11 Management of symptomatic fibroids: conservative ... · submucous; myolysis by heat, cold...
13
11 Management of symptomatic fibroids: conservative surgical treatment modalities other than abdominal or laparoscopic myomectomy Olav Istre * MD, PhD Consultant in Gynaecology Department of Gynaecology and Obstetrics, Endoscopic Unit, Ullevaal University Hospital, Kirkeveien 166, N-0407 Oslo, Norway Approximately 50% of women of reproductive age have fibroids, and at least 50% of these women have significant symptoms. However, until 15 years ago, the only surgical options availablewere hys- terectomy and myomectomy, and as yet there are no proven effective long-term medical therapies. Fortunately, the past decade has witnessed the emergence of highly sophisticated diagnostic and therapeutic technologies for fibroids. Magnetic resonance imaging and high-resolution ultrasound are non-invasive, high-quality diagnostic procedures. The new treatment modalities include: laparoscopic and vaginal myomectomy; uterine artery embolization (UAE); magnetic-resonance- guided focused ultrasound surgery (MRgFUS); hysteroscopic resection where the fibroids are submucous; myolysis by heat, cold coagulation and laser; laparoscopic uterine artery occlusion; and temporary transvaginal uterine artery occlusion. It is, however, abundantly clear that there is no panacea that suits every woman, nor are all treatment types universally available to all women, even in the developed world. Laparoscopic surgery requires skills that are not common place, and there are limitations on the size and number of fibroids that can be treated by this modality. Much the same applies to vaginal myomectomy. UAE is now widely used in the USA and Western Europe, and has been recommended by the National Institute for Clincial Excellence (NICE) in the UK as an alternative therapy to hysterectomy. However, UAE is still under evaluation in terms of comparison with myomectomy. UAE has a range of complications including premature ovarian failure, chronic vaginal discharge and pelvic sepsis, and may have limited efficacy when the fibroids are large. Although there are a number of reports of successful pregnancy following UAE, the expe- rience is limited and research is required in this area. MRgFUS was approved by the US Food and Drug Administration in 2004, while NICE recommended that the procedure should be used in an audit and research setting. Preliminary data following laparoscopic uterine artery occlusion * Tel.: þ47 22119800; Fax: þ47 22119775. E-mail address: [email protected] 1521-6934/$ - see front matter ª 2008 Elsevier Ltd. All rights reserved. Best Practice & Research Clinical Obstetrics and Gynaecology Vol. 22, No. 4, pp. 735–747, 2008 doi:10.1016/j.bpobgyn.2008.01.010 available online at http://www.sciencedirect.com
Transcript of 11 Management of symptomatic fibroids: conservative ... · submucous; myolysis by heat, cold...

Best Practice & Research Clinical Obstetrics and GynaecologyVol. 22, No. 4, pp. 735–747, 2008
doi:10.1016/j.bpobgyn.2008.01.010
available online at http://www.sciencedirect.com11
Management of symptomatic fibroids:
conservative surgical treatment modalities
other than abdominal or laparoscopic
myomectomy
Olav Istre* MD, PhD
Consultant in Gynaecology
Department of Gynaecology and Obstetrics, Endoscopic Unit, Ullevaal University Hospital, Kirkeveien 166,
N-0407 Oslo, Norway
Approximately 50% of women of reproductive age have fibroids, and at least 50% of these womenhave significant symptoms. However, until 15 years ago, the only surgical options available were hys-terectomy and myomectomy, and as yet there are no proven effective long-term medical therapies.Fortunately, the past decade has witnessed the emergence of highly sophisticated diagnostic andtherapeutic technologies for fibroids. Magnetic resonance imaging and high-resolution ultrasoundare non-invasive, high-quality diagnostic procedures. The new treatment modalities include:laparoscopic and vaginal myomectomy; uterine artery embolization (UAE); magnetic-resonance-guided focused ultrasound surgery (MRgFUS); hysteroscopic resection where the fibroids aresubmucous; myolysis by heat, cold coagulation and laser; laparoscopic uterine artery occlusion;and temporary transvaginal uterine artery occlusion. It is, however, abundantly clear that there isno panacea that suits every woman, nor are all treatment types universally available to all women,even in the developed world. Laparoscopic surgery requires skills that are not common place,and there are limitations on the size and number of fibroids that can be treated by this modality.Much the same applies to vaginal myomectomy. UAE is now widely used in the USA and WesternEurope, and has been recommended by the National Institute for Clincial Excellence (NICE) inthe UK as an alternative therapy to hysterectomy. However, UAE is still under evaluation in termsof comparison with myomectomy. UAE has a range of complications including premature ovarianfailure, chronic vaginal discharge and pelvic sepsis, and may have limited efficacy when the fibroidsare large. Although there are a number of reports of successful pregnancy following UAE, the expe-rience is limited and research is required in this area. MRgFUS was approved by the US Food andDrug Administration in 2004, while NICE recommended that the procedure should be used inan audit and research setting. Preliminary data following laparoscopic uterine artery occlusion
* Tel.: þ47 22119800; Fax: þ47 22119775.
