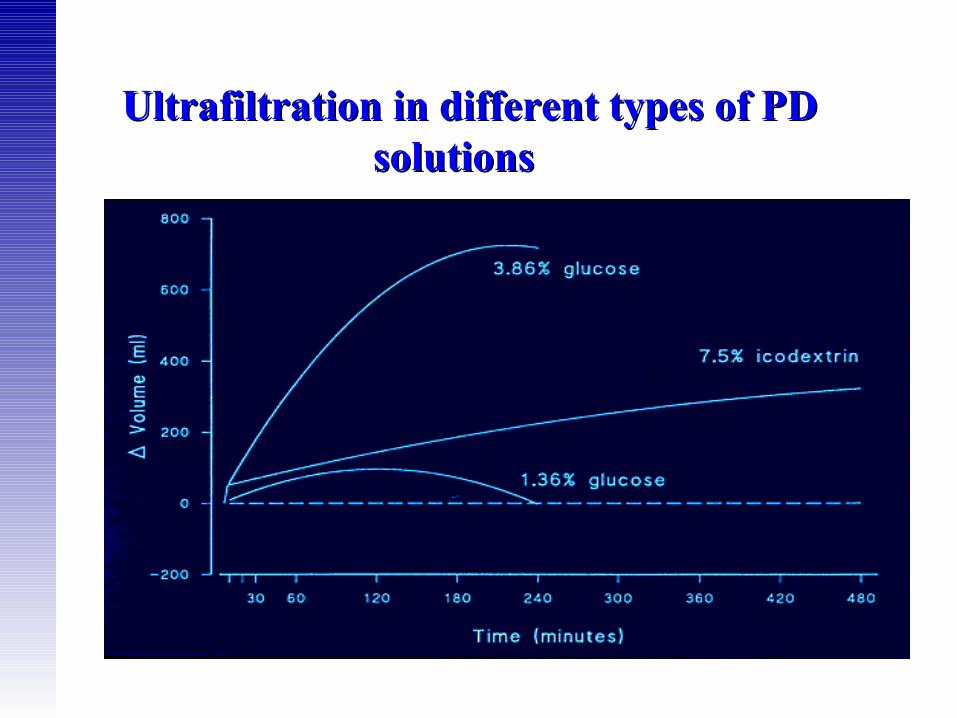
Ultrafiltration in different types of PD Ultrafiltration in different types of PD solutions solutions
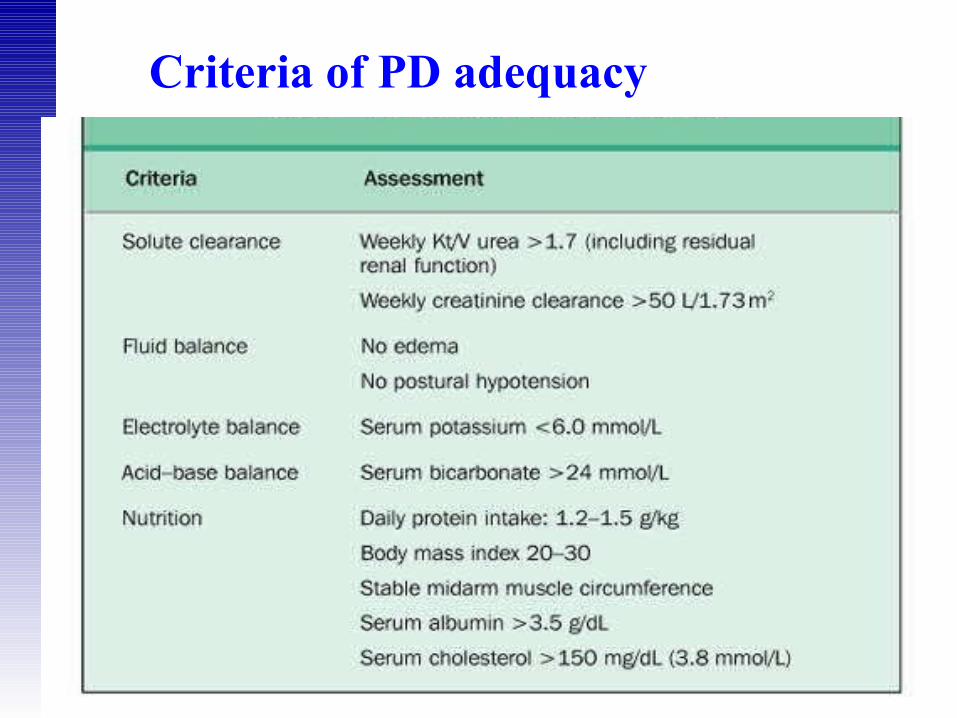
Criteria of PD adequacy

