1101 Budding of the Pre-Chylomicron Transport Vesicle is Controlled by Phosphorylation of Sar1b
2
AGA Abstracts 1098 Once-Daily Versus Twice-Daily Mesalazine for Mild to Moderately Active Ulcerative Colitis: Mucosal Healing and Early Response Data From MOTUS, a Multicentre, Controlled, Randomised, Investigator-Blinded Study Marie J. Pierik, Bernard Flourie, Herve Hagege, Gilbert Tucat, Ad Masclee, Olivier Dewit, Chris Probert, Per Broberg, Aoucheta Djamila Background: Reduced dosing frequency makes treatment easier and improves compliance with 5-ASA in ulcerative colitis (UC). The multicentre, controlled, randomised, investigator- blinded MOTUS study (sponsor: Ferring Pharmaceuticals; NCT00737789) showed non- inferiority of OD vs BD 5-ASA (Pentasa®) for the induction of remission in active UC; we describe mucosal healing and early response data. Methods: Patients (pts) with mild to moderately active UC were randomised to 5-ASA (prolonged release granules, new formula- tion) 4g/day for 8 weeks: 2x 2g OD or 1x 2g BD. All pts received 5-ASA enema (1g/day) for the first 4 weeks. Endpoints included: induction of remission; mucosal healing (UC- DAI endoscopic mucosal appearance score ≤1); time to cessation of bleeding (first bleeding- free day); and time to remission (normal stool frequency and cessation of bleeding; pts' diaries). Normal stool frequency (UC-DAI stool frequency subscore 0), clinical remission (abbreviated UC-DAI score 0), treatment failure (need for disallowed treatments), and non- bleeding stools (UC-DAI rectal bleeding subscore 0) at week 4 were also analysed. Observed case analyses are shown. Categorical variables were analysed by Cochran-Mantel Haenszel chi-squared test and time-to-endpoint variables by Cox survival analysis, all adjusted by country. Results: 206 pts were enrolled and 202 included in intent-to-treat analyses (n=101 per arm). OD 5-ASA was superior to BD for mucosal healing at week 8 (87.5% vs 71.1% respectively; difference 16.4% [CIs 4.5-28.2]; P=0.007). Median time to remission was significantly shorter with OD vs BD dosing (26 vs 28 days, respectively; P=0.042), as was time to cessation of bleeding (13 vs 21 days, respectively; P=0.139). At week 4, significantly more pts had normal stool frequency with OD vs BD dosing (P=0.013); there was no significant difference in rates of clinical remission, treatment failure or non-bleeding stools. Conclusion: Significantly more pts with active UC achieved mucosal healing at week 8 and normal stool frequency at week 4 with 4g 5-ASA OD vs BD, and median time to remission was significantly shorter with OD therapy. Time to cessation of bleeding was shorter with OD vs BD, but not significant. Other secondary endpoints were similar with OD and BD dosing at week 4. These data are consistent with those seen for induction of remission, and suggest that OD Pentasa® offers potential benefits to patients. 1099 A Retrospective Study of Colectomy Complications and Their Associated Costs for Patients With Ulcerative Colitis Edward V. Loftus, Paul Leonard, Mei Yang, Oscar Hayes, Parvez Mulani, Jingdong Chao Aim: Patients with refractory moderate to severe ulcerative colitis (UC) can benefit from removal of the diseased colon. Long-term claims data on colectomy complications are limited. Using a large health care claims database, this study investigated the long-term complications and their associated costs in patients with UC who undergo colectomy. Methods: To assess the complications of colectomy, a retrospective analysis of a Thomson Reuters MarketScan® claims database (Q1 2001-Q4 2010) was performed. The sample included patients with UC who (1) were ≥18 years of age with ≥2 UC claims (ICD-9-CM 556.xx) and no concurrent CD diagnosis (ICD-9-CM 555.xx), (2) received a colectomy (CPT-4: 44140-44160, 44204- 44213, 45113-45121) after their second UC diagnosis, and (3) had continuous health care coverage during the 6 months before colectomy and 1, 2, and 5 years after colectomy. The complications of colectomy (defined by ICD-9 codes) included abscess, small bowel obstruction, rectal anal stenosis, intestinal fistula, vaginal fistula, and sepsis. The complication rates pre- and postcolectomy were compared for patients with 1-, 2-, and 5-year follow-up data separately (Table 1), where cumulative rates were calculated for patients