11 Ergonomics in Osh
9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-1 © E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009 11 ERGONOMICS IN OSH The history of workplace development in the industrial world is characterised by jobs and technologies de- signed to improve processes and productivity. All too often in the past, little or no concern was given to the impact of the job process or technology on workers. As a result, work processes and machines have some- times been unnecessarily dangerous. Another result has been that new technologies have sometimes failed to live up to expectations. This is because, even in the age of high technology, human involvement in work processes is still the key to the most significant and enduring productivity improvements. If a machine or system is uncomfortable, difficult, overly complicated, or dangerous to use, human workers will not be able to derive its full benefit. The proliferation of uncomfortable and dangerous workplace conditions, whether created by job design or unfriendly technologies, is now widely recognised as a harmful to productivity, quality, and worker safety and health. The advent of the science of ergonomics is making the workplace more physically friendly. This, in turn, is making the workplace a safer and healthier place. Safety fact* Pain, discomfort, and loss of function in the back, neck, and extremities are common among working people. Within 27 countries of the European Union, about 25% of work- ers complain of backache and about 23% report muscular pain. Available cost estimates of these disorders put the cost at 0,5% to 2% of GDP. * EASHW (2007) 11.1 T HE SCIENCE OF ERGONOMICS Briefly, ergonomics is defined as the science of fitting the job to the worker (Hammer and Price 2001: 145). Minimising the amount of physical stress in the workplace requires continuous study of the ways in which people and technology interact. The insight learned from this study must then be used to improve the interac- tion. This is a wider de scription of the science of ergonomics. Thus ergonomics is a multidisciplinary science that seeks to conform the workplace and all of its physiological aspects to the worker. Ergonomics involves the following (Goetsch 2002: 147): Using special design and evaluation techniques to make tasks, objects, and environments more compati- ble with human abilities and limitations; Seeking to improve productivity and quality by reducing workplace stressors, reducing the risk of inju- ries and illnesses and increasing efficiency. The field of ergonomics is also called human engineering and human factors. The word “ergonomics” is derived from the Greek language. “Ergon” is Greek for “work”; “nomos” means “laws”. Therefore, in a lit- eral sense, ergonomics means work of laws. In practice, it consists of the scientific principles (laws) applied in minimising the physical stress associated with the workplace (work). The widely accepted benefits of er- gonomics are: Improved health and safety for workers, Higher morale throughout the workplace, Improved quality, Improved productivity, Improved competitiveness, Decreased absenteeism, Fewer workplace injuries/health problems. There are benefits to be derived from ergonomics. There are also problems, both financial and health-related, that can result from giving too little attention to ergonomics. The matter is complicated further because health problems tend to multiply company’s financial problems. Common indicators of the existence of ergonomic problems include the following: Occupational health problems collectively known as musculoskeletal disorders,
-
Upload
muhammad-asim -
Category
Documents
-
view
218 -
download
1
Transcript of 11 Ergonomics in Osh

8/2/2019 11 Ergonomics in Osh
http://slidepdf.com/reader/full/11-ergonomics-in-osh 1/9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-1
© E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009
11 ERGONOMICS IN OSH
The history of workplace development in the industrial world is characterised by jobs and technologies de-
signed to improve processes and productivity. All too often in the past, little or no concern was given to the
impact of the job process or technology on workers. As a result, work processes and machines have some-
times been unnecessarily dangerous. Another result has been that new technologies have sometimes failed to
live up to expectations. This is because, even in the age of high technology, human involvement in work processes is still the key to the most significant and enduring productivity improvements. If a machine or
system is uncomfortable, difficult, overly complicated, or dangerous to use, human workers will not be able
to derive its full benefit.
The proliferation of uncomfortable and dangerous workplace conditions, whether created by job design
or unfriendly technologies, is now widely recognised as a harmful to productivity, quality, and worker safety
and health. The advent of the science of ergonomics is making the workplace more physically friendly. This,
in turn, is making the workplace a safer and healthier place.
Safety fact*
Pain, discomfort, and loss of function in the back, neck, and extremities are commonamong working people. Within 27 countries of the European Union, about 25% of work-
ers complain of backache and about 23% report muscular pain. Available cost estimates
of these disorders put the cost at 0,5% to 2% of GDP.
