WHO priorities and plans 2012/13 Dr Jarno Habicht WHO Representative 15 December 2011.
Upload
charles-chaseCategory
view
214download
0
1
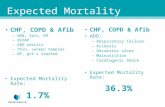
Risk of mortality is greater among women without access to hygiene,
sanitation,water
1
2.5
5.2
0
1
2
3
4
5
6
Exclusive BF no BF (with toilet
& piped water)
no BF (no toilet or
piped water)
Rel
ativ
e Ris
k
RR of Infant Mortality by Feeding Mode and Health Environment
Habicht et al., 1988

2
Percent of Total Population with Access to Safe Water
0
20
40
60
80
100Bot
swan
a
Mal
awi
Nig
eria
Tan
zani
a
Indi
a
Hon
dura
s
Rural
Urban
UNICEF, 2002

3
Percent of Total Population with Access to Adequate Sanitation
0
20
40
60
80
100
Botswana Malawi Nigeria Tanzania India Honduras
Rural
Urban
UNICEF, 2002
4
Feeding Options Currently Recommended by WHO (1998)
• Breastfeeding
– exclusive breastfeeding
– heat-treated breast milk
– wet-nursing
– milks banks
– early cessation of breastfeeding (as soon as feasible)
• Replacement feeding
– commercial infant formula
– home prepared infant formula (modified, with additional nutrients)
– enriched family diet with BMS/MN supplements after 6 months

5
What do we know about the feasibility of exclusive
breastfeeding? (BFHI/MCH/IMCI) -1
0%
20%
40%
60%
80%
100%
Program Control
% infants breastfed exclusively in previous 24 hours < 6 months
< 4 months
@ 3 months @ 5 months

6
EBF rates at 6 weeks - over time and after the introduction of an education and
counseling program on safer breastfeeding practices in Harare, Zimbabwe (n=9,931)
0102030405060
11/97 to
6/98
7/98 to
1/99
2/99 to
8/99
9/99 to
10/99
11/99 to
01/00
Study Period
%
Education and counseling intervention began
ZVITAMBO data

7
Exclusive breastfeeding rates in PMTCT programs with infant feeding counseling - Barcelona
AIDS abstracts
87%
59%
42%31%
0%
20%
40%
60%
80%
100%
Zambia South Africa India Botswana
Methodologies and ages at measurement varied

8
Methods used for measuring exclusive breastfeeding produce different rate
estimates n=970 mothers exposed to infant feeding counseling
ZVITAMBO data
Exclusive Breastfeeding at 3 months
14.120.9
31.738.8
01020
304050
Conditional
Ever
Ever 7 day recall 24 hr recall
9
What do we know about the feasibility of early/rapid
breastfeeding cessation? -1Potential risks for
infant
• Dehydration
• Anorexia
• Later behavior problems
• Malnutrition
• Illness or death
Potential risks for mother
• Engorgement • Mastitis• Increased risks of
pregnancy• Depression • Stigma• Possible reversion to
breastfeeding
Piwoz et al, 2002
10
What do we know about the feasibility of early breastfeeding
cessation? -2 Barcelona AIDS Conference
• Early, rapid cessation is possible (Uganda, Zambia, Botswana)
• Problems encountered– breast engorgement; mastitis; babies crying, trouble
sleeping, appetite loss, diarrhea; financial constraints with replacement feeding; family objections
– more problems when cessation < 6 months (Botswana)
• Trained counselors were able to help mothers overcome problems
• Provision of replacement feeds, family support facilitated process
• Impact on HIV transmission, survival not yet known
11
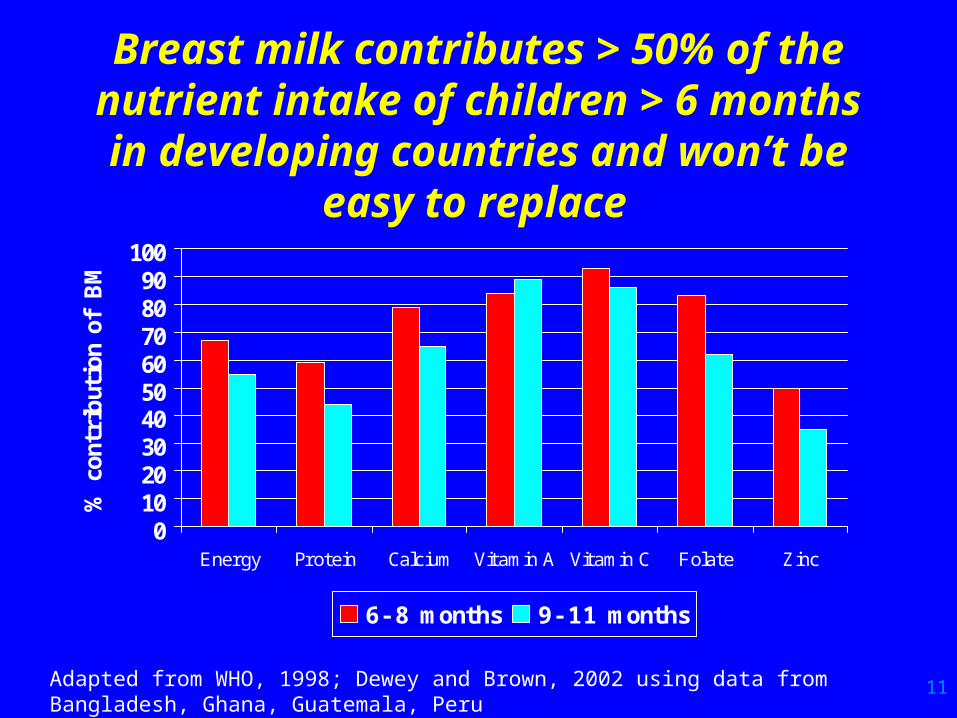
Breast milk contributes > 50% of the nutrient intake of children
> 6 months in developing countries and won’t be easy to
replace
0102030405060708090100
Energy Protein Calcium Vitamin A Vitamin C Folate Zinc
% c
ontr
ibut
ion
of B
M
6- 8 months 9- 11 months
Adapted from WHO, 1998; Dewey and Brown, 2002 using data from Bangladesh, Ghana, Guatemala, Peru

