Safe in Strathspey - Internet Safety and Responsible Use Presentation
8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 1/12
CARE International UK – September 2009
10 – 13 Rushworth Street, London, SE1 0RB, Telephone: 020 7934 9334, Fax: 020 7934 9335
Email: [email protected] www.careinternational.org.uk Registered charitynumber: 292506
Empowering Mothers for Health Behaviour, Accra,
Ghana
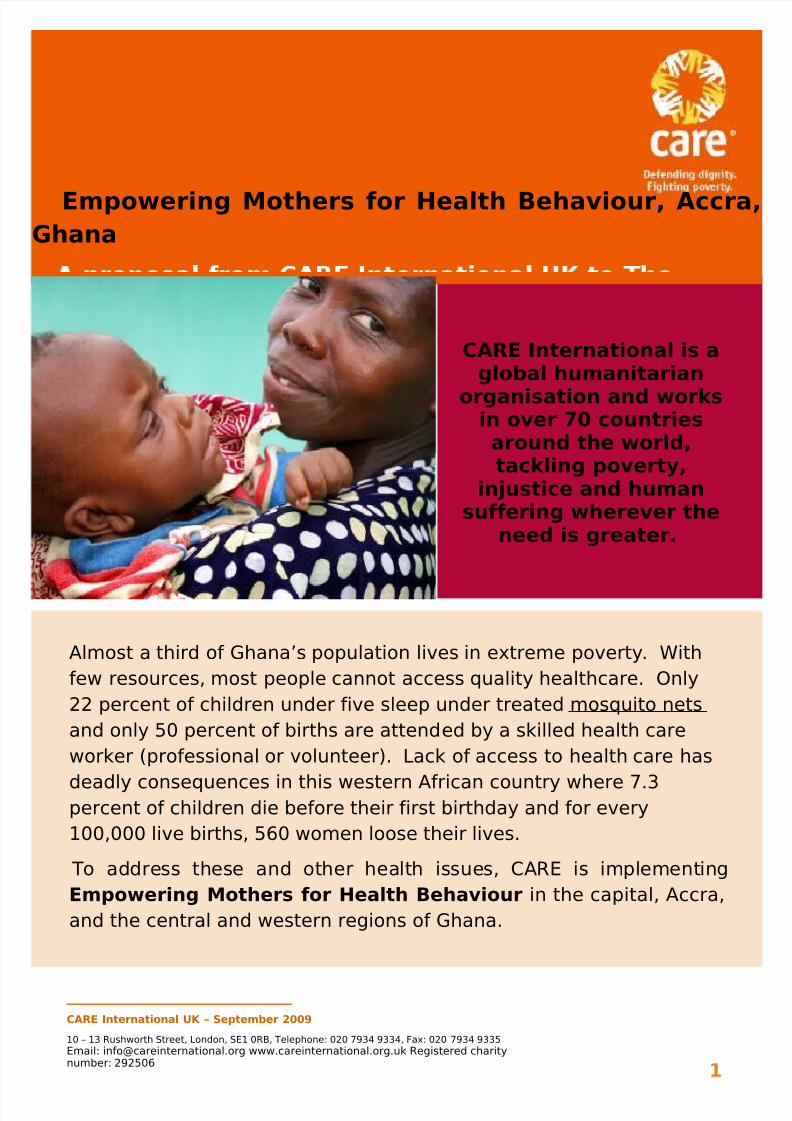
CARE International is aglobal humanitarian
organisation and worksin over 70 countriesaround the world,tackling poverty,
injustice and humansuffering wherever the
need is greater.
Almost a third of Ghana’s population lives in extreme poverty. With
few resources, most people cannot access quality healthcare. Only
22 percent of children under five sleep under treated mosquito nets
and only 50 percent of births are attended by a skilled health care
worker (professional or volunteer). Lack of access to health care has
deadly consequences in this western African country where 7.3percent of children die before their first birthday and for every
100,000 live births, 560 women loose their lives.
To address these and other health issues, CARE is implementing
Empowering Mothers for Health Behaviour in the capital, Accra,
and the central and western regions of Ghana.
