
Efficacy of glucocorticoids for the treatment of macrolide ...

The Efficacy of Brief Family Based Treatment inChanging Family Members' Attitudes Toward People withAddiction and Attitudes Toward a Relative with Addiction
Item Type text; Electronic Dissertation
Authors Kolodny, Teresa Lynn
Publisher The University of Arizona.
Rights Copyright © is held by the author. Digital access to this materialis made possible by the University Libraries, University of Arizona.Further transmission, reproduction or presentation (such aspublic display or performance) of protected items is prohibitedexcept with permission of the author.
Download date 26/05/2018 17:26:18
Link to Item http://hdl.handle.net/10150/193708

1
THE EFFICACY OF BRIEF FAMILY-BASED TREATMENT IN CHANGING
FAMILY MEMBERS’ ATTITUDES TOWARD PEOPLE WITH ADDICTION AND
ATTITUDES TOWARD A RELATIVE WITH ADDICTION
by
Teresa Lynn Kolodny __________________
A Dissertation Submitted to the Faculty of the
DEPARTMENT OF SPECIAL EDUCATION, REHABILITATION, AND SCHOOL
PSYCHOLOGY
In Partial Fulfillment of the Requirements For the Degree of
DOCTOR OF PHILOSOPHY
WITH A MAJOR IN REHABILITATION
In the Graduate College
THE UNIVERSITY OF ARIZONA
2009

2
THE UNIVERSITY OF ARIZONA GRADUATE COLLEGE
As members of the Dissertation Committee, we certify that we have read the dissertation
prepared by Teresa Lynn Kolodny entitled The Efficacy of Brief family-based Treatment
in Changing Family Members’ Attitudes toward People with Addiction and Attitudes
toward a Relative with Addiction and recommend that it be accepted as fulfilling the
dissertation requirements for the Degree of Doctor of Philosophy.
_________________________________________________Date: October 21, 2009 Dr. Charlene Kampfe, Ph. D. __________________________________________________Date: October 21, 2009 Dr. Amos Sales, Ed. D. __________________________________________________Date: October 21, 2009 Dr. Chih-Chin Chou, Ph. D.
Final approval and acceptance of this dissertation is contingent upon the candidate’s submission of the final copies of the dissertation to the Graduate College. I hereby certify that I have read this dissertation prepared under my direction and recommend that it be accepted as fulfilling the dissertation requirement. ____________________________________________________Date: October 21, 2009 Dissertation Director: Dr. Charlene Kampfe, Ph.D.

3
STATEMENT BY THE AUTHOR
This dissertation has been submitted in partial fulfillment of the requirements for an advanced degree at the University of Arizona and is deposited in the University Library to be made available to borrowers under rules of the Library. Brief quotations from this dissertation are allowable without special permission, provided that accurate acknowledgement of source is made. Requests for permission for extended quotation from this manuscript in whole or in part may be granted by the head of the major department of the Dean of the Graduate College. In other instances, however, permission must be obtained from the author.
SIGNED: Teresa L Kolodny

4
ACKNOWLEDGEMENTS Sincere acknowledgement is made to my dissertation committee members, Dr.
Charlene Kampfe, Ph.D., the Dissertation Chair, Dr. Amos Sales, Ed.D., and Dr. Chin
Chou, Ph.D. To them I owe a debt of gratitude for their time, patience, and
encouragement. I especially want to thank Dr. Kampfe for her strength, compassion, and
attention to detail which helped me to overcome many obstacles during this study.
Next I would like to thank Dr. Richard Morris, Ph.D. for assisting me in securing
a study site at Pima County Juvenile Court Center (PCJCC). Heartfelt appreciation goes
to the Court Director, staff, and family members at PCJCC, most notably, Dr. Beverly
Tobiason, Dr. Alvin Lewis, Paula Burns, and Pat Canterbury. I am also very appreciative
of the KARE Center staff, participants, and Director, Laurie Melrood. To all of them, I
extend my utmost appreciation for partnering with me and sharing their wisdom during
this research study.
Also, my statistician, Mark Borgstrom and my fellow doctoral students, Dr. Phil
Johnson, Cynthia Dowdall, and Dr. Lisa Degiorgio, my dear friends, Dr. Martha
Underwood and Wendy Sokol, and numerous barn buddies, Chris, Rita, Jean, and Vickie
Jo for their emotional support. Without their enthusiasm, humor, and excitement for my
study, completion would not have been possible.
Lastly, I most lovingly acknowledge my parents, Don and Rose Purcell, and dear
family members, Aaron and Amber Kolodny, Mary Kolodny, Dr. Carter Kolodny and

5
Kathleen Kolodny. Their ever-present support and prayers were a life-line to me during
my graduate studies at the University of Arizona.

6
DEDICATION
I dedicate this dissertation first, to my Savior, Jesus Christ. With Him, all things
are possible (even a Ph.D). Next, to my father-in-law, Dr. Stanley Kolodny, Sr., whose
belief in my abilities inspired me to follow my dreams to completion. Also, to my dear
husband, Stanley Kolodny, Jr., who listened patiently, held me when I cried, and always
said “you can do this.” And finally, to all the families who live with addiction, thank you
for sharing your story.

7
TABLE OF CONTENTS
LIST OF TABLES .............................................................................................................10
LIST OF ILLUSTRATIONS .............................................................................................11
ABSTRACT .......................................................................................................................12
CHAPTER ONE: INTRODUCTION ................................................................................14
Addiction................................................................................................…..…. …14
Addiction as a Disease ...........................................................................................15
Attitudes …………………………………………………………………………16
Brief Family-based Treatment ...............................................................................22
Statement of the Problem .......................................................................................24
Significance of the Study .......................................................................................24
Research Questions ................................................................................................25
Definition of Terms................................................................................................27
CHAPTER TWO: REVIEW OF THE LITERATURE .....................................................31
Addiction Statistics and Need for Treatment .........................................................31
Family Members’ Attitudes toward Addiction ......................................................34
Brief Family-based Treatment Approaches ...........................................................35
Summary ................................................................................................................51
CHAPTER THREE: METHOD ........................................................................................54
Participants and Settings ........................................................................................54
Procedure ...............................................................................................................59
Research Design.....................................................................................................61

8
Instrument ..............................................................................................................63
Piloted Study of the Attitudes Measurement: Brief Scales ....................................66
Analysis..................................................................................................................67
CHAPTER FOUR: FINDINGS .........................................................................................69
Results ....................................................................................................................70
Responsibility scale ...............................................................................................71
Negative scale ........................................................................................................73
Positive scale ..........................................................................................................76
Deservingness scale ...............................................................................................79
Entitlement scale ....................................................................................................82
Demographic Characteristics…………………………………………………….86
Summary of Findings .............................................................................................88
CHAPTER FIVE: DISCUSSION ......................................................................................90
Brief Review of the Methodology .........................................................................90
Discussion of Findings ...........................................................................................91
Limitations .............................................................................................................97
Conclusions and Recommendations ......................................................................99
APPENDIX A-1. RECRUITMENT FLYER FOR PCJCC .............................................101
APPENDIX A-1a. SUBJECT INFORMED CONSENT FORM FOR PCJCC ...............102
APPENDIX A-2. RECRUITMENT FLYER FOR KARE ..............................................103
APPENDIX A-2a. SUBJECT INFORMED CONSENT FORM FOR KARE................104
APPENDIX B-1. ATTITUDES MEASUREMENT: BRIEF SCALES (ORIGINAL) ...105

9
APPENDIX B-2. ATTITUDES MEASUREMENT: BRIEF SCALES (REVISED) ....106
APPENDIX B-3. ATTITUDES MEASUREMENT: BRIEF SCALES (REVISED) .....107
APPENDIX B-4. DEMOGRAPHIC QUESTIONNAIRE ..............................................108
APPENDIX C. ATTITUDES MEASUREMENT: BRIEF SCALES (SCORING) .......109
APPENDIX D. MAC TREATMENT READINESS PROGRAM (DESCRIPTION) ....111
REFERENCES ................................................................................................................113

10
LIST OF TABLES
Table 1: Analysis of Variance for the Responsibility Scale ..............................................71
Table 2: Analysis of Variance for the Negative Scale .......................................................74
Table 3: Analysis of Variance for the Positive Scale ........................................................77
Table 4: Analysis of Variance for the Deservingness Scale ..............................................80
Table 5: Analysis of Variance for the Entitlement Scale ...................................................83
Table 6: Demographic Characteristics……………………………………………………86

11
LIST OF ILLUSTRATIONS
Figure 1. Means for the Responsibility Scale ....................................................................73
Figure 2. Means for the Negative Scale .............................................................................76
Figure 3. Means for the Positive Scale ..............................................................................79
Figure 4. Means for the Deservingness Scale ....................................................................82
Figure 5. Means for the Entitlement Scale.........................................................................85

12
ABSTRACT
The family has been described as the center or heart of societal relationships, with
each family member playing an integral part in that relationship (Garrett & Landau, 2007;
Jay & Jay, 2000). Therefore, when a family member is affected by a disease such as
addiction, his or her predicament typically impacts other members of the family. When
this occurs, family members may seek therapy to provide solutions. One technique that
has been found to be beneficial to the entire family, by providing education about the
impact of addiction, is brief family-based treatment (FBT) (Jay & Jay; Johnson, 1998).
Brief family-based treatment teaches that as family members work together, they have a
much better chance of changing their own perceptions/attitudes about addiction, thereby
changing the outcome for the relative with addiction.
This quasi-experimental study explored the efficacy of brief family-based
treatment in changing family members’ attitudes toward people in general with addiction
and in changing family members’ attitudes toward a specific relative with addiction. The
participants were comprised of a convenience sample of two groups (i.e., treatment and
control). Participants in the treatment group (n = 19) received a brief family-based
treatment session and participants in the control group (n = 22) did not receive a brief
family-based treatment session.
This study had three phases: (a) recruiting, selecting, and determining eligibility
of family members from both groups to participate in the study, (b) applying the
intervention (i.e., brief family-based treatment) to the treatment group and collecting
data, and (c) analyzing the results. Two research questions were posed: (a) is there a

13
change in family members’ attitudes toward people in general with addiction from pre-
family based treatment to post-family based treatment and (b) is there a change in family
members’ attitudes toward a specific relative with addiction from pre- family-based
treatment to post-family-based treatment? Results of this study indicated that brief
family-based treatment resulted in no significant finding with regard to changing family
members’ attitudes toward people in general with addiction and in changing attitudes
toward a specific relative with addiction. Despite these results, however, some
significance was noted in other areas. Therefore, more research into all aspects of brief
family-based treatment should be explored so that interventions can be studied for more
effectiveness.

14
CHAPTER ONE
INTRODUCTION
Addiction
In 2006, approximately 30.5 million Americans aged 12 and older reported using
some type of illicit drug and an additional 54 million engaged in “heavy” drinking at least
one day out of the week, or “binge use,” within a 30 day period (SAMHSA, 2008). The
societal cost of addiction is over $300 billion and continues to rise each year. This has
resulted in one of the most severe health concerns facing America, today (SAMHSA).
Clearly, as the impact of addiction on society and families rises, so does the need to
define and better understand addiction.
Over the past few decades, the definition of addiction has been unclear, leaving
counselors and lay people with a variety of terms that are representative of the person
with an addiction (Gutman, 2006; Jay & Jay, 2000; Mumm, Olsen, & Allen, 1998; Sales,
2000; Summerall & Leshner, 2003). For example, addiction has been described as a
disease, a state of physiological or psychological dependence on an addictive substance,
where prolonged use may result in a chronic condition in which the symptoms of the
disease are likely to result in severe and damaging consequences to the person with
addiction or to family members of the person with addiction (Jay & Jay;
Gutman; Sulek, Korczak-DZiurdzik, Korbel-Pawlaws, Lyznicka, & Czarneck, 2006;
Summerall & Leshner, 2003; Wilson & Wilson, 1992). The Diagnostic and Statistical
Manual of Mental Disorders (DSM-IV TR, 2000) describes addiction as a physical

15
dependence on and abuse of drugs and other miscellaneous substances. According to
Sales (2000), “addiction, alcoholism, alcohol abuse, and chemical dependency” represent
and share many of the same characteristics (p. 2). As such, the terms alcohol addiction,
alcoholism, alcohol dependence, drug addiction, and drug dependence generally suggest
some form of addiction. In a recent study completed in 2008 by the National Institute on
Drug Abuse (NIDA), researchers determined that addiction is a complicated disease that
can encompass essentially every aspect of a person’s life.
Addiction as a Disease
As a disease, addiction has typical signs and symptoms that may progress in a
certain manner, with addiction becoming the primary concern and not the result of some
other condition (Wilson & Wilson, 1992). Jellnick defined addiction in the 1950’s as a
disease, and proffered the theory that a person with addiction has a physiological
deficiency that makes him or her incapable of tolerating the addictive substance (Smith &
Miller, 2000). Furthermore, as a primary disease, rather than being a symptom of some
other disorder or dysfunction, addiction often may be the cause or may, at the very least
exacerbate, other conditions whether they are physical or emotional (Johnson, 1998). For
example, a physician is unable to treat an addict with a diseased liver until the addict is
willing to submit to treatment for his or her addiction (Johnson). Addiction, like heart
disease, cancers, and type II diabetes, is a real and complex disease (NIDA, 2008). Once
a person is addicted, his or her behavior becomes a product of the disease and, as such,
the addiction requires that the person defer to it (i.e., the addiction) rather than to his or

16
her natural behavioral instincts which may tend to be less self-indulgent and more
manageable (Wilson & Wilson). A key principle of the disease model, therefore, is the
capacity to move addiction out of the realm of being a character flaw and moral issue to
that of a treatable disease (Washton & Zweben, 2006).
Attitudes
In many instances, addiction has been perceived by professionals as a moral
problem with public opinion alternating between hostility, aversion, and unconcern
toward people with addiction, on the one hand, to sympathy and consideration for their
well-being on the other hand,(Gutman, 2006). Beck, Matschinger, and Angermeyer
(2003) assert that negative perceptions and attitudes such as these have led the public to
conclude that a person with addiction is not entitled to the same type of treatment and
intervention as a person with other similar conditions.
To understand how these negative attitudes affect the outcomes of addiction, one
must first have a good definition of attitudes. Attitudes have been defined as emotionally
charged ideas that prompt a set of actions toward a certain class of individuals (Triandis,
1971). They are associated with a tendency to behave in a predictable and guarded way
toward, or in the presence of, members of a particular group (Hunt & Hunt, 2004). With
regard to attitudes, there are three common assumptions: (a) they include some kind of
judgment of someone; (b) they can be articulated through language; and (c) they are
associated with actions toward another (Eiser, 1986; McCarthy & Light, 2005). Other
terms used to describe attitudes include self-beliefs, beliefs, judgments, perceptions,
thoughts, and stigmas (Canale & Munn, 2005; Jay & Jay, 2000; Johnson, 1998). In this
17
same way, family members’ attitudes toward addiction are often characterized by
thoughts of judgment, misgiving, uncertainty, and guardedness (Wilson & Wilson,1992).
For the purpose of this study, the term attitude will represent all of the above beliefs and
actions and will focus on family member’s attitudes or perceptions toward addiction.
Family members’ beliefs about addiction and their feelings toward a specific
relative with addiction often play an essential part in the psychological aspect of the
recovery process of the relative with the addiction (Jay & Jay, 2000). For example,
family members who hold a relative with addiction responsible for his or her addiction,
or who have a negative attitude toward a relative with addiction, may cause the person to
continue to use as a way of coping with his or her situation. Therefore, if recovery is to
occur, it is imperative for family members to become aware of how their thoughts and
feelings impact the relative with addiction and how vital their role is in the family
intervention process (Wilson & Wilson, 1992).
To date, there is scarce data-based research available concerning family members’
attitudes toward addiction or toward a specific relative with addiction (Smith, 2006).
What have been reported, are limited studies or narratives of family members’ general
attitudes toward addiction and societal views of addicts and their families. Health
professionals’ attitudes toward individuals with addiction, on the other hand, have been
researched more carefully.

18
Studies and Research
Alexander and Dibb (1967) conducted a study in which they compared eight
families who had a son or daughter with addiction with eight families with a son or
daughter who did not have an addiction. Several differences were found between the two
family groups. For example, in the “addict” families, fathers and mother held their son or
daughter in low esteem and thought that the son or daughter was dishonest, secretive,
disappointing, and unsuccessful (Alexander & Dibb). These findings were thought to
“validate clinical observations that societal perception in addict families serves to
perpetuate opiate addiction by undermining addicts’ self-esteem” (Alexander & Dibb, p.
17). As a result, researchers determined that there was a need for a new approach to
addiction therapy that would help change the attitudes and perceptions of family
members toward the relative with addiction (Alexander & Dibb).
Regarding research on attitudes, very limited research has been conducted that
focuses on family attitudes toward addiction. There is, however, a body of research that
centers on healthcare providers’ attitudes. The results of these studies may have some
application to family attitudes. In a qualitative study of families’ opinions about the
general attitudes of the public toward addiction (Canale & Munn, 2005), researchers
found, through interviews and focus groups comprised of family members and people
with addiction, that negative attitudes of the general public toward addiction created
barriers to access of healthcare and support for themselves and family members. Some of
the stigmas experienced by family members and addicts were feelings of “negative
judgment, long-lasting labels, disgrace, embarrassment, and shame” (Canale & Munn, p.