with more than 1 year of data. The average total health care costs were evaluated from the day patients received a colectomy through the 1-, 2-, and 5-year postcolectomy periods and then were compared between patients with and without complications during each study period (Table 2). Results: There were 1016 patients with continuous medical coverage 1 year after colec- tomy, 658 patients with 2 years' coverage, and 196 patients with 5 years' coverage. Complica- tion rates increased substantially after colectomy over the course of 5 years of follow-up compared with the precolectomy period. The trends were consistent from Year 1 though Year 5. Average total health care costs since colectomy were significantly higher for patients with complications compared with those without complications. The costs increased consist- ently after the first year regardless of the patient's complication status. Conclusion: There is a high morbidity rate associated with colectomy among patients with UC, which is sustained for a long period of time. In addition to an expensive first year of total health care costs resulting from colectomy, the costs continue to increase in subsequent years and are especially high among patients with colectomy complications. Table 1. Complication Rates Pre- and Postcolectomy Table 2. Health Care Costs Postcolectomy S-198 AGA Abstracts a P <.01 for patients with complications vs. without complications. 1100 Health Resource Utilization of IBD Patients Treated With Anti-TNF and Immunomodulator Therapy: A VA Population Study Neena Abraham, Peter Richardson, Sunanda V. Kane New treatment goals beyond symptom control have been defined for IBD patients, including reductions in IBD-related surgery or hospitalization. The real-world effectiveness of early treatment with a biologic versus immunomodulator therapy on healthcare utilization remains poorly defined, thus, we assessed 1-year health resource utilization associated with biologic versus immunomodulator therapy in a national cohort of IBD patients. Methods: Veterans aged 18-99 diagnosed with Crohn's disease (CD) or ulcerative colitis (UC) (10/01/2001-09/ 30/2009) were identified from national administrative datasets of the Department of Veterans Affairs using a previously validated published algorithm. Inpatient, outpatient and death records were longitudinally linked to prescription fill data. Each person-day of follow- up was assessed for exposure to anti-TNF, immunomodulator, overlapping anti-TNF and immunomodulator (dual therapy) or absence of therapy (none). Time on regimen was measured (months), and Poisson regression models were used to assess outcomes after adjustment for demographics, comorbidity, smoking, prescription channeling, and other pharmacological effect modifiers (steroids, 5-ASA, NSAIDs and antibiotics). Results: A total of 20,474 patients were identified for inclusion (n=8,042 CD, n=12,432 UC; 93.9% male; 72.5% white; mean age, 60.9 [SD 14.5]). At index anti-TNF monotherapy (0.17%), immuno- modulator monotherapy (1.34%) and dual anti-TNF and immunomodulator therapy (1.48%) was prescribed with concomitant steroid (14%), 5-ASA (20.6%), NSAID (38.6%) and antibi- otics (28.7%). Unadjusted models revealed a protective benefit of immunomodulator mono- therapy on 1-year hospitalizations (OR 0.92; 0.90-0.94) and surgical rates (OR 0.93; 0.87- 0.99); however, when adjusted for UC vs. CD, smoking status, ethnicity, prescription channeling and pharmacological-effect modifiers, first-year risk reductions were observed for all strategies of interest. Immunomodulator monotherapy for 6.5 months resulted in fewer hospitalizations (42.4%) and surgeries (31.6%). Similarly, anti-TNF (mean, 6.1 months) resulted in a 13.3% reduction in hospitalizations and 40.7% reduction in surgery. Finally, as little as 3.4 months of dual therapy contributed to a 13.3% reduction in hospitaliza- tions and 39.2% reduction in surgery in the first year following index prescription. Conclu- sions: Among IBD patients, immunomodulator or anti-TNF monotherapy for as little as 6 months is associated with clinically significant reductions in 1-year health-resource utiliza- tion. Only 3.4 months of dual immunomodulator and anti-TNF therapy is required to achieve comparable health resource utilization benefits. Long-term maintenance of benefit requires further study, as does potential healthcare resource implications related to adverse drug events. 