12
What do we know about the feasibility of other
breastfeeding options?• Heat-treated breast milk
– heating milk to 56-62.5 degrees C for 12-15 min inactivates HIV in human milk (Jeffreys et al 2001)
– no data on feasibility of daily use from birth
– may be practical during transition period with early cessation
• Use of wet nurse - no data – monitoring HIV status of wet nurse a challenge
– practice may be less common because of HIV
• Milk banks - no data– may be feasible in some settings (Brazil, LA Region)

13
What do we know about the feasibility of commercial
formula?• High acceptance/adherence in some countries with
access to clean water, health care, subsidized cost
– Thailand, Brazil, South Africa, Botswana
• Adherence with exclusive use may be higher than for exclusive BF (Botswana)
• Stigma associated with its use widely reported in Africa
• Access to safe water, health care needed
• Proper instruction on safe preparation, feeding
• Cost - > 6 months supply

14
Formula use in selected programs where provided
free100% 98% 89%
46%33%
0%
20%
40%
60%
80%
100%
Brazil Thailand Botswana Uganda Cote
d'I voire
Barcelona AIDS Conference

15
Uptake of Infant Formula in PMTCT program sites in SA
0%
20%
40%
60%
80%
100%
W. Cape Mpumalanga Kwa Zulu
Natal
Eastern Cape
Peri/Urban Rural
McCoy et al, 2002

16
Evidence of Spillover?Infant feeding patterns in PMTCT vs.
non-PMTCT sites in Botswana (< 6 months, 24 hr recall)
0%10%20%30%40%50%60%70%80%
Exclusive
BF
Use Infant
Formula
Give other
fluids
PMTCT: HIV- negmothers
Comparison: Statusunknown
MOH/UNICEF, 2002
P< 0.001
EBF is lower, mixed feeding is higher in PMTCT sites

17
What do we know about the feasibility of home prepared
formula?• Nutritional adequacy and cost studied in KwaZulu
Natal, SA
• Fresh and powdered full-cream milk
• Findings:
– intakes of vitamins E, C, folic acid, pantothenic acid < 33% of adequate intake (AI)
– intakes of zinc, copper, selenium, vitamin A < 80% AI
– intakes of EFA were < 20-60% AI
– cost was $9.80/month or 20% of average monthly income
– preparation time was 20-30 minutes for 120 ml
Papathakis et al, 2002

