10.1016@S0009-89819800164-8
9
Clinica Chimica Acta 279 (1999) 97–105 Indirect reference limits estimated from patients’ results by three mathematical procedures a a , * ´ Montse Ferre-Masfe rre r , Xavier Fuent es- Ard eri u , Rafae l b ˜ ´ Puchal-Ane a ´ ` ` Servei de Bioquımica Clinica, Ciutat Sanitaria i Universitaria de Bellvitge, 08907 L’ Hospitalet de Llobregat , Barcelona, Spain b ` ` Servei de Medicina Nuclear , Ciutat Sanitaria i Universitaria de Bellvitge, 08907 L’ Hospitalet de Llobregat , Barcelona, Spain Received 1 July 1998; received in revised form 28 September 1998; accepted 4 October 1998 Abstract Presently, only a few clinical laboratories produce their own reference values, while the great major ity use refer ence inte rvals reporte d in the liter atur e. An alter nati ve to this unsatisf actor y situation is to estimate indirect reference limits by means of mathematical/statistical procedures from patients ’ results obta ined routine ly in the labo rator y. The proc edure s of Bhat tacha rya (A simple method of resolution of a distribution into Gaussian components. Biometrics 1967;23:115– ¨ 135) Martin et al. (Reference values based on populations accessible to hospitals. In: Grasbeck R, ¨ Alstrom T, editors. Reference Values in Laboratory Medicine. Chischester: Wiley, 1981:233–262) and Kairisto et al. (Generation of reference values for cardiac enzymes from hospital admission laboratory data. Eur J Clin Chem Clin Biochem 1994;32:789–796) were applied to 14 biochemical quantities. In order to verify these procedures, the indirect reference limits obtained from patients’ results were validated by statistical comparison with reference limits estimated from a reference sampl e accor ding to recommend ations of the Inter nati onal Feder ation of Clin ical Chemi stry (IFCC). Calculated indirect reference limits for most quantities studied were reliable, but indirect ref ere nce limits for bil iru bin s and potassiu m ion sub sta nce con cen tra tio ns, ala ni ne ami no- transferase, and aspartate aminotransferase catalyti c concentrations in serum were not suitable. We conclude that indirect reference limits can be obtained from patients’ results by all procedures studied when skewness and kurtosis of mixed distribution are not too large, but other factors also seem to have an influence on the reliability of these procedures. © 1999 Elsevier Science B.V. All rights reserved. Keywords: Reference values; Statistical methods; Patients’ results * Corresponding author. 0009-8 981/ 99/ $ – see front matt er © 1999 Elsevier Science B.V. All rights reserved. PII: S0009-8981(98)00164-8
Transcript of 10.1016@S0009-89819800164-8

8/9/2019 10.1016@S0009-89819800164-8
http://slidepdf.com/reader/full/101016s0009-89819800164-8 1/9

8/9/2019 10.1016@S0009-89819800164-8
http://slidepdf.com/reader/full/101016s0009-89819800164-8 2/9
´ 98 M . Ferre- Masferrer et al. / Clinica Chimica Acta 279 (1999) 97 –105
1. Introduction
Reference values are necessary to compare patients’ results. The InternationalFederation of Clinical Chemistry (IFCC) has published recommendations on the
theory of reference values, the selection of individuals for obtaining referencevalues and the statistical treatment of data in order to estimate reference limits[1]. Several European societies of clinical chemistry have published documents
on this topic, concluding that every clinical laboratory should produce its ownreference values [2]; however, only a few laboratories do so. The selection of
reference individuals is difficult, time-consuming and costly. Furthermore, thecontinued evolution of measurement procedures requires this process to berepeated too often.
Thus, it is not surprising that, in many laboratories, reference values are takenfrom the scientific or commercial literature. However, reference limits included
in text books or in manufacturers’ package inserts should not be used fordiagnostic purposes; these texts usually contain no information about themetrological quality (systematic error and imprecision) with which the reference
values have been produced. In fact, the reliability of reference limits shown in atext book is usually inversely proportional to the between-laboratory coefficientof variation observed in an external quality assessment scheme [3].
