
1/16/2017 - c.ymcdn.com · determir (levemir), 70/30 mix insulin (NovoLog and Novolin 70/30),...
27
1/16/2017 1 Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E. Director Beaumont Endocrine Center Chief Endocrinology, William Beaumont Hospital Grosse Pointe Type 2 Diabetes: A New Approach in a New Era of Therapies Conflict • I’m married to a drug representative and she works for Novo Nordisk • Makers of liraglutide (Victoza), aspart (NovoLog), determir (levemir), 70/30 mix insulin (NovoLog and Novolin 70/30), degludec (Tresiba), repaglinide (Prandin), glucagon (GlucaGen HypoKit), estradiol vaginal tablets (Vagifem), estradiol/norethindrone (Activella), somatropin (Norditropin), coagulation factor VIIIa (NovoSeven) • I’m a consultant on insulin pumps and lead groups for the Insulet Corporation • They make an insulin delivery system (pod/pump) called the Omni Pod Resources
Transcript of 1/16/2017 - c.ymcdn.com · determir (levemir), 70/30 mix insulin (NovoLog and Novolin 70/30),...

1/16/2017
1
Michigan Association of Osteopathic Family Physicians
Mid-Winter Family Medicine Update
Shanty Creek Resort, MI
January 19-22nd 2017
Michael R. Brennan D.O., M.S., F.A.C.E.
Director Beaumont Endocrine Center
Chief Endocrinology, William Beaumont Hospital Grosse Pointe
Type 2 Diabetes:
A New Approach in a New Era of Therapies
Conflict
• I’m married to a drug representative and she works for Novo Nordisk
• Makers of liraglutide (Victoza), aspart (NovoLog), determir (levemir), 70/30 mix insulin (NovoLog and Novolin 70/30), degludec (Tresiba), repaglinide (Prandin), glucagon (GlucaGen HypoKit), estradiol vaginal tablets (Vagifem), estradiol/norethindrone (Activella), somatropin (Norditropin), coagulation factor VIIIa (NovoSeven)
• I’m a consultant on insulin pumps and lead groups for the Insulet Corporation• They make an insulin delivery system (pod/pump)
called the Omni Pod
Resources

1/16/2017
2
Resources
Resources -https://www.aace.com/publications/algorithm
1/16/2017
3
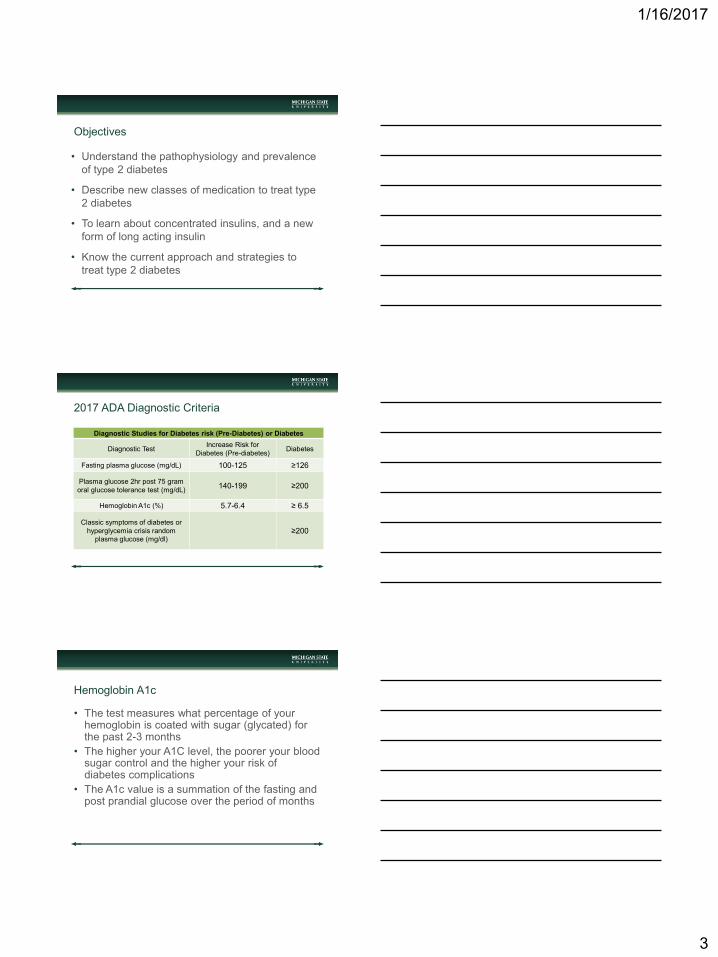
Objectives
• Understand the pathophysiology and prevalence
of type 2 diabetes
• Describe new classes of medication to treat type
2 diabetes
• To learn about concentrated insulins, and a new
form of long acting insulin
• Know the current approach and strategies to
treat type 2 diabetes
2017 ADA Diagnostic Criteria
Diagnostic Studies for Diabetes risk (Pre-Diabetes) or Diabetes
Diagnostic TestIncrease Risk for
Diabetes (Pre-diabetes)Diabetes
Fasting plasma glucose (mg/dL) 100-125 ≥126
Plasma glucose 2hr post 75 gram
oral glucose tolerance test (mg/dL)140-199 ≥200
Hemoglobin A1c (%) 5.7-6.4 ≥ 6.5
Classic symptoms of diabetes or
hyperglycemia crisis random
plasma glucose (mg/dl)≥200
Hemoglobin A1c
• The test measures what percentage of your hemoglobin is coated with sugar (glycated) for the past 2-3 months
• The higher your A1C level, the poorer your blood sugar control and the higher your risk of diabetes complications
• The A1c value is a summation of the fasting and post prandial glucose over the period of months