19
13). According to Canale and Munn, negative societal views of addiction or the negative
stigma toward addiction impacts the family member and relative with addiction in areas
such as (a) being treated with less respect when seeking medical care, (b) being judged
negatively by society because of their addiction, (c) experiencing self-loathing and
internalizing the disrespect of others, and (d) continuing the cycle of addiction to avoid
dealing with the negative attitudes of others. In a different study comprised of Chinese
health professionals (Tang, Wise, Mao, & Hou, 2005), researchers found that drug abuse
was viewed as an “ugly social phenomenon”. As a result, the attitudes of Chinese
doctors were negative toward people with addiction, causing inferior treatment results
(Tang et al.). Researchers found in another study (Martinez & Parker, 2003) that nursing
students held negative attitudes toward people with addiction. According to Martinez
and Parker, student nurses were critical of addicts and perceived this population to be
weak. It was also found that nurses’ beliefs and attitudes toward addicts’ correlated with
poor quality of care. In South West Sydney, researchers studied 416 General
Practitioners’ (GP) attitudes toward patients with addiction and found that many GP’s
perceived these patients as less-rewarding, time consuming, disruptive to their practice,
and difficult to treat (Abouyanni et al., 1999). Consequently, many GP’s were reluctant
to provide care and did not want to “turn their practices into drug clinics.” In a smaller
study relating to attitudes of GP’s, Abed and Niera-Munoz (1990) found that a small
percentage of GP’s (10%) agreed with the statement: “Addicts deserve whatever
misfortune befalls them.” In a study of allied health students and physician assistant
students from one public and one private university in the United States (Baldwin et al.,

20
2008), many students were unable to identify levels of drug use that were risky. Sixty
percent to seventy percent reported that they used alcohol at least on a monthly basis and
some revealed that they used legal and/or illegal drugs on occasion. The researchers
expressed concern regarding the high degree of acceptance of substance use by students
who were studying to be health professionals. The researchers further stated that they felt
that the students’ approval of the substance use may lead to permissive attitudes toward
addiction and when not properly dealt with could lead to negative outcomes for patients
and their families (Baldwin). In another study, Copello et al. (2000) examined attitudes
of 37 healthcare professionals’ (i.e., general practitioners, nurses, and health visitors)
toward family members with addiction. Researchers reported a lack of confidence and
ambivalence toward working with family members who have a relative with addiction
(Copello et al., 2000). The healthcare professionals received a brief family-based
treatment training that focused on their attitudes and confidence in working with family
members who have a relative with addiction. According to Copello, the health
professionals who received the training reported an improvement in their confidence
level and perceptions about working with family members who have a relative with
addiction in contrast to those healthcare professionals who did not receive the training.
As a result, the researchers concluded that providing brief family-based treatment training
to healthcare workers increased their confidence level and produced positive outcomes
for family members by lowering levels of stress and increasing coping skills (Copello).
Lastly, in a study using the Attitudes Measurement: Brief Scales (AMBS) created
by the National Centre for Education and Training on Addiction (NCETA, 2006) at

21
Flinders University in Adelaide, Australia, researchers focused on healthcare workers’
attitudes, (i.e., stigma) surrounding addiction and how those attitudes affect quality of
care for people with addiction (Skinner, Fether, Freeman, & Roche, 2007). Results from
the study indicated that many healthcare workers who deemed a person with an addiction
as being responsible for his or her condition, held a negative view toward the person
(2006). What was incongruent, however, was that healthcare providers routinely
provided “high-quality care and treatment to individuals who hold a significant degree of
personal responsibility for other health conditions (e.g., heart disease, obesity)” (Skinner
et al., p. 164). Therefore, being responsible for the addiction may not be the only reason
healthcare workers were reluctant to provide treatment to addicts. There is some
validation that indicates that deservingness judgments are likely to influence healthcare
workers services toward persons with addiction (Skinner et al.). In the study at NCETA,
nurses were presented with two opportunities in which high and low quality health care
was provided to addicts. There were three antecedents of deservingness: (1) affective
reactions to the drug user, (2) attributions of responsibility for drug use, and (3) values
(i.e., general beliefs and attitudes) held by nurses. According to Skinner et al., the results
supported the efficacy of a “social-justice perspective in understanding the dynamics of
health-care practices regarding stigmatized conditions” (p. 165). For example, the
research supported the influence of affective responses of healthcare workers regarding
decisions about whether high or low level care is deserved. Moreover, positive affect
(i.e., sympathy, concern) predicted deservingness of high level care, while negative affect
(i.e., anger, disappointment) predicted deservingness of low level care. Furthermore, the

22
judgments of addicts’ “deservingness of low (or high) quality of care” influenced the
healthcare workers own level of satisfaction with the standard of care (i.e., general
beliefs, values) (Skinner et al.).
As noted earlier, most researchers have studied attitudes of healthcare providers.
According to Smith (2006), there is still a need to study whether attitudes of family
members’ will change and the factors that may facilitate that change. One intervention,
brief family-based treatment, has demonstrated some success in this area.
Brief Family-based Treatment
Brief family-based treatment (FBT) involves a comprehensive training curriculum
that is respectful, inviting, supportive, and healing (Wilson & Wilson, 1992). Family
members share what they have experienced due to the family member’s misuse of drugs
or alcohol through newly learned communication skills, psychodrama, role play, and by
completing a strength-based family assessment (Jay & Jay, 2000). FBT therapies are
intended to change patterns of beliefs and behavior among family members (Carich &
Spilman, 2004; Miller, Meyer, & Tonigan 1999). In view of this intention, treating a
relative with addiction is considered by those who practice FBT to be a “change-oriented
process that occurs in the context of a contractual, empowering, and empathetic
relationship” (Zeig & Munion, 1990, p. 14). Thus, the goal of intervening in the family
system is to create change (Carich & Spilman). Furthermore, brief family-based
treatment can be very useful in helping family members change negative feelings and
attitudes about a relative with addiction without disrupting relationships within the family

23
system (Washton & Zweben, 2006). An important component of the change-oriented
process is helping family members understand how they function and how their self-
belief (i.e., attitudes) can contribute to positive outcomes for a relative in terms of
providing supports in the recovery process using a family-based treatment model
(Vannicelli, Gingerich, & Ryback, 1983)
According to O’Farrell (1995), involving family members in the FBT process has
resulted in more positive results for the family and the addict by decreasing his or her
substance abuse and increasing interest in treatment. FBT may also help family members
to (a) have more rational attitudes toward the relative with addiction, (b) motivate the
relative with addiction to remain in treatment, and (c) recognize and address situations
that impede recovery (O’Farrell).
Additional research in the area of family involvement has also concluded that
“family members can do something to instigate change” (Miller et al. 1999, p. 695). In
an interview with therapists from Addictions Intervention Resources (A.I.R.), Dempsey
(2006) reported that the therapists believed the primary reason most relapses among
clients who are addicts occur is due to a lack of personal care and family support that is
needed to intervene and change destructive patterns of behavior. Colandro (n.d.)
maintained that it makes sense to engage parents and family members in the treatment
process to assist their relative with an addiction.
24
Statement of the Problem
Recent research regarding brief family-based treatment has suggested that
working with family members of relatives with addiction can lead to positive results for
family members by offering education about the impact of addiction on the family system
(Beck et al., 2003; Jay & Jay, 2000; Johnson, 1998; Rotunda, West, & O’Farrell, 2004;
Sulek et al., 2006). Few studies, however, have been conducted that focus specifically on
examining changes in family members’ attitudes toward addiction or toward a specific
relative with addiction. To date, there is a scarcity of data regarding how FBT impacts the
opinions, self-beliefs, attitudes, and judgments of family members toward people in
general with addiction and toward a relative with addiction. Until a more conclusive
body of research exists regarding its effectiveness, practitioners, family members,
theorists, advocates, and scholars can not make definitive statements regarding the
relevance of FBT and how family member’s attitudes are affected by this intervention.
Significance of the Study
There is a developing concern today regarding the increase in addiction in our
country (Smith et al., 2006), which until recently has been seen as an individual problem
(Beck et al., 2003; Copello, Templeton, Krishnan, Orford, & Velleman, 2000; Rotunda
et al., 2004; Sulek et al., 2006). While issues related to how the family plays a role in the
addiction process have been considered, they have rarely been a component of the
treatment plan for the person with addiction (Orford, Templeton, Velleman, & Copello,
2005). Consequently, most therapies have been designed to treat addiction and have

25
focused on the individual person and not the family itself (Nelson & Sullivan, 2007).
Family-based treatment, however, teaches family members why the addictive behavior
exists, how to set consequences for behaviors, and how to focus on creating a positive
approach (i.e., change perceptions about the relative with addiction) in order to decrease
their addictive behavior (Smith, et al., 2006).
According to Smith (2006), there is a growing awareness in the therapy
community that indicates a need for more research that focuses on helping family
members to create a more positive home environment and improve their feelings, beliefs,
and perceptions (i.e., attitudes) toward addiction treatment and toward a relative with
addiction by attending a brief family-based treatment session. The purpose of the current
study is to examine whether brief family-based treatment impacts family members
attitudes toward people in general with addiction and toward a specific relative with
addiction.
Research Questions
1. Is there a change in family members’ attitudes toward people in general
with addiction from pre- family-based treatment to post-family-based treatment?
2. Is there a change in family members’ attitudes toward a specific relative
with addiction from pre- family-based treatment to post-family-based treatment?

26
Independent and Dependent Variables
1. Independent variable: FBT training; dependent variable:
perceptions/attitudes toward people in general with addiction.
2. Independent variable: FBT training; dependent variable:
perceptions/attitudes toward a specific relative with addiction.
Alternative Hypothesis
1. It is hypothesized that after brief family-based treatment, family member’s
perception of people in general with addiction will be changed in a more positive
manner.
2. It is hypothesized that after brief family-based treatment, family member’s
attitude toward a specific relative with addiction will be changed in a more positive
manner.
Null Hypothesis
1. It is hypothesized that after brief family-based treatment, there will be no
change in the family member’s perception of people in general with addiction.
2. It is hypothesized that after brief family-based treatment, there will be no
change in the family member’s attitude toward a specific relative with
addiction.

27
Definition of Terms
Addiction: a complicated disease (NIDA, 2008) that includes abuse of and physical and
mental dependence on alcohol or legal or illegal drugs; physical dependence on and
abuse of drugs and other miscellaneous substances (DSM-IV TR); and a chronic,
consistent repetition of disproportionate behavior that a person is unable or unwilling to
stop, despite its destructive consequences to the person with addiction, his or her family
members, and society (Gutman, 2006).
Anger: A feeling toward the relative with addiction that may seem like a love/hate
relationship. The person is loved, while the addiction and what it’s doing to the family I
hated. There is an inability to separate the person from the disease of addiction (Jay and
Jay, 2000).
Attitudes: Emotionally charged ideas that prompt a set of actions toward a certain class
of individuals (Triandis, 1971). Attitudes are associated with a tendency to behave in a
predictable and guarded way toward or in the presence of members of a particular group
(Hunt & Hunt, 2004). Attitudes communicate three common beliefs: (a) they include
some kind of judgment of someone; (b) they can be articulated through language; and (c)
they are associated with actions toward another (Eiser, 1986; McCarthy & Light, 2005).
Other terms used to describe attitudes include beliefs, values, opinions, self-beliefs,
judgments, perceptions, thoughts, feelings, and stigmas. Therefore, for the purpose of
this study, the term attitude will represent all of the above definitions.
Binge use: Five or more drinks on the same occasion, at the same time and within a few
hours of each other within a 30 day period (NIDA, 2008).

28
Contractual, empowering, and empathetic relationship: The capacity to recognize or
understand another's state of mind or emotion in a way that shows respect, rapport,
joining, compassion, cooperation, flexibility, safety, goal orientation, and multi-level
communication. Contractually, this framework provides a guide for the practitioner to
conduct the treatment in a way that is goal oriented and focused on intervening in the
family system to create change (Carich et al., 2004).
Current use: At least one drink in the past 30 days, this includes binge and heavy
drinking.
Differentiation: The ability of each family member to preserve his or her own identity,
while still remaining connected to the family system.
Disease of addiction: Refers to addiction as a complicated disease that can encompass
essentially every aspect of a person’s life that has typical signs and symptoms that may
progress in a certain manner (Wilson & Wilson, 1992). The person with addiction has a
disease that has a physiological deficiency that makes him or her incapable of tolerating
the addictive substance (Smith & Miller, 2000).
Drink: A can or bottle of beer, a glass of wine or wine cooler, a shot of liquor, or a mixed
drink with liquor in it.
Family: The foundation of social relationships among all cultures (Garrett et al., 2007).
Family Member: Traditional close relatives such as a mothers, fathers, spouses, siblings,
and extended family members such as grandparents, aunts, uncles, cousins, partners, and
family friends and loved ones known as significant others

29
Family-based treatment (FBT) (also referred to as brief family-based treatment,
family systems model, family systems intervention, and couple and family therapy):
A branch of psycho-education that works with families and couples in intimate
relationships to encourage change and development. Changes in terms of the systems of
interaction between family members emphasize that family relationships are an important
factor in psychological health.
Heavy drinking: Five or more drinks on the same occasion occurring on five or more
days within a 30 day period.
Homeostasis: A state that occurs when the family members seek to maintain a healthy
balance. Families tend to resist change, consequently, the family therapist can use the
concept of homeostasis to explain why a certain family symptom has surfaced at a given
time, why a specific member has become the identified patient, and what is likely to
happen when the family begins to change.
Identified patient (IP): Generally, the family member who has an addiction or who is
presented as the main symptom-bearer in the family. However, individuals referred for
family systems treatment are often incorrectly labeled "patients" when, in fact, their
symptoms are manifestations of family, not individual, dysfunction or pathology.
Recovery: A complicated, painful process of extreme transformation that is never easy
and rarely effortless for anyone involved (Brown, 1997).
Relative with addiction/loved one with addiction: A person within the family who is
identified as having an addiction to either a legal or illegal drug, or alcohol.
30
Significant other/friend: Extended family members such as grandparents, aunts, uncles,
cousins, and partners as well as individuals, known as significant others, who are not
considered to be typical family members.
Treatment goals: An assessment of the individual/family to gather a family history,
training to provide the individual/family with tools to understand addiction, and an
aftercare plan designed to help the family and individual set and achieve goals set forth in
therapy (Jay et al., 2000).

31
CHAPTER TWO
REVIEW OF THE LITERATURE
Chapter Two provides an overview of the published literature with regard to the
following aspects of addiction and treatment: (a) addiction statistics and the need for
treatment, (b) attitudes toward and beliefs about addiction, and (c) family-based treatment
approaches.
Addiction Statistics and Need for Treatment
In a study conducted by the National Survey on Drug Use and Health (NSDUH,
2007), researchers found that the rate of drug use among youth aged 12 to 29 grew
slightly from 8.1% in 2005 to 8.3% of the population in 2006. The researchers also found
that more than half of youth in America (125 million) aged 12 to 29, reported drinking on
occasion; whereas 6.9% (17 million) aged 12 to 29, reported drinking heavily in 2006.
For example, the following statistics illustrated the percentage of alcohol used by youth;
12 and 13 year olds (3.9%); 14 and 15 year olds (16%); 16 and 17 year olds (29%); 18 to
20 year olds (51%); 21 to 25 year olds (68%); and 26 to 29 year olds (63.5%).
In another study completed by SAMSHA (2006), it was estimated that 30.5 million
people, aged 12 and older, were dependent on, or addicted to either drugs or alcohol.
The societal cost of addiction, according to the SAMHSA report, is over $300 billion per
year, continues to rise each year, and has resulted in one of the most severe health
concerns facing America, today. The results of a survey completed in 2007 for The

32
National Survey on Drug Use and Health National, entitled Illicit Drug or Alcohol Use
Treatment and Treatment Need, provide additional support for the need for treatment:
1. In 2007, 23.2 million persons aged 12 or older needed treatment for an
illicit drug or alcohol use problem (9.4 percent of the persons aged 12 or older). Of these,
2.4 million (1.0 percent of persons aged 12 or older and 10.4 percent of those who needed
treatment) received treatment at a specialty facility. Thus, 20.8 million persons (8.4
percent of the population aged 12 or older) needed treatment for an illicit drug or alcohol
use problem but did not receive treatment at a specialty substance abuse facility in the
past year. These estimates are similar to the estimates for 2006 and for 2002.
2. Of the 2.4 million people aged 12 or older who received specialty
substance use treatment in 2007, approximately 1,000,000 persons received treatment for
alcohol use only, 750,000 persons received treatment for illicit drug use only, and
650,000 persons received treatment for both alcohol and illicit drug use. These estimates
are similar to the estimates for 2006 and for 2002.
3. In 2007, among persons who received their last or current substance use
treatment at a specialty facility in the past year, 53.3 percent reported using their "own
savings or earnings" as a source of payment for their most recent specialty treatment,
34.9 percent reported using private health insurance, 26.3 percent reported using public
assistance other than Medicaid, 19.7 percent reported using Medicare, 19.6 percent
reported using funds from family members, and 18.2 percent reported using Medicaid.
None of these estimates changed significantly between 2006 and 2007 and between 2002

33
and 2007, except that the 53.3 percent reported using their "own savings or earnings" as a
source of payment in 2007 was higher than the 42.1 percent reported in 2006. (Note that
persons could report more than one source of payment.)
4. Of the 20.8 million persons in 2007 who were classified as needing
substance use treatment but not receiving treatment at a specialty facility in the past year,
1.3 million persons (6.4 percent) reported that they perceived a need for treatment for
their illicit drug or alcohol use problem. Of these 1.3 million persons who felt they
needed treatment but did not receive treatment in 2007, 380,000 (28.5 percent) reported
that they made an effort to get treatment, and 955,000 (71.5 percent) reported making no
effort to get treatment (p. 80).
While researchers in the United States have concluded that substance abuse
declined slightly among adolescents, there are still 2.1 million youth in the United States,
aged 12 to 17 (8.3 % of the population) in need of treatment for illegal drug use
(SAMHSA, 2005). According to the researchers, youth who engage in substance abuse
(and especially minority youth) are found to be responsible for negative behaviors such
as criminal activities. According to the National Mental Health Association, in 2000
there were one million youth within the justice center being charged with criminal
behavior associated with drug use in the United States and many were repeat offenders.
What is clear, therefore, is that substance abuse exacerbates and prolongs criminal
behavior (Young, Dembo, & Henderson, 2007). For example, substance misuse in itself
binds one to illegal behavior (i.e., purchasing and possessing illegal substances). In
addition, youth who engage in these activities are more likely to be predisposed to

34
criminal behavior as they look for opportunities to obtain money to buy more drugs
(Chassin, Knight, Vargas-Chanes, Losoya, & Naranjo, 2009). In looking for treatment
outcomes, Stanton (2004) suggests that youth with substance disorders are generally very
close to their parents or people who raised them and as a result, parents may be
significant candidates from which to seek help.
Family Members’ Attitudes toward Addiction
The tragedy surrounding addiction is evident (Stanton et al., 1979). Especially
since addiction sets the stage for the profusion of other problems, such as criminal
activity, incarceration, emotional highs and lows, instability within the family, separation
from family, and an increase in negative attitudes about addiction and the relative with
addiction (English, 2000; Jay & Jay, 2000; Johnson, 1998). Family members who have a
relative with addiction respond not only to the addiction process, but also to their
perceptions (i.e., attitudes) associated with addiction (Bradshaw, 1996). These attitudes
include, but are not limited to, belief that the relative with addiction is personally
responsible for his/her condition, thoughts that the person with addiction does not deserve
respect, disappointment in the relative with addiction, anger toward the relative with
addiction, negative opinions about the relative with addiction, and belief by others that
the relative with addiction may not deserve the same level of medical care as individuals
who are not addicted (Bradshaw).