An alternative to IFCC recommendations is the estimation of indirect1
reference limits by means of mathematical–statistical procedures applied to thepatients’ results obtained daily in the laboratory, after differentiating them into
‘pathological’ and ‘non-pathological’ (health-related) results [4–12]. The aim of this study is to apply, compare and validate three different procedures for this
alternative [8,10,12].
2. Materials and methods
2.1. Reference individuals
For validation purposes, 120 healthy reference individuals (the reference
sample) were selected according to IFCC recommendations. For practicalreasons, we enrolled only women aged 20–45 years because they were easily
available in our hospital. These women were not pregnant and had no history of either severe diseases or surgery in the previous 3 months. They were advised toavoid physical exercise and cigarette smoking the night before testing and any
alcohol consumption during the prior day. In the last 8 h they had neither eatensolid food nor drank any liquid except water, and they had remained seated for
1
This term has been proposed by Kairisto et al. [11].

8/9/2019 10.1016@S0009-89819800164-8
http://slidepdf.com/reader/full/101016s0009-89819800164-8 3/9
´ M . Ferre- Masferrer et al. / Clinica Chimica Acta 279 (1999) 97 –105 99
15 min before blood sampling.Venous blood was drawn between 8:00 and 10:00h, using evacuated blood-collection tubes with gel (Vacutainer, Becton Dickin-
son, ref. 368510). After 30 min, the tubes were centrifuged at 1200 g for 15 min.Serum samples were tested within 4 h of blood collection.
2.2. Patients
The hospital where the work was conducted has 1000 beds comprising allmain clinical medical specialities, except paediatrics and obstetrics. During
1995, the clinical biochemistry laboratory of the hospital received 119 583requests corresponding to 85 618 different patients, 67 565 of which were
outpatients (79%), and 18 053 (21%) were inpatients.All patients’ results have been stored during 1995 in a laboratory information
system (Omega, Boehringer Mannheim, Barcelona, Spain); among them, results
from 5578 women aged 20–45 years were selected and filed using a personalcomputer connected on-line to the laboratory information system. Only the firstresult for each patient was included (Table 1).
2.3. Measurement procedures
Biochemical quantities selected for this study were:
• Mass concentration of albumin and protein in serum• Substance concentration of bilirubins, calcium(II), creatininium, phosphate,
potassium ion, sodium ion, urate and urea in serum• Catalytic concentration of aspartate aminotransferase, alkaline phosphatase,
alanine aminotransferase and g-glutamyltransferase in serum
All measurements were made with a Hitachi 747 analyser (BoehringerMannheim, Germany); details of the measurement procedures are irrelevant forthis study and have been omitted. A human serum freeze-dried calibrator
(Boehringer Mannheim, Germany, ref. 759350) was used once a day forcalibration. During the study, internal quality control was made using Moni-TrolI-X and Moni-Trol II-X (Dade International Inc. Miami, FL).