1/16/2017
4
Hemoglobin A1c
A1C level (%) Estimated average blood glucose (mg/dl)
5 97
6 128
7 154
8 183
9 212
10 240
11 269
12 298
13 326
14 355
Types of Diabetes
• Type 2 Diabetes
• Type 1 Diabetes and Latent-onset Autoimmune Diabetes of Adulthood
• Gestational Diabetes
• Monogenic DM (formerly Maturity Onset Diabetes of the Young, e.g. MODY)
• Type 3 – A category of diabetes that is a secondary form of diabetes. e.g. pancreatitis, cystic fibrosis, or glucocorticoid induced
Beta Cell Function
• Type 2 diabetes is hallmarked by the body
systemically having insulin resistance, and
therefore at first insulin excess
• Type 1 diabetes is defined by the body having
beta cell destruction, and therefore insulin
deficiency

1/16/2017
5
Type 2 Diabetes (T2DM)
• The most common form of DM, accounting for more than 90% of cases
• Typically identified in patients older than 30 years who are overweight or obese and/or have a positive family history, but do not have auto antibodies (characteristic of type 1)
• Most persons with T2DM have evidence of insulin resistance (such as high triglycerides or low high-density lipoprotein cholesterol [HDL-C])
The Diabetes Epidemic in the United States
In 2012, 29.1 million Americans or 9.3% of the U.S. population had diabetes (in 2010 it was 25.8 million or 8.3%)
In 2012, among U.S. residents age 65 and older, 25.9% had diabetes
By 2050 it is estimated that 1 in 3 people in the U.S. will have diabetes
–http://www.diabetes.org/diabetes-basics/statistics/
–http://www.cdc.gov/chronicdisease/resources/publications/AAG/ddt.htm
Simple Description of T2DM
Gerich JE. Mayo Clin Proc. 2003;78:447-456
outpatient.aace.com/sites/all/files/T2DM-S2-Clinical-Presentation.pptx

1/16/2017
6
Transition to T2DM
Figure courtesy of CADRE.
Adapted from Holman RR. Diabetes Res Clin Pract. 1998;40(suppl):S21-S25;
Ramlo-Halsted BA, Edelman SV. Prim Care. 1999;26:771-789; Nathan DM. N Engl J Med. 2002;347:1342-1349; UKPDS Group. Diabetes. 1995;44:1249-1258
outpatient.aace.com/sites/all/files/T2DM-S2-Clinical-Presentation.pptx
2017 ADA Approach
2016 AACE Approach