35
Consequently, family systems where addiction is present generally operate in
chaos, resulting in a confused state with regard to family members’ beliefs toward the
relative who is using (Suleck et al., 2006). Many of these same families remain in a
holding pattern with very little change in family attitudes or behavior while the relative
with addiction continues to use (Steinglass, 1980). Some family members, however,
wish to address the issue of addiction and support their relative. Many of these family
members search for guidance by attending a brief family-based treatment session to
address attitudinal and perception change (Cottrell et al., 2002).
Brief Family-based Treatment Approaches
Treatment for addiction is conducted in many different ways using a variety of
therapeutic approaches (NIDA, 2008). No single treatment is effective for every
individual. Because addiction is generally a chronic condition, typified by reuse and
relapse, it is often necessary for multiple treatment interventions. Consequently, the
parameters of treatment are as varied as the therapeutic techniques used (Sexton &
Alexander, 2002). Family-based treatment is one therapeutic intervention technique that
addresses the ways in which each family member plays a part in the family as a whole
(Bradshaw, 1996). The term, family-based treatment, depicts a variety of family
interactions (Cottrell & Boston, 2002) and has been found to be effective in the treatment
approaches for a variety of disorders (Sexton & Alexander). Furthermore, several studies
have rated brief family-based treatment approaches for adolescent substance abuse as the

36
treatment of choice (Stanton & Shadish, 1997; Williams & Chang, 2000). For the
purpose of this study, the focus will be on addiction and family-based treatment.
Because addiction is a disease of the family, every relative with addiction directly
impacts at least five to eight other family members. Family-based treatment, therefore, is
not about the relative with addiction, but about family members and how they choose to
view or react to the relative with addiction (Jay & Jay, 2000). The principle of FBT is to
engage the members of a specific or extended family in training that will provide
education and encourage them to adjust their self-beliefs, opinions, and perceptions (i.e.,
attitudes) in a positive manner toward people in general with addiction, and toward a
specific relative with addiction (Carich et al. 2004; Stanton, 1979; Vannicelli et al.,
1983).
FBT uses an approach that distinctly focuses on shifting the interactions between
or among family members and seeks to improve the functioning of the family system
(Gurman et al., 1986). The theory of FBT suggests that the family is the patient and
views the relative with addiction as the sign of “family psychopathology” (Bradshaw,
1996). The goal of family-based treatment, therefore, is to help family members
understand their relative’s addiction and adjust their attitudes toward the relative with
addiction and toward addiction in general. The objective of FBT is to provide short-term
treatment with the focus on intense restructuring of family functioning and greater
discernment of the problem (Steinglass, 2008). The intent, according to Cottrell and
Boston (2002), is to evaluate family members in terms of their perceptions about
addiction, focusing on training them about addiction while attempting to shift their

37
attitudes toward addiction and the specific relative with addiction in a more positive and
well-informed direction.
Family-based treatment is considered to be a valuable counseling tool for
therapists for two reasons: (a) there is increased evidence that what was once thought of
as an individual problem (i.e., substance abuse, depression, eating disorders) can be
successfully treated with FBT (Gurman et al., 1986), and (b) FBT has demonstrated
successes with families from diverse cultural backgrounds and as a consequence has
become the treatment of choice for adolescents with substance abuse and behavior
disorders (Sexton et al., 2002).
Researchers suggests that family-based treatment training programs help identify
and change attitudes and perceptions about addiction and a relative with addiction
(Cottrell et al., 2002; 2001; English, 2000; Jay & Jay, 2000; Johnson, 1998; McLendon,
McLendon, & Petr, 2005). Key points (e.g., definitions, goals, and outcomes) of family-
based treatment models are reported by various researchers (Bergin & Garfield, 1994;
Cannon & Levy, 2008; Cottrell & Boston; Connors et al.; English; O’Farrell et al.; Jay &
Jay; McLendon et al.; Miller et al.; Santisteban et al., 2003; Sexton & Alexander, 1999;
Sexton & Alexander, 2000; Sexton & Alexander 2002; Smith et al. 2006; Vetere, 2001)
and core definitions and goals of the different types of FBT are presented by researchers
or scholars (Cannon & Levy; English; Jay & Jay; Johnson; Liddle et al.; McLendon et al.;
O’Farrell et al.; Sexton & Alexander, 2000). Mixed results were found by two
researchers. Connor et al. and Miller et al. found family-based treatment to be
confrontational in nature, thereby limiting the efficacy of the intervention with 70% of

38
family members failing to complete therapy. Conversely, other researchers found
positive family/client outcomes due to family involvement, therapist involvement, the
family members’ change in attitudes toward addiction and a relative with addiction, and
the development of more effective communication and problem solving with intervention
training (Bergin & Garfield; Cannon & Levy; Liddle et al.; McLendon et al.; Santisteban
et al.; Sexton & Alexander, 2000). Following are some recognized brief family-based
treatment models that have shown promise in working with the family unit and relative
with addiction.
Brief Strategic Family Therapy
Brief Strategic Family Therapy (BSFT) was developed at the Spanish Family
Guidance Center in the Center for Family Studies, University of Miami in 1975 and has
been conducted at these centers since that time. The Center for Family Studies has been
described as the Nation’s oldest and most prominent center for development and testing
of minority family therapy interventions for prevention and treatment of adolescent
substance abuse and related behavior problems (Santisteban et al., 2003). Therapy
consists of as few as one brief session to 4 to 20 weekly, 1-hour sessions with family
members that focus on changing the environment of the adolescent in the family who has
an addiction while also identifying patterns of family interactions and attitudes toward
addiction that are associated with the adolescent’s addictive behavior (Cannon & Levy,
2008). Assessments and interviews are conducted with family members to determine
concerns about addictive behavior and the desire for abstinence and positive aftercare

39
follow-ups when the relative returns home. A therapist meets with the family with whom
the child with addiction lives to review and recommend attainable aftercare treatment
goals (O’Farrell et al., 2008).
BSFT is based on three basic sets of guidelines; first, the assumption that the
family members are interdependent of one another and therefore what impacts one family
member, often impacts another; second, patterns of behavior that exist in the family
influence the stability and balance of the family; and third, because the homeostasis of
the family is disrupted by addictive behavior, it is vital to plan therapy designed to
change patterns of interactions, ways of thinking (i.e., attitudes), and behavior within the
family unit (NIDA, 2005). The goals of BSFT are two-fold and include eradicating or
decreasing the adolescent’s addiction and changing the attitudes, perceptions, and
interactions of family members that are associated with the addiction. Therefore, to
ensure that these goals are accomplished, the family therapist must “join, diagnose, and
restructure families” (Cannon et al., 2008, p. 201). Involvement with the family is also
critical, and must be open and supportive from the beginning and focused on working
together to accomplish therapeutic goals. A literature review of BSFT conducted by
Cannon et al. assessed the treatment and engagement of Hispanic youth who were found
to have an addiction. Researchers reviewed fifteen records found in the ProQuest Social
Science Journal (1996-2006, p. 199) as well 96 records retrieved from an internet search
of key words such as “youth, substance abuse, and Latino or Hispanic.” They concluded
that BSFT was more successful because it was geared toward family involvement that
focused on changing family behavior patterns (i.e., beliefs, judgments, attitudes) toward

40
addiction, more so than traditional group therapy for youth with early stages of addiction
(Cannon et al.). As a result, BSFT was recommended for Hispanic families who had
children with addiction, in particular, because of the highly sensitive understanding
relating to a variety of cultural issues (Santisteban, et al.). In a study completed by
Santisteban et al., while working with Hispanic families, the researchers found that most
adolescent problem-behaviors were linked to dysfunctional family dynamics, unclear
family boundaries, improper family relationships, and the belief that the youth with
addiction were the cause of the families’ problems. For that reason, therapists worked
closely with family members to address dynamics, such as setting appropriate
boundaries, assigning leadership in the family, understanding how the addiction impacts
the family (i.e., perceptions of the problem of addiction), and utilizing conflict resolution.
Multidimensional Family Therapy
Multidimensional Family Therapy (MDFT) is a family-based treatment model
that was developed for adolescents with addiction and behavior problems. The MDFT
intervention has evolved over the last 17 years within a federally funded research
program designed to develop and evaluate family-based intervention for addiction
treatment for adolescents. This approach has been recognized as one of a new generation
of comprehensive, adaptable, “theoretically-derived and empirically-supported adolescent
drug abuse treatments” (Liddle, Dakof, Turner, Henderson, & Greenbaum, 2008). There
are several different therapeutic approaches of MDFT, such as home-based, residential,
office-based, and brief-intensive out-patient. Sessions vary from one to three times per

41
week over a course of 4-6 months based on the severity of the addiction and the needs of
the family and youth. What are most notable about MDFT are the four domains used by
therapists that are critical in all of the approaches. The first domain deals with the
adolescent and teaches youth how to engage in treatment by (a) using effective
communication with families, (b) acquiring coping skills that lead to emotional stability
and more effective problem-solving abilities, (c) improving social capabilities and school
or vocational performance skills, and (d) learning alternative behavior that steer clear of
addiction. The second domain is the parent domain which engages parents in therapy by
(a) increasing their emotional presence with the adolescent; (b) improving parenting
skills, especially in the areas of supervising, clarifying and deciding consequences for
behavior; and (c) addressing their “psychosocial functioning apart from their role and
responsibility as a parent” (p. 1663) (Liddle et al., 2008). The third domain deals with
interactions and focuses on (a) decreasing family conflict, (b) improving relationships, (c)
communicating more effectively, and (d) learning successful ways to problem-solve. The
fourth domain centers on extra-familial issues that foster family competencies in
numerous social systems to include school, work, courts, and leisure/entertainment. With
regard to improving parenting skills, the MDFT perspective asserts that symptom
reduction and improvement of normal social functioning in adolescents with addiction
occurs when the family system is the objective for the therapy/intervention. Furthermore,
certain behaviors, and ways of thinking (i.e., attitudes) known to be related to the
problem addiction are replaced by new behaviors and perceptions that are linked with
family functioning (Liddle et al., 2002).

42
In a study assessing adolescent addiction for problem-severity and frequent use,
MDFT was found to reduce the rate of drug use both during treatment and in the 6-month
follow-up. In addition, MDFT was found to decrease the severity of drug use, thereby
indicating that Multidimensional Family Therapy was a more effective intervention for
youth than other therapy models that did not include the family (Liddle et al., 2008).
Functional Family Therapy
Functional Family Therapy (FFT) is an intervention strategy supported by 30
years of clinical research. FFT examines the practice of youth with addiction or antisocial
behavior problems and has been applied to a wide range of youth and their families in
various multi-ethnic, multicultural contexts and with pre-adolescents and adolescents
diagnosed with conduct disorders, violent acting out and substance abuse (Sexton &
Alexander, 2000). The primary focus of Family Functional Therapy is on family
intervention and positive and negative behaviors (i.e., family belief systems and
strengths) and how those behaviors influence family and individual functioning.
According to Sexton and Alexander, FFT provides family members with a motivation for
changing their perspective (i.e., attitudes, viewpoints), by helping families build on their
strengths in ways that cultivate self-determination and detail specific goals for
improvement within the family system.
FFT is a “multi-systemic and multi-leveled” family system intervention that
focuses on three major components (a) the treatment system, (b) the family and
individual functioning, and (c) the therapist (Sexton & Alexander, 2000). FFT, like most

43
brief family-based treatment incorporates family strengths and aspirations to improve
their circumstances as a starting point. At the point of clinical engagement, “FFT
includes a systematic and multiphase-intervention map” (Sexton et al., p. 2) titled Phase
Task Analysis, which provides the basis for clinical decision-making. This map provides
a format that portrays FFT to have a flexible structure for the intervention process by
identifying treatment modalities that have a high probability of success and assisting
counselor’s with options for presenting strategies for each family therapy session. It is
also culturally sensitive and responsive to youth, their families, and their communities
(Sexton et al., 2000). The primary focus of Functional Family Therapy (FFT) is on the
family. The objective of the intervention is to reproduce a mirror image of the positive
and negative behaviors that cause and are caused by various relational systems operating
within the family.
FFT was designed in 1969 to meet the needs of a growing population of youth
who were involved in violent crimes and drug addiction (Alexander & Parsons, 1973).
The developers argued that successful treatment of youth with addiction required
therapists who were aware of culturally diverse families, and who were also
knowledgeable to work with them, especially as it related to the families resistance to
treatment. As a result, over the past 30 years, FFT counselors have recognized that
helping families identify strengths and build self-respect are keys to improving family
functioning (Sexton & Alexander, 2002). What is more, FFT developers have noted the
need to evolve as the needs of the families have changed. For example, in the late
1990’s, Functional Family Therapy advanced the phases of intervention by developing a

44
systemic approach (Sexton & Alexander, 1999) to training and systematic execution with
the addition of an all-inclusive system of individual, process, and outcomes assessment
using a computer-based component that monitors and traces clients using a device called
the Functional Family Therapy – Clinical Services System (FFT-CSS). The FFT-CSS
helps therapists identify and implement intervention goals aimed at creating change in a
way that promotes accountability through technique and outcome evaluation. As a result,
FFT has grown into an intervention model that includes systematic training, monitoring
of techniques, and assessment of outcomes that are all directed at improving the delivery
of intervention services to families in communities where juvenile addiction rates are
high (Sexton & Alexander, 2000).
Functional Family Therapy is a brief, short-term, “family-based prevention and
intervention” process that has shown efficacy in a number of difficult situations dealing
with youth between the ages of 11 and 18 who were underserved and at risk along with
their families (Sexton & Alexander, 2000). In most cases, clients are seen 8 to 12 times
for a total of 30 direct session hours over a three month period of time.
There are three intervention phases in FFT: (a) engagement and motivation, (b)
changing the negative behavior of the adolescent, and (c) generalization. The phases are
inter- and intra-dependent of one another; each have specific goals and assessment
objectives to be incorporated in therapy to change family beliefs and attitudes from
dysfunctional perceptions toward the expectation that change is possible. FFT is family-
centered, therefore, the goals are to (a) improve and build an alliance with the family and
counselor, (b) generate respect for individuals and family members, (c) change

45
maladaptive behavior while decreasing despotic negativity within families, (d) assess at
each phase how negative behaviors impact the family and relationships, and (e)
generalize the positive family changes from within the community to work
collaboratively and to create valuable alliances and support networks.
Family Functional Therapy is one of the brief family-based treatment modalities
for adolescent addiction and other behavior issues. The results of more than 30 years of
data-based research propose that following FFT guidelines may reduce addiction,
juvenile crime, violence and other delinquency problems (Sexton & Alexander, 2000).
Distinct to FFT is how the intervention focuses on family interactions from a cultural
perspective. From 1973 to the present, published data have reflected the positive
outcomes of FFT. For example, data have shown that when compared to standard
adolescent and family treatment interventions as well as alternative treatment approaches,
FFT is highly successful (Sexton & Alexander). Both randomized trials and non-
randomized comparison group studies have revealed that FFT significantly reduces
negative addictive behavior by increasing family functioning as described above.
Structural Family Therapy
Structural Family Therapy (SFT) is a method of family therapy that is linked to
the work of Salvador Minuchin; however, many other clinicians in the family therapy
arena have contributed ideas and concepts (Vetere, 2001). The emphasis is on building
family strengths by working together and learning practical ways to solve problems.
Contracts are written and agreed upon with family members. SFT is time limited, relying

46
primarily on quick and concise feedback regarding specific problems within the family
system. Many of the ideas are similar to other brief family-based treatments, such as
family roles and rules, triangulation of conflict, subsystems and boundaries,
collaborations, and stability and change. What is unique about SFT, however, is how the
therapist focuses on the organizational characteristics of the family unit and family
dynamics and the hidden and exposed rules that effect interpersonal choices and
interactions in the family (Vetere, 2001). Encouraging family members to investigate
problems and discover alternative responses to situations in the safety of the therapeutic
setting is central to SFT. Structured Family Therapy is based on the theory of action
preceding understanding, using reframing to think beyond the negative problematic
behaviors and current conflicts to see how each member’s choices affect the family
structure and relationships within the family system. The intervention is supported in
three areas: (a) challenging the behavior that is problematic, (b) challenging the family
structure, and (c) challenging the family belief system (i.e., attitudes, perceptions)
(Vetere, 2001)
A primary goal of SFT is to encourage family members to interact with one
another (i.e., communicate), problem solve together, and rethink their decisions within
the family that are considered to be dysfunctional so as to change the structure of the
family system. An essential strategy of SFT involves having the therapist enter or join
with the family system as a catalyst for positive change (Vetere, 2001). This is
accomplished when the therapist “engages the family through interactive activities”
(English, 2000, p. 194). Patterns of family behaviors, rules, roles, subsystems, conflicts,

47
collaborations, and boundaries emerge and can then be evaluated for change. According
to English, change occurs as the therapist collects information and begins to recognize
family dynamics and family structure. Slowly the therapist begins to understand the
family’s “perceived reality.” The goal, therefore, is to confront the family members’
perceived reality and to shift perceptions and self-beliefs (i.e., attitudes) from the primary
“symptom bearer” to the entire family system. Therefore, in order for therapy to be
functional, the therapist must form a new system with the family group (Vetere, 2001).
By doing so, the therapist “joins” with the family by understanding each family member,
being careful not to become biased. In addition, the therapist must also adjust to the
needs of family members. This is accomplished by accommodating family members,
which includes (a) providing support and feedback for areas where family interactions are
working and offering guidance in areas that require a change in structure, (b) carefully
assessing how the family interacts, and (c) relating to the family’s culture and range of
effect through role modeling and mirroring (Vetere). SFT posits that change is a fragile
process, too little intervention by the therapist will result in continuance of the status quo
and too much intervention will result in fear of confrontation and blaming causing a
premature ending of therapy by family members (Vetere).
With regard to the efficacy of SFT, researchers in the United Kingdom report the
use of controlled and uncontrolled group comparison designs and single case design
comparing the relative importance of SFT (Bergin & Garfield, 1994). The overall
findings from the data from the meta-analysis revealed that FST showed significant
results when working with the following problems: (a) marital conflict, (b) women with