3. Procedures for dividing mixed distributions
3.1. Bhattacharya procedure
The Bhattacharya procedure, as modified by Naus et al. [6], assumes that
health-related distributions can be described by a gamma function. Health-
8/9/2019 10.1016@S0009-89819800164-8
http://slidepdf.com/reader/full/101016s0009-89819800164-8 4/9
´ 100 M . Ferre- Masferrer et al. / Clinica Chimica Acta 279 (1999) 97 –105
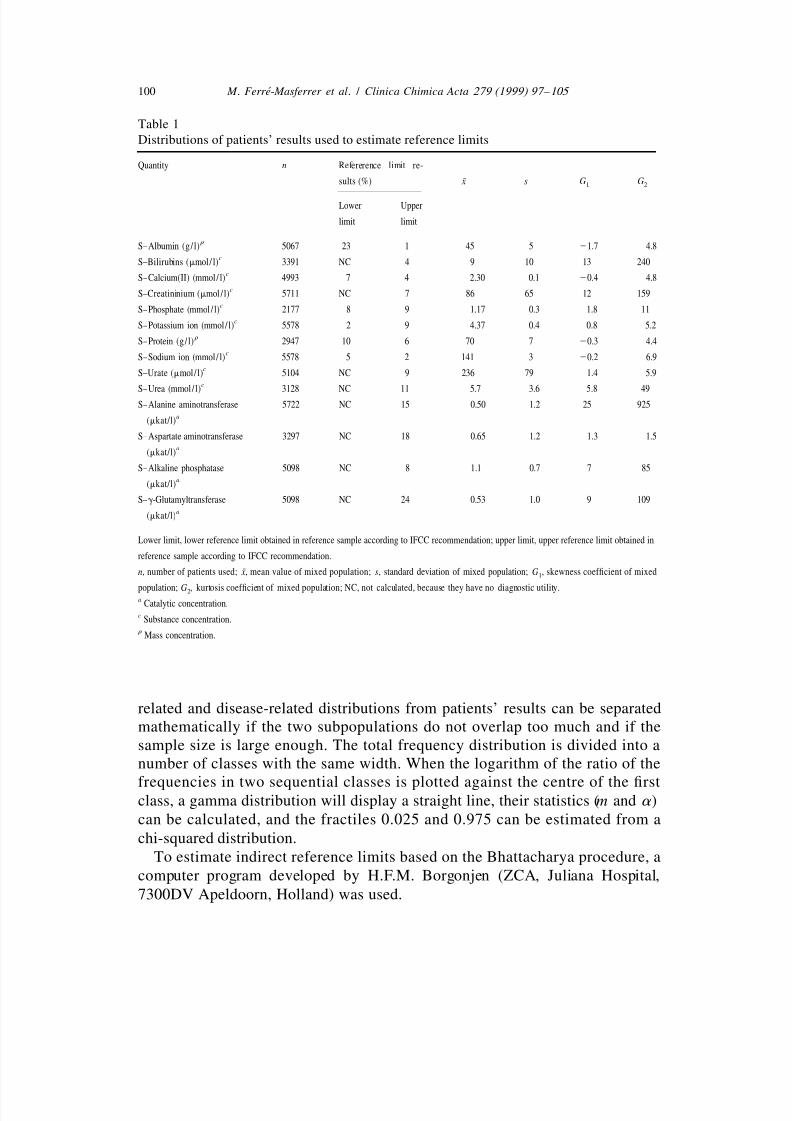
Table 1
Distributions of patients’ results used to estimate reference limits
Quantity n Refererence limit re-
¯ sults (%) x s G G1 2
Lower Upper
limit limit
r S–Albumin (g/ l) 5067 23 1 45 5 21.7 4.8
cS–Bilirubins (mmol/ l) 3391 NC 4 9 10 13 240
cS–Calcium(II) (mmol/ l) 4993 7 4 2.30 0.1 20.4 4.8
cS–Creatininium (mmol / l) 5711 NC 7 86 65 12 159
cS–Phosphate (mmol / l) 2177 8 9 1.17 0.3 1.8 11
cS–Potassium ion (mmol/ l) 5578 2 9 4.37 0.4 0.8 5.2
r S–Protein (g/ l) 2947 10 6 70 7 20.3 4.4
cS–Sodium ion (mmol/ l) 5578 5 2 141 3 20.2 6.9
cS–Urate (mmol/ l) 5104 NC 9 236 79 1.4 5.9
c
S–Urea (mmol/ l) 3128 NC 11 5.7 3.6 5.8 49S–Alanine aminotransferase 5722 NC 15 0.50 1.2 25 925
a(mkat/l)
S–Aspartate aminotransferase 3297 NC 18 0.65 1.2 1.3 1.5a
(mkat/l)
S–Alkaline phosphatase 5098 NC 8 1.1 0.7 7 85a
(mkat/l)
S–g-Glutamyltransferase 5098 NC 24 0.53 1.0 9 109a
(mkat/l)
Lower limit, lower reference limit obtained in reference sample according to IFCC recommendation; upper limit, upper reference limit obtained in
reference sample according to IFCC recommendation.