1/16/2017
7
Where is your intervention in the
progression of diabetes?
Spectrum of Diabetes Type of Prevention
No disease
Impaired fasting glucose/impaired glucose tolerance
Primary
Diagnosis of Diabetes Secondary
Complications of Diabetes Tertiary
Death
What’s Your Approach To T2DM Treatment?
• Pathophysiologic approach to correct the core defects with T2DM? -Preferred!!!!!
• Treat with an agent until failure by A1C readings?
What approach you chose is based on several variables, i.e. your familiarity with the medicine, patient age and comorbidities, insurance, formulary, cost, medication side effects, patient adherence, etc…
Ideal Treatment
• Try to select complimentary anti-diabetes agents that correct specific pathophysiologic disturbances present in T2DM
• Treatment should be based upon reversal of known pathogenic abnormalities and not simply on reducing HbA1c
• Early treatments can prevent/slow progressive beta cell failure/T2DM
1/16/2017
8
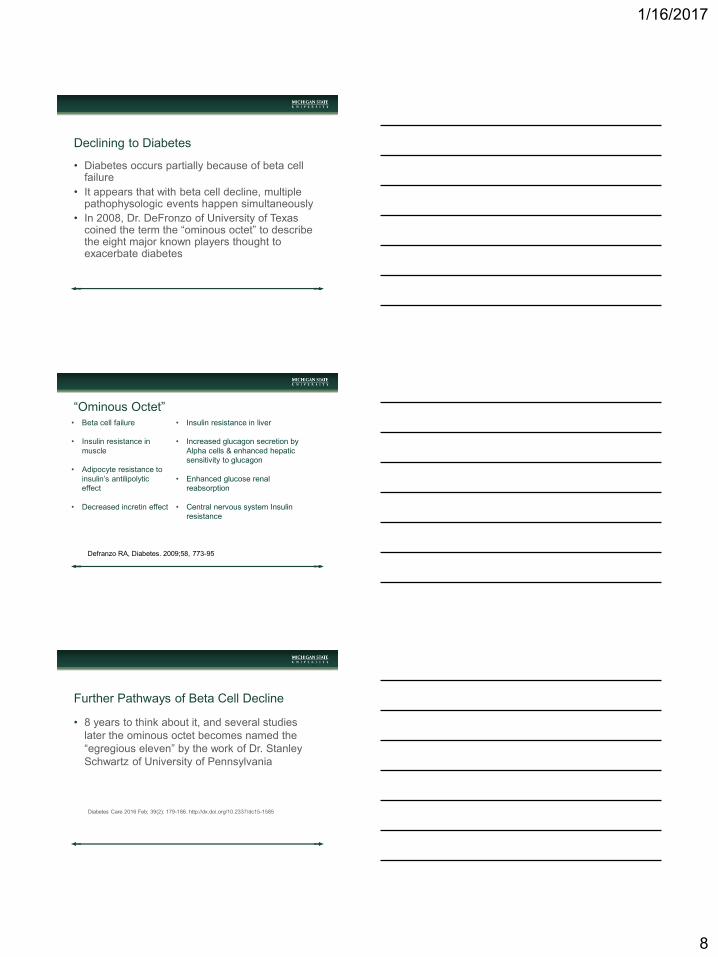
Declining to Diabetes
• Diabetes occurs partially because of beta cell failure
• It appears that with beta cell decline, multiple pathophysologic events happen simultaneously
• In 2008, Dr. DeFronzo of University of Texas coined the term the “ominous octet” to describe the eight major known players thought to exacerbate diabetes
“Ominous Octet”• Beta cell failure
• Insulin resistance in
muscle
• Adipocyte resistance to
insulin’s antilipolytic
effect
• Decreased incretin effect
• Insulin resistance in liver
• Increased glucagon secretion by
Alpha cells & enhanced hepatic
sensitivity to glucagon
• Enhanced glucose renal
reabsorption
• Central nervous system Insulin
resistance
Defranzo RA, Diabetes. 2009;58, 773-95
Further Pathways of Beta Cell Decline
• 8 years to think about it, and several studies
later the ominous octet becomes named the
“egregious eleven” by the work of Dr. Stanley
Schwartz of University of Pennsylvania
Diabetes Care 2016 Feb; 39(2): 179-186. http://dx.doi.org/10.2337/dc15-1585