E-mail address: [email protected]
1521-6934/$ - see front matter ª 2008 Elsevier Ltd. All rights reserved.

736 O. Istre
suggest that outcomes are similar to those with UAE, but these data are derived from studies involv-ing relatively small numbers. Temporary uterine artery occlusion is also promising, but has yet to beevaluated robustly. Thus there is no room for complacency; research involving the available treat-ment modalities is urgently needed, while innovations in search of newer and more effective thera-pies must continue. This chapter will review surgical treatment modalities other than hysterectomyand abdominal or laparoscopic myomectomy.
Key words: fibroids; laparoscopy; hysteroscopy; uterine artery; occlusion.
INTRODUCTION
Incidence and biology
Fibroids are the most common benign uterine tumours, with an incidence range of 5.4–77% in women of reproductive age depending on the diagnostic method.1 They increasein incidence towards the end of a woman’s reproductive life. Fibroids are particularlycommon in Black populations, with a nine-fold increase compared with Caucasian pop-ulations.2,3 Macroscopically, they are firm, round or oval-shaped tumours composed ofsmooth muscle bundles in a whorl-like pattern. They often appear singular but are gen-erally multiple, varying in dimensions and locations. Fibroids can occur within the myo-metrial layer (intramural) of the uterus, in the inner aspect of the myometrium(submucosal) and outside the myometrium (subserosal). Occasionally, fibroids can ob-tain a blood supply separate from the myometrium and are then known as ‘parasitic fi-broids’. They can occur at unusual locations such as the uterine cervix or within thelayers of the broad ligament.4 Histologically, they are composed of a mixture of connec-tive tissue and smooth muscle fibres. The aetiology of fibroids is unknown. It is believedthat they are derived from a single cell which has undergone a growth control geneticmutation. Many chromosomal re-arrangements have been noted in fibroid cells, and itis hypothesized that these abnormalities contribute to the loss of normal cellulargrowth.5,6 Fibroids are oestrogen-dependent tumours, which shrink after the meno-pause and also in response to downregulation treatment with gonadotrophin-releasinghormone (GnRH) agonists. There is also evidence that progesterone plays a pivotal rolein the growth of fibroids.7 Although fibroids have receptors for oestrogen and progester-one, it is believed that action of the hormones is mediated via local growth factors such asepithelial growth factor and vascular endothelial growth factor.8 These growth factorsare hormone signals that communicate with fibroid tissues and cause fibroids to increasein size. Oestrogen and progesterone increase their quantity, and hence fibroid growth.The growth factors are present at higher concentrations in fibroids compared with localmyometrium. It is not fully understood what triggers this tumourigenesis, but work in thefield of molecular biology has identified vascular endothelial growth factor-A, upregula-tion of types I and III collagen, transforming growth factor9 and interleukin 810 as impor-tant factors. In addition, there appears to be a genetic predisposition.11 At least one gene,HMGIC, appears to be implicated in a subgroup of fibroids where 12:15 translocationshave been identified.12
Clinical presentation of fibroids
It is estimated that 50% of fibroids are asymptomatic and are an incidental finding atthe time of clinical or ultrasound examination. When fibroids are symptomatic, they

Management of symptomatic fibroids 737
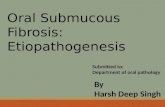
present in a variety of ways including menorrhagia, dysmenorrhoea, pressure symp-toms and subfertility. Wegienka et al studied the relationship between self-reportedbleeding symptoms and the size and location of uterine leiomyomas13 in a randomsample of women aged 35–49 years. Abdominal and transvaginal ultrasound wereused to measure the size and location of leiomyomata, and the women were askedabout symptoms of heavy bleeding in a telephone interview. Reported use of eightor more pads/tampons on the heaviest days of menstrual bleeding increased with leio-myoma size, with a nearly 2.5-fold risk for women with large leiomyomata comparedwith women without leiomyomata (Figure 1). Non-submucosal fibroids were associ-ated with essentially the same increase in heavy bleeding as submuscosal fibroids ofsimilar size. The authors concluded that small leiomyomata were associated with in-creased risk of heavy bleeding, and risk increased with size. Contrary to published ar-ticles, non-submucosal fibroids were associated with heavy bleeding to the sameextent as submucosal fibroids.
Approximately 0.1% of fibroids present as a sarcomatous fibroid; this is a rare butserious smooth muscle malignant tumour.14 Submucous fibroids or intramural fibroidsin close relation to the uterine cavity are found in 40% of patients with heavy and/orprolonged menstrual bleeding.15–18 The therapeutic goal for fibroids and debilitatingmenorrhagia must take into account the needs and desires of the patient in termsof her lifestyle (e.g. days lost from work because of symptoms) and childbearing plans.