1101 Budding of the Pre-Chylomicron Transport Vesicle is Controlled by Phosphorylation of Sar1b Shahzad Siddiqi, Charles M. Mansbach Recombinant liver fatty acid binding protein (FABP1) can bud the pre-chylomicron transport vesicle (PCTV) from intestinal ER in the absence of ATP. Intestinal cytosol, containing 3% FABP1, requires ATP to bud PCTV. Our current data answer this conundrum. Cytosol isolated from primary rat enterocyte cultures fed 3H-oleate was separated on a Sephacryl S-100 HR column. The 3H-oleate eluted in the volume of a 75 kDa protein. FABP1 co- eluted with the 3H-oleate, not at its expected 14 kDa. A FABP1 pull down from the 3H- oleate-containing column fractions showed 4 proteins, FABP1, Sar1b, Sec13, and SVIP (total Mr = 77 kDa) by immunoblot. The 3H-oleate containing column fractions were passed over an anti-FABP1 antibody adsorption column. The eluted, adsorbed proteins migrated as a 75 kDa protein on native PAGE and were identified as FABP1, Sar1b, Sec13, and SVIP. These combined data all support the novel concept that FABP1 in native intestinal cytosol is present in a 4-membered protein complex. On incubation of the complex with intestinal ER, no increase in FABP1 binding to the ER was found over that present in resting ER and no increase in PCTV budding from the ER was found. On phosphorylation of the complex by PKCζ, the kinase required for PCTV ER budding from native cytosol (J. Cell Sci.: 121:2327-2338, 2008), active PCTV budding occurred. When the complex was incubated with γ-32P-ATP and PKCζ and separated on 2D gels, autoradiography showed only one protein was phosphorylated. This protein was identified as Sar1b by immunoblot and by LC-MS-MS with 56% coverage of the protein. The PKCζ phosphorylated a Thr on Sar1b. The effect of Sar1b phosphorylation on the 75 kDa complex was shown by separating the 75 kDa complex by native PAGE. Untreated, the complex with FABP1 migrated as a 75 kDa protein. The complex remained intact if the complex were treated with ATP and PKCζ incubated on ice, or PKCζ but no ATP, or ATP but no PKCζ both incubated at 370C. By contrast if the complex were incubated with PKCζ and ATP at 370C, the complex was completely disrupted as shown by immunoblot of the resulting proteins which all migrated at their expected monomer Mr on native PAGE. When FABP1 was released from the complex, but not when it remained part of the complex, it bound avidly to intestinal ER. We further show that only when the complex is incubated with PKCζ and ATP at 370C, is it able to actively bud PCTV from the ER. We conclude that FABP1 is a component of a 4-membered protein complex in intestinal cytosol. As a complex member, it is inhibited from binding to the ER and generating PCTV. Phosphorylation of Sar1b, a complex member, by PKCζ
-
Upload
shahzad-siddiqi -
Category
Documents
-
view
212 -
download
0
Transcript of 1101 Budding of the Pre-Chylomicron Transport Vesicle is Controlled by Phosphorylation of Sar1b

AG
AA
bst
ract
s1098
Once-Daily Versus Twice-Daily Mesalazine for Mild to Moderately ActiveUlcerative Colitis: Mucosal Healing and Early Response Data From MOTUS, aMulticentre, Controlled, Randomised, Investigator-Blinded StudyMarie J. Pierik, Bernard Flourie, Herve Hagege, Gilbert Tucat, Ad Masclee, Olivier Dewit,Chris Probert, Per Broberg, Aoucheta Djamila
Background: Reduced dosing frequency makes treatment easier and improves compliancewith 5-ASA in ulcerative colitis (UC). The multicentre, controlled, randomised, investigator-blinded MOTUS study (sponsor: Ferring Pharmaceuticals; NCT00737789) showed non-inferiority of OD vs BD 5-ASA (Pentasa®) for the induction of remission in active UC; wedescribe mucosal healing and early response data. Methods: Patients (pts) with mild tomoderately active UC were randomised to 5-ASA (prolonged release granules, new formula-tion) 4g/day for 8 weeks: 2x 2g OD or 1x 2g BD. All pts received 5-ASA enema (1g/day)for the first 4 weeks. Endpoints included: induction of remission; mucosal healing (UC-DAI endoscopic mucosal appearance score ≤1); time to cessation of bleeding (first bleeding-free day); and time to remission (normal stool frequency and cessation of bleeding; pts'diaries). Normal stool frequency (UC-DAI stool