Infectious:
• exit-site inflammation (flare, suppurative secretion,
granulation)
• peritonitis (turbid dialysate, abdominal pain, fever)
Non-infectious:
• hernias
• hydrothorax
• sclerosing encapsulating peritonitis (rare, life threatening complication, mostly after ≥ 6 years on PD, peritoneum is massively thickened and calcificated, leading to intestinal obstruction)
Complications of PD 1Complications of PD 1

Non-infectious:
• Leakage of dialysate along the peritoneal catheter
• Drainage failure of dialysate (dislocation or catheter obstruction by fibrin)
• Morphologic changes of peritoneum following long-lasting PD (peritoneal fibrisis, mesotelial damage, vasculopathy and neo-angiogenesis) leading to loss of UF capacity – reason for PD cessation in 24% of all patients, and in 51% of patients treated above 6 years.
Complications of PD 2Complications of PD 2
• Large vascular surface of peritoneum (due to neo-angiogenesis, vasodilation), leading to high (fast) type of transport including fast loss of osmotic glucose pressure
• Decreased function of aquaporins
• High lymfatic absorption
Causes of UF failure Causes of UF failure

Morphologic changes of peritoneum due Morphologic changes of peritoneum due to PD (1)to PD (1)
Obr.1-before starting PD, norm. peritoneum (omentum)

Morphologic changes of peritoneum due to PD Morphologic changes of peritoneum due to PD (2)(2)
Obr.2-after 3 years of PD, submesotelial fibrosis and neo-angiogenesis (enlargement of vascular surface of peritoneum)

Peritonitis • Clinical features: cloudy PD effluent, abdominal pain,
nausea, vomiting, • Laboratory: leucocytosis, CRP, > 100wbc/ mm3, PD fluid
culture• Bacteriology: Gram + cocci (incl. S.aureus) in 75%,
Gram – (incl. Pseudomonas) in 25%, culture negative, mycobacterial (1%), fungal (3%), allergic (Icodextrin)
• Complications: relapses, antibiotic treatment failure, acute and chronic UF failure
• Treatment for. 14-21 days : Gram + cocci: Vankomycin / cephalosporin, Gram -: aminoglycoside / cephalosporin III. Generation (+ antimycotics, metronidazole)
• Goal: < peritonitis / 18 months
From PD gudelines (ISPD)
• biocompatible PD solutions - normal pH, low concentration of glucose
• insertion of PD catheter – 10 days-6 weeks before RRT
• urea / creatinine clearance measured every 6 months• PET: 6 weeks after commencing treatment + annually• avoid routine use of high glucose concentrations )use
of icodextrin, aminoacids instead)• preserve residual diuresis, obtain UF above 750 ml/day• peritonitis and exit-site infection rates, regular revision
of technique• invasive procedures cover by ATB prophylaxis• topical ATB administration if needed (S.aureus, Ps.
aeruginosa)• beware central obesity

∀ ↓ GDPs and AGEs∀ ↓ Lactate• Physiologic pH and pCO2
∀ ↑ Membrane and immune cell function
PhysionealPhysioneal11
Perspectives - New dialysis solutions Perspectives - New dialysis solutions protect peritoneal membrane protect peritoneal membrane
11Skoufos, et al. Skoufos, et al. Kidney IntKidney Int. 2003;64(suppl 88):S94-S99.. 2003;64(suppl 88):S94-S99.22Vardhan, et al. Vardhan, et al. Kidney Int.Kidney Int. 2003;64(suppl 88):S114-S123. 2003;64(suppl 88):S114-S123.
Nutrineal2
• No glucose exposure• No GDPs or AGEs∀ ↑ Membrane and immune cell
function
• Isosmolar to plasmaIsosmolar to plasma• No glucose exposureNo glucose exposure∀ ↓↓ GDPs and AGEsGDPs and AGEs∀ ↑↑ Membrane and immune cell Membrane and immune cell
functionfunction
ExtranealExtraneal22