Treatment modalities – a historical perspective
The traditional surgical treatments for symptomatic fibroids are laparotomy withhysterectomy or myomectomy, both of which involve considerable morbidity.19–21
Hysterectomy for benign indications has been associated with an increased risk forlower urinary tract sequalae.22 The authors looked at 165 260 women who had un-dergone hysterectomy and a control group of 479 506 individuals who had not hadthis procedure in Sweden. During the 30-year observation period, the rate of urinarystress incontinence surgery per 100 000 person-years was 179 [95% confidence inter-val (CI) 173–186] in the exposed cohort versus 76 (95%CI 73–79) in the unexposedcohort, irrespective of surgical technique. Risk for urinary stress incontinence surgeryvaried slightly with time of follow-up; the highest overall risk was recorded within 5
1.41.6
1.9
1
0.5
1
1.5
2
2.5
3
3.5
No fibroids <2 cm 2-5 cm >5 cmSize of largest fibroid
RR
fo
r g
ush
in
g-typ
e b
leed
in
g
Figure 1. The presence and size of fibroids correlates with the severity of bleeding; therefore, even women
with undiagnosed fibroids are likely to have symptoms. RR, relative risk.

738 O. Istre
years of surgery. The authors concluded that hysterectomy for benign indications, ir-respective of surgical technique, increases the risk for subsequent urinary stress incon-tinence surgery. They also found that hysterectomy increased the risk of havingsubsequent pelvic prolapse surgery at a later stage. Therefore, women should becounselled regarding associated risks related to hysterectomy, and other treatmentoptions should be considered before this major intervention.
Hysterectomy continues to be more costly, in both monetary terms (billions of dol-lars are spent annually) and the more fundamental terms of morbidity and mortality,than the less invasive alternatives of myomectomy, ablation and myolysis.20 Myomec-tomy involves the ‘shelling out’ of fibroids from the myometrium, and in the case ofsubmucosal fibroids, these can be removed surgically via hysteroscopic procedures.23
Although morbidity is reduced with endoscopic surgery, this technique is not widelyavailable and has limitations.
Endometrial ablation is now more common than hysterectomy for heavy menstrualbleeding, and second-generation methods are now more commonly performed thanhysteroscopic endometrial ablation. There is every indication that endometrial abla-tion will continue to increase in practice in England24, and consequently there hasbeen a decline in the number of hysterectomies performed in the UK.
The demand for alternative treatments has increased during the last decade, pushedforward by women resisting hysterectomy and physicians looking for less invasiveprocedures.
The past decade has witnessed highly sophisticated diagnostic and therapeutic tech-nology for fibroids. Currently available tools permit greater management flexibility,which must be tailored to the individual clinical situation. Uterine fibroid embolizationhas become one such alternative procedure, while laparoscopic occlusion of uterinevessels is another alternative.
CONSERVATIVE SURGICAL TREATMENT MODALITIES OTHERTHAN HYSTERECTOMY AND ABDOMINAL OR LAPAROSCOPICMYOMECTOMY
Vaginal myomectomy
In a prospective study published in 1999, Davies et al25 demonstrated the feasibility ofperforming myomectomy via the vaginal route. Out of 35 women with symptomaticfibroids requiring myomectomy, it was completed vaginally in 32 (91.4%) women,none of whom required a hysterectomy. The overall operating time was 78 mins,estimated operative blood loss was 313 mL, and mean postoperative hospital staywas 4 days. Pelvic haematomas developed in four patients, and one colpotomy requiredresuture. Seventy-four percent of the women reported symptom relief at 3-month fol-low-up. Thus, for well-selected patients in good surgical hands, vaginal myomectomy isfeasible and well tolerated. The use of fibroid ‘morcellation’ also renders it feasible toperform the procedure even in cases of large, numerous and intramural fibroids. Unlikewith laparoscopic myomectomy, conventional suture of myoma dead spaces and clo-sure of serosa allows optimal reconstruction of the uterine wall. Randomized trialsare required to establish the place of vaginal myomectomy in comparison with theopen transabdominal procedure, especially with regard to the issue of postoperativeadhesion formation, risk of recurrence and blood loss in comparable cases.

Management of symptomatic fibroids 739
Fibroid myolysis
Ablation techniques reported for the treatment of symptomatic fibroids have includedthe use of temperature to destroy tissue, including myolysis, cryomyolysis and laser.Despite reports of apparently successful outcomes26–28, these techniques have not en-joyed widespread popularity and use. The techniques require placement of probes intothe fibroid, usually via laparoscopy, and the fibroid tissue is destroyed by heat (unipolaror, preferably, bipolar), cold coagulation (cryomyolysis) or laser. It appears that inwomen with symptomatic fibroids and menorrhagia, myolysis can be combined withother procedures such as endometrial ablation or resection, markedly improvingthe success rates of these minimally invasive alternatives to hysterectomy.29 Myomacoagulation combined with endometrial ablation also reduces all subsequent surgeryrates compared with endometrial ablation alone.