1
8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 2/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
Background to Ghana
• Please include context of poverty in Ghana
Poverty in Ghana
Ghana has witnessed a general decline in poverty levels by a large margin in the last
two decades. The incidence of poverty is relatively lower in female headed households
than in male headed household. It is endemic among rural folks than among urban
dwellers.
Whilst all the administrative regions saw a declining trend in poverty in the first half
of the period, Greater Accra and Upper West regions witnessed a reversal trend (an
increase) in poverty in the second half.
Despite the general positive outlook of poverty trends, the incidence of poverty is still
considerably high and relatively higher among Ghanaians in the informal and
agriculture sectors of the economy, particularly among food crop farmers who live in
the rural areas. Majority of the people living in rural areas fit into the World Bank
classification of extreme poverty, getting by on an income less than $1 a day.
Households cannot meet basic needs for survival.
Poverty among rural folks is said to be driven largely by environmental factors
including irregular rainfall patterns and poor soil fertility, whilst that among urban
dwellers is more by shifts in macro-economic conditions characterized by changes in
consumption and availability of cash employment (Ashong & Smith, 2001). It is also
argued that because of low level of education, rural folks are unable to diversify into
more productive livelihood activities. Additionally the social network systems are not
well developed to enable them gain access to finance and work opportunities, making
them more vulnerable to poverty (ibid).
Individuals and societies that are poor tend to remain so if they are not empowered to
participate in the decisions that shape their lives.
This calls for a more coordinated effort in addressing the remaining deficits in the
human development outcomes with emphasis on health improvements and macro-
economic management amongst others. Intervention in healthcare, human capital
development, microcredit provision, a strong savings promotion, capacity-building
training programmes for micro-enterprises and a generalfocus on women will
be able tomake a difference.
2
8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 3/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
• Stats on population and demographics
Greater Accra had a population of 2,905,726 in the 2000 National population
census and a growth rate of 4.4% which gives an estimated mid year population for
2006 of 3,762,336. The total fertility rate in the region of 2.9 from the 2003 Ghana
demographic and health survey is the lowest in the country. The high population
growth rate in the region is thus a mixture of natural increase and rapid migration
into the urban parts of the region from all over the country. Observation suggests
that a fair number of the migrants are unskilled rural migrants moving into the city
to look for non-existent jobs and ending up in the pool of urban poor.
Its population density from the 2000 census was 1,019 persons per squarekilometre. It is the only region in the country where the rural urban ratio is
reversed. Eighty eight percent (88%) of its population lives in localities defined as
urban (population five thousand or more) and only 12 percent live in small rural
communities.
Many of its urban localities are very large with population running into tens of
thousands. The region therefore currently has six administrative districts Accra
Metropolis, Tema Municipality, Ga West, Ga East, Dangme East and Dangme West.
• Please include information about the area where the project is operating and
context of poverty.
The project will be implemented in 25 communities in 2 districts in the Greater
Accra Region – Dangbe East and Ga East.
Dangbe East District
The Dangme East like the Dangme West district is completely rural and typical of rural
districts elsewhere in Southern Ghana. Dangme East had a population of 93,112 in the
2000 census. Poverty is widespread. Most of the population are subsistence farmers
using non-mechanized rain fed agriculture; and along the coast, fishermen.
Dangme East district has 2 functional CHPS compounds, 5 health centres and ahospital that was completed and started operation in 2003. There are four sub-districts
namely Ada-Foah, Kasseh, Sege and Pediatorkope.
Ga East District
The Ga East district used to be almost entirely rural but has been caught up in the
urban spread of the Accra metropolis and Tema municipality and is rapidly urbanizing
especially in the areas bordering Accra - Tema. Its estimated 2005 midyear population
is 258,478. There is one functional CHPS compound, 3 health centres, one small MCH
clinic and no government hospitals or polyclinics. The lack of health infrastructure is
because urban growth has rapidly outstripped the infrastructure that used to beadequate for a sparsely populated rural district. There are numerous small private
3
8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 4/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
clinics in the urbanized parts and one small CHAG hospital run by the church of
Pentecost.