¯ n, number of patients used; x, mean value of mixed population; s, standard deviation of mixed population; G , skewness coefficient of mixed1
population; G , kurtosis coefficient of mixed population; NC, not calculated, because they have no diagnostic utility.2a
Catalytic concentration.c
Substance concentration.r
Mass concentration.
related and disease-related distributions from patients’ results can be separatedmathematically if the two subpopulations do not overlap too much and if thesample size is large enough. The total frequency distribution is divided into anumber of classes with the same width. When the logarithm of the ratio of the
frequencies in two sequential classes is plotted against the centre of the firstclass, a gamma distribution will display a straight line, their statistics (m and a )can be calculated, and the fractiles 0.025 and 0.975 can be estimated from a
chi-squared distribution.To estimate indirect reference limits based on the Bhattacharya procedure, a
computer program developed by H.F.M. Borgonjen (ZCA, Juliana Hospital,
7300DV Apeldoorn, Holland) was used.

8/9/2019 10.1016@S0009-89819800164-8
http://slidepdf.com/reader/full/101016s0009-89819800164-8 5/9

8/9/2019 10.1016@S0009-89819800164-8
http://slidepdf.com/reader/full/101016s0009-89819800164-8 6/9
´ 102 M . Ferre- Masferrer et al. / Clinica Chimica Acta 279 (1999) 97 –105
statistical test comparing an observed fractile with a theoretical one [15] wasused.
4. Results
The distribution of patients’ results for each quantity has been reported by
some statistics (Table 1). In order to calculate the proportion of pathologicalresults in the mixed distribution, the reference limits obtained following IFCC
recommendations with the reference sample have been used. The results outsidethe reference intervals defined by these reference limits have been considered asdisease-related.
The indirect reference limits estimated from patients’ results using the threeprocedures and the reference limits estimated following to IFCC recommenda-
tions are given in Table 2.In this work, the three procedures studied gave indirect reference limits
similar to those obtained in a reference sample according to IFCC recom-
mendations. However, after validating the indirect reference limits, statisticaldifferences have been found for some quantities.
As regards serum concentration of bilirubins, creatinium, urate and urea, we
have only validated the upper indirect reference limit, because this is the onlyone having diagnostic utility in our hospital.
The upper indirect reference limits for substance concentration of bilirubins
and catalytic concentration of alanine aminotransferase in serum obtained by thethree procedures are significantly different (P , 0.05) from fractile 0.975 of the
reference distribution.The upper indirect reference limit for catalytic concentration of aspartate
aminotransferase in serum obtained using the Kairisto et al. procedure [11] is
statistically different (P , 0.05) from fractile 0.975 of the reference distribution.The lower indirect reference limit for substance concentration of potassium
ion in serum obtained using Martin et al. [10] and Kairisto et al. procedures [11]
is statistically different (P , 0.05) from fractile 0.025 of the reference dis-tribution.