frequency subscore 0), clinical remission(abbreviated UC-DAI score 0), treatment failure (need for disallowed treatments), and non-bleeding stools (UC-DAI rectal bleeding subscore 0) at week 4 were also analysed. Observedcase analyses are shown. Categorical variables were analysed by Cochran-Mantel Haenszelchi-squared test and time-to-endpoint variables by Cox survival analysis, all adjusted bycountry. Results: 206 pts were enrolled and 202 included in intent-to-treat analyses (n=101per arm). OD 5-ASA was superior to BD for mucosal healing at week 8 (87.5% vs 71.1%respectively; difference 16.4% [CIs 4.5-28.2]; P=0.007). Median time to remission wassignificantly shorter with OD vs BD dosing (26 vs 28 days, respectively; P=0.042), as wastime to cessation of bleeding (13 vs 21 days, respectively; P=0.139). At week 4, significantlymore pts had normal stool frequency with OD vs BD dosing (P=0.013); there was nosignificant difference in rates of clinical remission, treatment failure or non-bleeding stools.Conclusion: Significantly more pts with active UC achieved mucosal healing at week 8 andnormal stool frequency at week 4 with 4g 5-ASA OD vs BD, and median time to remissionwas significantly shorter with OD therapy. Time to cessation of bleeding was shorter withOD vs BD, but not significant. Other secondary endpoints were similar with OD and BDdosing at week 4. These data are consistent with those seen for induction of remission, andsuggest that OD Pentasa® offers potential benefits to patients.
1099
A Retrospective Study of Colectomy Complications and Their AssociatedCosts for Patients With Ulcerative ColitisEdward V. Loftus, Paul Leonard, Mei Yang, Oscar Hayes, Parvez Mulani, Jingdong Chao
Aim: Patients with refractory moderate to severe ulcerative colitis (UC) can benefit fromremoval of the diseased colon. Long-term claims data on colectomy complications are limited.Using a large health care claims database, this study investigated the long-term complicationsand their associated costs in patients with UC who undergo colectomy. Methods: To assessthe complications of colectomy, a retrospective analysis of a Thomson Reuters MarketScan®claims database (Q1 2001-Q4 2010) was performed. The sample included patients withUCwho (1) were≥18 years of age with≥2 UC claims (ICD-9-CM 556.xx) and no concurrentCD diagnosis (ICD-9-CM 555.xx), (2) received a colectomy (CPT-4: 44140-44160, 44204-44213, 45113-45121) after their second UC diagnosis, and (3) had continuous health carecoverage during the 6 months before colectomy and 1, 2, and 5 years after colectomy.The complications of colectomy (defined by ICD-9 codes) included abscess, small bowelobstruction, rectal anal stenosis, intestinal fistula, vaginal fistula, and sepsis. The complicationrates pre- and postcolectomy were compared for patients with 1-, 2-, and 5-year follow-updata separately (Table 1), where cumulative rates were calculated for patients with morethan 1 year of data. The average total health care costs were evaluated from the day patientsreceived a colectomy through the 1-, 2-, and 5-year postcolectomy periods and then werecompared between patients with and without complications during each study period (Table2). Results: There were 1016 patients with continuous medical coverage 1 year after colec-tomy, 658 patients with 2 years' coverage, and 196 patients with 5 years' coverage. Complica-tion rates increased substantially after colectomy over the course of 5 years of follow-upcompared with the precolectomy period. The trends were consistent from Year 1 thoughYear 5. Average total health care costs since colectomy were significantly higher for patientswith complications compared with those without complications. The costs increased consist-ently after the first year regardless of the patient's complication status. Conclusion: Thereis a high morbidity rate associated with colectomy among patients with UC, which issustained for a long period of time. In addition to an expensive first year of total healthcare costs resulting from colectomy, the costs continue to increase in subsequent years andare especially high among patients with colectomy complications.Table 1. Complication Rates Pre- and Postcolectomy
Table 2. Health Care Costs Postcolectomy
S-198AGA Abstracts
aP <.01 for patients with complications vs. without complications.