* EASHW (2007)
11.1 T HE SCIENCE OF ERGONOMICS
Briefly, ergonomics is defined as the science of fitting the job to the worker (Hammer and Price 2001: 145).
Minimising the amount of physical stress in the workplace requires continuous study of the ways in which
people and technology interact. The insight learned from this study must then be used to improve the interac-
tion. This is a wider description of the science of ergonomics. Thus ergonomics is a multidisciplinary science
that seeks to conform the workplace and all of its physiological aspects to the worker. Ergonomics involves
the following (Goetsch 2002: 147):
Using special design and evaluation techniques to make tasks, objects, and environments more compati-
ble with human abilities and limitations;
Seeking to improve productivity and quality by reducing workplace stressors, reducing the risk of inju-
ries and illnesses and increasing efficiency.
The field of ergonomics is also called human engineering and human factors. The word “ergonomics” is
derived from the Greek language. “Ergon” is Greek for “work”; “nomos” means “laws”. Therefore, in a lit-
eral sense, ergonomics means work of laws. In practice, it consists of the scientific principles (laws) applied
in minimising the physical stress associated with the workplace (work). The widely accepted benefits of er-
gonomics are:
Improved health and safety for workers,
Higher morale throughout the workplace,
Improved quality,
Improved productivity,
Improved competitiveness,
Decreased absenteeism,
Fewer workplace injuries/health problems.
There are benefits to be derived from ergonomics. There are also problems, both financial and health-related,
that can result from giving too little attention to ergonomics. The matter is complicated further because
health problems tend to multiply company’s financial problems.
Common indicators of the existence of ergonomic problems include the following:
Occupational health problems collectively known as musculoskeletal disorders,

8/2/2019 11 Ergonomics in Osh
http://slidepdf.com/reader/full/11-ergonomics-in-osh 2/9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-2
© E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009
Trends in accidents and injuries,
Absenteeism,
High turnover rates,
Employee complaints,
Employee generated changes,
Poor quality, and
High incidence of manual material handling.
11.2 D OMAINS OF ERGONOMICS
The International Ergonomics Association (IEA1) divides ergonomics broadly into three domains:
Physical ergonomics. It is concerned with human anatomical, anthropometric, physiological and
biomechanical characteristics as they relate to physical activity (Relevant topics include working
postures, materials handling, repetitive movements, work related musculoskeletal disorders, workplace
layout, safety and health).
Cognitive ergonomis. It is concerned with mental processes, such as perception, memory, reasoning, and
motor response, as they affect interactions among humans and other elements of a system (Relevanttopics include mental workload, decision-making, skilled performance, human-computer interaction,
human reliability, work stress and training as these may relate to human-system design).
Organizational ergonomics. It is concerned with the optimization of sociotechnical systems, including
their organizational structures, policies, and processes(Relevant topics include communication, crew
resource management, work design, design of working times, teamwork, participatory design,
community ergonomics, cooperative work, new work paradigms, virtual organizations, telework, and
quality management).
11.3 M USCULOSKELETAL DISORDERS
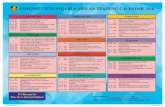
Musculoskeletal disorders cause more than 30% of all occupational injuries and diseases in the United States
(Goetsch 2002: 150). In the European Union, musculoskeletal disorders are the cause of about 50% of work-
related health problems (Figure 11.1) (European Social Statistics 2002: 104).
Musculoskeletal disorder (MSD) is an umbrella term that covers a number of injuries caused by awk-
ward movements repeated frequently over time. Other aggravating factors include poor posture, an improp-
erly designed workstation, poor tool design, and work stress. MSDs occur to the muscles, nerves, and ten-
dons of the hands, arms, shoulders, and neck. Box 11.1 shows a classification of musculoskeletal disorder.
MSDs are also called by names such as occupational overuse disorders, cumulative trauma disorders, and
repetitive stress injuries.
Muscle and tendon disorders
Tendons connect muscles to bones. They can accommodate very little in the way of stretching and are
prone to injury when overused. Overworking a tendon can cause small tears in it. These tears can becomeinflamed and cause intense pain. This condition is known as tenditis. Shoulder tenditis occurs in the muscles
of a shoulder. Forearm tenditis causes pain in fingers, wrist, and muscles in the top of the hand.