1/16/2017
9
“Egregious Eleven”
• Beta cell failure
• Insulin resistance in
muscle
• Adipocyte resistance to
insulin’s antilipolytic
effect
• Decreased incretin
effect
• Insulin resistance in liver
• Increased glucagon
secretion by Alpha cells &
enhanced hepatic
sensitivity to glucagon
• Enhanced glucose renal
reabsorption
• Central nervous system
Insulin resistance
• Increased
inflammation and
immune dysregulation
• Colon/Microbiom
dysregulation
• Stomach and small
intestine increased
absorption of glucose
Diabetes Care 2016 Feb; 39(2): 179-186. http://dx.doi.org/10.2337/dc15-1585
T2DM Treatment
• If no intervention occurs and beta cells are
destroyed, then all roads lead to insulin
• Insulin is a miracle medicine and will arguably
always work, but some caveats exist
The Medications for T2DM Treatment
• ALL approaches begin with metformin, if
possible
• ALL approaches end with insulin, if possible
• What pharmacological agents are used between
metformin and insulin is your clinical decision
1/16/2017
10
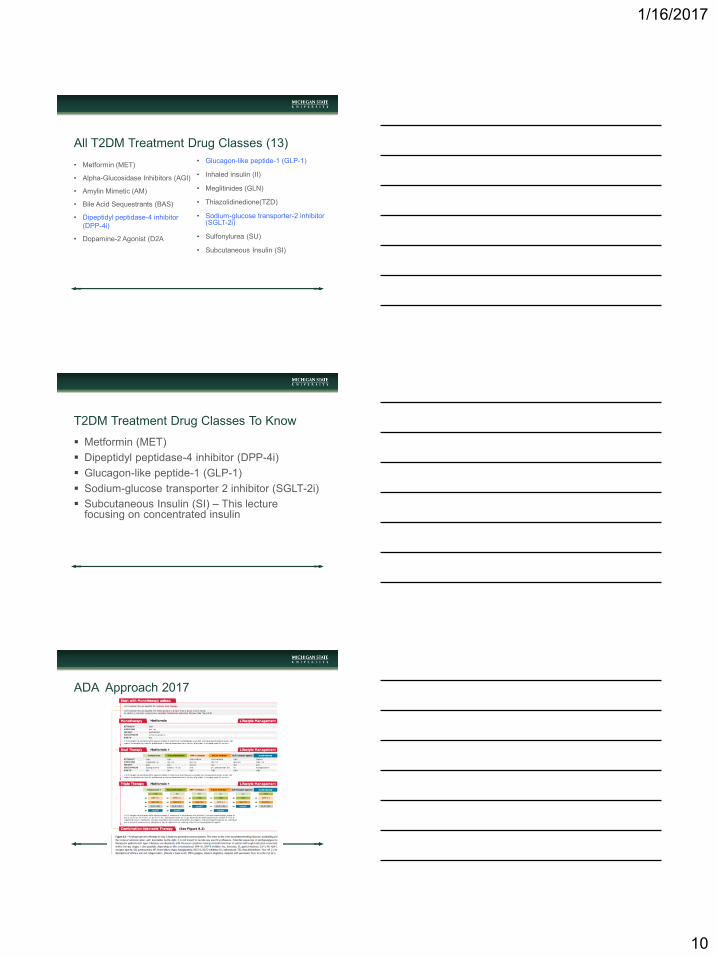
All T2DM Treatment Drug Classes (13)
• Metformin (MET)
• Alpha-Glucosidase Inhibitors (AGI)
• Amylin Mimetic (AM)
• Bile Acid Sequestrants (BAS)
• Dipeptidyl peptidase-4 inhibitor
(DPP-4i)
• Dopamine-2 Agonist (D2A
• Glucagon-like peptide-1 (GLP-1)
• Inhaled insulin (II)
• Meglitinides (GLN)
• Thiazolidinedione(TZD)
• Sodium-glucose transporter-2 inhibitor (SGLT-2i)
• Sulfonylurea (SU)
• Subcutaneous Insulin (SI)
T2DM Treatment Drug Classes To Know
Metformin (MET)
Dipeptidyl peptidase-4 inhibitor (DPP-4i)
Glucagon-like peptide-1 (GLP-1)
Sodium-glucose transporter 2 inhibitor (SGLT-2i)
Subcutaneous Insulin (SI) – This lecture focusing on concentrated insulin
ADA Approach 2017
1/16/2017
11
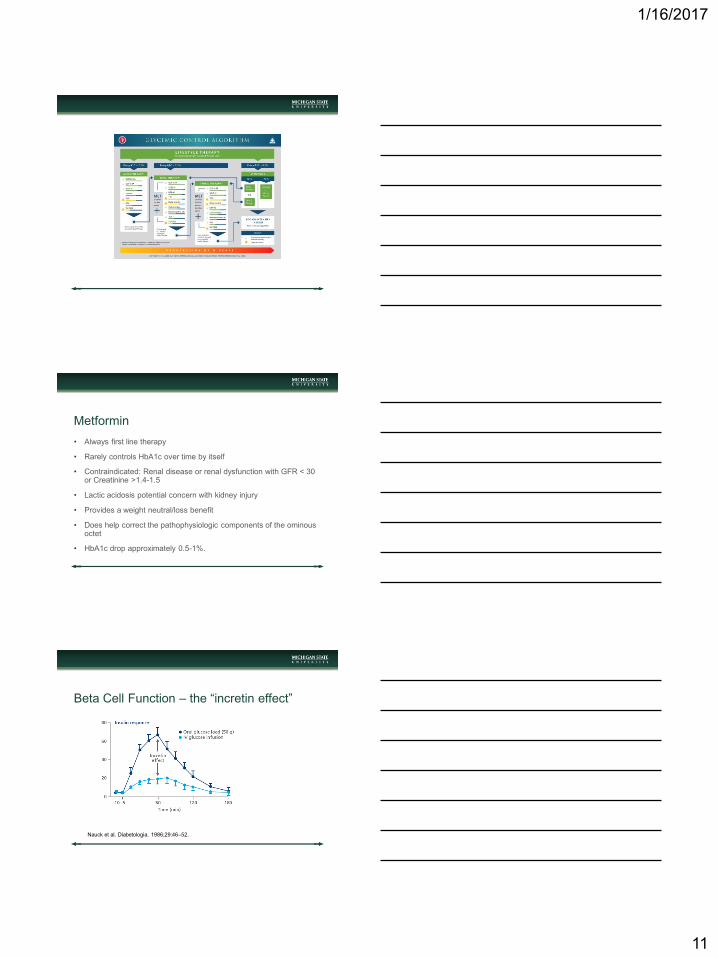
Metformin
• Always first line therapy
• Rarely controls HbA1c over time by itself
• Contraindicated: Renal disease or renal dysfunction with GFR < 30 or Creatinine >1.4-1.5
• Lactic acidosis potential concern with kidney injury
• Provides a weight neutral/loss benefit
• Does help correct the pathophysiologic components of the ominous octet
• HbA1c drop approximately 0.5-1%.
Beta Cell Function – the “incretin effect”
Nauck et al. Diabetologia. 1986;29:46–52.