• History of CARE working in Ghana and what it’s priority focus areas are
CARE has successfully implemented HIV & AIDS projects in Ghana since 1996. CARE
GoG has had the capacity and experience to build the capacity of partners to carry out
effective (a) Health and Nutritional Support and (b) HIV & AIDS programming.
CARE’s HIV/AIDS and Health programs in Ghana since 1996 have included projects like
SAPIMA and Wassa West Reproductive Health (WWRH) in Wassa West District in June
2003. WWRH was an integrated STI/HIV/AIDS and family planning project targeting
mine workers and their partners, CSWs and the general communities in mining towns
in two districts.
a) ARCH in Adansi West District,b) The Western and Ashanti STI/HIV & AIDS (WASH) project in eight districts and sub-
metros in Western and Ashanti Regions - funded by United States Department of Agriculture. WASH was implemented from 2002 to 2005 and it strengthened thecapacity of local institutions to implement STI/HIV & AIDS programs. It wasimplemented through 10 partner organizations (local NGOs, CBOs, FBOs) in theWestern and Ashanti regions of Ghana.
The youth project through HACI in the Wassa West District. As part of the WASH
project, CARE received funds from Hope for African Children Initiative (HACI) for a
project to target orphans and other vulnerable children (OVC).
PREVENT (August 2008 – December 2010)
The CARE consortium comprising CARE Denmark and Gulf of Guinea is implementing
PREVENT – Traditional Institutions and Positive People Preventing HIV/ AIDS and
Stigma.
Ahensan Water and Sanitation (AWSAN), 2007 -2008
The Ahensan Water and Sanitation (AWSAN) project provided:
• Clean water supply, sanitation facilities and hygiene education to selected schools.
• Pay-for-use toilet blocks in the community; and• Improved hygienic conditions at the Kumasi Abattoir through provision of water
reservoirs to augment the water available at the Abattoir for cleaning meat and theAbattoir premises
The Water and Sanitation for Urban Poor (WASUP) 2010-2013 is currently being
implemented in the city of Kumasi, which is the fastest growing city in Ghana with a
growing concern about environmental degradation due to poor sanitary conditions and
pollution of waterways.
4
8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 5/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
The project will deliver clean water, improved sanitation facilities, and environmental
and personal hygiene education to the urban poor dweller in five communities within
the Kumasi Metropolis.
The target communities have a total population of approximately 108,500. About 71%of the target population does not have access to hygienic toilet facilities. Women and
children spend long hours to fetch water
Trans-boundary Area (TBA) Water Project (2007 – 2008)
This a Water management and development alliance between the he Coca Cola
Company and the USAID focused on Community Water Management in Trans-
boundary Watersheds (western Ghana and Eastern Ivory Coast).
GHANA SUSTAINABLE CHANGE PROJECT (GSCP) –JUNE 2004 TO MAY 2009
In June 2004, USAID awarded the Ghana Sustainable Change Project (GSCP) to the
Academy for Educational Development and its partners, CARE, the Manoff Group and
EXP Momentum. This five-year Program had the mandate to support the Ghana
Health Service and other private and civil society groups to increase the health status
of Ghanaians through communication interventions which can be sustained over time.
The Project, with its partners and counterparts, ensured evidence-based
communication interventions that increasingly impacted on reproductive and child
health, and HIV/AIDS, and that took into consideration all aspects of a supportive
environment including capacity building, advocacy and social marketing. The GSCP
provided technical assistance to strengthen training and the implementation of
communication programs for health, along with limited commodity support to the
health sector under the four Project goals (Communication, Capacity Building, Social
Marketing and Advocacy.
CARE currently implements over twenty projects in 56 districts (7 regions) in
Ghana. For CARE, partnerships with, and capacity building for, government institutions
and civil society, including community based organizations, are central to its mission
in Ghana. CARE’s portfolio in Ghana includes a broad range of complementary
livelihoods and social services provision and capacity building in agriculture & naturalservices, girls’ education, health and HIV&AIDS, water/sanitation and community
micro-finance.