48
depression, (c) adult and adolescent addiction, and (d) child and adolescent conduct
disorder (Vetere). According to Minuchin (1998), SFT focuses on family
communications by preserving the value of the family system. What is of importance to
the study of SFT, according to Vetere, is that “structural family therapy continues to
evolve in response to challenges mounted from within and out with the systemic field,
and as part of integrative practice and multisystemic approaches, with practitioners ever
mindful of the need for regular feedback from family members themselves” (p. 133).
Family-Directed Structural Therapy
Family-Directed Structural Therapy (FDST) is based upon the traditional
concepts of family therapy found in Structured Family Therapy ( McLendon et al., 2005).
The FDST model is comprised of an easy to administer assessment tool that adult family
members complete. The assessment is time-limited, making it easy to measure. Designed
to empower the family, FDST employs a process that is a goal-oriented, and uses a time
limited approach that helps families identify strengths and enhance family functioning
while also addressing areas of problematic behavior. FDST also teaches intra- and
interdependence that may be used by the family, both inside and outside the clinical
setting. FDST focuses on family strengths and on lessening family conflict in a time-
limited manner. McLendon et al. (2005) described the following assessment process:
The initial assessment generally requires one 90 minute session and then seven to
nine sessions to assist the family in incorporating the process and vocabulary of
FDST into their daily lives. These seven to nine sessions occur as family needs

49
dictate, although experience has shown that sessions occurring at six weeks, three
months, and six months post-intake can help to reinforce FDST concepts, assist
families to assess any new areas of concern, and apply the FDST framework
accordingly. (p. 327).
With FDST, the core concepts which are “commitment, credibility,
empowerment, control of self, and consistency” serve as the foundation of family
functioning (Mclendon, 2005, p. 328). Commitment, according to McLendon, is to see
things through to completion, regardless of personal differences and conflicts. Credibility
is giving one’s word and demonstrating the capability to follow through, and
empowerment is having a confidence that personal thoughts and views are valued and
regarded, thereby believing that a person can inspire change. Control of self is making a
personal effort to change negative opinions (i.e., attitudes, beliefs) in a way that results in
less conflict within the family and more positive relationships, and finally, consistency is
behaving and communicating in an appropriate manner, thereby creating a sense of
wellbeing within the family. These core issues are used in association with the constructs
of roles, boundaries, external stressors, and the framework of communications to help
families identify strengths and discover problematic areas.
The function of roles in FDST are related to husband/wife (partner), wife/husband
(partner), parent, father, mother, individual, and child and are similar to roles in
Structured Family Therapy (Minuchin, 1974). Each family member plays an exclusive
role with one other family member (e.g., mother to child is different than father to child).
Boundaries are differentiated by the different roles played by family members and

50
between the family as a whole (McLendon et al., 2005). In FDST the boundaries are
based on family roles, not between subsystems in the family. External stressors are those
stressful events that occur from outside of the family structure. The impact from these
stressors may be positive (e.g., going on vacation, getting a promotion at work, or going
to a movie with the family) to negative stressors (e.g., losing a job, dealing with a family
member with drug addiction, or having health problems). Lastly, the framework of
communications consists of how family members express how they feel, using “I” and
“you” messages, engaging in conversation and the dynamics and rules that are followed,
or problem-solving techniques, such as taking personal responsibility for one’s actions
(McLendon et al.).
Family-Directed Structural Therapy uses an assessment tool to help families
understand the core issues and how the concepts of FDST are defined and easily
implemented by the family. By using a scoring system, families are able to rate
themselves in various areas. For example, a mother might rate her level of commitment to
her husband as well as her belief about his commitment to her. Family members also rate
themselves and other family members with regard to roles they play and roles they see
other family members play (McLendon et al., 2005). External stressors are also rated by
family members from each personal perception rather negative or positive. Once the
assessment is complete, the therapist uses the results to help families set goals by
evaluating their core issues and addressing areas of strength and areas that are
problematic.

51
Over the past 12 years, FDST has been presented to over 450 families from
diverse ethnic backgrounds; however, little data are available with regard to efficacy.
Currently FDST is being evaluated at a major university (McLendon et al., 2005). Two
types of family interactions are being studied, (i.e., one group of families is receiving
standard counseling services only, and the other family group is receiving Family-
Directed Structural Therapy). Both family groups are being studied at specified dates
after base-line to determine if there are changes to family functioning, what those
changes are, and if the changes are maintained over time. With regard to limitations,
McClendon emphasizes that the use of FDST is contraindicated in families where there is
“active domestic violence or threat of harm to self” (p. 335). In situations such as this it
is important to provide some sort of crisis intervention as well as FDST.
Summary
Addiction is a complicated disease that can encompass essentially every aspect of
a person’s life, including social and economic status, family, work, and community
interactions (NIDA, 2008). Fortunately, there is some information to support the
effectiveness of family-based treatment with regard to addiction (Cottrell & Boston,
2002). Brief family-based treatment is time-limited, relying primarily on quick and
concise feedback regarding specific problems within the family system. Counseling
supports may begin and end in a one day session or in one week (i.e., five days) of daily
sessions or one day a week for up to twenty weekly sessions (Cannon & Levy, 2008;
McLendon et al., 2005; Sexton & Alexander, 2000). In the brief family-based treatment

52
sessions, all members of the family as well as the therapist play a role. The therapist
seeks to analyze the process of family interactions and communication style, and family
members share through various modalities of communication (e.g. role playing and list
work) the symptoms or problems that brought them into treatment. A 25-year study was
conducted by the Hazelden Foundation, with addicts, family members, and treatment
interventions (Jay & Jay, 2000). It was determined that treatment must begin with people
who are knowledgeable of the disease of addiction and people who are knowledgeable of
and connected to the person with the addiction (Jay & Jay, 2000). For that reason, it has
been deemed vital to have an effective training model with clear goals that involve family
members of people with addiction in the treatment process (Meyers et al., 2002).
The goal of brief family-based treatment is to help family members understand
their relative’s addiction and to understand how each family member plays a role in the
addiction process. The objective of FBT is to provide brief, short-term treatment with the
focus on intense restructuring of family functioning and greater discernment of the
problem (Steinglass, 2008). The intent, according to Cottrell and Boston (2002), is to
evaluate family members in terms of their perceptions about addiction, focusing on
training them about addiction while attempting to shift their attitudes toward addiction
and the specific relative with addiction in a more positive and well-informed direction. It
is for this reason that professionals in the field of addiction have over the past decade
developed a different framework for FBT which is presented in a manner that is
respectful, caring, and conveys unconditional love and acceptance toward the person with
addiction. Consequently, family members work together in a therapeutic teaching

53
environment that is designed to encourage open communication about their feelings
toward a specific relative with addiction (Johnson, 1998). Additionally, intervening with
family members using FBT facilitates change (Garrett & Landau, 2007) by identifying
family strengths, working from this core to help family members address the problems of
addiction through education and counseling with an end toward changing family
member’s self-beliefs and perceptions toward addiction in a more positive direction
(Bradshaw, 1996; Gurman et al. 1986; Johnson, 1998).
Family has become a primary focus in the family-based treatment model for
addiction, and as a result, FBT has gained approval and acceptance over the past few
decades (Meyers et al., 2002). Furthermore, despite FBT’s popularity with many
therapists not all modalities of FBT have been evaluated using well-designed studies,
(Cottrell & Boston, 2002). For example, even though family-based treatment has been
utilized for many years, only Functional Family Therapy has been studied extensively
(Sexton & Alexander, 2000). FBT has, however, shown efficacy in the treatment of
substance misuse and behavior disorders on a smaller scale. One measure of efficacy that
has not been studied in depth is the change in the family member’s attitudes toward
addiction and their attitudes toward a relative with an addiction.

54
CHAPTER THREE
METHOD
Participants and Setting
This quasi-experimental study included a convenience sample of 41 participants
who were family members of persons with addiction. Nineteen participants (i.e.,
treatment group) were family members who had a relative with addiction who were
involved in brief family-based treatment (FBT) training at Pima County Juvenile Court
Center (PCJCC) in Tucson, Arizona; and twenty-two participants (i.e., control group)
were family members who had a relative with addiction who were involved in the KARE
Center, a local family support agency in Tucson, Arizona.
Description of Treatment Program
The treatment group received brief family-based treatment. Only those family
members who were 18 years and older and who had a relative with addiction were
eligible to participate. Eligibility and recruitment was based on confidential information
provided by counselors at the Pima County Juvenile Court Center (PCJCC) (see
Appendix A-1).
The Pima County Juvenile Court Center is located in South Tucson, Arizona and
was created to serve delinquent youth who have problems with criminal behavior and
substance abuse. PCJCC staff assist youth remanded to the program to (a) grow up to
become law-abiding adults, (b) find safe, permanent and nurturing homes, and (c) help

55
families in need gain access to the support and services they need to overcome the
problems that bring them into the court system (PCJCC, 2009).
“The mission of the Pima County Juvenile Court is to promote the interest and
safety of the community, promote the rehabilitation of children and families, facilitate the
protection of children who are abused and neglected, and facilitate the provision of
services to children and families involved with the court, all in accordance with the due
process of law. The Juvenile Court works actively with and provides leadership to the
community, public and private agencies to promote justice, education, and the prevention
of delinquency and abuse” (PCJCC, 2009).
The Pima County Juvenile Court Center has a Make a Change (MAC) program that
focuses on treatment readiness for family members’ who have an adolescent (youth) with
addiction. The program has a 20 bed detention center that was originally designed to
meet the needs of males between the ages of 15-17. Recently, however, an option to
include females and juveniles younger than 15 was added in a separate section.
Youth, whose family members participate in the MAC program, are detained in
the residential detention facility at the court center for 3 to 14 days. While the youth are
in detention, family members participate in a brief family-based, multi-family educational
treatment readiness session. The program components include: (a) increasing the family
member’s knowledge about the effects of substance abuse and challenging the family
member’s belief system (i.e., attitudes, perceptions) about addiction, (b) improving the
family member’s communication skills, (c) illustrating the importance of parental
supervision and support of the adolescent with addiction, and (d) offering community

56
support to family members who have an adolescent with addiction (PCJCC, 2009).
Family members meet with a structured family therapist one evening, on the first or third
Wednesday of the month for approximately two hours. The goal of the MAC program is
to help family members who have a relative with addiction to (a) understand the
addiction process, (b) identify warning signs of addiction, (c) develop positive
relationships with the youth with addiction, (d) examine their personal lifestyle and
perceptions to see what examples or judgments they may be setting for youth, and (e)
work together, in concert with other family members, to show healthy unity to youth. (A
detailed description of the treatment protocol/outline is provided in Appendix D).
Description of Therapeutic Support Program
The control group did not receive a family-based treatment session. Only those
family members who were 18 years and older and who had a relative with addiction were
eligible to participate. Eligibility and recruitment was based on confidential information
provided by the Director and counselors at the KARE Center (see Appendix A-2).
The KARE Center is a service-oriented facility where family members (i.e.,
traditional close relatives such as a mothers, fathers, sons, daughters, spouses, siblings,
and extended family members such as grandparents, aunts, uncles, nephews, nieces,
cousins, partners, and family friends and loved ones) receive out-patient family services
in the form of general and substance abuse support meetings. For example, family
members who are in need of supportive services meet on Tuesday mornings with staff to

57
discuss various concerns (e.g., substance abuse) that are related to their specific relative
(Melrood, 2008).
The KARE Center is located in Southern Arizona. The KARE campus offers the
following services to people caring for children who are born to others: (a) legal advice
about guardianship and adoption, (b) advocacy for caregivers with children in school, (c)
assistance with filling out benefits applications, (d) support groups for families raising
children of others, and (e) senior support services such as assessing financial and medical
needs for caregivers over 60 years of age. Many of the family members who receive
services from the KARE Center are supporting a person in the family who has an
addiction. The KARE Center does not offer a residential program for addiction. The
KARE Center does however, offer support services for family members who have a
relative with addiction. KARE members’ relatives with addiction are often incarcerated
for criminal behavior related to addiction and do not receive the same treatment as the
relatives with addiction at traditional treatment centers (Melrood, 2008).
Recruitment of the Treatment Group
The treatment group was found to be eligible for this study if they were age 18
years or older and had a relative who was in detention at the PCJCC. Upon arrival at
PCJCC and before the FBT session, family members read a flyer with details about the
study (see Appendix A-1).
On Wednesday evening, before the brief family-based session began, family
members met with the principle investigator (PI). The PI explained that the purpose of

58
the study was to examine family members’ perceptions toward people with addiction and
toward a specific relative with addiction (pre- and post-FBT). Family members were
advised that they would be asked to complete two pre-test and two post-test
questionnaires that had been developed to evaluate (a) perceptions toward people with
addiction and (b) perceptions toward a specific relative with addiction. Both
questionnaires were administered to family members by the PI. The pre-test
questionnaire and a demographic survey were administered before the FBT session and
the post-test questionnaires were administered after the FBT session on the same day.
Family members were informed that there was no obligation to participate in this study
and that they were free to withdraw at any time without affecting their participation or
their relative’s participation at the Pima County Juvenile Court Center. A copy of their
right to privacy and participation was signed by them and the PI prior to data collection
and before FBT class began (See Appendix A-1a).
Recruitment of the Control Group
The control group was found to be eligible for this study if they were age 18 years
or older, and members of The KARE Center. Family members in the control group read a
flyer on the day that they arrived for a support meeting at KARE (see Appendix A-2).
Upon arriving at the KARE Center on Tuesday morning for the support meeting,
family members met with the PI. The PI explained that the purpose of the study was to
examine family members’ perceptions of people with addiction and of a specific relative
with addiction. Family members were advised that they would be asked to complete two

59
pre-test and two post-test questionnaires that had been developed to evaluate (a)
perceptions about people with addiction and (b) perceptions about a specific relative with
addiction. Both questionnaires were administered to family members by the PI. The pre-
test questionnaire and a demographics questionnaire were administered on Tuesday
morning at a scheduled weekly support group meeting and the post-test questionnaires
were administered on the same day, following the Tuesday morning support group
meeting. Family members were advised that there was no obligation to participate in this
study and that they were free to withdraw at any time without affecting their participation
or their relative’s participation at the KARE Center. A copy of their right to privacy and
participation was signed by the family members and the PI on Tuesday morning, before
administering the pre-test (See Appendix A-2a).
Procedure
Pre-test questionnaires and post-test questionnaires were administered to the
treatment group and control group. A demographic questionnaire was administered to
both groups at the same time that the pre-test questionnaires were administered. The
demographic questionnaires included questions regarding general information about
participants in each group (i.e., the experimental group and the control group). The
treatment group received family-based treatment and completed two post-test
questionnaires immediately after the session. The control group did not receive FBT, but
they completed two post-test questionnaires immediately after their regular meeting at
KARE. Every effort was made to ensure that both groups were similar (i.e., recruitment

60
of participants, explanation of the study, administration of the pre-test/post-test
questionnaires, and family members of a relative with addiction) (see Appendix C).
Step one. Before family members were selected, the PI met with therapists at
PCJCC to discuss the research protocol, review the participant eligibility requirements
(i.e., age 18 or older, familymembers who have a relative with addiction, and are
involved with PCJCC), and to determine the family members who were eligible to
participate in the study. Similarly, the PI met with staff at the KARE Center to discuss
the research protocol, review the eligibility requirements (i.e., age 18 or older, family
members who have a relative with addiction, and are attending some type of support
group at the KARE Center due to a relative with addiction), and to determine the family
members who were eligible to participate in the study.
Step two. The PI met with the families at PCJCC before beginning the FBT
sessions and at The KARE Center on Tuesday morning, before the weekly support group
to discuss protocol, timelines, procedures and confidentiality, and to obtain signatures on
consent forms according to IRB requirements.
Step three. At the beginning of the FBT session, and immediately after meeting
with the PI, the family members at PCJCC completed one demographic questionnaire and
two pre-test questionnaires that were administered prior to the FBT class. Likewise, on
Tuesday morning, after meeting with the PI, family members from The KARE Center
61
completed one demographic questionnaire and two pre-test questionnaires that were
administered before their weekly support group. The instructions included a request for
the family members to provide a memorable identification number at the top left hand
side of each questionnaire. Example: 0315 (birth month and day) TIL (first three letters
of pet/place/etc…).
Step four. Family members from PCJCC completed two post-test questionnaires
that were administered after the FBT session and family members from The KARE
Center completed two post-test questionnaires that were administered following their
regular support group meeting. The instructions included a request for family members
to provide the same memorable identifier that they used on each questionnaire.
Research Design
The effects of FBT on participants’ (i.e., family members) perceptions of and
beliefs about people in general with addiction and a relative with addiction were explored
in this study. Participants in this study were chosen from a convenience sample rather
than at random, therefore, this was a quasi-experimental design. This quasi-
experimental design involved collecting data from a convenience group (i.e., treatment
group) who received FBT and collecting data from a convenience group (i.e., control
group) that did not receive FBT. A Quasi-experimental design typically imposes an
intervention such as the FBT, on a group of participants in the interest of observing the
response and measuring a cause and effect relationship between participant responses

62
(pre-test and post-test). In this study, the participants were a convenience sample and
either received brief family-based treatment, or did not. The goal was to measure whether
family members changed their perceptions (i.e., attitudes) toward people in general with
addiction and toward a specific relative with addiction pre- and post- FBT (i.e., the
intervention).
The control group in this study augmented the integrity of the experiment by
isolating the attitudes of family members in order to come to a conclusion about changes
in perceptions (i.e., attitudes) from pre-test questionnaire to post-test questionnaire. The
control group design used participants who were similar to the experimental group but
who were not subjected to the intervention process and compared them with the
experimental group (who were subjected to the intervention process) to test a causal
hypothesis (Leedy, 1993). Every attempt was made to ensure that the control and
experimental groups were identical in all relevant ways (i.e., recruitment, explanation of
the study, administration of the pre-test/post-test questionnaire, and family members of a
relative with addiction) except that the experimental group received FBT (i.e., the causal
agent) and the control group did not receive the intervention. Therefore, if the suspected
causal agent (i.e., FBT) was actually a causal factor of some event (i.e.,
perception/attitudes change), then that event should have manifested itself more
significantly in the experimental than in the control group. For example, if “C” causes
“E”, when we introduce “C” into the experimental group but not into the control group,
we should find “E” occurring in the experimental group at a significantly greater rate than

63
in the control group. Significance is measured by relation to chance: if an event is not
likely due to chance, then its occurrence is significant (Leedy).
Instruments
The instruments that were used to measure family members’ general perceptions
toward addiction and their perceptions toward a specific relative with an addiction were
based on the Attitudes Measurement: Brief Scales (AMBS). The original AMBS was
developed by the National Centre for Education and Training on Addiction, Flinders
University, Adelaide, Australia (NCETA, 2006) (see Appendix B for the original). The
original AMBS utilized a 5-point, 9-item Likert-type scale. Number 7 on the scales was
inadvertently omitted on the original AMBS (NCETA). The 9-item scales were designed
to assess health care workers attitudes and beliefs regarding their judgments about people
with addictions and their deservingness of treatment. Examples of responses on the
scales range from: 1 = not at all responsible to 5 = very responsible; 1 = not at all angry
to 5 = very angry; 1 = not at all disappointed to 5 = very disappointed; and 1 = not at all
concerned to 5 = very concerned.
Key elements in the original instrument include five scales: (a) Responsibility, (b)
Negative Affect, (c) Positive Affect, (d) Deservingness, and (e) Entitlement. The
questions associated with each scale are located in Appendix C. According to the
researchers at NCETA (2006), three major beliefs influence judgments or attitudes: (a)
responsibility for an outcome (i.e., if a person studies hard for a test and makes a good
grade, it’s understood that he or she is deserving of the good grade), (b) relationship

64
between a person’s behavior and an outcome (i.e., positive behavior leads to a person
receiving a reward for his or her behavior and negative behavior leads to the person
receiving a penalty for his or her behavior), and (c) attitudes toward the person (i.e.,
positive feelings towards the person often leads to them being in receipt of more
sympathy and concern and deservingness of treatment, whereas negative attitudes toward
the person is likely to result in them being the recipients of disapproval and anger,
thereby resulting in poorer quality of care).
The AMBS, according to the NCETA research team, were primarily designed for
educators and trainers who address alcohol or drug related issues in their training courses.
The scales are used to assess attitudes and beliefs related of healthcare workers, but can
be adapted for use with other populations in the field of addiction (NCETA, 2006).
For the current study, the following revisions were made: one AMBS
questionnaire, as revised for the current study (i.e., General Perceptions toward People
with Addiction), included the eight questions that were specific to perceptions toward
people in general with addiction (see Appendix B-2). This instrument focused on family
member’s attitudes/perceptions toward people in general with addiction. The word
“attitudes” was changed to “perceptions” because there was a concern by committee
members’ that the word attitudes would influence family members’ responses in a
negative way. The questions on B-2 were also revised and renumbered for accuracy and
the instructions to the participants were revised to ask them to respond to items based on
their perceptions toward people in general with addiction.