18
Challenges for the Future• Policy issues:
– Can we reframe the debate on breastfeeding versus replacement feeding?
– What is the role of commercial infant formula?
• Implementation:– How do we implement October 2000 guidance/scale up?
• Research:– Risk analysis and counseling hampered by uncertainty
– Can breastfeeding or replacement feeding be made safer for HIV+ women?
• Learning from ALL our experience
19
Can we reframe our thinking and discussion on this issue? -1
• Let’s talk about improving HIV-free survival instead of reducing HIV transmission– reflects higher objective
– resolves conflicting strategies
• Let’s talk about reducing postnatal transmission instead of HIV transmission through breastfeeding– more accurate
– less emotional
– less burdened with the weight of history

20
Can we reframe our thinking and discussion on this issue? -2
• Focus on maternal health & nutrition – Keeping HIV+ mothers well may be among the most
important things we can do to prevent P/N transmission
– BF transmission was ~2% between 6 w-24 months in WA study among women with CD4 >500 (Leroy et al, 2002)
– Nutrition depletion, weight loss during BF may increase risk of maternal mortality (Nduati et al, 2001)
– Keeping mothers alive will improve child’s chances for survival (Nduati et al, 2001)
– ARV use during BF now being studied

21
Can we make breastfeeding safer for HIV+ women? -1
• Enhance health/nutrition care for women
• Provide adequate lactation counseling and support, involving families/communities
– increase adherence to exclusive breastfeeding
– promote good breastfeeding techniques
– prevent cracked nipples, maintain breast health
• Immediate treatment for mastitis, other systemic infections that could affect viral load in BM
– could prevent a sizeable fraction of BF transmission
– may be most important in early month(s)

22
Can we make breastfeeding safer for HIV+ women? -2
• Assist families with early breastfeeding cessation
– assess health status of mother and infant
– prepare for the process so that the transition is safe (cup-feeding, safe preparation/hygiene, stigma)
– heat treat breast milk if weaning is gradual
– could prevent sizeable fraction of BF transmission
• Provide adequate nutrition after breastfeeding ends
– appropriate breast milk substitutes and/or multi-nutrient supplements should be provided to prevent malnutrition
23
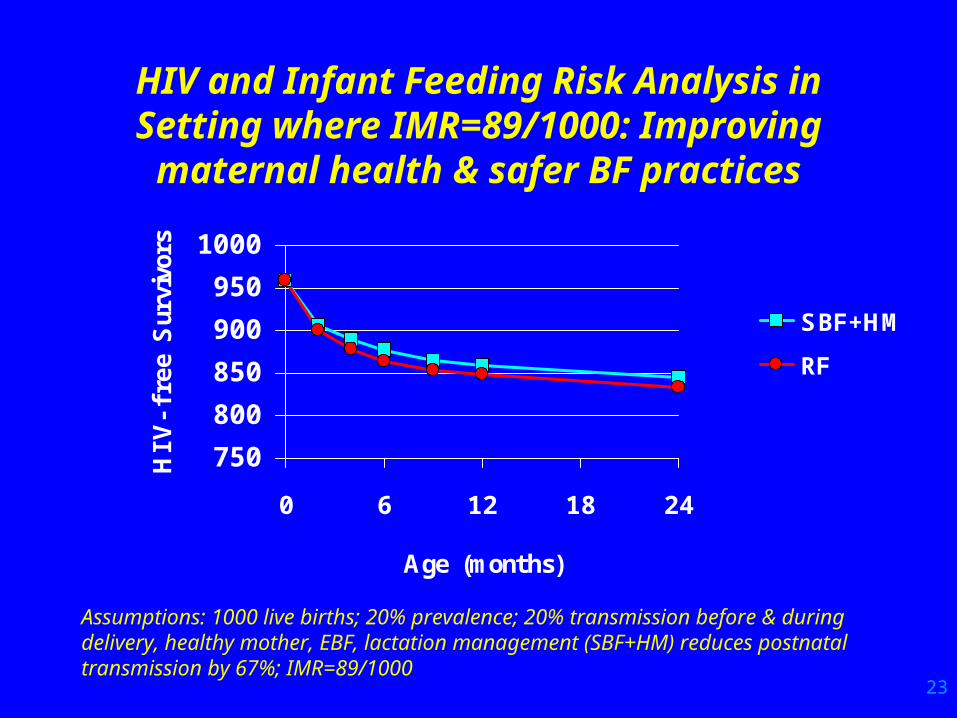
HIV and Infant Feeding Risk Analysis in Setting where IMR=89/1000:
Improving maternal health & safer BF practices
750
800
850
900
950
1000
0 6 12 18 24
Age (months)
HIV
-fr
ee S
urvi
vors
SBF+HM
RF
Assumptions: 1000 live births; 20% prevalence; 20% transmission before & during delivery, healthy mother, EBF, lactation management (SBF+HM) reduces postnatal transmission by 67%; IMR=89/1000