1100
Health Resource Utilization of IBD Patients Treated With Anti-TNF andImmunomodulator Therapy: A VA Population StudyNeena Abraham, Peter Richardson, Sunanda V. Kane
New treatment goals beyond symptom control have been defined for IBD patients, includingreductions in IBD-related surgery or hospitalization. The real-world effectiveness of earlytreatment with a biologic versus immunomodulator therapy on healthcare utilization remainspoorly defined, thus, we assessed 1-year health resource utilization associated with biologicversus immunomodulator therapy in a national cohort of IBD patients. Methods: Veteransaged 18-99 diagnosed with Crohn's disease (CD) or ulcerative colitis (UC) (10/01/2001-09/30/2009) were identified from national administrative datasets of the Department of VeteransAffairs using a previously validated published algorithm. Inpatient, outpatient and deathrecords were longitudinally linked to prescription fill data. Each person-day of follow-up was assessed for exposure to anti-TNF, immunomodulator, overlapping anti-TNF andimmunomodulator (dual therapy) or absence of therapy (none). Time on regimen wasmeasured (months), and Poisson regression models were used to assess outcomes afteradjustment for demographics, comorbidity, smoking, prescription channeling, and otherpharmacological effect modifiers (steroids, 5-ASA, NSAIDs and antibiotics). Results: A totalof 20,474 patients were identified for inclusion (n=8,042 CD, n=12,432 UC; 93.9% male;72.5% white; mean age, 60.9 [SD 14.5]). At index anti-TNF monotherapy (0.17%), immuno-modulator monotherapy (1.34%) and dual anti-TNF and immunomodulator therapy (1.48%)was prescribed with concomitant steroid (14%), 5-ASA (20.6%), NSAID (38.6%) and antibi-otics (28.7%). Unadjusted models revealed a protective benefit of immunomodulator mono-therapy on 1-year hospitalizations (OR 0.92; 0.90-0.94) and surgical rates (OR 0.93; 0.87-0.99); however, when adjusted for UC vs. CD, smoking status, ethnicity, prescriptionchanneling and pharmacological-effect modifiers, first-year risk reductions were observedfor all strategies of interest. Immunomodulator monotherapy for 6.5 months resulted infewer hospitalizations (42.4%) and surgeries (31.6%). Similarly, anti-TNF (mean, 6.1months) resulted in a 13.3% reduction in hospitalizations and 40.7% reduction in surgery.Finally, as little as 3.4 months of dual therapy contributed to a 13.3% reduction in hospitaliza-tions and 39.2% reduction in surgery in the first year following index prescription. Conclu-sions: Among IBD patients, immunomodulator or anti-TNF monotherapy for as little as 6months is associated with clinically significant reductions in 1-year health-resource utiliza-tion. Only 3.4 months of dual immunomodulator and anti-TNF therapy is required toachieve comparable health resource utilization benefits. Long-term maintenance of benefitrequires further study, as does potential healthcare resource implications related to adversedrug events.