5. Discussion
The establishment of reference values is difficult, time-consuming and costly;
consequently, it is not surprising that only a few laboratories do it. Probably, oneof the main problems is to obtain a sufficient number of adequate samples forobtaining reference values, particularly for quantities that are not distributed
according to Laplace–Gauss’ law and for which partitioning criteria should be

8/9/2019 10.1016@S0009-89819800164-8
http://slidepdf.com/reader/full/101016s0009-89819800164-8 7/9
´ M . Ferre- Masferrer et al. / Clinica Chimica Acta 279 (1999) 97 –105 103
Table 2
Indirect reference limits obtained from patients’ results using Bhattacharya [4], Martin et al. [10],
and Kairisto et al. [11] procedures
Quantity (units) Procedure
a
Bhattacharya Martin at al. Kainsto at al. IFCC [1]
[4] [10] [11]
r
S–Albumin (g/ l) 41–52 39–51 39–52 41–53c
S–Bilirubins (mmol/ l) 3–14* 3–16* 2–13* 4–18c
S–Calcium(II) (mmol / l) 2.13–2.48 2.12–2.48 2.11–2.47 2.15–2.46c
S–Creatininium (mmol/ l) 64–96 62–93 62–95 65–96c
S–Phosphate (mmol/ l) 0.84–1.55 0.82–1.52 0.84–1.56 0.87–1.45c
S–Potassium ion (mmol/ l) 3.74–4.95 3.78*–5.04 3.80*–5.05 3.66–4.89r
S–Protein (g / l) 63–81 63–81 61–80 64–79c
S–Sodium ion (mmol/ l) 138–146 138–146 136–146 138–146c
S–Urate (mmol / l) 129–366 120–345 120–337 134–325c
S–Urea (mmol / l) 2.9–8.2 2.6–7.8 2.3–7.5 3.0–7.3S–Alanine aminotransferase ,0.47* ,0.52* ,0.51* ,0.60
b
(mkat/l)
S–Aspartate aminotransferase ,0.45 ,0.49 ,0.41* ,0.46b
(mkat/l)
S–Alkaline phosphatase ,1.5 ,1.7 ,1.5 ,1.4b
(mkat/l)
S–g-Glutamyltransferase ,0.41 ,0.48 ,0.44 ,0.43b
(mkat/l)
a
Reference limits obtained from reference sample were produced according to the FCC recommendations.b
Catalytic concentration.c
Substance concentration.r
Mass concentration.* Significantly different (P#0.05) than fractile 0.975 of the reference distribution.
used. For this reason, there are three alternatives to solve this problem: (i)
adoption of reference limits produced by other laboratories after verifying their
transferability [1], (ii) the multicentric production of reference values [16], and
(iii) the use of patients’ results to estimate reference limits by direct or indirect
methods [4–14].In any case, the ideal situation is to have true interchangeability of reference
limits, and consequently, common interpretation of results coming from different
laboratories.Among these alternatives, the estimation of reference limits from patients’
results has many advantages:
• It is the easiest procedure
• It is the cheapest procedure
• Reference limits are derived from values obtained with the same pre-

8/9/2019 10.1016@S0009-89819800164-8
http://slidepdf.com/reader/full/101016s0009-89819800164-8 8/9
´ 104 M . Ferre- Masferrer et al. / Clinica Chimica Acta 279 (1999) 97 –105
metrological conditions as the patients’ results which will be compared withreference limits
• Patients’ results can be easily selected according to biological variationfactors when it is necessary.
The upper indirect reference limits for substance concentration of bilirubins
and catalytic concentration of alanine aminotransferase in serum obtained by thethree procedures have not been used for diagnostic purposes. This is probably
due to the shapes of the mixed distributions; these distributions have coefficientsof skewness and kurtosis greater than the other quantities studied (Table 1). Theshape of mixed distributions seems to have an influence on the reliability of
these procedures. We observed that the three procedures are reliable whendistribution of patients’ result has a coefficient of skewness of 12 or lower and a
coefficient of kurtosis of 159 or lower, but they are not reliable when these
values are 13 and 240 or higher, respectively.The upper indirect reference limit for catalytic concentration of aspartate
aminotransferase in serum obtained by the Kairisto et al. procedure [11] and thelower indirect reference limit for substance concentration of potassium ion inserum obtained by the Martin et al. [10] and Kairisto et al. [11] procedures are
not valid, but we do not have an explanation for these differences.We conclude that the three procedures used to estimate reference limits from
patients’ results are good enough for the following quantities: substanceconcentrations of calcium(II), creatininium, phosphate, sodium ion, urate andurea in serum; mass concentration of albumin and protein in serum; and catalytic
concentration of alkaline phosphatase and g-glutamyltransferase in serum.