CARE has a long term presence in the Western Region of Ghana, and it is recognized
for its capacity building work at community, district and national levels, as well as its
policy advocacy and gender expertise. CARE’s experience in building local capacities
includes technical and organizational development training and facilitation of district
level service providers’ networks/forums in a dozen districts in Northern and Western
Ghana. Currently CARE works with over 200 women’s groups in Northern Ghana.
5

8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 6/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
Background to problem
• What is the problem relating to Health and Malaria in Ghana and more
specifically where the project is operating?
In Ghana, malaria is a major public health problem and cause of morbidity andmortality anddirectly contributes to poverty, low productivity, and reduced school attendance.Malariaaccounts for more than 61% of hospital admissions for children under age five, and 8%of pregnant women. Nearly 38% of outpatient visits are related to malaria, which is theleadingcause of lost workdays due to illness. It is estimated that malaria kills 22% of childrenunder age five (or 20,000 children every year) and is the main case of death amongchildren in the postnatal period, and 9% of maternal deaths.
Again in recent BCS advocacy meetings in the Ga East and Dangme East districtsmalaria emerged as the topmost issue in the districts of which women and children
are the most vulnerable (these came up in the presentations made by the District
Directors of Health Services).
To address these and other health issues, CARE is implementing Empowering Mothers
for Health Behaviour in the Greater Accra, central and western regions of Ghana. The
first phase will be implemented in two districts in the Greater Accra region.
Background to 4 year Programme supported by USAID and also CARE’s
experience in working in Health and Malaria prevention
The Behaviour Change Support (BCS), a 4-year Behaviour change CommunicationUSAID funded project (August 2009 - September, 2013) The project focuses onfostering positive health practices in households and communities by creating andstrengthening social norms around health thinking and health behaviour andsustaining these practices in three regions within Ghana (the Greater Accra, Centraland Western Regions – all communities 3,600).
The BCS Project is designed to create broad, ongoing interventions that addressmultiple, integrated health topics over the life of the project to bring aboutimprovement in health and works through four key elements - Behaviour ChangeCommunication(BCC), Community Mobilization(CM), Community BasedDistribution(CBD) and Capacity Building. These elements are well coordinated to formthe framework of - Communication for Social Change Framework (CFSC).In the CFSC framework, BCC campaigns serve as the catalyst of change; communitydialogue and action of CM accelerates and deepens that change; community-baseddistribution allowspeople to take action based on transformed community norms; and capacity building,sustains change.
The integrated thematic health areas are: Family Planning, Maternal Neonatal ChildHealth, Malaria, Nutrition, Water and Sanitation.
6
8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 7/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
The project teams work with counterparts in GHS units to maximize the contribution of BCC towards building on the successes, reversing the negative trends and creatingmomentum to move the stagnant indicators in a positive direction; as well as withother USAID funded projects, the private sector and stakeholders at the various levels
in the target areas to enable them to make input and have ownership of the processfor sustainability.
The Johns Hopkins Bloomberg School of Public Health Centre for CommunicationPrograms (JHU/CCP), in partnership with CARE Gulf of Guinea and PLAN International,form the team of choice to manage the implementation of the Project.
With over 15 years experience in Ghana, CARE has demonstrated extensive capacity
in community mobilization. CARE’s role in this partnership is to conduct and
coordinate both rural and urban community mobilization in two regions of Ghana
(Greater Accra and Western Region), and urban community mobilization in one region
(Central Region).
Our community mobilization approach will not only help people improve their health,
but by its very nature will strengthen and enhance the ability of the community to
work together for any goal that is important to its members. The end result will not
only be a health issue “addressed” but also increased capacity to successfully address
other community needs and desires (BCS Project Proposal, 2009).
• Information on Programme, objectives, who is involved and the timeframe
Goal
The overall goal of the project is to increase demand for and use of malaria
prevention services among women groups in the Greater Accra Region.
Objectives
o Adopt the VSLA strategy to attract and draw women to regular meetings
to share messages on malaria prevention and discuss how to apply
information to real life situation for sustainable behaviour change.
o Increase antenatal attendance and demand for SP by pregnant women.
o Improve the skills of women in the home management of malaria’
o Increase the demand and nightly use of LLINs by individuals and families.
o Form VSLA groups in 10 communities in the Ga East and 5 communities
in the Dangme East Districts with income generation as a driving force to
attract other women for health promotion in malaria.