Overexertion can cause myofacial muscle damage. The symptom of this disorder is soreness that persists
even when resting. Muscles may burn and be sensitive to the touch. When the muscles become inflamed and
swell, the symptoms are aggravated even further by nerve compression.
1See URL http://www.iea.cc

8/2/2019 11 Ergonomics in Osh
http://slidepdf.com/reader/full/11-ergonomics-in-osh 3/9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-3
© E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009
0 5 10 15 20 25 30 35 40 45 50 55
Percentage
Musculoskeletal disorders, 52%
Stress depression, anxiety, 18%
Lung disorders, 8%
Cardiovascular disorders, 4%
Headaches, visual fatigue, 3%
Hearing disorders, 3%
Infectious diseases, 3%
Skin problems, 3%
Other, 6%
Figure 11.1 Work-related health problems by diagnosis group (the old 15 countries of the European Union, 1999; seri-
ous health problem only, with or without days’ absence from work, %, source European Social Statistics (2002: 108))
Box 11.1: classification of musculoskeletal disorders (MSDs)*
Muscle and tendon disorders
Tendinitis:
– Shoulder tendinitis,
– Bicipital tendinitis,
– Rotator cuff tendinitis,Muscle damage,
Tenosynovitis,
Stenosing tenosynovitis:
– DeQuervain’s disease,
– Trigger finger (flexor tenosynovitis),
Forearm tendinitis:
– Flexor carpi radials tendinitis,
– Extensor tendinitis,
– Flexor tendinitis,
Epicondylitis,
Ganglion cysts.
Cervical Radiculopathy
Tunnel syndromes
Carpal tunnel syndrome,
Radial tunnel syndrome,
Sulcus ulnaris syndrome,
Cubital tunnel syndrome,
Guyons canal syndrome.
Nerve and circulation disorders
Thoracic outlet syndrome,
Raynaud’s disease,
* Goetsch (2002: 175)

8/2/2019 11 Ergonomics in Osh
http://slidepdf.com/reader/full/11-ergonomics-in-osh 4/9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-4
© E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009
Tendons which curve around bones are encased in protective coverings called sheaths. Sheaths contain a
lubricated substance known as synovial fluid. When tendons rub against the sheath too frequently, friction is
produced. The body responds by producing additional synovial fluid. Excess build-up of this fluid can cause
swelling which, in turn, causes pressure on the surrounding nerves. This condition is known as tenosynovitis.
Chronic tenosynovitis is known as stenosing tenosynovitis.
Epicondilitis and ganglion cysts are two muscle and tendon disorders. Epicondilitis affects an elbow.
The common term for this disorder is “tennis elbow”. Ganglion cysts grow on the tendon, tendon sheath, or
synovial lining, typically on the top of the hand, on the nail bed, above the wrist, or on the inside of the wrist.
Cervical radiculopathy
This disorder is most commonly associated with holding a telephone receiver on an upraised shoulder when
typing. This widely practised act can cause compression of the cervical discs in the neck making it painful to
turn the head. Putting the body in an unnatural posture while using the hands is always dangerous.
Tunnel syndromes
Tunnels are conduits for nerves that are formed by ligaments and other soft tissues. Damage to the soft tis-
sues can cause swelling that compresses the nerves that pass through the tunnel. These nerves are the medial,
radial, and ulnar nerves that pass through the tunnel in the forearm and wrist. Pain experienced with tunnel
injuries can be constant and intense. In addition to pain, people with a tunnel injury might experience numb-ness, tingling, and a loss of gripping power.
Nerve and circulation disorders
When friction or inflammation cause swelling, both nerves and arteries can be compressed and so restrict the
flow of blood to muscles. This can cause a disorder known as thoracic outlet syndrome. The symptoms of
this disorder are pain in the entire arm, numbness, coldness, and weakness in the arm, hand, and fingers.
If the blood vessels in the hands are restricted, Raynaud’s disease can result. Symptoms include painful
sensitivity, tingling, numbness, coldness, and paleness in the fingers. It can affect one or both hands. This
disorder is also known as vibration syndrome because it is associated with vibrating tools.