65
A second revised AMBS questionnaire (i.e., Perceptions toward a Specific
Relative with Addiction) was revised for the current study and included eight questions
that focused on perceptions of family members toward a specific relative with addiction.
As previously stated, the word “attitudes” was changed to “perceptions.” Items were
renumbered for accuracy and instructions to participants were revised so as to focus on
perceptions toward a specific relative with addiction (see Appendix B-3).
The questionnaires were color-coded for clarity (i.e., to identify that they are two
separate instruments). For example, the pre-test/post-test questionnaire used to examine
family members’ perceptions toward people in general with addiction (AMBS: General
Perceptions toward People with Addiction) were color-coded in light blue and the pre-
test/post-test questionnaires used to examine family member’s perceptions toward a
relative with addiction (AMBS: Perceptions toward a Specific Relative with Addiction)
were color-coded in light grey. To learn more about the participants in this study, family
members were asked to complete a demographic questionnaire that focused on several
personal characteristics, such as, the age and gender of the relative with addiction, and
the income, ethnicity, and gender of the family member/participant (see Appendix B-4).
All questionnaires included a participant identification code on the left hand corner of the
page. For Spanish speaking/reading participants, the AMBS was translated to a paper
pre-test/post-test questionnaire by a certified Spanish translator.

66
Scoring the AMBS
The AMBS is scored for five scales: Responsibility, Negative Affect, Positive
Affect, Deservingness, and Entitlement. For an explanation of how the AMBS was
originally scored see Appendix C-1. For the purpose of this study the Responsibility
scale on the AMBS was calculated in a different way than the original. On the
Responsibility scale in the original AMBS, item one is reverse scored. In this current
study, however, the first item on the Responsibility scale was not reverse scored because
the wording did not seem clear. In particular, the first question asked the respondent to
circle to what extent challenges in ones life were likely to be responsible for people or a
relative’s addiction. The respondent had five choices ranging from (1) not responsible at
all to (5) very responsible. If the respondent chose (1) not responsible at all, it would be
reverse scored, thereby indicating that the person was (5) very responsible for his or her
addiction. Although the question was confusing, and even though it was not reverse
scored, a positive correlation was found after running an SPSS analysis. This
indicated that respondents most likely saw challenges as personal, which correlated with
item number two on the responsibility scale. The remaining four scales, (i.e., Negative,
Positive, Deservingness, and Entitlement) were all scored according to the original
AMBS.
Piloted Study of the AMBS
To better understand whether the two revised instruments (i.e., AMBS: General
Attitudes toward People with Addiction and AMBS: General Perceptions toward a

67
Specific Relative with Addiction) would measure what is intended for this study and
whether the demographic questionnaire was adequate for this study, a pilot test was
conducted by the PI with 10 participants who had a relative or significant other with
addiction. The following was learned from the pilot test. There was a need for clearer
instructions for completing the pre/post test (i.e., change the wording to direct the
participant to “circle the number that best fits his or her perceptions). In the original
AMBS, item number 7 was omitted; for the current study, items on the AMBS were
numbered accurately. There was a broad range of responses; however, most responses
were more positive than negative. This broad range is an indication that the AMBS
appears to allow for differing responses regarding attitudes toward people in general with
addiction and attitudes toward a specific relative with addiction. A broad range indicates
that the AMBS is more likely to achieve variance which is important for use with the
ANOVA (Johnson & Christensen, 2004). There was also a need to develop an identifier
for the individual participants that would be used from pre-tests to post-tests. The
following identifiers were suggested, birth month and day, plus the first three letters of a
pets’ name (e.g., 0130taz). Lastly it was learned that there was a need to insert other
categories in the demographics to include, niece, nephew, and combine friend and
significant other into one category.
Analysis
The data were analyzed to determine if family members’ (a) perceptions toward
people in general with addiction changed from pre-test to post-test and perceptions

68
toward a specific relative with addiction changed from pre-test to post-test (for the family
members in the treatment group at Pima County Juvenile Court Center) and (b)
perceptions toward people in general with addiction and a relative with addiction changed
for family members in the control group (who did not receive FBT) at The KARE Center
from pre-test to post-test.
A three-way Analysis of Variance (ANOVA) was used to compare the three
effects in the study (see Chapter 4, Results). The ANOVA tests differences in means (for
groups or variables) for statistical significance (Johnson & Christenson, 2004). This is
accomplished by partitioning the total variance into the components that are due to true
random error and the components that are due to differences between means. These latter
variance components are then tested for statistical significance. If not significant (i.e., no
change occurs due to the treatment), the null hypothesis is retained. If a change occurs
due to the treatment, however, the alternative hypothesis is accepted (Statsoft, 2008). For
analysis in this study, the p-value was set at .05 for significance.
Dependent and independent variables: the variables that were measured (e.g.,
perceptions toward people in general with addiction and a specific relative with
addiction) were the dependent variables. The variable that was manipulated or controlled
(e.g., FBT) was the independent variables.
69
CHAPTER FOUR
FINDINGS
The current research is an investigation of the efficacy of brief family-based
treatment in changing family members’ attitudes toward people in general with addiction
and attitudes toward a specific relative with addiction after a brief family-based treatment
session. As noted in chapter one, family members’ beliefs about addiction and their
feelings toward a specific relative with addiction often play an essential part in the
psychological aspect of the recovery process of the relative with the addiction. The
purpose of the current study was to examine whether brief family-based treatment
impacts family members’ attitudes toward people with addiction in general and toward a
specific relative with addiction. The following research questions were addressed in this
study:
RQ1: Is there a change in family members’ attitudes toward people in general
with addiction from pre-family-based treatment to post-family-based treatment?
RQ2: Is there a change in family members’ attitudes toward a specific relative
with addiction from pre-family-based treatment to post-family-based treatment?
Two groups were surveyed (i.e., treatment, control). One group (treatment)
received a brief two hour family-based treatment session and one group (control) did not
receive a brief family-based treatment session. Family members in this study, from both
groups, completed a demographic survey and two Attitudes Measurement Brief Scales
(AMBS) pre-test questionnaires and two (AMBS) post-test questionnaires (i.e.,

70
perceptions toward people in general with addiction and perceptions toward a specific
relative with addiction). The treatment group completed the demographic survey and
pre-test questionnaires before a brief family-based session and the post-test
questionnaires immediately after the brief family-based session. The control group
completed the demographic test and pre-test questionnaires before a support group
meeting and the post-test questionnaires immediately after the support meeting. The
results of the pre and post tests were calculated using SPSS (Incorporated, #17) and are
described below.
Results
Three-way analyses of variance (ANOVA) were conducted to address three
factors. Factor A, was to measure treatment vs. control group; Factor B, was to measure
pre-tests vs. post-tests for each instrument; and Factor C, was to measure attitudes
regarding people in general versus relatives with addiction. The five scales in the AMBS
(i.e., Responsibility, Negative, Positive, Deservingness, and Entitlement) were used to
determine whether family members’ attitudes toward people (in general) with addiction
changed from pre-test questionnaire to post-test questionnaire, and whether family
members’ attitudes toward a specific relative with addiction changed from pre-test
questionnaire to post-test questionnaire. As stated earlier, two groups were surveyed, the
treatment group (n = 19) received a brief two hour family-based treatment session and the
control group (n = 22) did not receive a brief family-based treatment session. The results

71
of the ANOVA for the five scales are listed in Tables 1-5 and the means for each of the
five scales are illustrated in Figures 1-5.
Responsibility Scale
Two questions on the Responsibility scale measured the extent to which
respondents hold people or a relative responsible for his or her addiction. The ANOVA
results for the Responsibility scale are reported in Table 1, where TX represents the
Treatment group, CG represents the Control Group, People represents people in general
with addiction, and Relative represents a specific relative with addiction.
Table 1
Analysis of Variance for the Responsibility Scale
Source df F Parial η p
Between subjects
TX vs. CG (A) 1 0.367 .01 .55 S within-group error 39 (3.398)
Within subjects
Pre vs. Post (B) 1 1.452 .04 .24
A X B 1 1.198 .03 .28
A X B within-group error 39 (0.433)
People vs. Relative (C) 1 0.023 .00 .88
A X C 1 2.318 .06 .14

72
Table 1 (continued)
Analysis of Variance for the Responsibility Scale
Source df F Parial η p
Within subjects
A X C within-group error 39 (0.542)
B X C 1 0.110 .00 .74
A X B X C 1 0.433 .01 .51
A X B X C within-group error 39 (0.264)
Results displayed on Table 1 reveal that the three-way ANOVA interaction
(AXBXC) was not significant. The scores between Pre and Post tests of the
Responsibility Scale did not change after a brief two hour family-based treatment session.
There was also no TX vs. CG, and Pre-test vs. Post-test (AXB) or TX vs. CG, and People
vs. Relative (AXC) interaction, therefore no significant effects or interactions for the
Responsibility scale were found. The findings revealed that the perceptions of the
treatment group and control group did not change from pre-test to post-test (i.e., brief
family-based treatment) with regard to holding people or a relative responsible for his or
her addiction. Thus, the null hypothesis was retained.
Figure 1 represents means for the Responsibility scale. The mean results are
reported on the bottom line of the bar graph and the line segments at the top represent the
confidence interval parameters.

73
Figure 1. Responsibility Scale Means
Negative Scale
The Negative scale has two questions that measures the degree to which
respondents experience anger or disappointment toward people or a relative with
addiction. A higher score represents more anger and disappointment toward someone
with addiction. ANOVA results for the Negative scale are reported in Table 2.
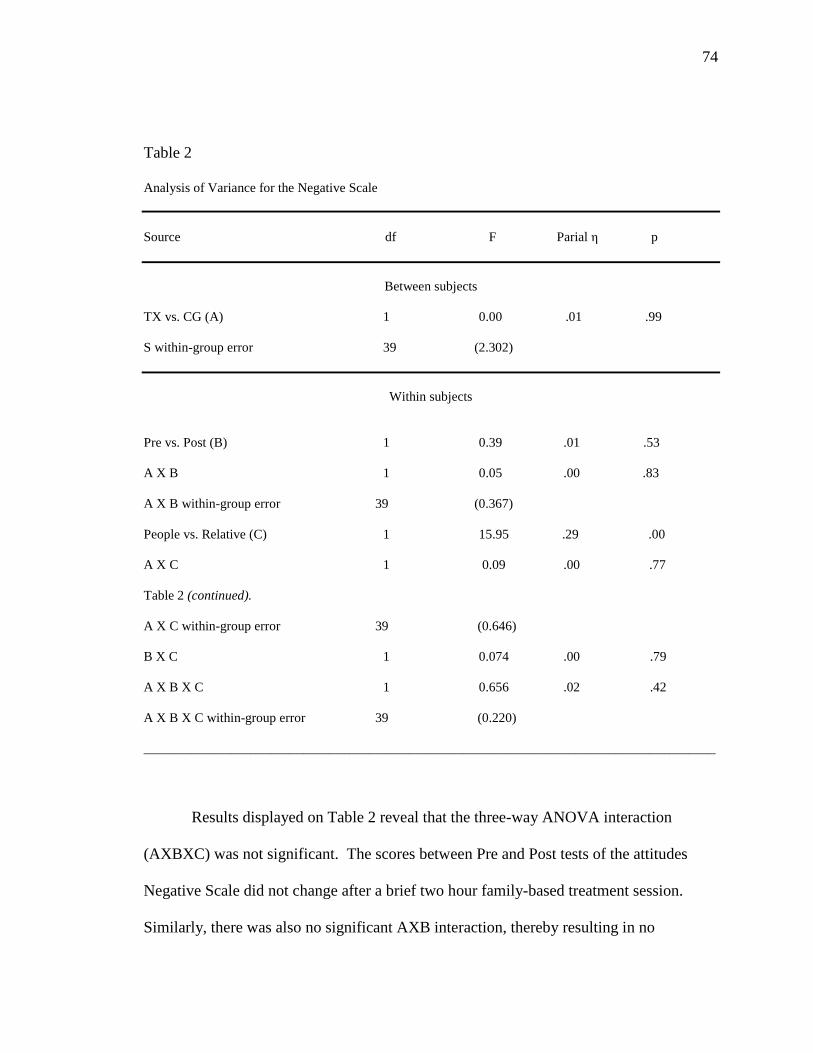
74
Table 2
Analysis of Variance for the Negative Scale
Source df F Parial η p
Between subjects
TX vs. CG (A) 1 0.00 .01 .99 S within-group error 39 (2.302)
Within subjects
Pre vs. Post (B) 1 0.39 .01 .53
A X B 1 0.05 .00 .83
A X B within-group error 39 (0.367)
People vs. Relative (C) 1 15.95 .29 .00
A X C 1 0.09 .00 .77
Table 2 (continued).
A X C within-group error 39 (0.646)
B X C 1 0.074 .00 .79
A X B X C 1 0.656 .02 .42
A X B X C within-group error 39 (0.220)
______________________________________________________________________________________
Results displayed on Table 2 reveal that the three-way ANOVA interaction
(AXBXC) was not significant. The scores between Pre and Post tests of the attitudes
Negative Scale did not change after a brief two hour family-based treatment session.
Similarly, there was also no significant AXB interaction, thereby resulting in no

75
significance difference between the TX vs. CG and no significant AXC interaction
between the TX vs. CG and People vs. Relative after a brief family-based treatment
session was introduced to the treatment group. Significance was found, however, on the
Negative scale (factor C) with regard to family members’ attitudes toward people with
addiction compared with family members’ attitudes toward a relative with addiction (i.e.,
People vs. Relatives). An F value of (F (1, 39) = 15.95, p < .001) was observed. Both
the treatment group and the control group had significantly more negative attitudes (i.e.,
angrier and more disappointment) toward a specific relative with addiction than toward
people in general with addiction.
The means for the Negative scale are reported in Figure 2. The mean results are
reported on the bottom line of the graph and the line segments at the top represent the
confidence interval parameters.

76
Figure 2. Negative Scale Means
Positive Scale
The Positive scale has two questions that examine the intensity to which
respondents convey concern or sympathy toward people or a relative with addiction.
ANOVA results for the Positive scale are reported in Table 3.

77
Table 3
Analysis of Variance for the Positive Scale
Source df F Parial η p
Between subjects
TX vs. CG (A) 1 4.02 .09 .05 S within-group error 39 (2.568)
Within subjects
Pre vs. Post (B) 1 0.22 .01 .66
A X B 1 0.03 .00 .87
A X B within-group error 39 (0.326)
People vs. Relative (C) 1 31.67 .45 .00
A X C 1 5.80 .13 .02
A X C within-group error 39 (0.319)
B X C 1 0.342 .01 .56
A X B X C 1 0.016 .00 .90
A X B X C within-group error 39 (0.224)
Results displayed on Table 3 reveal that the three-way ANOVA interaction
(AXBXC) was not significant. The scores between Pre and Post tests of the Positive
Scale did not change after a brief two hour family-based treatment session. Therefore the
null hypothesis was retained. Significance was found (i.e., F value of (F (1, 39) = 5.80,

78
p = .021) on the Positive scale with regard to the TX vs. CG and People vs. Relative
interaction (AXC), demonstrating that both the control group and treatment group were
less concerned and sympathetic toward people in general with addiction than for a
specific relative with addiction. Another main effect that was significant was the People
vs. Relatives interaction. An F value of (F (1, 39) = 31.67, p < .01) was found, indicating
that family members in the treatment group had more sympathy and concern (overall) for
a specific relative with addiction than did the control group. The reason for this response
is uncertain and may be due to the differences in demographic characteristics between the
treatment and control group. Further explanation about demographic
characteristics/differences will be discussed in Chapter 5 in the differences between
groups and limitations sections.
The means for the Positive scale are illustrated in Figure 3. The mean results are
reported on the bottom line of the graph and the line segments at the top represent the
confidence interval parameters.

79
Figure 3. Positive Scale Means
Deservingness Scale
One question on the Deservingness scale examines the extent to which
respondents believe that people or a relative with addiction are worthy of the same type
of medical treatment as people who are not addicted to drugs. ANOVA results for the
Deservingness Scale are reported on Table 4.