Power colour Doppler imaging was performed pre- and postoperatively to deter-mine the effectiveness of cryomyolysis in reducing or eliminating the primary bloodsupply, as well as regression of the myomas (Figure 2). Myomas regressed by up to80%, and the major blood supply to the myomas was eliminated. Another study re-ported that cryomyolysis is able to maintain (or slightly reduce) uterine fibroids atpost-GnRH agonist size, whereas all other uterine tissues return to their pre-treat-ment size.30
In the event of pregnancy occurring after myolysis, intensive surveillance is re-quired. The author would advocate elective caesarean section delivery at term, andcertainly emergency caesarean section if there are any signs of uterine rupture, or ifthe woman goes into labour prior to the planned caesarean section.
Magnetic-resonance-guided focused ultrasound surgery for the treatmentof uterine fibroids
Magnetic-resonance-guided focused ultrasound surgery (MRgFUS) is a non-invasivethermo-ablative technique that uses focused high-energy ultrasound to ablate fibroidtissue. As in conventional diagnostic ultrasound, the ultrasound waves pass throughthe anterior abdominal wall. Significant heating only occurs where the waves convergeat the focus. Magnetic resonance guidance provides continuous imaging of the fibroidand other vital structures such as bowel, bladder and sacral nerves.31
Significant improvement in quality-of-life parameters has been reported in womenundergoing MRgFUS. Given considerable symptoms at enrolment and a large decreasein mean symptom levels, this appears to be a clinically significant result. The volumereduction after treatment is small compared with the mean levels seen after both my-omectomy and uterine artery embolization (UAE). MRgFUS appears to be a safe inter-vention for uterine fibroids.31 None of the MRgFUS-treated patients had urgentsurgical procedures or bowel injuries, which are reported in many early studies ofnew investigational devices for uterine fibroids.32 Furthermore, women who havetreatment with MRgFUS do not appear to develop symptoms similar to the postem-bolization syndrome symptoms associated with UAE.
The mean time of return to work after MRgFUS was approximately 1 day, com-pared with 13 days after UAE and approximately 6 weeks after abdominal myomec-tomy or hysterectomy.33 However, the true place of MRgFUS has yet to beestablished in comparison with the other available treatment modalities by way of ran-domized controlled clinical trials.

Figure 2. Needle placement in fibroid before and after freezing.
740 O. Istre
Hysteroscopic resection
Hysteroscopic resection, in appropriately selected cases, can provide excellent resultsand eliminate the need for major surgery.
The first resectoscopes were unipolar electrodes that required non-electrolytic so-lutions (such as glycine 1.5%, sorbitol or mannitol) to distend the uterine cavity. Thesefluids have the potential to cause non-physiological excessive fluid absorption, causingchanges in serum electrolyte levels leading to hyponatraemic encephalopathy and brainoedema.34,35 General fluid overload may cause pulmonary oedema, especially in el-derly patients or patients with right-sided heart failure, kidney or liver disease. Duringthe last decade, technological improvements have led to the production of new instru-ments using bipolar rather than monopolar energy. The most important benefit of bi-polar resection is the use of saline solution rather than non-ionic distension media, aswell as the reduction of energy spread through the tissue during resection. In addition

Figure 3. Uterine blood supplies.
Management of symptomatic fibroids 741
to the irrigation media used, the main difference between different types of equipmentis the loop size. Theoretically, smaller loops will cut more superficially and removea smaller amount of tissue. Consequently, it may be necessary to resect twice atthe same level to remove the basal layer. The endometrium has a remarkable abilityto regenerate and, in order to achieve an effective result, it is necessary to go beneaththe basalis or destroy the endometrium to a depth of at least 5 mm when consideringthe early to mid-proliferative phase of the cycle.
Versapoint (Gynecare Inc, Menlo Park, CA, USA) bipolar equipment has been avail-able since 1999, and TCRiS (Olympus, Hamburg, Germany) bipolar equipment becameavailable in Europe in 2004. The loop size of TCRiS is smaller than that for monopolarequipment, but larger than the Versapoint loop.
Interference with blood supply to the uterus
Treatments interfering with blood supply to the uterus or fibroids include UAE per-formed by an interventional radiologist, or laparoscopic uterine artery occlusion per-formed by a gynaecologist.36 Before discussing these in detail, it is important todescribe the uterine (and therefore fibroid) blood supply.