11.4 R ISK FACTORS FOR MSD S
Identification of ergonomic hazards is based on ergonomic risk factors: conditions of the work process,workstations, or work method which contribute to the likelihood of developing MSDs. Not all of these risk
factors will be present in every MSD probe occupational activity, nor is the existence of one of these factors
necessarily sufficient to cause a MSD. Some of the risk factors for MSDs of the upper extremities include the
following:
Repetitive and/or prolonged activities;
Forceful exertions usually with the hands (including pinch grips);
Prolonged static pressures;
Awkward postures of the upper body, including reaching above the shoulders or behind the back and
twisting the wrists and other joints to perform tasks;
Continued physical contact with work surfaces (soft tissue compression);
Excessive vibration from the power tools; Cool temperatures;
Inappropriate or inadequate tool design;
High wrist acceleration;
Fatigue (inadequate recovery time);
Use of gloves.
Risk factors for back disorders include items such as the following:
Bad body mechanics such as continued bending over the waist, continued lifting from below the knees
or above the shoulders, and twisting at the waist, especially while lifting (see Figure 11.2);
Lifting or moving objects of excessive weight or asymmetric size;
Prolonged sitting, especially with poor posture;
Lack of adjustable chairs, footrests, body supports, and work surfaces at workstations;
Poor grips on handles;

8/2/2019 11 Ergonomics in Osh
http://slidepdf.com/reader/full/11-ergonomics-in-osh 5/9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-5
© E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009
Slippery footing.
Safety fact*
Almost all of us will experience back pain at sometime in our life. It is normal and a fact
of life. All epidemiology studies indicate that up to 90% of persons between the ages of
18-55 years (i.e., of working age) will recall an episode of low back pain that interfered
with their ability to function for at least 24 hours at some time. All social and occupa-
tional groups are the same. Approximately 40% of us will experience recurring problems
with our backs.
Most primary care patients who seek treatment for back pain will improve considerably
over the first 4 weeks, but only 30% will be pain free. At one year 70-80% will still re-
port some recurring back symptoms; one third will have intermittent or persistent pain of
at least moderate intensity, and about 15-20% will have a poor functional outcome. The
period prevalence of neck and arm pain in the population is similar to low back pain but
not as frequently disabling.
* Gardiner and Harrington (2005: 42)
Works, operations, or workstations that have multiple risk factors have a higher probability of MSDs.
The combined effect of several risk factors in the development of MSD is sometimes referred to as multiple
causation.
Figure 11.2 Workstation in a pharmaceutical plant: before and after adjustments were made to the workstation(EASHW 2007)
11.5 P REVENTION OF MSD S
MSDs can occur across all types of jobs and work sectors. However, some types of employment groups seem
to be particularly at risk. Specific industries (occupations) with high exposures and groups at high risk in-
clude (EASHW 2008: 17):
Agriculture, forestry and fisheries;
Manufacturing, mining;
Machine operators;
Craft workers, tailors;
Construction;
Wholesale, retail and repairs;
Hotels, restaurants and catering;
Secretaries, typists;
Loaders and unloaders.
Evidence suggests that MSDs affect women more than men largely because of the type of work they do than
because of any gender or other personal factors.Physical causes of MSD include manual handling, loads, poor posture and awkward movements, highly
repetitive movements, forceful hand applications, direct mechanical pressure on body tissues, vibrations, and
cold work environments. Causes in the organisation of work include pace of work, repetitive work, time pat-

8/2/2019 11 Ergonomics in Osh
http://slidepdf.com/reader/full/11-ergonomics-in-osh 6/9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-6
© E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009
terns, payment systems, monotonous work, and also psychosocial work factors. Some types of disorders are
associated with particular tasks or occupations.
To prevent musculoskeletal disorders effectively, the risk factors in the workplace must be identified
and then practical measures taken to prevent or reduce the risks. Eight variables that can influence the
amount of physical stress experienced on the job are as follows (Goetsch 2002: 147):
Sitting versus standing.
Stationary versus movable/mobile.
Large demand for strength/power versus small demand for strength/power.
Good horizontal work area versus bad horizontal work area.
Good vertical work area versus bad vertical work area.
Non-repetitive motion versus repetitive motion.
Low surface versus high surface.
No negative environmental factors versus negative environmental factors.
For the prevention of MSDs, attention needs to be paid to: risk assessment; health surveillance; training;
employee information and consultation; ergonomic work systems (i.e., looking at the effect of the whole
workplace, equipment, work methods, and work organisation, etc. to identify problems and solutions); and
prevention of fatigue. These components of MSD prevention are already recognised in the European practice(EASHW 2008). Solutions of the MSD problem include:
1 Administrative solutions:
A reduction in daily working hours, modification of work, and job rotation may reduce MSDs;
The introduction of additional breaks into repetitive work may be achievable without the loss of produc-
tivity.