1101
Budding of the Pre-Chylomicron Transport Vesicle is Controlled byPhosphorylation of Sar1bShahzad Siddiqi, Charles M. Mansbach
Recombinant liver fatty acid binding protein (FABP1) can bud the pre-chylomicron transportvesicle (PCTV) from intestinal ER in the absence of ATP. Intestinal cytosol, containing 3%FABP1, requires ATP to bud PCTV. Our current data answer this conundrum. Cytosolisolated from primary rat enterocyte cultures fed 3H-oleate was separated on a SephacrylS-100 HR column. The 3H-oleate eluted in the volume of a 75 kDa protein. FABP1 co-eluted with the 3H-oleate, not at its expected 14 kDa. A FABP1 pull down from the 3H-oleate-containing column fractions showed 4 proteins, FABP1, Sar1b, Sec13, and SVIP (totalMr = 77 kDa) by immunoblot. The 3H-oleate containing column fractions were passed overan anti-FABP1 antibody adsorption column. The eluted, adsorbed proteins migrated as a75 kDa protein on native PAGE and were identified as FABP1, Sar1b, Sec13, and SVIP.These combined data all support the novel concept that FABP1 in native intestinal cytosolis present in a 4-membered protein complex. On incubation of the complex with intestinalER, no increase in FABP1 binding to the ER was found over that present in resting ER andno increase in PCTV budding from the ER was found. On phosphorylation of the complexby PKCζ, the kinase required for PCTV ER budding from native cytosol (J. Cell Sci.:121:2327-2338, 2008), active PCTV budding occurred. When the complex was incubatedwith γ-32P-ATP and PKCζ and separated on 2D gels, autoradiography showed only oneprotein was phosphorylated. This protein was identified as Sar1b by immunoblot and byLC-MS-MS with 56% coverage of the protein. The PKCζ phosphorylated a Thr on Sar1b.The effect of Sar1b phosphorylation on the 75 kDa complex was shown by separating the75 kDa complex by native PAGE. Untreated, the complex with FABP1 migrated as a 75kDa protein. The complex remained intact if the complex were treated with ATP and PKCζincubated on ice, or PKCζ but no ATP, or ATP but no PKCζ both incubated at 370C. Bycontrast if the complex were incubated with PKCζ and ATP at 370C, the complex wascompletely disrupted as shown by immunoblot of the resulting proteins which all migratedat their expected monomer Mr on native PAGE.When FABP1 was released from the complex,but not when it remained part of the complex, it bound avidly to intestinal ER. We furthershow that only when the complex is incubated with PKCζ and ATP at 370C, is it able toactively bud PCTV from the ER. We conclude that FABP1 is a component of a 4-memberedprotein complex in intestinal cytosol. As a complex member, it is inhibited from bindingto the ER and generating PCTV. Phosphorylation of Sar1b, a complex member, by PKCζ

disrupts the complex, releasing FABP1. The released FABP1 binds to the ER membrane andgenerates PCTV. In humans, genetic defects in Sar1b result in chylomicron retention in the ER.
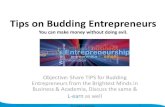
Phosphorylation of Sar1b disassembles the FABP1 containing, 75 kDa complex. A) Thecomplex in native cytosol. B) Phosphorylation of Sar1b Thr by PKCζ. C) Phosphorylationof Sar1b completely disassembles the complex. D) The freed FABP1 binds to the ER. Notshown: On FABP1 binding to the ER, PCTV are generated. FABP1 cannot bind to the ERwhen a member of the 75 kDa complex.
1102
Pharmacologic Blockage of Cholesterol Absorption With Ezetimibe Reveals aNovel Homeostatic Network in EnterocytesLuke Engelking, Guosheng Liang, Matthew R. McFarlane, Christina Li
BACKGROUND: Ezetimibe is a widely-used drug that lowers plasma cholesterol by blockingNPC1L1-mediated sterol absorption in small intestine. Enterocyte cholesterol homeostasisis controlled by the aggregated rates of sterol synthesis, efflux, and uptake from plasma andgut lumen. Endogenous cholesterol synthesis and low density lipoprotein (LDL) uptake arecoordinately regulated by transcription factors termed Sterol Regulatory Element-BindingProteins (SREBPs). Liver-X-receptors (LXRs), another family of transcription factors, areactivated by sterols and control other aspects of sterol metabolism, especially cholesterolefflux. How blockade of cholesterol absorption by ezetimibe (EZE) affects intestinal SREBPs,LXRs, and key effector molecules, such as LDL Receptor (LDLR) and HMG-CoA Reductase(HMGR) is unknown. AIM: To study the effect of EZE on regulatory molecules that controlsterol synthesis and LDL uptake in small intestine. METHODS: C57BL/6 mice were fed achow diet with indicated drugs. Liver and small intestine were harvested. Jejunal enterocyteswere isolated, and tissues fractionated for immunoblotting, which were quantified by densito-metry. mRNAs were