• CARE’s experience and expertise in this area – Health and Malaria prevention
CARE has over 15 years experience in Ghana and has demonstrated extensive
capacity in community mobilization in health. Currently CARE plays a similar role in
the BCS partnership in conducting and coordinating both rural and urban communitymobilization in two regions of Ghana (Greater Accra and Western Region), and urban
community mobilization in one region (Central Region).
7
8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 8/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
Summary of Project
• A paragraph explaining project, the aim and how many women it will reach
• The ‘Empowering Mothers for Health Behaviour’ project aims at deepening the
existing activities being implemented by the GHS and NGOs with respect to the
adoption of healthy behaviours in Malaria and other related issues to improve
the health of the people in the selected communities and gradually expand
while building on the initial experiences. This initial phase will be implemented
in 15 communities in the greater Accra Region; 2 groups will be formed in each
community. The idea is to use the VSLA approach to attract and draw women to
regular meetings where malaria control messages will be consistently discussed
using materials produced by ProMPT and also used by BCS. Through this
initiative, the women will appreciate the relationship between health and
economic wellbeing. When the women start managing income from VSLA they
would want to be healthy always to continue to contribute to accumulate
wealth. They will therefore be motivated to apply the health messages for the
desired behaviour change to take place. The successes of the initial groups will
lead to the formation of more groups and the number of health advocates in the
communities will increase.
Implementation starts from the Greater Accra Region because Hopeline Institute
is currently implementing the VSLA in some communities in the Ga East District
and we plan to expand the base and at the same time introduce Prolink to the
VSLA strategy to be implemented in the Dangme East District. In this first phase
Hopeline will manage a minimum of 20 groups and Prolink, 10 groups. We hope
to extend to the Western and Central Regions in the next phase.
Because children are also vulnerable, 5 basic schools will be reached with
malaria prevention information; the emphasis will be on children at the
kindergarten level (the under 5 vulnerable group).
Project goal, objectives, activities and expected outputs
Please provide:
Project goal
The overall goal of the project is to support households to experience improved quality
life through a combination of health and financial behaviour change approaches.
Objectives and specific activities
Objectives
8
8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 9/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
o Adopt the VSLA strategy to attract and draw women to regular meetings
to share messages on malaria prevention/home management and discuss
how to apply information to real life situation for sustainable behaviour
change. The women will adopt healthy behaviours and become advocatesin their communities.
o Increase antenatal attendance and demand for SP by pregnant women.
o Improve the skills of women in the home management of malaria’
o Increase the demand and use of LLINs by individuals and families.
o Form VSLA groups in 10 communities in the Ga East and 5 communities
in the Dangme East Districts with income generation as a driving force to
attract other women for health promotion in malaria (form 2 VSLA groups
in each community with between 15 to 25 members per group).
Activities
Facilitation of workshops for about 500 women (15 women groups in rural areas,peri-urban, communities and market/trading communities of the Greater AccraRegion) to share knowledge, attitudes, and practices on malaria, using alreadydeveloped materials.
Training sessions to prepare the women’s groups to appreciate the concept of VSLA.
Capacity building workshops for the Prolink Organization, the NGO partner in theDangme East District on VSLA to enable them supervise the groups in theirdistrict.
Workshops with the communities to build commitment for specific actions,including support to the set up of group level malaria emergency funds within thevillage savings and loans group procedures;
Support the implementation of a Malaria day in 5 basic schools, to raiseawareness and commitment to actions amongst pupils and their families.
Facilitate 30 women groups’ representatives to attend major health meetings/eventsat the Regional level, to share their efforts and stories and influencerelevant decision makers with some key evidence from the communities.
This project will improve the health of thousands of Ghanaians and improve their
capacity to access and advocate for better health care in the future.
Expected outputs
Please provide timescale of project.
• Expected Outputs
9

8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 10/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
• Timescale of the project
Empowering Mothers for Health Behaviour
Activity Month Output Responsibility
Advocacy meeting with the
NGO partners
October,
2010
Hopeline Institute and Prolink
Organization CM staff (10)
CM Team/ VSLA Expert
Capacity building for theProlink Organization, theNGO partner in theDangme East District onVSLA to enable themsupervise the groups intheir district.