The most effective procedure studied is the one proposed by Bhattacharya [4]modified for gamma distributions.
References
[1] International Federation of clinical chemistry. Approved Recommendation on the Theory of
Reference Values. Part I to VI. J Clin Chem Clin Biochem 1987;25:337–342; J Clin Chem
Clin Biochem 1987;25:639–644; J Clin Chem Clin Biochem 1987;25:645–656; J Clin Chem
Clin Biochem 1987;25:657–662; J Clin Chem Clin Biochem 1988;26:593–598; J Clin Chem
Clin Biochem 1991;29:531–535.
˜´ ´ ´ ´[2] Queralto Compano J.M., dir. Teorıa de los valores de referencia. Documentos de la Comisionde Valores de Referencia. Barcelona: SEQC, 1993.
´[3] Fuentes-Arderiu X, Ferre-Masferrer M. On the reliability of published reference limits. Eur J
Clin Chem Clin Biochem 1996;34:143.
[4] Bhattacharya CG. A simple method of resolution of a distribution into Gaussian components.
Biometrics 1967;23:115–35.
[5] Naus AJ, Borst A, Kuppens PS. The use of patient data for the calculation of reference
values for some haematological parameters. J Clin Chem Clin Biochem 1980;18:621–5.

8/9/2019 10.1016@S0009-89819800164-8
http://slidepdf.com/reader/full/101016s0009-89819800164-8 9/9
´ M . Ferre- Masferrer et al. / Clinica Chimica Acta 279 (1999) 97 –105 105
[6] Naus AJ, Borst A, Kuppens PS. Determination of n-dimensional reference ellipsoids using
patient data. J Clin Chem Clin Biochem 1982;20:75–80.
[7] Baadenhuijsen H, Smit JC. Indirect estimation of clinical chemical reference intervals from
total hospital patient data: application of a modified Bhattacharya procedure. J Clin Chem
Clin Biochem 1985;23:829–39.
[8] Hemel JB. Critical discussion on a method for derivation of reference limits in clinical
chemistry from a patient population. J Autom Chem 1985;7:20–30.
[9] Oosterhuis WP, Modderman TA, Pronk C. Reference values: Bhattacharya or the method
proposed by the IFCC?. Ann Clin Biochem 1990;27:359–65.
[10] Martin HF, Hologgitas JV, Driscoll J, Fanger H, Gudzinowicz BJ, Reference values based on
¨ ¨populations accessible to hospitals. In: Grasbeck R, Alstrom T, editors. Reference Values in
Laboratory Medicine. Chischester: Wiley, 1981:233–262.
¨ ¨ ¨[11] Kairisto V, Hanninen KP, Leino A, Pulkki K, Peltola O, Nanto V, Voipio-Pulkki LM, Iriala K.
Generation of reference values for cardiac enzymes from hospital admission laboratory data.
Eur J Clin Chem Clin Biochem 1994;32:789–96.
[12] Kairisto V, Poola A. Software for illustrative presentation of basic clinical characteristics of
laboratory tests: GraphROC for Windows. Scand J Clin Lab Invest 1995;55(222):43–60.
[13] Pryce SD. Level of haemoglobin in whole blood and red blood-cells, and proposedconvention for defining normality. Lancet 1960;2:333–6.
[14] Hoffmann RG. Statistics in the practice of medicine. J Am Med Assoc 1963;185:864–73.
[15] Conover WJ, Practical Non-parametric Statistics. New York: Wiley, 1980:105–111.¯´ ¨ ´[16] Ferre-Masferrer M, Fuentes-Arderiu X, Alvarez-Funes V, Guell-Miro R, Castineiras-Lacam-
bra MJ. Multicentric Reference Values, Shared Reference Limits. Eur J Clin Chem Clin
Biochem 1997;35:715–8.