1/16/2017
12
The Incretin Effect
• The hormone Glucagon Like Peptide-1(GLP-1)
is currently the best know agent responsible for the
incretin effect
• It is the understanding of the GLP-1 hormone
receptors and its metabolism/breakdown by which
the GLP-1RA and DPP-4i drug classes work
Glucagon Like Peptide-1 Receptor Agonist
(GLP-1 RA)
• Albiglutide (Tanzeum)
• Dulaglutide (Trulicity)
• Exenatide (Byetta)
• Exenatide Extended release (Bydureon)
• Liraglutide (Victoza)
• Lixisenatide (Adlyxn) – Use in U.S.A 2017/18
GLP-1 Receptor Agonist
Disadvantages:
• Requires an injection
• Used to have limited formulary coverage
(Greatly improved recently)
• Can have GI difficulty
• Black box warning for medullary thyroid
carcinoma in rats

1/16/2017
13
GLP-1 Receptor Agonist
Advantages:
• Restore beta cell glucose sensitivity
• May replenish beta cell insulin stores, and may cause beta cell proliferation
• Appears to slow gastric empting and cause satiety
• Inhibit glucagon secretion
• Cause weight loss
• Minimal to no hypoglycemia
• Estimated A1c decline 0.5 to 1.5%
Dipeptidyl peptidase- 4 inhibitor (DPP- 4i)
• Aloglipitin (Nesina)
• Linagliptin (Trajenta)
• Saxaglipitin (Onglyza)
• Sitagliptin (Januvia)
DPP- 4 Inhibitor
Disadvantage:
• The effect of the drug depends on endogenous
GLP-1 quantity
• Used to have limited formulary coverage
(Greatly improved recently)
• Every formulation, except linagliptin, requires
adjustment based on renal function