Uterine and fibroid vascular supply
The uterus has a very rich blood supply through two extrinsic arterial systems, theuterine and ovarian arteries (Figure 3). Intrinsic uterine arteries consist of ascendinguterine, arcuate, radial and peripherial arteries providing free flow through the uterus.Fibroids receive their blood supply from the intrinsic arteries, primarily from branchesof the arcuate arteries, and the vessels are located in the pseudo capsule around thefibroid. The ipsilateral uterine and ovarian arteries are connected via a communicating(anastomotic) branch. In addition to its primary (uterine artery) and secondary (ovar-ian artery) extrinsic blood supply, the uterus has a vast network of lesser known arterialcollaterals.37 If the blood supply from the right or left uterine artery is occluded, bloodfrom the left or right artery supplies the myometrium by vascular communications

742 O. Istre
through the arcuate arteries. If both uterine arteries are occluded, the ovarian arteriesprovide a blood supply to the myometrium via the anastomoses. In addition to the pri-mary and secondary blood flow, the uterus has a vast network of collateral arterial com-munication from the aorta, external iliac and femoral artery branch.38
To occlude primary blood flow, uterine artery occlusion must be more distal thanthe internal iliac artery, in case occlusion of both internal iliac arteries does not stopantegrade blood flow.39 As such, it does not cause uterine ischaemia, and the Dopplerflow remains unchanged after bilateral internal iliac artery ligation.40 When bilateralinternal iliac occlusion is performed distal to the posterior division, reverse flow inthe middle haemorrhoidal artery reconstitutes antegrade flow in each uterine artery.Under these conditions, the antegrade flow in each uterine artery persists and pulsepressure is damped, resembling a venous system instead of an arterial system; conse-quently, it does not cause uterine ischaemia.
Uterine artery embolization
There is a whole chapter devoted to UAE in this issue; therefore, this section will bebrief and is only included for completeness. There can be no doubting the immensepopularity that UAE has gained in the USA and Western Europe over the past decade.It is performed by highly skilled interventional radiologists, and studies and reports todate indicate significant efficacy in inducing fibroid shrinkage, improving fibroid-relatedsymptoms and improving quality of life. A number of issues are still to be resolved, anddefinitive studies to compare UAE with myomectomy or MRgFUS are awaited. The keyto success in the provision of a UAE service lies in close collaboration between inter-ventional radiologists and gynaecologists. This allows for optimal patient selection andpreparation for the procedure, and for appropriate pre- and post-treatment care ofwomen, since interventional radiologists are not trained in gynaecology, and gynaecol-ogists cannot perform UAE. Some practitioners insist that women should have endo-metrial sampling and/or hysteroscopic imaging prior to UAE, since women withsubmucous fibroids may be better served by hysteroscopic resection than UAE.Others require bacteriological screening and removal of intra-uterine devices priorto UAE, and all these interventions are within the domain of gynaecologists. In routinepractice in the UK, radiologists rarely have inpatient admitting beds, and the womenwould therefore need to be admitted under the care of gynaecologists. When compli-cations occur, such as chronic vaginal discharge, fibroid extrusion through the vagina,premature ovarian failure or severe pelvic sepsis, women will present to gynaecolo-gists. Therefore, the importance of close collaboration between gynaecologists and ra-diologists cannot be overemphasized.
Laparoscopic uterine artery occlusion
Perhaps, in part, because of frustration at not being able to perform UAE, some inno-vative gynaecologists have developed what is effectively an equivalent procedure toUAE; laparoscopic bipolar coagulation of uterine arteries and anastomotic sites ofuterine arteries with ovarian arteries.41,42 The peritoneum overlying the external iliacartery is incised with a T incision between the round ligament and the infundibulo-pel-vic ligament. The iliac vessels are identified, and the retroperitoneal space is developed(Figure 4). The uterine artery is occluded with an endoclip at the level of the internaliliac artery. An identical procedure is performed on the opposite side. The collateral

Figure 4. Uterine artery during laparoscopic occlusion before and after placement of clips.
Management of symptomatic fibroids 743
arteries between ovaries and uterus (in the utero-ovarial ligament) are coagulatedusing bipolar forceps.
In the author’s institution, 46 premenopausal women with symptomatic fibroidswere studied, of whom 24 underwent UAE and 22 underwent laparoscopic occlusionof the uterine arteries.43,44 The picture blood assessment scores were reduced by 50%in both groups after 6 months, and uterine volume was reduced by 35–40% in bothgroups. Interestingly, less post-treatment pain, less nausea and shorter hospital staywere reported in the laparoscopic uterine artery occlusion group compared withthe UAE group. On the downside, more women in the laparoscopic occlusion groupexperienced heavy menstrual bleeding at 6 months compared with the UAE group. Itcan be tentatively concluded that laparoscopic uterine artery occlusion therapy isa promising new method for treating fibroid-related symptoms, with outcomes at leastcomparable to UAE. However, it is recognized that the numbers in this study weresmall, and there is a need for a randomized trial of the two procedures before defin-itive conclusions can be made.