2 Engineering solutions:
Technical ergonomic measures can reduce the workload on the back and upper limbs (e.g., in the case of ergonomic hand tools), and thus the occurrence of MSDs, without the loss of productivity;
Technical interventions may also include redesign of physical environment, introduction of lifting and
transfer aids, etc. (Figure 11.3).
3 Behavioural modification:
Training on working methods in manual handling is not effective if it is used as the only measure to pre-
vent low back pain;
Physical training can reduce the recurrence of back pain and neck-shoulder pain. But to be effective, the
training should include vigorous exercise and be repeated at least three times a week.
4 Implementation strategies:
A combination of several kinds of interventions (multidisciplinary approach) – including organisational,
technical and personal measures – is needed to prevent MSDs. Interventions based on single measures
are unlikely to prevent MSDs;
A participative approach that includes the workers in the process of change may have a positive effect
on the success of an intervention.

8/2/2019 11 Ergonomics in Osh
http://slidepdf.com/reader/full/11-ergonomics-in-osh 7/9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-7
© E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009
Figure 11.3 Hand-guided pneumatic balancer and folding trolley used as lifting and transfer aids
11.6 T HE R OLE OF ERGONOMICS IN ACCIDENT PREVENTION
Besides improving the ease with which workers can undertake tasks such as reading dials, good ergonomics
will reduce fatigue, erroneous actions, and wrong decisions (Figure 11.4). Ergonomics has resulted in the
design of better tools, controls for equipment, seats and chairs, and many other items that affect comfort and
safety. Investigation of the accident in the nuclear power plant at Three Mile Island cited two principal
causes: human error and bad ergonomics. Much of the operator error occurred in making decisions and re-
sponses required because of inadequate designs.
Ergonomics
Better workplaces and workprocesses
Minimizing the work-related stress and fatigue
Reduces the possibility of human error andwrong decisions
Contributes to the prevention of workplace
accidents and industrial accidents
Prevents occupational diseases,first of all, muscular-skeletal
disorders (MSDs)
Figure 11.4 The role of ergonomics in prevention of accidents and occupational diseases
Ergonomics attempts to obtain maximum effectiveness in any human-machine operation by integrating
the best capabilities of both. It is concerned with the design of equipment so that it can be operated easily and
rapidly with a minimum of undue effort or strain. A control panel designed for operation by a single personcan overwhelm the worker’s mental and physical capabilities, if an overabundance of data from instruments
must be monitored or its controls operated at one time. Should the instruments on a panel be widely sepa-
rated, an operator would either quickly be exhausted trying to perform an almost impossible task, make er-
rors or ignore some of the instruments, possibly leading to an accident. Much work has been done in the pre-
vious decades in the development of ergonomics. An ergonomic analysis of a very common operation is
given in Table 11.1.

8/2/2019 11 Ergonomics in Osh
http://slidepdf.com/reader/full/11-ergonomics-in-osh 8/9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-8
© E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009
Safety fact*
It often takes a major accident to get the attention of management and the engineering
community regarding the lack of good ergonomics. Such an event occurred on 28 March
1979 at the Three Mile Island nuclear plant in Pennsylvania. Accident investigations
disclosed that this catastrophe was due to a variety of factors:
inadequate training,
a control room poorly designed for people,
questionable emergency operating procedures, and
inadequate provisions for the monitoring of the basic parameters of plant function-
ing.
The event was a turning point for the nuclear power industry because it emphasized the
central importance of ergonomics to safe plant operation. The President’s Commission
on the Accident at Three-Mile Island stated that: “There are many examples in our report
that indicate the lack of attention to the ergonomics in nuclear safety. The control room,
through which the operation of the Three Mile Island plant is carried out, is lacking in
many ways. The control panel is huge, with hundreds of alarms, and there are some key
indicators placed in locations where the operators cannot see them. There is little evi-dence of the impact of modern information technology within the control room … it is
seriously deficient under accident conditions.”