quantified by qPCR and microarray analysis. RESULTS: Feeding EZEincreased active nuclear SREBP-2 by 8-fold in intestine, leading to increases in mRNAs forHMGR and LDLR by 1.3-fold +/- 0.03 (P<0.01) and 2.0-fold +/- 0.13 (P<0.01), respectively.HMGR and LDLR protein levels increased much more profoundly (24-fold and 6-fold,respectively). Microarray analysis revealed that in jejunum, EZE increased the expression of20 out of 21 SREBP-2 target genes encoding enzymes required for sterol biosynthesis. ThemRNA of a LXR target gene, Inducible Degrader Of the LDLR (IDOL), was reduced by 46%+/- 6% (P<0.01) in EZE-treated intestine. Coadministration of EZE with an LXR agonist(T0901317) abolished EZE-mediated reduction in IDOL mRNA and prevented its inductionof LDLR protein in the intestine. Hepatic LDLR was unaffected in these studies. CONCLU-SION: To maintain sterol homeostasis in the face of EZE-induced blockade of cholesteroluptake, enterocytes boost LDL uptake by increasing LDLR levels and boost sterol synthesisby increasing HMGR and other genes needed for sterol synthesis. These changes in geneexpression are mediated by an increase in active SREBP-2. For HMGR and LDLR, it is likelythat this regulation is mediated by both transcriptional and posttranscriptional mechanisms.The reduced sterol input caused by EZE is associated with a reduction in LXR target genesincluding IDOL. The concerted increase in LDLR mRNA through SREBP-2 and reductionin IDOL leads to a dramatic increase in LDLR protein levels. These studies reveal a previouslyunknown homeostatic network in enterocytes engaged by pharmacologic blockage of choles-terol absorption.
S-199 AGA Abstracts
1103
Dietary Protein Influences Growth Through a Complex Mechanism CouplingProteolysis and Intestinal Peptide Transporter ExpressionStephanie A. Hansen, Aaron Ashley, Debra Titmus, Brian M. Chung
Adequate intestinal nutrient absorption is required for growth and development. Dietaryproteins must be digested to amino acids or peptides that can be absorbed via heteromericamino acid carriers or intestinal peptide transporters. We hypothesized that intestinal peptidetransport impacts growth more than amino acid absorption. Caenorhabditis elegans wasused to assay the roles of the intestinal peptide transporter Opt-2 (homologous to PepT1)and amino acid carrier regulatory protein ATGP-1 (neutral amino acid carrier SLC3A1homologue) on growth. Animals were raised in polymeric (NGM) or elemental (CeHR) dietand harvested daily for 4-days to assay age-related body length. Additionally, RNA wasisolated to determine Opt-2 and ATGP-1 transcript levels and dietary green fluorescentprotein (GFP) was used as a marker of intestinal proteolysis. Data were analyzed for variance(ANOVA) and expressed as mean±SEM. A significant effect of diet on daily body lengthwas found at days 1 and 2 where animals fed a polymeric diet demonstrated 46% increasedgrowth (d1=508±11, d2=1007±22μm, n=36) compared to those fed an elemental diet (CeHR,d1=370±9, d2=649±11, p<0.05). NGM animals demonstrated almost 100% increased Opt-2 mRNA expression compared to CeHR, with no effect on ATGP-1 transcription. NGManimals also demonstrated significantly decreased (80%) intestinal proteolytic activity asmeasured by increased dietary GFP activity along the entire gut length compared to CeHR.Interestingly, animals transferred to NGM after 1 day in CeHR demonstrated an immediateimprovement in growth (d2=822±16, p<0.05) with no increase in Opt-2 or ATGP-1 mRNAcompared to CeHR. These transferred animals also showed a marked decrease in dietaryGFP proteolytic activity mimicking that of those grown solely in NGM. These findingsdemonstrate that intestinal absorption of peptides plays a more influential role over growththan amino acid absorption, however the effect is not simply related to intestinal peptidetransporter levels. Sole reliance on intestinal amino acid absorption through the provisionof elemental diet increases intestinal proteolytic activity with no corresponding increase inamino acid transporter expression or improvement in growth. Animals transferred fromelemental to polymeric diet demonstrated significantly improved growth despite decreasedproteolytic activity despite expressing far fewer intestinal peptide transporters as animalsfed solely polymeric diet. The metabolic cost of complete digestion can apparently be offsetby incomplete digestion to permit more intestinal peptide absorption, potentially releasingenergy for improved growth. In conclusion, the careful design of enteral formulae to efficientlybalance proteolytic activity with intestinal peptide absorption could improve outcomes forshort bowel syndrome or pediatric intestinal failure.