744 O. Istre
Temporary transvaginal occlusion of uterine artery
It is reasonable to assume that UAE and direct surgical uterine artery occlusion causefibroid death due to ischaemia. It is also teleologically sound to suppose that fibroids,due to their more tenuous blood supply, are more sensitive to ischaemia than the my-ometrium. When the blood supply is interrupted, presumably the ischaemia thus cre-ated stimulates recruitment of the collateral circulation, but this may take some time.Thus, while the myometrium is able to ‘hold its breath’, the fibroids are unable to tol-erate the ischaemia. The collateral flow occurs too late for the fibroids to survive,while the myometrium recovers from the temporary ischaemia. This may explainthe recent finding by Banu et al of no serum markers of myometrial ischaemia follow-ing UAE.45 This thinking leads to the supposition that temporary occlusion of the uter-ine arteries could cause fibroid death without affecting the myometrium, which wouldbe subject to the temporary ischaemia but would be able to recover fully.
This hypothesis (effect of temporary uterine artery occlusion) was tested at the au-thor’s institution in 2004 on a 43-year-old woman who had a 16-week-size fibroiduterus and had suffered for several years with menorrhagia, dysmenorrhoea and pelvicpain.46 Her uterine arteries were non-invasively identified through the vagina and oc-cluded for 6 h with a clamp that was guided by audible Doppler ultrasound. Followingremoval of the clamp, blood flow in the uterine arteries returned immediately. Threemonths following treatment, uterine volume had reduced by 49% and dominant fibroidvolume had reduced by 54%.
The technique
The system for temporary uterine artery occlusion consists of a guiding cervical tenac-ulum, a transvaginal vascular clamp with integrated Doppler ultrasound crystals, anda small, battery-powered transceiver that generates an audible Doppler sound (Figure 5).
The clamp slides along the guiding tenaculum to the level of the lateral vaginal fornicesat the 9 o’clock and 3 o’clock cervical positions. When the crystals on the arms of theclamp make contact with the vaginal mucosa, they return audible signals from the right
Figure 5. Transvaginal vascular clamp left in place for 6 h to treat fibroids.

Management of symptomatic fibroids 745
and left uterine arteries. When the clamp advances further along the guiding tenaculum,the clamp displaces the uterine arteries superior to their points of insertion into theuterus. When closed, the clamp occludes the uterine arteries bilaterally by squeezingthem against the lateral borders of the uterus. The clamp remains in situ for 6 h.
It has since been demonstrated that temporary bilateral occlusion of the uterinearteries (for 6 h) is sufficient to treat multiple fibroids in several patients. This ap-proach can also be used in other situations, such as during and after laparoscopic my-omectomy in order to reduce peri- and postoperative blood loss, and as adjuvanttherapy of residual myomas following other treatment modalities.
There is an ongoing multicentre trial of temporary uterine artery occlusion involv-ing centres in Europe and the USA, that intends to recruit 300 patients with symptom-atic fibroids.
Although promising and already of proven efficacy, the current methods of uterineartery occlusion, be it by embolization, permanent laparoscopic occlusion or the tem-porary procedure, have limitations in their potential for widespread use. These tech-niques require complex facilities and considerable skill, and this limits their availabilityto major medical centres with the requisite facilities and expertise.
CONCLUSIONS
At present, there is no surgical panacea for the treatment of uterine fibroids, whichmay present with a variety of symptoms, may be single or multiple, and may occurat different ages. Never has the need for the individualization of treatment beenmore pertinent than in this very common disease. Gone are the days when theonly surgical options were hysterectomy or open myomectomy. Vaginal, laparoscopicand hysteroscopic myomectomy are just three invasive surgical options, while UAE,MRgFUS, and permanent and temporary uterine artery occlusion offer less invasiveapproaches. All of these treatments have been shown to be efficacious, but the degreeof efficacy remains to be fully assessed. The challenge now is for definitive randomizedtrials to establish the true place of these newer treatment modalities, so that womencan be offered therapies that are optimal to their specific clinical presentation.
Practice points
� until 15 years ago, the choice of surgical therapy available to women with symp-tomatic fibroids was confined to hysterectomy and abdominal myomectomy� the armamentarium of therapeutic options for symptomatic uterine fibroids now
includes: laparoscopic and vaginal myomectomy; hysteroscopic resection; ablativetechniques that use heat, laser or cold coagulations; UAE; MRgFUS; laparoscopicuterine artery occlusion; and temporary transvaginal uterine artery occlusion� ablative techniques using heat, laser or cold coagulation have failed to gain in
popularity or widespread use� laparoscopic uterine artery occlusion appears to have similar outcomes to
those seen with UAE, but larger definitive studies are required for comparison� temporary occlusion of the uterine arteries appears to result in symptom im-
provement and fibroid regression, but definitive studies are awaited� the newer treatment modalities tend to require technical expertise or high-
technology, expensive facilities, which limits their availability to large centres

Research agenda
� long-term outcomes of laparoscopic uterine artery occlusion in comparisonwith UAE� randomized controlled trials of conventional surgical treatments (myomectomy)
versus the newer treatment modalities (laparoscopic uterine artery occlusion)� randomized controlled trials of permanent laparoscopic versus temporary
transvaginal uterine artery occlusion in the management of symptomaticfibroids
746 O. Istre
REFERENCES
*1. Lethaby A & Vollenhoven B. Fibroids (uterine myomatosis, leiomyomas). Clin Evid 2002 Jun; (7): 1666–
1678; Review 15366172. Clin Evid 2003 Jun; (9): 2028–2043.