24
HIV and Infant Feeding Risk Analysis in Setting where IMR=100/1000:
Improving maternal health & safer BF practices
750
800
850
900
950
1000
0 6 12 18 24
Age (months)
HIV
-fr
ee S
urvi
vors
SBF+HM
RF
Assumptions: 1000 live births; 20% prevalence; 20% transmission before & during delivery, healthy mother, EBF, lactation management (SBF+HM) reduces postnatal transmission by 67%;
25
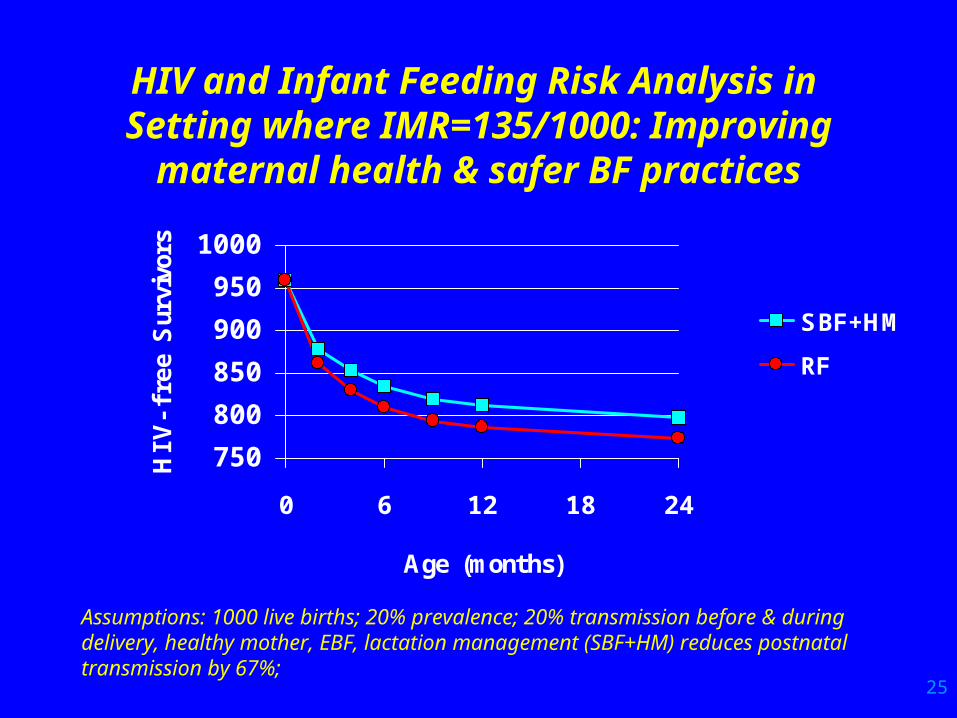
HIV and Infant Feeding Risk Analysis in Setting where IMR=135/1000:
Improving maternal health & safer BF practices
750
800
850
900
950
1000
0 6 12 18 24
Age (months)
HIV
-fr
ee S
urvi
vors
SBF+HM
RF
Assumptions: 1000 live births; 20% prevalence; 20% transmission before & during delivery, healthy mother, EBF, lactation management (SBF+HM) reduces postnatal transmission by 67%;
26
What is the role of commercial formula for replacement
feeding? • It is the best option for RF if conditions can be met
– formulated specially for humans, nutritionally fortified
– safe water, access to health care, training in safe preparation, feeding required to make it safe
– postnatal follow-up also required (monitor growth, ensure adequate access/availability)
– cost will make it NOT affordable for poor families to purchase
– cost may make it NOT sustainable for governments
– Code of Marketing of BMS protects against misuse if enacted/enforced
– But “spillover” may be unavoidable if BF support for HIV-negative and status unknown mothers is not adequate
27
Can we make replacement feeding safer for HIV+ women?
• Provide safe water & environmental conditions
• Family support, community understanding
• Postnatal follow-up and enhanced care
– essential child health interventions
• Screen mothers, target use to those most at risk
• Take measures to prevent unnecessary use of RF
• We must strengthen, not abandon, our efforts to support optimal infant feeding for all because of HIV. The need is even greater when PMTCT programs provide infant formula to HIV+ women.

28
Thank you