1104
Molecular Aspects of Nutrient Sensing in the Human Gastrointestinal TractMadusha Peiris, Michael A. Atiba, Andy Hubball, David C. Bulmer, Charles H. Knowles,L. Ashley Blackshaw
Background: Nutrient sensing within the gastrointestinal (GI) tract occurs via specific recep-tors that detect a variety of luminal stimuli. Activation of these receptors leads directly tohumoral and neural signals that modulate absorption, motility and satiety. However, detailedknowledge of mechanisms involved in nutrient/receptor interaction and nutrient activationof enteroendocrine cells (EEC) is currently lacking. Aim: To characterise taste receptorexpression profile and co-localisation with specific gut hormones, as well as, elucidate theeffect of nutrient exposure on EEC. Methods: Healthy colon, ileum and antrum sampleswere obtained from surgical resection specimens. Fluorescent immunohistochemistry wasperformed on sections cut from Zamboni's fixed tissue. Nutrient exposure studies werecarried out on freshly dissected mucosa using an Ussing Chamber. Results: Human antralmucosa showed immunoreactivity (IR) for the amino acid sensing receptors T1R1 andcalcium sensing receptor (CaSR), and the long chain fatty acid receptors GPR40 and GPR120.Only CaSR was IR in the ileum and the ascending colon. Gut hormones GLP-1 and PYYwere found throughout the GI tract and co-localisation studies in the ascending colonshowed 68.7 ± 9.2% of GLP-1 positive cells co-localised with PYY. Both GLP-1 and PYYalso co-localised with CaSR (54.5 ± 9.1% and 45.6 ± 8.6%, respectively) in the ascendingcolon. In order to identify nutrients that would activate EEC, we stimulated mucosa ofascending colon with 10 mmolL-1 glutamic (Glu)/aspartic (Asp) acids (which activate T1R1and CaSR) and 50 mmolL-1 phenylalanine (Phe)/tryptophan (Trp) (selective activators ofCaSR). Using pERK as a marker for cell activation, more EEC were activated in Glu/Aspstimulated mucosa compared to buffer controls. However, in mucosa stimulated with Phe/Trp, pERK activation was not observed. Since recombinant CaSR activation is associatedwith pCAMKII activation (Rey et al., Cell Physiol 2010), we localised pCAMKII and foundPhe/Trp stimulation markedly increased pCAMKII expression in EECs compared to buffercontrols. Conclusions:While short-chain fatty acid receptors are foundmainly in the stomach,amino acid receptors, along with associated hormones are expressed until the ascendingcolon. We have also shown that human colonic EEC respond to specific nutrient stimulationvia distinct pathways. Taken together, these results suggest that the colon is an importantsite for nutrient sensing and is therefore a potential target for appetite regulation. Supportedby Wellcome Trust.
1105
Blocking Intestinal Chylomicron Assembly Improves Systemic GlucoseTolerance Through Incretin Mediated Effects on Glucose Absorption and FGF-15 Mediated Alterations of Hepatic Glucose MetabolismHitoshi Matsumoto, Yan Xie, Susan Kennedy, Jianyang Luo, Nicholas O. Davidson
Intestinal microsomal triglyceride transfer protein (Mttp) is required for the assembly andsecretion of chylomicrons. Conditional intestine-specific Mttp-knockout (Mttp-IKO) miceexhibit defective intestinal lipid absorption and reduced serum lipid levels. We now findthat Mttp-IKO mice exhibit improved glucose tolerance, despite no significant differencesin body weight. Oral glucose tolerance testing revealed reduced AUC in Mttp-IKO mice
AG
AA
bst
ract
s