* with modifications from Korwowski (2001: 76)
Table 11.1 Ergonomic analysis of a straight ladder (Hammer and Price 2001:147)
Misuse mode Behavioural factors Design consideration
User sets ladder at angle too near
vertical so that it tips backward as
he ascends or gets near top
Lack of experience, user doesn’t
know proper erection-angle limits;
doesn’t know or realise his bodyneeds to remain close to rungs; not
familiar with centre of gravity fac-
tor
Warning-use instruction label con-
spicuously located (consider use of
alternate orientation of ladder);built-in safe-angle indicator; design
instruction with “pictures”
User sets ladder at shallow angle so
that ladder bends or bounces when
he is near centre of span
Same as above Same as above; over design struc-
turally; minimise bending charac-
teristics
Ladder is too short for situation souser stands on upper rungs with no
hard support
Doesn’t think ahead or recognisepotential hazards; tries to “make
do” – takes a chance
Warning - use instruction
Due to uneven surface, ladder is not
set up properly (e.g., it lists right or
left causing ladder to twist, shift
c.g.(1)
, or introduce structuralstress); feet of ladder slip or pene-trate surface unevenly
Not conscious of support surface
condition; poor judge of verticality;
too lazy or too much in a hurry to
prepare surface; willing to takechance due to inexperience; doesn’tconsider which end of ladder
should be down or up
Self-levelling, broad-footprint foot
design; conspicuous warning; built-
in vertical level indication
… … …
User doesn’t pick ladder up at c.g.(1)
for carrying, causing him to drop it
or dig one end into ground
Lack of experience; doesn’t know
where c.g. is
Warning; mark pick up point
User injuries himself picking up
ladder which is too heavy to carry
Doesn’t know ladder too heavy;
doesn’t think about it before he tries
to pick up; doesn’t pick up properly
Warning – indicate weight
User foot slips off rung or misses
and slips between rungs
Climbs without looking at feet; puts
them where he thinks rungs should
be
Use non-skid surface; use standard
rung spacing and vertical separation
… … …
Metal ladder comes in contact with Unaware of hazard User materials which will not carry

8/2/2019 11 Ergonomics in Osh
http://slidepdf.com/reader/full/11-ergonomics-in-osh 9/9
Occupational Safety Management and Engineering: Ergonomics in OSH 11-9
© E. R. Vaidogas, Lecture Notes on OSH, VGTU, 2009
high-tension electrical wire or com-
ponent; may cause shock or burn as
user touches ladder
electrical current
In backing off roof or high place,
misses rung with foot; may kick
ladder and change its orientation,
causing it to be unsteady
Can’t see where he is putting foot;
unsteady; preoccupied with holding
on to structure; in awkward position
for determining orientation
Maximise ladder width; point out
hazard in operation instruction
(1)
c.g. = centre of gravity
References
EASHW (2007) Prevention of Work-Related MSDs in Practice. Bilbao: European Agency for Safety and Health at
Work.
EASHW (2008) Work-related musculoskeletal disorders: Prevention report, EN 4. Bilbao: European Agency for Safety
and Health at Work.
European social statistics (2002) Accidents at work and work related health problems. Data 1994-2000. European
Communities, 2002. Retrieved October, 2007, from http://epp.eurostat.cec.eu.int/cache/ITY_OFFPUB/KS-BP-02-
002-3A/EN/KS-BP-02-002-3A-EN.PDFGardiner, K.; Harrington, J. M. (Eds.) (2005) Occupational Hygiene. 3rd
ed. Malden: Blackwell Publishing.
Goetsch, D. L. (2002) Occupational Safety and Health for Technologists, Engineers, and Managers. 4th ed. Upper Side
River, New Jersey: Prentice Hall.
Hammer, W. & Proce, D. (2001) Occupational Safety Management and Engineering. 5th Ed., New Jersy: Prentice
Hall.
Korwowski, W. (2001) International Encyclopedia on Ergonomics and Human Factors. Vol. I. London and New York:Taylor and Francis.
Examination questions
1 Define the term “ergonomics”. Explain benefits of ergonomics.
2 What is the main cause of occupational injuries and diseases in the European Union?
3 What is the approximate percentage of MSDs among serious work-related health problems?
4 List five risk factors associated with MSDs.5 Which industries and occupations have an increased risk of MSDs?
6 Explain four possible solutions of the MSD problem. Provide one or two examples of each solution.