PhysionealPhysioneal↓↓ Infusion painInfusion pain↓↓ PeritonitisPeritonitis↑↑ Glycemic controlGlycemic control↑↑ AppetiteAppetite↑↑ Patient acceptancePatient acceptanceNo No ↓↓ UF UF
Clinical advantages of new dialysis Clinical advantages of new dialysis solutions solutions
ExtranealExtraneal↓↓ Glucose load Glucose load ↑↑ Glycemic controlGlycemic control↑↑ UF, control of fluid statusUF, control of fluid status↓↓ DyslipidemiaDyslipidemia↑↑ Quality of lifeQuality of life↑↑ Time on PDTime on PD
Pecoits-Filho, et al. Pecoits-Filho, et al. Kidney IntKidney Int. 2003;64(suppl 88):S100-S104.. 2003;64(suppl 88):S100-S104.Vardhan, et al. Vardhan, et al. Kidney Int.Kidney Int. 2003;64(suppl 88):S114-S123. 2003;64(suppl 88):S114-S123.
NutrinealNutrineal↓↓ Glucose loadGlucose load↑↑ Glycemic controlGlycemic control↑↑ Protein intake, nutritional statusProtein intake, nutritional status
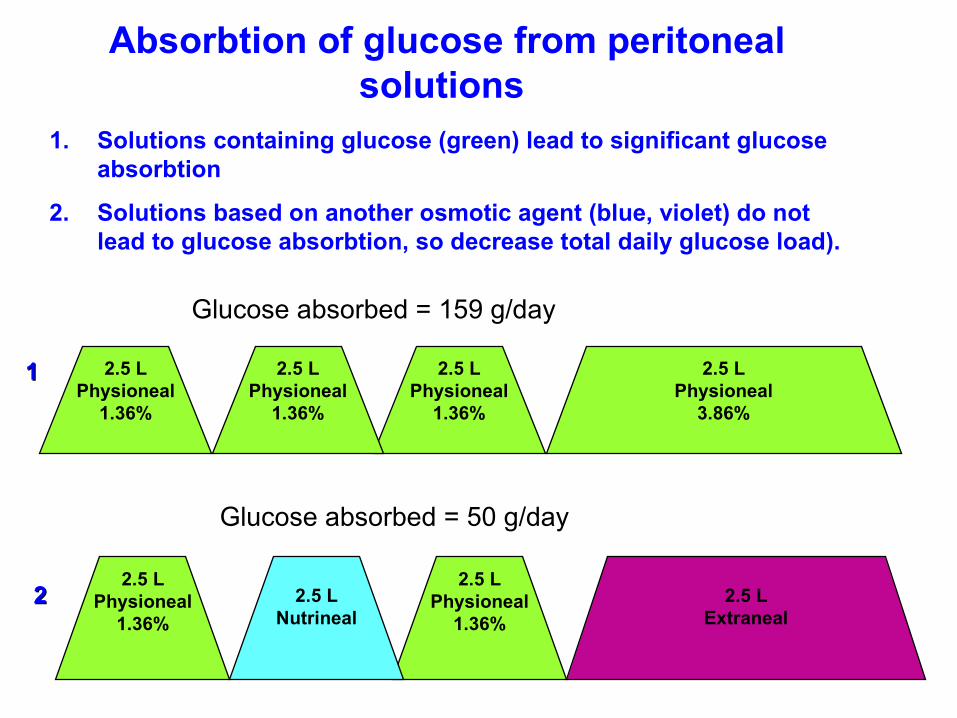
2.5 LPhysioneal
1.36%
2.5 LPhysioneal
1.36%
2.5 LPhysioneal
1.36%
2.5 LPhysioneal
3.86%
Glucose absorbed = 159 g/day
2.5 LPhysioneal
1.36%
2.5 LNutrineal
2.5 LPhysioneal
1.36%
2.5 LExtraneal
Glucose absorbed = 50 g/day
Absorbtion of glucose from peritoneal solutions
1. Solutions containing glucose (green) lead to significant glucose absorbtion
2. Solutions based on another osmotic agent (blue, violet) do not lead to glucose absorbtion, so decrease total daily glucose load).
11
22