80
Table 4
Analysis of Variance for the Deservingness Scale
Source df F Parial η p
Between subjects
TX vs. CG (A) 1 7.88 .17 .01 S within-group error 39 (3.984)
Within subjects
Pre vs. Post (B) 1 0.22 .01 .64
A X B 1 0.35 .00 .85
A X B within-group error 39 (0.261)
People vs. Relative (C) 1 2.98 .07 .09
A X C 1 0.78 .02 .38
A X C within-group error 39 (0.264)
B X C 1 0.435 .01 .51
A X B X C 1 0.069 .00 .80
A X B X C within-group error 39 (0.133)
Results displayed on Table 4 reveal that the three-way ANOVA interaction
(AXBXC) was not significant. The scores between Pre and Post tests of the
Deservingness Scale did not change after a brief two hour family-based treatment
session. Therefore the null hypothesis was retained. Similarly, there was also no
significance found in the AXB or AXC interactions. Main effects (TX vs. CG), however,

81
were found to be significant with an F value of (F (1, 39) = 7.88, p = .01). The responses
of the treatment group were significantly higher than the control group. This indicated
that participants in the treatment group believed that people (i.e., people in general with
addiction) and a relative (i.e., specific relative with addiction) were more deserving of
treament for addiction than did the family members in the control group. This finding,
however, may have confines due to the varied demographic characteristics of the
treatment group and control group and will be discussed further in Chapter 5 in the
differences between groups and limitations sections.
The means for the Deservingness scale are illustrated in Figure 4. The mean
results are reported on the bottom line of the graph and the line segments at the top
represent the confidence interval parameters.

82
Figure 4. Deservingness Scale Means
Entitlement Scale
One question on the Entitlement scale examines the extent to which respondents
deem that people or a relative with addiction should be permitted to have the same type
of medical treatment as people who are not addicted to drugs. ANOVA results for the
Entitlement scale are reported in Table 5.

83
Table 5
Analysis of Variance for the Entitlement Scale
Source df F Parial η p
Between subjects TX vs. CG (A) 1 8.44 .18 .01 S within-group error 38 (4.449)
Within subjects
Pre vs. Post (B) 1 0.37 .01 .55
A X B 1 0.37 .01 .55
A X B within-group error 38 (0.245)
People vs. Relative (C) 1 1.78 .05 .19
A X C 1 0.51 .01 .48
A X C within-group error 38 (0.236)
B X C 1 4.80 .11 .35
A X B X C 1 1.022 .03 .32
A X B X C within-group error 38 (0.079)
Results displayed on Table 5 reveal that the three-way ANOVA interaction
(AXBXC) was not significant. The scores between Pre and Post tests of the Entitlement
Scale did not change after a brief two hour family-based treatment session. Therefore the
null hypothesis was retained. Similarly, there was also no significance found in the AXB
or AXC interactions. Main effects, however, were found to be significant regarding TX

84
vs. CG, with an F value of (F (1, 38) = 8.44, p = .01). The treatment group was
significantly higher than the control group with regard to beliefs that people in general
with addiction and a specific relative with addiction should be permitted to have the same
type of medical treatment as people/relatives who are not addicted to drugs. This effect
may be similar to the results found on the Deservingness scale since the definition is very
similar. Furthermore, as stated previously regarding the Negative, Positive, and
Deservingness scales, this deduction may be due to demographic characteristics and will
be discussed in further detail in Chapter 5 in the differences between groups and
limitations sections.
The means for the Entitlement scale are illustrated in Figure 5. The mean results
are reported on the bottom line of the graph and the line segments at the top represent the
confidence interval parameters.

85
Figure 5. Entitlement Scale Means
Demographic Characteristics
As noted in Chapter 3, this study used a convenience sample comprised of one
treatment group (n = 19) and one control group (n = 22). Demographic characteristics of
both groups are listed in Table 6.

86
Table 6 Demographic Characteristics ______________________________________________________________________________________ Demographic Treatment Group Control Group ______________________________________________________________________________________ Gender of Participant
Female
73% 95%
Male 27% 5% Age of Relative with Addiction
15
32%
16
26%
17
42%
19 – 22
9%
30 – 45
36%
46 – 63
23%
Did not answer question 32% Relationship of Participant to Relative with Addiction
Father
26% 5%
Mother
58% 14%
Grandmother
16% 14%
Spouse
14%
Sister
14%
Son
9%
Cousin
5%
Niece
5%
Did not answer question 47% 22%
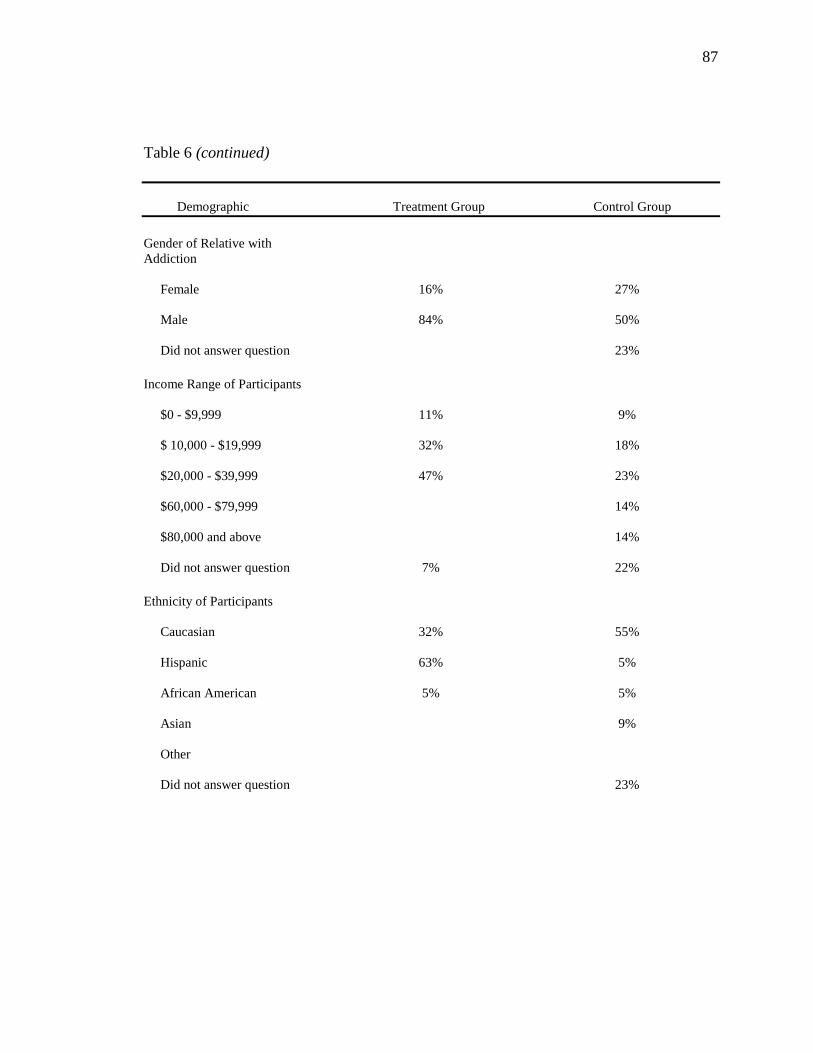
87
Table 6 (continued) Demographic Treatment Group Control Group
Gender of Relative with Addiction
Female
16% 27%
Male
84% 50%
Did not answer question 23% Income Range of Participants
$0 - $9,999
11% 9%
$ 10,000 - $19,999
32% 18%
$20,000 - $39,999
47% 23%
$60,000 - $79,999
14%
$80,000 and above
14%
Did not answer question 7% 22% Ethnicity of Participants
Caucasian
32% 55%
Hispanic
63% 5%
African American
5% 5%
Asian
9%
Other
Did not answer question 23%

88
Table 6 (continued) Demographic Treatment Group Control Group
Age of Participants
18-28
5% 9%
29-38
26% 0
39-49
47% 9%
50-64
15% 36%
65 and above
23%
Did not answer question 5% 23% Note: Percentages do not always equal 100% due to rounding.
Summary of Findings
With regard to the two research questions posed in this study, there were no
significant differences from pre-test to post-test on any of the AMBS scales for the
treatment or control group. Therefore, the null hypothesis was retained for both specific
research questions. Significance was found however, on the Negative scale within
subjects. Both the treatment group and control group had more negative attitudes (i.e.,
more anger and more disappointment) toward a relative with addiction than toward
people in general with addiction. On the Positive scale, significance was again found
within subjects. The treatment group and control group had more positive attitudes (i.e.,
concern and sympathy) toward a specific relative with addiction than toward people in
general with addiction. The family members’ in the treatment group, however, had
significantly more concern and sympathy for a specific relative than did the control

89
group, both pre-test and post-test. Regarding the Deservingness scale, family members in
the treatment group believed more so than the family members in the control group that
all people with addiction deserve (i.e., are worthy of) medical treatment whether they are
a specific relative or people in general. Finally, regarding Entitlement, the treatment
group’s responses were significantly higher than the control group’s responses with the
treatment group asserting that people with addiction and a relative with addiction should
be entitled to (i.e., guaranteed) the same medical treatment as people who are not
addicted to drugs.

90
CHAPTER FIVE
DISCUSSION
This chapter provides a discussion of the results presented in Chapter 4 and
includes (a) a brief review of the methodology; (b) discussion of the findings, which
includes the differences in perceptions between people in general who have addiction
versus a specific relative with addiction, the findings regarding the differences between
the treatment and control group, and differences in demographic characteristics; (c)
limitations of this study; and (d) conclusions and recommendations.
Brief Review of the Methodology
The purpose of this study was to determine whether perceptions of family
members were changed after they participated in a brief family-based treatment session.
An attempt was made to address the practical limitations of comparable research
pertaining to attitudes/perceptions of family members toward people in general with
addiction and a specific relative with addiction with regard to brief family-based
treatment. A questionnaire format was used to obtain information regarding family
members’ attitudes toward people in general with addiction and a specific relative with
addiction. A small convenience sample of participants (n = 41) was included in this
study. Nineteen of the participants were from the treatment group and twenty-two were
from the control group.

91
Discussion of Findings
The result of this current study indicated that one brief family-based treatment
session did not contribute to significant changes in attitudes or perceptions toward people
in general with addiction or toward a specific relative with addiction. Because no
significance was found with regard to the two research questions, this study did not
support the hypothesis that attitudes and perceptions would change from pre-test to post-
test using the Attitudes Measurement: Brief Scales.
With respect to the AMBS, on the Responsibility scale, no significance difference
was found between the treatment group and control group concerning responsibility for
behavior whether it was people in general with addiction or a specific relative with
addiction, on either instrument. One reason may have been the scoring of the instruments
in this study. In the original AMBS the first question on the Responsibility scale was
reverse scored; however, in this current study the first question was not reverse scored.
The first question on the Responsibility scale asks specifically whether people or a
relatives’ addiction are related to life’s challenges. A family member may answer that
the challenges in the person’s life are not likely to be responsible for his or her addiction
(i.e., low score of 1). The opposite however, would be reported (i.e., high score of 5)
when the answer is reverse-scored. Therefore, reverse scoring would indicate that
challenges in one’s life are more likely to contribute to his or her addiction.
Consequently, had the first question been reverse scored, it may have resulted in a
significant finding on this scale.
92
With regard to the remaining scales, significance differences were found on the
Negative and Positive scales within subjects (People vs. Relative) and on the Positive,
Deservingness, and Entitlement scales between subjects (TX vs. CG). These findings will
be discussed in the following sections.
Differences in Perceptions between People vs. a Specific Relative
This section will include a discussion about the ANOVA results and the
differences in perceptions between people in general with addiction and a specific
relative with addiction on the Negative and Positive scales. It is interesting to note that
on the Negative scale, family members’ tended to be less angry and less disappointed
toward people in general with addiction and angrier and more disappointed toward a
specific relative with addiction for both the treatment and the control group. It is possible
that family members’ responses were due to their close relationship to their relative with
addiction and their lack of closeness to people in general with addiction. Conversely, on
the Positive scale, the opposite was found with regard to concern and sympathy. Family
members’ attitudes in both groups tended to be less sympathetic and less concerned about
people in general with addiction and more sympathetic and more concerned toward a
specific relative with addiction from pre-test to post-test. While this differs from their
response on the Negative scale, it is again most likely due to their close proximity to a
relative with addiction and their concern for his or her wellbeing.
On the two remaining scales (i.e., Deservingness and Entitlement), no
significance difference was found between people versus a relative with addiction. This

93
is a potential indication that family members’ did not distinguish between a specific
relative or people in general with regard to receiving medical care. Significance was
found on the Deservingness and Entitlement scales as well as the Positive scale with
regard to differences between the treatment group and control group and will be
discussed in the next section.
Differences between the Treatment and Control Group
This section will include a discussion about the differences between the two
groups (i.e., treatment vs. control) with regard to the three scales mentioned above (i.e.,
Positive, Deservingness, and Entitlement). Also discussed in this section will be the
speculation about the demographic characteristics and how they may have influenced the
findings.
Regarding the Positive Scale, family members in the treatment group had more
concern and sympathy for people in general with addiction and significantly more
concern and sympathy for a specific relative than did the control group, at both pre-test to
post-test. One reason for these findings may be due to the differences in demographic
characteristics among the treatment and control groups. For instance, the treatment group
may have been more sympathetic and concerned because they and their relative with
addiction were younger and did not have the long-term experience with addiction that
perhaps the control group had. In addition, older family members may have lived with an
adult relative with addiction longer and therefore may have experienced more
disappointments and unmet expectations.

94
Similar to the Positive scale, main effects for both the Deservingness scale and
Entitlement scale were found to be significantly different between the treatment group
and control group concerning worthiness of treatment and eligibility of treatment. Once
again, the treatment group had higher scores than the control group on these two scales,
indicating that the treatment group felt that people in general and a specific relative with
addiction were more deserving and entitled to help than did the control group. As stated
earlier, this deduction may be due to differences in demographic characteristics. For
example, members in the treatment group had lower incomes than the control group.
Perhaps members in the control group had used their resources to finance treatment
options that were not successful in the past and were now somewhat guarded toward a
specific relative’s worthiness and appropriateness of receiving more treatment. Also,
because the participants in the control group were older and had relatives with addiction
who were older, they may have had more experience overall with addiction and were not
hopeful of seeing positive results from any new therapy interventions. Therefore, they did
not see the need for more treatment.
Inconsistencies in demographics, such as the ones discussed above, most likely
affected the results of the current study. As a result, it is important to discuss in detail the
other differences that were found between the treatment and control group.
Differences in Demographic Characteristics
Several demographic characteristics were examined in this study. With regard to
gender characteristics of the participants, five participants (10%) in the treatment group

95
were male and fourteen were female, while in the control group one participant was male
and sixteen were female. It was unclear whether gender had any impact on the study.
Age of the relative with addiction also was unique with 100 % of participants in
the treatment group reporting the age of their relative with addiction to be fifteen to
seventeen. Relatives in the control group, on the other hand, reported ages of relatives to
be nineteen to sixty-three with more than 50% over the age of thirty. Age of the relative
may have contributed to some inequality between both groups. For example, relatives in
the control group were older and may have been dealing with addiction problems for a
longer period of time than relatives in the treatment group who were younger. As a
result, the participants in the control group may have had less sympathy and concern
toward people and a relative with addiction due to history. Many of the treatment
groups’ relatives were younger and recently incarcerated and this may also have
contributed to the treatment group feeling more concern for their relative.
Another difference between the two groups is that the control group may have
regularly attended Tuesday support group meetings, whereas the treatment group had
only a brief two hour session. These differences in support may have influenced the
perceptions of partifcipants in each group with regard to responsibility, negative, postive,
deservingness, and entitlement toward people in general and a specific relative with
addition.
Disparity was also found between both groups with regard to the relationship of
participants/family members and their relative with addiction. In the treatment group,
family members were either a mother, father, or grandmother, whereas in the control

96
group, family members were mixed (i.e., father, mother, grandmother, spouse, son,
cousin, sister, niece). Having closer family ties with someone with addiction has been
shown to improve the outcomes for that person. In this instance, family members in the
treatment group may have had closer ties and as a result tended to be more concerned and
sympathetic and to believe that their relative was more deserving and entitled to
treatment. What was not clear, however, was why the treatment group felt that people in
general were also more deserving and entitled to treatment, than did the control group.
Income range also differed, with all participants in the treatment group reporting
incomes of $39,999 or less and the control group reporting incomes of up to $80,000 and
above. It is thought that perhaps participants in the control group also had a higher level
of education because they reported a higher income. Having more education may also
have contributed to less sympathy and concern. Perhaps the participants in the control
group had found ways to use their resources to help cope more effectively with their
situation. Regarding ethnicity, a high percentage of participants in both groups were
Caucasian (i.e., treatment group – 32% and control group – 55%). In the treatment
group, however, 63% of participants reported being Hispanic while only 5% reported
being Hispanic in the control group. Ethnicity may have caused discrepancies in the
findings due to different beliefs about addiction. Family members who grow up in
households may not have the same perceptions or attitudes toward people in general or a
specific relative with addiction problems. Finally, with regard to age of the participants,
a majority of the responders in the treatment group fell within the age ranges of twenty-
nine to forty-nine whereas a majority of the responders in the control group fell within
97
the age ranges of fifty to sixty-five and above. As noted earlier, age and experience with
addiction may have played an important role in the inconsistencies found within the
results of this study. With all of this in mind, it is very likely that these differences may
have contributed to a variety of limitations and bias within the study.
Limitations
Good experimental design involves eliminating as many of the possible
confounding variables as possible. Although the task of designing this research was
relatively logical and fairly simple, there were several potential confounding variables
that most likely contributed to limitations in the study. First, this was a convenience
sample with only a small number of participants (n = 41). Six of the twenty-five family
members in the treatment group decided not to participate in the study. Five of the
twenty-two family members in the control group did not complete the demographic
survey, stating that sharing personal information about themselves or a relative with
addiction was problematic for them and one family member in the control group did not
answer all of the survey questions. As a result, the group was not well represented and
not generalizable. Second, the recruitment process may have been distracting, leading to
unwillingness of participation. For example, one family member in the treatment group
became very upset and vocal during the recruitment process. This set a negative tone for
the other participants, resulting in four family members declining the offer to contribute
to the study. Third, there was no manualized treatment protocol for the treatment group.
Therefore, it would be difficult for a researcher to replicate this study without a step-by-

98
step guide. This is not a reflection on the program, but a weakness of the research design
because it is not possible to describe clearly the treatment that the participants received.
It should be noted, however, that no manualized format was discussed in Chapter Two.
Additionally, while brief family-based treatment at PCJCC did focus on many of the
tenets of FBT, discussed in Chapter Two, only one two hour session was offered to the
treatment group as opposed to the research that suggests numerous sessions are more
effective. Several FBT modalities discussed in Chapter Two recommended at least six or
eight-one hour sessions in succession (Bergin & Garfield, 1994; Cannon & Levy; Cottrell
& Boston, 2002; Connors et al.; English, 2000; Jay & Jay, 2000; Liddle; McLendon et al.
2005; Miller et al.1999; O’Farrell et al.1995; Santisteban et al. 2003). Consequently, this
observer may postulate that having only one brief two-hour session is not adequate time
to provide a therapeutic brief family-based session that will result in a meaningful change
in perceptions toward people in general with addiction and a specific relative with
addiction. Furthermore, because there were a number of components in the treatment
readiness session at PCJCC, changing perceptions about addiction were only briefly
discussed. Fourth, the instrument used (i.e., Attitudes Measurement: Brief Scales) was
designed for use with healthcare workers and not family members. While the AMBS was
revised for use with this study, a more-well constructed scale designed with family
members’ issues in mind would have been more practical. In addition, there were some
difficulties with the scoring of the instrument. On the original AMBS, the first question
on the Responsibility scale, which questions whether the respondent feels that people or a
relatives’ “challenges in life” are responsible for his or her addiction, is meant to be

99
reverse scored, but was not reverse scored in the current study. It is likely that scoring it
like the original would have made some difference with regard to results on the
Responsibility scale and should be strongly considered for any future studies. Finally,
the fact that it was not possible to control the demographic characteristics of participants
(i.e., age, relationship to relative with addiction, income, and age of relative with
addiction) between participants in the treatment group and the control group, were also
limiting factors (see differences in demographic characteristics).
Conclusions and Recommendations
Despite the limitations of the current research, this study has offered an analysis
of the efficacy of brief family-based treatment in changing family members’ attitudes
toward people in general with addiction and family members’ attitudes toward a specific
relative with addiction. Family members’ responses to both questionnaires revealed no
significant impact on the efficacy of attending one brief family-based treatment in
changing family members’ attitudes toward people with addiction and attitudes toward a
specific relative with addiction after a brief family-based treatment session. The most
likely reason for this was due to several limitations (i.e., small sample size, short
treatment time, lack of control of demographic characteristics, and instrument
discrepancy). Despite the results, however, some significance was noted. Therefore,
more research into all aspects of brief family-based treatment should be explored so that
interventions can be studied for more effectiveness. For example, based on these
findings, implications for future research may include, (a) comparing results to shorter vs.