2. Kjerulff KH, Guzinski GM, Langenberg PW et al. Hysterectomy and race. Obstet Gynecol 1993; 82: 757–
764.
*3. Kjerulff KH, Langenberg P, Seidman JD et al. Uterine leiomyomas. Racial differences in severity, symp-
toms and age at diagnosis. J Reprod Med 1996; 41: 483–490.
4. Meniru GI, Wasdahl D, Onuora CO et al. Vaginal leiomyoma co-existing with broad ligament and mul-
tiple uterine leiomyomas. Arch Gynecol Obstet 2001; 265: 105–107.
5. Klotzbucher M, Wasserfall A & Fuhrmann U. Misexpression of wild-type and truncated isoforms of the high-
mobility group I proteins HMGI-C and HMGI(Y) in uterine leiomyomas. Am J Pathol 1999; 155: 1535–1542.
6. Mao X, Barfoot R, Hamoudi RA et al. Allelotype of uterine leiomyomas. Cancer Genet Cytogenet 1999;
114: 89–95.
7. Reinsch RC, Murphy AA, Morales AJ et al. The effects of RU 486 and leuprolide acetate on uterine artery
blood flow in the fibroid uterus: a prospective, randomized study. Am J Obstet Gynecol 1994; 170:1623–1627.
8. Gentry CC, Okolo SO, Fong LF et al. Quantification of vascular endothelial growth factor-A in leiomyo-
mas and adjacent myometrium. Clin Sci (Lond) 2001; 101: 691–695.
9. Stewart EA. Uterine fibroids. Lancet 2001; 357: 293–298.
10. Senturk LM, Sozen I, Gutierrez L et al. Interleukin 8 production and interleukin 8 receptor expression
in human myometrium and leiomyoma. Am J Obstet Gynecol 2001; 184: 559–566.
*11. Luoto R, Kaprio J, Rutanen EM et al. Heritability and risk factors of uterine fibroids - the Finnish Twin
Cohort Study. Maturitas 2000; 37: 15–26.
12. Mine N, Kurose K, Konishi H et al. Fusion of a sequence from HEI10 (14q11) to the HMGIC gene at
12q15 in a uterine leiomyoma. Jpn J Cancer Res 2001; 92: 135–139.
13. Wegienka G, Baird DD, Hertz-Picciotto I et al. Self-reported heavy bleeding associated with uterine
leiomyomata. Obstet Gynecol 2003; 101: 431–437.
*14. Parker WH, Fu YS & Berek JS. Uterine sarcoma in patients operated on for presumed leiomyoma and
rapidly growing leiomyoma. Obstet Gynecol 1994; 83: 414–418.
15. Dodson MG. Use of transvaginal ultrasound in diagnosing the etiology of menometrorrhagia. J Reprod
Med 1994; 39: 362–372.
16. Gimpelson RJ & Whalen TR. Hysteroscopy as gold standard for evaluation of abnormal uterine bleed-
ing. Am J Obstet Gynecol 1995; 173: 1637–1638.
17. Gimpelson RJ. Office hysteroscopy. Clin Obstet Gynecol 1992; 35: 270–281.
18. Fraser IS. Hysteroscopy and laparoscopy in women with menorrhagia. Am J Obstet Gynecol 1990; 162:
1264–1269.
19. Farquhar CM & Steiner CA. Hysterectomy rates in the United States 1990–1997. Obstet Gynecol 2002;
99: 229–234.
*20. Guarnaccia MM & Rein MS. Traditional surgical approaches to uterine fibroids: abdominal myomectomy
and hysterectomy. Clin Obstet Gynecol 2001; 44: 385–400.

Management of symptomatic fibroids 747
21. Dicker RC, Greenspan JR, Strauss LTet al. Complications of abdominal and vaginal hysterectomy among
women of reproductive age in the United States. The Collaborative Review of Sterilization. Am J Obstet
Gynecol 1982; 144: 841–848.
*22. Altman D, Granath F, Cnattingius S et al. Hysterectomy and risk of stress-urinary-incontinence surgery:
nationwide cohort study. Lancet 2007; 370: 1494–1499.
23. Fernandez H, Sefrioui O, Virelizier C et al. Hysteroscopic resection of submucosal myomas in patients
with infertility. Hum Reprod 2001; 16: 1489–1492.