1/16/2017
14
DPP- 4 Inhibitor
Advantages:
• Restores Beta cell glucose sensitivity
• Appears to slow gastric emptying
• Inhibit glucagon secretion
• Weight neutral
• Minimal to no hypoglycemia
• Estimate A1c decline 0.5-1.0%
GLP-1 Receptor Agonists vs. DPP-4 Inhibitors
GLP-1 RA DPP-4i
Injection Oral
SupraphysiologicLimited by endogenous GLP-1
level
Large A1c decline Moderate A1c decline
Weight Loss Weight Neutral
GI upset, Black box warningSome renal adjustment, well
tolerated
Sodium Glucose Transporter 2 Inhibitors (SGLT2-i)
• Canagliflozin (Invokana)
• Dapagliflozin (Farxiga)
• Empagliflozin (Jardiance)
1/16/2017
15
SGLT-2 Inhibitor
Disadvantages:
• Not recommended for prescribing to people with kidney disease as kidney disease prevents the drug from working
• Increase urinary tract yeast infection
• Clinical trials display possible liver damage as well as breast and bladder cancers (not high enough degree to indicate a clear increase in risk)
• Questionable induction of DKA
SGLT-2 Inhibitor
Advantages:
• Work by preventing the kidneys from reabsorbing glucose back into the blood stream
• Increase insulin sensitivity in muscle and in liver tissue
• Decrease gluconeogenesis
• Weight neutral or loss
• Estimate A1c decline 0.5-1.0%
Insulin Injections
General clinical classes of insulin:
• Rapid
• Regular
• Mix
• NPH
• Basal

1/16/2017
16
Insulin Injections
Disadvantages:
• Possible weight gain
• In type 2 diabetes, treating a hyper insulinemic state with more insulin may beget macrovascular disease
• Hypoglycemia
• Injections are considered by some patients and physicians to require more maintenance
Insulin Injections
Advantages:
• All roads lead to insulin once all other methods have failed
• Improved glucose storage
• Decreased glucagon production
• Decreased hepatic glucose production
• Universally effective
• Estimate A1c decline = can always get to goal
Introduction To Concentrated Insulin

1/16/2017
17
A Unit Of Insulin
• 1 unit of insulin is approximately 50 micrograms of
crystalline insulin
• This “unit” was termed by Dr. Fredrick Banting (One of
two people who won the Nobel Prize for the discovery of
insulin)
• This unit of insulin would lower a fasting rabbit’s blood
sugar approximately 50 mg/dL
The term U
• The “U” represents the amount of a particular enzyme
(e.g. U/ml). Written on an insulin vial, it describes the
number of insulin units (or concentration) in one 1ml or
1cc of fluid
Therefore:
• U-100 is 100 units of insulin per 1 ml or cc
• U-200 is 200 units of insulin per 1 ml or cc
• U-300 is 300 units of insulin per 1 ml or cc
• U-500 is 500 units of insulin per 1 ml or cc
1 Unit of Insulin
• 1 unit of insulin in the United States comes in a variety of
fluid concentrations (U-40, U-80, U-100, U-200, U-300
and U-500)
• The most commonly used concentration of insulin in
clinical medicine today is the U-100 insulin concentration
• U-500 first entered the U.S. market in 1952 to address
patients with diabetes requiring high dose insulin therapy
• In 1952 patients with diabetes requiring high insulin
doses were those with antibodies to pork insulin

1/16/2017
18
Which Has More Insulin?
1 Unit Of U-100 Insulin Or 1 Unit Of U-500
Insulin?
Answer: They are the same!
Akin to the following:
Which weighs more?
A pound of feathers or a pound of
bricks?
Both are a pound
Point of Confusion – U-100 syringe
Point of Confusion
In the US, insulin syringes were designed for U-100 insulin. If any concentration of insulin other than U-100 is drawn into an insulin syringe, then it WOULD NOT correlate with the demarcated dose
A thought experiment for example: Draw the insulin up in the syringe to the 10 unit line…
• If drawn up with U-100 then the dose is 10 units
• If drawn up with U-200 then the dose is 20 units
• If drawn up with U-300 then the dose is 30 units
• If drawn up with U-500 then the dose is 50 units

1/16/2017
19
Points of Clarity – U-100 and U-500 syringe
No Longer A Point Of Confusion
To stop this confusion of dosing concentrated insulins, the pharmaceutical industry created pens to help the patient, the pharmacist, the nurse, and the prescriber
When administering with a concentrated insulin pen, the dose on the pen is the amount of insulin the patient will receive
Example: Take 50 units of U-200 insulin in the pen. The patient simply places the pen to 50 unit mark and administers dose (the proper volume is administered by the pen)
Concentrated Insulin Today
Concentrated Insulin – Insulin resistance can be
so severe that the volume of the insulin injection
can be overwhelming. Therefore, the units of
insulin can be manufactured and delivered in a
smaller volume.
• U-500 Regular (Humulin R)
• U-300 Glargine (Toujeo)
• U-200 Lispro (Humalog)
• U-200 Degludec (Tresiba)