100
longer treatment sessions; (b) manualizing the treatment protocol and describing
precisely what the session will entail; (c) watching for selection bias by recruiting from
one site and randomly selecting participants, which will also ensure a more homogenous
sample; (d) sending out a descriptive flier in advance to ensure that participants are fully
aware of the study so that disagreements will not arise during the treatment session; (e)
running an analysis of the relationships between demographics and results and how they
are related to each of the scales to help identify why some participants’ answers are more
positive, and some are more negative; and (f) developing a more effective instrument that
focuses specifically on attitudes of family member’s toward people in general with
addiction and a specific relative with addiction.

101
APPENDIX A-1
RECRUITMENT FLYER FOR PCJCC (1 of 1)
PROJECT TITLE: THE EFFICACY OF FAMILY-BASED TREATMENT
Dear Pima County Juvenile Court Center Family Member:
You are being asked to participate in a valuable study conducted by Teresa Kolodny, Ph.D.
Candidate and the Primary Investigator (PI) for a study at the University of Arizona’s College of
Education Department of Special Education, Rehabilitation, and School Psychology.
The purpose of the study is to examine family member’s perceptions of addiction and
perceptions of a relative with addiction pre- and post- Family-Based Treatment (FBT). To
achieve results, two pre- and post-test questionnaires have been developed to evaluate (1)
perceptions of addiction and (2) perceptions of a relative with addiction. Both surveys will be
administered to family members by Teresa. By comparing the pre-test questionnaires with the
post-test questionnaires, Teresa will be able to evaluate whether family member’s perceptions of
addiction and family member’s perceptions of a relative with addiction have changed. Please
understand that you are under no obligation to participate in this study and are free to withdraw at
any time without causing bad feelings or affecting your participation or your relative’s
participation at Pima County Juvenile Court Center.
Thank you very much for volunteering; your participation is greatly appreciated.
Sincerely,
Teresa Kolodny, Ph.D. Candidate

102
APPENDIX A-1a
SUBJECT INFORMED CONSENT FORM FOR PCJCC
AUTHORIZATION
Before giving my consent by signing this form, the methods, inconveniences, risks, and
benefits have been explained to me and my questions have been answered. I may ask
questions at any time and I am free to withdraw from the project at any time without
causing bad feelings or affecting my participation or my relative’s participation at Pima
County Juvenile Court Center. If new information develops during the course of this
study which may affect my willingness to continue in this research project, it will be
given to me as it becomes available. This consent form will be filed in an area designated
by the Human Subjects Committee with access restricted by the Principal Investigator,
Teresa Kolodny, Ph.D. Candidate at (520) 370-9032 or authorized representative of the
University of Arizona’s College of Education Department of Special Education,
Rehabilitation and School Psychology. I do not give up any of my rights by signing this
form. A copy of this signed consent form will be given to me.
___________________________________ ______________________________
Subject’s Name (printed) Signature
____________________________________
Date

103
APPENDIX A-2
RECRUITMENT FLYER FOR KARE
PROJECT TITLE: THE EFFICACY OF FAMILY-BASED TREATMENT
Dear KARE Center Family Member:
You are being asked to participate in a valuable study conducted by Teresa Kolodny, Ph.D.
Candidate and the Primary Investigator (PI) for a study at the University of Arizona’s College of
Education Department of Special Education, Rehabilitation, and School Psychology.
The purpose of the study is to examine family member’s perceptions toward addiction and
family member’s perceptions toward a relative with addiction. To achieve results, two pre- and
post- test questionnaires have been developed to evaluate (1) perceptions toward addiction and
(2) perceptions toward a relative with addiction. Both questionnaires will be administered to
family members by Teresa. By comparing the pre-test questionnaires with the post-test
questionnaires, Teresa will be able to evaluate whether family member’s perceptions toward
addiction and family member’s perceptions toward a relative with addiction have changed.
Please understand that you are under no obligation to participate in this study and are free to
withdraw at any time without causing bad feelings or affecting your participation or your
relative’s participation at the KARE Center.
Thank you very much for volunteering; your participation is greatly appreciated.
Sincerely,
Teresa Kolodny, Ph.D. Candidate
104
APPENDIX A-2a
SUBJECT INFORMED CONSENT FORM FOR KARE
AUTHORIZATION
Before giving my consent by signing this form, the methods, inconveniences, risks, and
benefits have been explained to me and my questions have been answered. I may ask
questions at any time and I am free to withdraw from the project at any time without
causing bad feelings or affecting my participation or my relative’s participation at the
KARE Center. If new information develops during the course of this study which may
affect either my willingness to continue in this research project, it will be given to me as
it becomes available. This consent form will be filed in an area designated by the Human
Subjects Committee with access restricted by the Principal Investigator, Teresa Kolodny,
Ph.D. Candidate at (520) 370-9032 or authorized representative of the University of
Arizona’s College of Education Department of Special Education, Rehabilitation and
School Psychology. I do not give up any of my rights by signing this form. A copy of this
signed consent form will be given to me.
___________________________________
Subject’s Name (printed)
___________________________________ _______________________________
Signature Date

105
APPENDIX B-1 ATTITUDE MEASUREMENT: BRIEF SCALES (ORIGINAL)
ATTTITUDES TOWARD ADDICTION
These scales should be used as part of the training course evaluation. It is recommended that participants complete the scales prior to training and also on completion of training. Comparison of the pre and post training score will indicate the extent to which attitude change has been achieved. The wording of the scales can be adapted in order to measure attitudes toward specific drugs (e.g. heroin, methamphetamines, alcohol, etc…)
1. To what extent are adverse life circumstances likely to be responsible for a person’s
problematic drug use? 1 2 3 4 5
Not responsible at all moderately responsible very responsible 2. To what extent is an individual personally responsible for their problematic drug use?
1 2 3 4 5 Not responsible at all moderately responsible very responsible
3. To what extent do you feel angry towards people using drugs?
1 2 3 4 5 Not angry at all moderately angry very angry
4. To what extent do you feel disappointed towards people using drugs?
1 2 3 4 5 Not at all disappointed moderately disappointed very disappointed
5. To what extent do you feel sympathetic towards people using drugs?
1 2 3 4 5 Not at all sympathetic moderately sympathetic very sympathetic
6. To what extent do you feel concerned towards people using drugs?
1 2 3 4 5 Not at all concerned moderately concerned very concerned
7. To what extent do people who use drugs deserve the same level of medical care as
people who don’t use drugs? 1 2 3 4 5
Not at all deserving moderately deserving definitely deserving
8. To what extent are people who use drugs entitled to the same level of medical care as people who don’t use drugs? 1 2 3 4 5 Not at all entitled moderately entitled definitely entitled
106
APPENDIX B-2 ATTITUDE MEASUREMENT: BRIEF SCALES (REVISED)
Pre-test____ Post-test____ CG____ TX____ Participant ID____________
GENERAL PERCEPTIONS TOWARD PEOPLE WITH ADDICTION
Please circle the number that most closely fits your general perceptions toward addiction.
1. To what extent are the challenges in ones life likely to be responsible for his or her difficult substance abuse?
1 2 3 4 5 Not responsible at all moderately responsible very responsible
2. To what extent do you feel an individual is personally responsible for his or her
problems with substance abuse? 1 2 3 4 5 Not responsible at all moderately responsible very responsible 3. Do you feel angry toward other people’s substance abuse? 1 2 3 4 5 Not angry at all moderately angry very angry
4. Do you feel disappointed toward other people’s substance abuse?
1 2 3 4 5 Not at all disappointed moderately disappointed very disappointed
5. How sympathetic do you feel toward other people with substance abuse problems? 1 2 3 4 5 Not at all sympathetic moderately sympathetic very sympathetic
6. How concerned are you toward other people’s substance abuse?
1 2 3 4 5 Not at all concerned moderately concerned very concerned
7. Do you feel that people who use drugs deserve the same level of medical care as
people who don’t use drugs? 1 2 3 4 5 Not at all deserving moderately deserving definitely deserving
8. Do you feel that people who use drugs are entitled to the same level of medical
care as people who don’t use drugs? 1 2 3 4 5 Not at all entitled moderately entitled definitely entitled

107
APPENDIX B-3 ATTITUDE MEASUREMENT: BRIEF SCALES (REVISED)
Pre-test____ Post-test____ CG___ TX___ Participant ID____________
GENERAL PERCEPTIONS TOWARD A SPECIFIC RELATIVE WITH ADDICTION Please circle the number that most closely fits your general perceptions toward a specific relative with addiction.
1. To what extent are the challenges in your relative’s life likely to be responsible for his or her difficult substance abuse?
1 2 3 4 5 Not responsible at all moderately responsible very responsible
2. To what extent do you feel your relative is personally responsible for his or her problems with substance abuse?
1 2 3 4 5 Not responsible at all moderately responsible very responsible
3. Do you feel angry toward your specific relative’s substance abuse?
1 2 3 4 5 Not angry at all moderately angry very angry
4. Do you feel disappointed toward your specific relative’s substance abuse?
1 2 3 4 5 Not at all disappointed moderately disappointed very disappointed
5. How sympathetic do you feel toward your specific relative with substance abuse?
1 2 3 4 5 Not at all sympathetic moderately sympathetic very sympathetic
6. How concerned are you toward your specific relative who has substance abuse issues?
1 2 3 4 5 Not at all concerned moderately concerned very concerned
7. Do you feel that your specific relative who uses drugs deserves the same level of medical care as people who don’t use drugs?
1 2 3 4 5 Not at all deserving moderately deserving definitely deserving 8. Do you feel your relative who uses drugs is entitled to the same level of medical care as people who don’t use drugs? 1 2 3 4 5 Not at all entitled moderately entitled definitely entitled

108
APPENDIX B-4 DEMOGRAPHIC QUESTIONNAIRE
Pre-test____ Post-test____ CG____ TX____ Participant ID___________ Please circle or write in the best answer to each question that best fits who you are.
1. What is your gender? Female Male
2. What is the age of your relative with addiction? _______
3. What is your relationship to your specific relative with addiction? I am his or her: Mother Son Father Daughter Stepmother Spouse Stepfather Brother Legal Guardian Sister Parent/significant other Nephew Foster Parent Niece Grandmother Cousin Grandfather Step-sibling Aunt Uncle 4. Please circle the best answer: My relative with addiction is a Male Female 5. Please circle the number that best fits your annual income. $0-$9,999 $10,000 - $19,999 $20,000 - $39,000 $40,000 - $59,000 $60,000 – $79,000 $80,000 - $ 99,000 $100,000 and above 6. Please circle all of the categories that apply. I am: Caucasian Hispanic Asian African-American Native-American Other _________ 7. Please circle the answer that best fits. My age is: 18 – 28 29 – 38 39 – 49 50 – 64 65 (+)

109
APPENDIX C
ATTITUDES MEASUREMENT: BRIEF SCALES (SCORING)
The AMBS was designed by The National Center for Education and Training on
Addiction (NCETA) for use by educators and trainers who address alcohol and substance
abuse concerns in their training programs (NCETA, 2006). For several years, NCETA
staff has worked on numerous projects relating to addiction. The most recent project was
in Adelaide in September of 2006 and involved research to examine the impact of
attitudes of healthcare providers toward patients with addiction.
One of the materials included in the project was the AMBS, a short survey that
measures attitudes of healthcare workers towards individuals who use heroin,
amphetamines, tobacco, and alcohol (see Appendix B-1). Participants completed the
AMBS prior to training and also at the completion of training. Comparison of the pre-
test and post-test results indicated whether, or to what extent there was a change in
attitudes of the healthcare worker towards people with addiction.
Scoring Instructions:
The AMBS is a short 8-item scale that assesses the attitudes of healthcare workers toward
people who use drugs (NCETA, 2006). Trainees complete a pre-test questionnaire before
training and a post-test questionnaire after training. Comparison of pre and post training
scores assess the extent of attitude changes. Questions one and two on the pre/post-test
entail responsibility. The responsibility scale measures how much a trainee/healthcare

110
APPENDIX C (continued)
worker feels that a person with addiction is responsible for his or her addiction.
Responses range from 1 to 5, with 5 being the most responsible for his or her addiction.
The sum of the two questions is averaged after the first question is reverse-scored.
Questions three and four assess how negative (i.e., angry or disappointed) the trainee is
toward the person with addiction. Responses on the Negative scale range from 1 to 5,
with 5 being very angry or very disappointed. The sum of the two questions is then
averaged to determine a score. Questions five and six measures to what degree a trainee
feels positive regard (i.e., concern or sympathy) toward a person with addiction.
Responses on the Positive scale range from 1 to 5, with 5 being very concerned or
sympathetic. The sum of the two questions on the Positive scale is then averaged to
determine a score. Question seven has to do with deservingness. The Deservingness
scale measures whether a trainee believes that a person with addiction is worthy of
receiving medical treatment. Responses on the Deservingness scale range from 1 to 5,
with 5 stating that the person is very deserving. Because there is only one question,
there is no need to average the score. Question eight has to do with entitlement. The
Entitlement scale assesses whether a trainee believes that a person with addiction should
be permitted medical treatment. Responses on the Entitlement scale range from 1 to 5,
with 5 asserting that the person with addiction is definitely entitled to medical treatment.
Similar to question seven, because there is only one question on the Entitlement scale,
there is no need to average the score (Freeman, 2008).

111
APPENDIX D
MAC TREATMENT READINESS PROGRAMMING (DESCRIPTION) A detailed description of the MAC program as described by this observer: Treatment Readiness Program Components:
1. Daily treatment readiness group sessions (youth) 2. Individual treatment and readiness sessions (minimum of one session) 3. Multi-family educational session (Brief Family-based) 4. Weekly family treatment readiness session 5. Detention programming including Step Up, CBT skill building, and prosocial recreation (youth) 6. Case management for parent and community engagement transition
Youth in the MAC living unit are expected to participate in daily group and at least one individual readiness session with a master’s level trained, licensed substance abuse counselor. Family involvement is highly encouraged. A weekly multi-family educational session is offered each Saturday afternoon and brief family based sessions are offered evenings and weekends to best meet the needs of family schedules. MAC programming is focused on preparing youth and their families to engage in their outpatient substance abuse treatment programs and on-going sobriety. Treatment Readiness Groups: Treatment readiness group sessions for youth focus on motivational enhancement, cognitive behavioral skill building, relapse planning, and decision making. Youth attend daily groups. A positive peer culture is encouraged in the MAC living unit. Individual Treatment Readiness: Individual sessions for youth focus on motivational enhancement, cognitive behavioral skill building, and an assessment of the obstacles which are interfering with successful engagement in outpatient substance abuse and treatment. Multi-family Treatment Readiness Education Classes: Multi-family education classes (i.e., Brief Family-based treatment) focus on increasing knowledge about addiction, the importance of parental supervision and support of their youth with substance abuse in outpatient treatment, perceptions about addiction and increasing the knowledge on the effects of substance abuse on youth and families, and offering community resources for ongoing support of families and youth. Family Treatment Readiness: Family sessions will be encouraged and will focus on increasing parental supervision and support for their youth with substance abuse while in outpatient treatment and improving family cohesion and communication skills. Detention Programming: Daily detention programming includes Step Up, cognitive behavioral skill building, and guided prosocial recreation (i.e., sports, arts, writing, reading). Case Management: Case management will focus on engaging families, community transitional planning, and follow-up services.
112
APPENDIX D (continued)
Mental Health and Medical Service: All additional mental health and medical services will be provided by University Physicians Healthcare, Inc. (UPH). MAC Treatment Readiness Plan Youth Name: _____________________________________________________ JC#: _____________________________________________________________ DOB: ____________________________________________________________ Treatment Readiness Plan: Presenting Problem: Substance abuse and treatment readiness Objectives/Goals: 1. Increase youth readiness to engage in community-based substance abuse treatment. 2. Increase substance refusals. 3. Increase parent involvement in supporting/supervising youth in treatment (Brief Family-based). Interventions: 1. Daily educational group sessions using motivational enhancement, cognitive behavioral skills, relapse planning, and decision making. 2. Minimum of one individual session using the above skills. 3. Minimum one multi-family education session for parent/legal guardian to increase knowledge about addiction and skills on support and supervision of youth and to increase knowledge of effects of substance abuse on families and youth. 4. Minimum of one family readiness session to increase parental support and
supervision. Additional Focus: Changing family’s perceptions about addiction and youth with addiction by increasing knowledge and understanding about the addiction process, helping youth admit he/she has a problem, discussing misconceptions about acceptable use, developing cohesive/clear family relationships through contracting and setting rules, discussing friendships that are healthy and lead to sobriety, encouraging youth to engage in natural highs, work/volunteer opportunities, and getting serious about completing a GED or high school education. How to Help Yourself: 1. Look at your perceptions toward addiction and your teen with addiction, are they healthy and realistic, are they negative or positive? 2. Examine the example that you are setting for your teen? What are your opinions about substance abuse/addiction?
3. Work in concert with your other family members to show unity and understanding of substance abuse problems to your youth.
4. Plan to attend an Alanon meeting to learn about your own awareness about addiction. 5. Accompany your teen to an AA meeting to discuss views about addiction.