24. Reid PC. Endometrial ablation in England – coming of age? An examination of hospital episode statistics
1989/1990 to 2004/2005. Eur J Obstet Gynecol Reprod Biol 2007 Dec; 135(2): 191–194. [Epub 2006 Oct
12; PMID: 17045729].
25. Davies A, Hart R & Magos AL. The excision of uterine fibroids by vaginal myomectomy: a prospective
study. Fertil Steril 1999; 71: 961–964.
26. Goldfarb HA. Laparoscopic coagulation of myoma (myolysis). Obstet Gynecol Clin North Am 1995; 22:
807–819.
27. Odnusi KO, Rutherford TJ, Olive DL et al. Cryomyolysis in the management of uterine fibroids: tech-
nique and complications. Surg Technol Int 2000; VIII: 173–178.
28. Zreik TG, Rutherford TJ, Palter SF et al. Cryomyolysis, a new procedure for the conservative treat-
ment of uterine fibroids. J Am Assoc Gynecol Laparosc 1998; 5: 33–38.
29. Goldfarb HA. Myoma coagulation (myolysis). Obstet Gynecol Clin North Am 2000; 27: 421–430.
30. Olive DL, Rutherford T, Zreik Tet al. Cryomyolysis in the conservative treatment of uterine fibroids. J
Am Assoc Gynecol Laparosc 1996; 3: S36.
31. Stewart EA, Rabinovici J, Tempany CM et al. Clinical outcomes of focused ultrasound surgery for the
treatment of uterine fibroids. Fertil Steril 2006; 85: 22–29.
32. Gurtcheff SE & Sharp HT. Complications associated with global endometrial ablation: the utility of the
MAUDE Database. Obstet Gynecol 2003; 102: 1278–1282.
33. Pron G, Mocarski E, Bennett J et al. Tolerance, hospital stay, and recovery after uterine artery embolization
for fibroids: the Ontario Uterine Fibroid Embolization Trial. J Vasc Interv Radiol 2003; 14: 1243–1250.
34. Istre O, Jellum E, Skajaa K et al. Changes in amino acids, ammonium, and coagulation factors after trans-
cervical resection of the endometrium with a glycine solution used for uterine irrigation. Am J Obstet
Gynecol 1995; 172: 939–945.
*35. Istre O, Bjoennes J, Naess R et al. Postoperative cerebral oedema after transcervical endometrial re-
section and uterine irrigation with 1.5% glycine. Lancet 1994; 344: 1187–1189.
36. Istre O. Uterine artery occlusion for the treatment of symptomatic fibroids: endoscopic, radiological
and vaginal approach. Minim Invas Ther Allied Technol 2005; 14: 167–174.
*37. Burbank F & Hutchins Jr. FL. Uterine artery occlusion by embolization or surgery for the treatment of
fibroids: a unifying hypothesis – transient uterine ischemia. J Am Assoc Gynecol Laparosc 2000; 7: S1–S49.
38. Chait A, Moltz A & Nelson Jr. JH. The collateral arterial circulation in the pelvis. An angiographic study.
Am J Roentgenol Radium Ther Nucl Med 1968; 102: 392–400.
39. Burchell RC. Physiology of internal iliac artery ligation. J Obstet Gynaecol Br Commonw 1968; 75: 642–651.
40. Chitrit Y, Guillaumin D, Caubel P et al. Absence of flow velocity waveform changes in uterine arteries
after bilateral internal iliac artery ligation. Am J Obstet Gynecol 2000; 182: 727–728.
41. Liu WM. Laparoscopic bipolar coagulation of uterine vessels to treat symptomatic leiomyomas. J Am
Assoc Gynecol Laparosc 2000; 7: 125–129.
42. Liu WM, Ng HT, Wu YC et al. Laparoscopic bipolar coagulation of uterine vessels: a new method for
treating symptomatic fibroids. Fertil Steril 2001; 75: 417–422.
43. Hald K, Langebrekke A, Klow NE et al. Laparoscopic occlusion of uterine vessels for the treatment of
symptomatic fibroids: initial experience and comparison to uterine artery embolization. Am J Obstet Gy-
necol 2004; 190: 37–43.
*44. Hald K, Klow NE, Qvigstad E et al. Laparoscopic occlusion compared with embolization of uterine ves-
sels: a randomized controlled trial. Obstet Gynecol 2007; 109: 20–27.
45. Banu NS, Gaze DC, Bruce H et al. Markers of muscle ischaemia, necrosis and inflammation follwoing
uterine artery embolization in the treatment of symptomatic uterine fibroids. Am J Obstet Gynecol 2007
Mar; 196: 213. e1–e5.
*46. Istre O, Hald K & Qvigstad E. Multiple myomas treated with a temporary, noninvasive, Doppler-di-
rected, transvaginal uterine artery clamp. J Am Assoc Gynecol Laparosc 2004; 11: 273–276.