1/16/2017
20
Regular U-500 also known as Humulin R U-500
Used for meals and/or basal insulin
Recent FDA approval now available in a prefilled pen
Each pen contains 3mL of fluid and 1,500 units
Warning! This insulin is available in both pens and vials
Regular U-500 also known as Humulin R U-500
Lispro U-200 also known as Humalog U-200
• Concentrated version of rapid mealtime insulin
• Each pen contains 3mL of fluid and 600 units

1/16/2017
21
Lispro U-200 also known as Humalog U-200
Glargine U-300 also known as Toujeo
Concentrated version of a basal insulin
Each pen contains 1.5 mL of fluid and 450 units
Glargine U-300 also known as Toujeo

1/16/2017
22
Degludec U-100 and U-200 also known as
Tresiba U-100 and U-200
• New class of basal insulin (1st one in a decade)
• Half life is 25 hours, with 42+ hours of clinical
duration of action
• U-100 pen holds 3mL of fluid and 300 units
• U-200 pen holds 3mL of fluid and 600 units
Degludec U-100 and U-200 also known as
Tresiba U-100 and U-200
Advantages:
• Has a better clinical effect by having less
variability, less hypoglycemia, and less stringent
dosing time
• Because of the afore mentioned effects, it
appears that it is a more clinically appropriate
basal insulin
Degludec U-100 and U-200 also known as
Tresiba U-100 and U-200

1/16/2017
23
Degludec (Treisba) U-100 and U-200
So Why Use Concentrated Insulin?
This is generally for patients receiving greater than 60 units of U-100 insulin per injection
• There may be better absorption and physiologic effect
• Potentially, less pain with injection
• Likely, less loss of insulin with injection
• Patient may get more insulin for the same price
New Mix! Long acting insulin plus GLP-1
Insulin Glargine plus Lixisenatide (Soliqua 100/33)
• Both are once a day injection formats to manage Type 2 diabetes
• One drug takes care of lack of Basal glucose control
• Glargine
• One drug takes care of lack of post prandial control• Lixisenatide

1/16/2017
24
New Mix! Long acting insulin plus GLP-1
Insulin Glargine plus Lixisenatide (Soliqua 100/33)
Clinical Application
Current Applications For T2DM
(After METFORMIN)
• Use a weight neutral, and beta cell preservation
strategy
• Be familiar with at least one agent of the
following classes:
• DPP-4i
• SGLT-2i
• GLP-1RA
1/16/2017
25
Not a Good Combination
(After METFORMIN)
• GPL-1RA and DPP-4i are NOT given together
• Both work in the incretin pathway
Theoretical Combinations (AFTER
METFORMIN)
• Add one of the following either a GLP-1 RA,
SGLT-2i, or DPP-4i
• If still not to goal
• Try combination either GLP-1 RA and SGLT-2i,
or DPP-4i and SGLT-2i
• If still not to goal, consider
thiazolidinedione(TZD), alpha-glucosidase
inhibitors(AGI) or insulin
Best Approach
• Great T2DM therapeutic approaches improve the following:
• Long lasting tolerability
• Glucose lowering efficacy
• Have a weight loss effect
• Improve blood pressure
• Decrease lipid profile
• Provide cardiovascular protection
• Decrease side effects (e.g. particularly hypoglycemia)

1/16/2017
26

1/16/2017
27
In Conclusion
• Once T2DM is diagnosed, use a pathophysiologic approach, not a treat until failure (A1c rises) approach
• Be familiar with at least one drug from the following class: DPP-4i, GLP-1RA, and SGLT-2i
• Use concentrated insulin PENS, so the dosing is simplified
• The science and art of medicine are both very important in the management of diabetes
• Giving great care to your patients, can result in long and healthy lives without complications
Thank you!
• Questions?
• To Contact Dr. Michael R. Brennan
• Contact the Beaumont Endocrine Center• 25631 Little Mack, Suite 204
• St. Clair Shores, MI 48084
• Phone: 586-443-2380
• Fax: 586-443-2381
• Call Beaumont Health system and ask to have him paged• 248-898-5000
Inhaled Insulin


