October,
2010
Prolink Staff trained, training
report produced
CM Team/ VSLA Expert
Identify VSLA communities October,
2010.
About 15 communities CARE/GHS/VSLA
Expert/NGO Partners.
Community entry –Advocacy meetings withstakeholders in thecommunities.
November,
2010
About 15 communities
covered
CARE/GHS.
Formation of the VSLAgroups and introduction toVSLA Approach
November,
2010
About 30 VSLA groups
formed
CARE/GHS/VSLA
Expert/NGO Partners.
Training of the women
groups
December,
2010.
About 600 women in 30
groups trained to manage
VSLA
CMTeam/VSLA Expert/NGO
Partners.
Implementation of VSLA in
the communities
Jan – Sept,
2011
List of group members and
their shares documented;
Terms of reference for each
group in place. Meeting
schedule developed.
CARE/NGOs/Mobilizers.
Communities workshops
on building commitment
for specific actions, e.g.
malaria emergency
funds within the VSLA
group procedures.
April, 2011 Workshops held in 15
communities; Malaria funds
set up for each community;
15 workshop reports
produced.
CMTeam/VSLA Expert/NGO
Partners/. VSLA Group
members
Support theimplementation of aMalaria day in 5 basicschools, to raiseawareness andcommitment to actions
amongst pupils and theirfamilies.
Feb-
March,
2011
Malaria day organized in 5
schools and reports produced
CMTeam/VSLA Expert/NGO
Partners/. VSLA Group
members
10

8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 11/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
Facilitate 30 womengroups’ representativesto attend major healthmeetings/events
Representatives of 30
women’s groups attended
Health meetings/events
CARE/NGOs/Mobilizers/GHS
Monitor implementation of
community Action Plans
October,
2010
September,
2011
Monitoring checklists
developed for use.
Monitoring visits conducted
by Mobilizers, NGO partners,
VSLA Expert and CM Team
CARE CM/NGOs/Mobilizers/
VSLA Expert.
Hold stakeholders review
meetings
August-
September,2011
Weekly meetings by group
members held.
Monthly review meetings with
mobilizers.
Quarterly review meetings
with, NGO Partners and CM
Team.
Stakeholders’ review
meetings
CARE CM/NGOs/Mobilizers/
VSLA Expert/VSLA groupmembers.
Location of project and a summary of the project beneficiaries
Monitoring and Evaluation
- Neighbour to neighbour information sharing pairs.
- No of VSLA women of women groups formed and the number of women whoparticipate in meetings regularly.
- List of best practices identified, documented, shared and employed by other
groups.
- No of schools reached, number of teachers and children, number of meetings
held with each school and action taken by the schools in response.
- % of pregnant women 15-45 years who slept under ITN/LLIN the previous night.
- % of children under 5 who slept under ITN/LLIN the previous night.
- % of pregnant women who have received IPT two times and above
11
8/6/2019 1 Strathspey Proposal Empowering Mothers in Malaria Health Behaviour, Ghana
http://slidepdf.com/reader/full/1-strathspey-proposal-empowering-mothers-in-malaria-health-behaviour-ghana 12/12
Empowering Mothers for Health Behaviour, Accra,
GhanaA
Can you describe how the project will be monitored (I assume that the larger project
will monitor these activities?)
- Development of workplans at all levels (VSLA groups, mobilizers, NGO
Partners, CM Team)
- Weekly meetings by group members. A checklist will be developed to be
completed by group leaders capturing data on the activities.
- Monthly review meetings – VSLA Groups with mobilizers; NGOs with mobilizers;
CM Team with NGO partners/mobilizers/VSLA group members.
- Quarterly review meetings with, NGO Partners/CM Team/ Community
stakeholders
- Activity reports, minutes of meetings, quarterly reports and annual report.
CARE Ghana is requesting £25,000. In summary the funds will be used (in up to 1 yr,
starting Oct, 08) see attached budget:
12