113
REFERENCES
Abouyanni, G., Stevens, L. J., Harris, M. F., Wickes, W. A., Ramakrishna, S. S., Ta, E.,
& Knowlden, S. M. (2000). GP attitudes to managing drug and alcohol
dependent patients: A reluctant role. Drug and Alcohol Review, 19, 165-170.
Alexander, B. K., & Gibb, G. S. (1967). Interpersonal perceptions in addict families.
Family Processes, 16, 17-28.
Alexander, J. F., & Parsons, B. V. (1973). Short-term family intervention: A therapy
outcome study. Journal of Consulting and Clinical Psychology, 2, 195-201.
Anderson, H. (1999). Reimagining family therapy: Reflections on Minuchin’s invisible
family. Journal of Family Therapy, 25, 1-8.
American Psychological Association. (2000). Diagnostic and statistical manual of mental
disorders (DSM-IV-TR) (text version). Washington, DC: Author.
Baldock, E. (2007). Grandparents raising grandchildren because of alcohol and other
drug issues. Family Matters, 76, 70-74.
Baldwin, J. N., Davis-Hall, R. E., DeSimmone II, E. M., Scott, D. M., Agrawal, S., &
Thomas, P. R., (2008). Survey of attitudes and behaviors toward alcohol and
other drug use in allied health and physical assistant students. Journal of Allied
Health, 38, 156-161.
Beck, M., Dietrich, S., Matschinger, H., & Angermeyer, M. C. (2003). Alcoholism:
Low standing with the public? Attitudes toward spending financial resources on
medical care and research on alcoholism. Alcohol and Alcoholism, 38, 602-605.
Bergin, A., & Garfield, S. (Eds.) (1994). Handbook of Psychotherapy and Behavior

114
Change (4th ed.). New York: Wiley.
Bloch, M. (n.d.). Retrieved May 26, 2008, from
http://[email protected]
Bowen, M., (1974). Alcoholism as viewed through family systems theory and family
Psychotherapy. Annals of the New York Academy of Science, 233, 115-122.
Bradshaw, J. (1996). Bradshaw on: The Family. (Rev. ed.). Deerfield Beach, FL: Health
Communications.
Brown, S. (1997). National Association of Children of Alcoholics. Retrieved June 4,
2008, from http://www.nacoa.org
Canale, M., & Munn, E. (2005). The stigma of addiction project. Visions Journal, 2,
13-15.
Cannon, E. & Levy, M. (2008). Substance-using Hispanic youth and their families: A
review of engagement treatment strategies. The Family Journal: Counseling and
Therapy for Couples and Families, 16, 199-203.
Carich, M. S., & Spilman, K. (2004). Basic principles of intervention. The Family
Journal, 12, 405-410.
Carr, C., Xu, J., Redko, C., Lane, T. D., Rapp, R. C., & Goris, J. et al. (2008).
Individual and system influences on waiting time for substance abuse treatment.
Journal of Substance Abuse Treatment, 34, 192-201.
Chan, J. G. (2003). Examination of family-involved approaches to alcoholism treatment.
The Family Journal: Counseling and Therapy for Couples and Families, 11,
129-138.

115
Chassin, L., Knight, G., Vargas-Chanes, D., Losoya, S. H., & Naranjo, D. (2009).
Substance use treatment outcomes in a sample of male serious juvenile offenders.
Journal of Substance Abuse Treatment, 36, 183-194.
Coatsworth, J. D., Santisteban, D. A., McBride, C. K., & Szapocznik, J. (2001). Brief
strategic family therapy versus community control: Engagement, retention, and an
exploration of the moderating role of adolescent symptom severity. Family
Process, 40, 313-332.
Colandro, C. (n.d.). Interventions by invitation: Long Island Council offers systems
family intervention. Retrieved August 16, 2007, from
http://www.licadd.org/systemic.htm
Connors, G. J., Donovan, D. M., & DiClemente, C. C. (2001). Substance abuse
treatment and the stages of change: Selecting and planning interventions. NY:
Guilford Press.
Copello, A., Templeton, L., Krishnan, M., Orford, J., & Velleman, R. (2000). A
treatment package to improve primary care services for relatives of people with
alcohol and drug problems. Addiction Research, 8, 471-484.
Copello, A., & Oxford, J. (2002). Alcohol and the family: Is it time for services to take
notice of the evidence? Addiction, 97, 319-333.
Cottrell, D., & Boston, P. (2002). Practitioner review: The effectiveness of systemic
family therapy for children and adolescents. Journal of Child Psychology and
Psychiatry, 43, 573-586.
Dempsey, C. (2006, July 24). Firms extend professional recovery model to broader
116
population. Alcoholism & Drug Abuse Weekly. Retrieved August 29, 2007,
from http://www.interscience.wiley.com
Denton, R. E., & Kampfe, C. M. (1994). The relationship between family variables and
adolescent substance abuse: A literature review. Adolescence, 29, 475-495.
Eiser, J. R. (1986). Social psychology: Attitudes, cognition and social behavior.
Cambridge, UK: Cambridge University Press.
Ellenwood A. E., & Jenkins, J. E. (2007). Unbalancing the effects of the chronic illness:
Non-traditional family therapy assessment and intervention approach. The
American Journal of Family Therapy, 35, 265-277.
English, R. W. (2000). Working with families affected by substance abuse. In A. Sales
(Ed.), Substance abuse and counseling (pp. 177-214). Greensboro, NC: CAPS.
Garrett, J., Landau, J., Shea, R., Stanton, M. D., Baciewicz, G., & Brinkman-Sull, D.
(1998). The ARISE intervention: Using family and network links to engage
addicted persons in treatment. Journal of Substance Abuse Treatment, 15, 333-
343.
Garrett, J., & Landau, J. (2007). Family motivation to change: A major factor in
engaging alcoholics in treatment. Alcoholism Treatment Quarterly, 25, 65-83.
Goodman, C. C., & Silverstein, M. (2001). Grandmothers who parent their
grandchildren: An exploratory study of the close relations across three
generations. Journal of Family Issues, 22, 557-578.
Gurman, A. S., Kniskern, D. P., & Pinsof, W. M. (1986). Research on marital and family

117
therapies. In S. L. Garfield & A. E. Bergin (Eds.), Handbook of psychotherapy
and behavior change (3rd ed.). New York: Wiley.
Gutman, S. A. (2006). Why addiction has a chronic, relapsing course. The neurology of
addiction: Implications for occupational therapy practice. Occupational Therapy
in Mental Health, 22, 1-29.
Hunt, S., & Hunt, B. (2004). Changing attitudes toward people with disabilities:
Experimenting with an education intervention. Journal of Managerial Issues, 2,
266-280.
Jay, J., & Jay, D. A. (2000). Love first: A new approach to interventions for alcoholism
and drug addiction. Center City, MN: Hazelden.
Johnson, B., & Christensen, L. (2004). Educational research: Quantitative, qualitative,
and mixed approaches (2nd ed.). Boston: Pearson.
Johnson, V. E. (1998). Intervention: A step-by-step guide for families and friends of
chemically dependent persons. Center City, MN: Hazelden.
Kelly, J. (2006). The joy of recovery: People who have been through systemic family
intervention share what it is like, what they learned. Retrieved August 16, 2007,
from http://www.joyofrecovery.com
Kolomer, S. R., & McCallion, P. (2005). Depression and caregiving mastery in
grandfathers caring for their grandchildren. International Journal on Aging and
Human Development, 60, 283-294.
Landau, J., Brinkman-Sull, D., Stanton, D., Ikle, D., McCormick, D., & Garret, J.

118
et al. (2004). Outcomes with the ARISE approach to engaging reluctant drug and
alcohol dependent individuals in treatment. The American Journal of Drug and
Alcohol Abuse, 30, 711-748.
Leedy, P. D., (1993). Practical research: Planning and design (4th ed.). New York:
McMillan Publishing Company.
Liddle, H. A., Dakof, G. A., Turner, R. M., Henderson, C. E., & Greenbaum, P. E.
(2008). Treating adolescent drug abuse: A randomized trial comparing
multidimensional family therapy and cognitive behavior therapy. Addiction, 103,
1660-1670.
Liddle, H. A., Rowe, C. L., Quille, T. J., Dakof, G. A., Mills, D. S., Sakaran, E., &
Biaggi, H. (2002). Transporting a research-based treatment into practice. Journal
of Substance Abuse Treatment, 22, 231-243.
Martinez, R. J., & Murphy-Parker, D. (2003). Examining the relationship of addiction
education and beliefs of nursing students toward persons with alcohol problems.
Archives of Psychiatric Nursing, XVII, 156-164.
McCarthy, J., & Light, J. (2005). Attitudes toward individuals who use augmentative and
alternative communication: Research review. Augmentative and Alternative
Communication, 21, 41-55.
McLendon, D., McLendon, T., & Petr, C. G. (2005). Family-directed structural therapy.
Journal of Marital and Family Therapy, 31, 327-339. Retrieved July 28, 2009,
from http://findarticles.com
McCown, W. G., & Johnson, J. (1993). Therapy with treatment resistant families.

119
Birmingham, New York: Hawthorne Press.
Meyers, R. J., Apodaca, T. R., Flicker, S. M., & Slesnick, N. (2002). Evidence-based
approaches for the treatment of substance abusers by involving family members.
The Family Journal: Counseling and Therapy for Couples and Families, 10, 281-
288.
Miller, W. R., Meyer, R. J., & Tonigan J. S. (1999). Engaging the unmotivated in
treatment for alcohol problems: A comparison of three intervention strategies.
Journal of Consultation and Clinical Psychology, 67, 688-697.
Minkler, M., & Roe, K. M. (1993). Grandmothers as caregivers: Raising children of the
crack cocaine epidemic. Newbury Park, CA: Sage.
Minuchin, S. (1974). Families and family therapy. Cambridge, MA: Harvard
University Press.
Mumm, A. M., Olsen, L. J., & Allen, D. (1998). Families affected by substance abuse:
Implications for generalist social work practice. Families in Society: The Journal
of Contemporary Human Services, 23, 384-394.
National Institute on Drug Abuse. (2005). Brief strategic family therapy for
adolescent drug abuse. Retrieved May 26, 2008, from
http://www.drugabuse.gov/TXManuals/BSFT
National Institute on Drug Abuse. (2008). Principles of drug addiction
treatment: A research-based guide. (NIH Publication No. 08-4180).
National Mental Health Association (2000). Justice for juveniles: How communities

120
respond to mental health and substance abuse needs of youth in the juvenile
justice system. Retrieved June 12, 2009, from http://www.nmha.org/children
National Survey on Drug Use and Health. (2007). Retrieved May 29, 2008,
from http://www.oas.samsha.gov
National Centre for Education and Training on Addiction. (2006). Health professionals’
attitudes towards licit and illicit drug users [Brochure]. Flinders University,
Australia: Author.
Nelson, T. S., & Sullivan, N. J. (2007). Couple therapy and addiction. Journal of
Couple and Relationship Therapy, 6, 45-56. Retrieved May 25, 2008, from
http://www.jert.haworthpress.com
O’Farrell, T. J. (1995). Marital and family therapy. Handbook of alcoholism treatment
approaches: Effective approaches (2nd ed.). Boston: Allyn & Bacon.
O’Farrell, T. J., Murphy, M., Alter, J., & Fals-Stewart, W. (2008). Brief family
treatment intervention to promote aftercare among substance abusing patients in
inpatient detoxification: Transferring a research intervention to clinical practice.
Addictive Behaviors, 33, 464-471.
Orford, J., Natera, G., Davies, J., Nava, A., Mora, J., Rigby, K. et al. (1998). Stresses
and strains for family members living with drinking or drug problems in England
and Mexico. Salud Mental, 21, 1-13.
Orford, J., Templeton, L., Velleman, R., & Copello, A. (2005). Family members of
relatives with alcohol, drug, and gambling problems: A set of standardized
questionnaires for assessing stress, coping, and strain. Addiction, 100, 1611-1624.
121
Paniagua, F. A. (1996). Cross-cultural guidelines in family therapy practice. The Family
Journal: Counseling and Therapy for Couples and Families, 4, 127-138.
Perrino, T., Coatsworth, J. D., Briones, E., Pantin, H., & Szapocznik, J. (2001). Initial
engagement in parent-centered preventive interventions: A family systems
perspective. The Journal of Primary Prevention, 22, 21-44.
Reynolds, G. P., Wright, J. V., & Beale, B. (2003). The roles of grandparents educating
today’s children. Journal of Instructional Psychology, 30, 316-325.
Rotunda, R. J., West, L., & O’Farrell, T. J. (2004). Enabling behavior in a clinical
sample of alcohol-dependent clients and their partners. Journal of Substance
Abuse Treatment, 26, 269-276.
Santisteban, D. A., Coatsworth, J. D., Perez-Vidal, A., Kurtines, W. M., Murray, E. J.,
Schwartz, S. J. et al. (2003). Efficacy of brief strategic family therapy in
modifying Hispanic adolescent behavior problems and substance abuse use
[Electronic Version]. Journal of Family Psychology, 17, 121-133.
Sales, A. (2000). Substance abuse and counseling. In A. Sales (Ed.). Substance abuse
and counseling (pp. 1-19). Greensboro, NC: CAPS.
Schaler, J. A. (1987). Thinking about drinking: The power of self-fulfilling prophecies.
The International Journal of Drug Policy, 7, 187-192.
Sexton, T. L., & Alexander, J. F. (1999). Functional family therapy: Principles of
clinical intervention, assessment, and implementation. Henderson NV: RCH
Enterprises.
Sexton, T. L., & Alexander, J. F., (2000, December). Functional family therapy. United

122
States Department of Justice Juvenile Justice Bulletin, 30, 1-8.
Sexton, T. L., & Alexander, J. F. (2002). Family-based empirically supported
interventions. The Counseling Psychologist, 30, 238-261.
Skinner, N., Freeman, T., Feather, N. T., & Roche, A. (2007). Stigma and discrimination
in health-care provision to drug users: The roles of values, affect, and
deservingness judgments. Journal of Applied Social Psychology, 37, 163-186.
Smith, T. E., Sells, S. P., Rodman, J., & Reynolds, L. R. (2006). Reducing adolescent
substance abuse and delinquency: Pilot research of a family-oriented
psychoeducation curriculum. Journal of Child & Adolescent Substance Abuse,
15, 105-115.
Smith, M., & Miller, E. (2000). Drugs and addiction. In A. Sales (Ed.), Substance
abuse and counseling (pp. 177-214). Greensboro, NC: CAPS.
Stanton, M. D. (1979). Family treatment approaches to drug abuse problems: A Review.
Family Process, 18, 251-280.
Stanton, M. D., (2004). Getting reluctant substance abusers to engage in treatment/self-
help: A review of outcomes and clinical options. Journal of Marital and Family
Therapy, 30, 165-182.
Stanton M. & Shadish, W. (1997). Outcome, attrition, and family-couples
treatment for drug use: A meta-analysis and review of the controlled comparative
studies. Psychology Bulletin, 122, 170-191.
Statsoft, P. (2008). Retrieved January 4, 2009, from http://www.statsoft.com
Steinglass, P. (2008). Family systems and motivational interviewing: A systemic-

123
motivation model for treatment of alcohol and other drug problems. Alcoholism
Treatment Quarterly, 26, 9-29.
Substance Abuse and Mental Health Services Administration. (2005). Substance abuse
and mental health statistics. Retrieved March 29, 2008, from
http://oas.samsha.gov/
Suian, D. (2005). Navigating the stigma of mental illness and addiction. Visions
Journal, 2, 20-21.
Sulek, J., Korczak-DZiurdzik, A., Korbel-Pawlaws, M., Lyznicka, D., & Czarneck, D.
(2006). Attitude toward alcoholics and their families. Journal of Physiology and
Pharmacology, 57, 349-358.
Summerall, P., & Leshner, A. (2003). Alcohol, drugs and the brain
[Transcript]. The Dana Foundation.
Swan, N. (1998). Some child abuse victims are more vulnerable than
others to drug abuse: Child abuse and drug abuse. (NIDA Notes: 13).
Tang, Y., Wiste, A., Mao, P., & Hou, Y. (2005). Attitudes, knowledge, and perceptions
of Chinese doctors toward drug abuse. Journal of Substance Abuse Treatment,
29, 215-220.
Triandis, H .C. (1971). Attitudes and change. New York: John Wiley & Sons.
United States Bureau of Census (2000). Washington, D.C: Author. (p.248-249).
Vannicelli, M., Gingerich, S., & Ryback R. (1983). Family problems related to the
treatment and outcome of alcoholic patients. British Journal of Addiction, 78,
193-204.

124
Vetere, A. (2001). Therapy matters: Structural family therapy. Child Psychology &
Psychiatry Review, 6, 133-139.
Washton, A. M., & Zweben, J. E., (2006). Treating alcohol and drug problems in
psychotherapy practice: Doing what works. New York: The Guilford Press.
Williams, P. B. (2007, October). Family systems: Brief M.R.I. family systems
intervention training. Presented at a conference by the Family Systems Institute,
Tucson, AZ.
Williams, R. J., & Chang, S. Y. (2000). A comprehensive and comparative review of
adolescent substance abuse treatment outcome. Clinical Psychology: Science and
Practice, 7, 138-166.
Wilson, J. R., & Wilson, J. A. (1992). Addictionary: A primer of recovery terms and
concepts from abstinence to withdrawal. Hazelden: Center City, Minnesota:
Fireside/Parkside.
Worley, D., & O’Connor, J. (2008). Supervision: Theory and Practice. Presented at a
training by Southwest Institute for Group and Family Therapy, Tucson, AZ.
Young, D., Dembo, R., & Henderson, C. (2007). A national survey of substance abuse
treatment for juvenile offenders. Journal of Substance Abuse Treatment, 32, 255-
266.
Zeig, J. K., & Munion, M. W. (1990). What is psychotherapy? Contemporary
perspectives (pp. 1-14). San Francisco: Jossey-Bass.


















