1 Revisiting hypoxia therapies for tuberculosis
24
Revisiting hypoxia therapies for tuberculosis 1 2 Stefan H Oehlers 3 4 Tuberculosis Research Program at the Centenary Institute, The University of Sydney, Camperdown, 5 NSW 2050, Australia 6 The University of Sydney, Discipline of Infectious Diseases & Immunology and Marie Bashir 7 Institute, Camperdown, NSW 2050, Australia 8 Corresponding author [email protected] 9 10 Funding: 11 This work was supported by an Australian National Health and Medical Research Council CJ 12 Martin Early Career Fellowship APP1053407 and Project Grant APP1099912; The University of 13 Sydney Fellowship G197581; NSW Ministry of Health under the NSW Health Early-Mid Career 14 Fellowships Scheme H18/31086; and the Kenyon Family Foundation Inflammation Award 15 (S.H.O.). 16 17 Abstract 18 The spectre of the coming post-antibiotic age demands novel therapies for infectious diseases. 19 Tuberculosis, caused by Mycobacterium tuberculosis, is the single deadliest infection throughout 20 human history. M. tuberculosis has acquired antibiotic resistance at an alarming rate with some 21 strains reported as being totally drug resistant. Host-directed therapies attempt to overcome the 22 evolution of antibiotic resistance by targeting relatively immutable host processes. Here I 23 hypothesise the induction of hypoxia via anti-angiogenic therapy will be an efficacious host- 24 directed therapy against tuberculosis. I argue that anti-angiogenic therapy is a modernisation of 25 industrial revolution era sanatoria treatment for tuberculosis, and present a view of the tuberculosis 26 This accepted manuscript has been published https://doi.org/10.1042/CS20190415
Transcript of 1 Revisiting hypoxia therapies for tuberculosis

Revisiting hypoxia therapies for tuberculosis 1
2
Stefan H Oehlers 3
4
Tuberculosis Research Program at the Centenary Institute, The University of Sydney, Camperdown, 5
NSW 2050, Australia 6
The University of Sydney, Discipline of Infectious Diseases & Immunology and Marie Bashir 7
Institute, Camperdown, NSW 2050, Australia 8
Corresponding author [email protected] 9
10
Funding: 11
This work was supported by an Australian National Health and Medical Research Council CJ 12
Martin Early Career Fellowship APP1053407 and Project Grant APP1099912; The University of 13
Sydney Fellowship G197581; NSW Ministry of Health under the NSW Health Early-Mid Career 14
Fellowships Scheme H18/31086; and the Kenyon Family Foundation Inflammation Award 15
(S.H.O.). 16
17
Abstract 18
The spectre of the coming post-antibiotic age demands novel therapies for infectious diseases. 19
Tuberculosis, caused by Mycobacterium tuberculosis, is the single deadliest infection throughout 20
human history. M. tuberculosis has acquired antibiotic resistance at an alarming rate with some 21
strains reported as being totally drug resistant. Host-directed therapies attempt to overcome the 22
evolution of antibiotic resistance by targeting relatively immutable host processes. Here I 23
hypothesise the induction of hypoxia via anti-angiogenic therapy will be an efficacious host-24
directed therapy against tuberculosis. I argue that anti-angiogenic therapy is a modernisation of 25
industrial revolution era sanatoria treatment for tuberculosis, and present a view of the tuberculosis 26
This accepted manuscript has been published https://doi.org/10.1042/CS20190415

granuloma as a “bacterial tumour” that can be treated with anti-angiogenic therapies to reduce 27
bacterial burden and spare host immunopathology. I suggest two complementary modes of action, 28
induction of bacterial dormancy and activation of host Hypoxia Induced Factor-mediated immunity, 29
and define the experimental tools necessary to test this hypothesis. 30
31
1. Introduction 32
After a period of relative success during the golden age of antibiotics in the second half of the 20th
33
century, tuberculosis (TB) rates climbed dramatically with the HIV pandemic from the 1980s. 34
Although recent advances in HIV treatment have seen a fall in the rates of HIV-related TB 35
mortality, the failure to completely eradicate TB and subsequent emergence of multidrug resistant 36
strains of M. tuberculosis has created pockets of endemic TB of global importance. 37
38
The emergence of extensively and totally drug resistant TB strains have led to the contemplation of 39
living in a post-antibiotic era with this ancient killer. Given the short lag between the deployment of 40
a new antibiotic and reports of resistance, new efforts are being directed to discover host-directed 41
therapies (HDTs) for TB. This hypothesis will discuss the history and recent evidence supporting 42
the induction of granuloma hypoxia as an intervention for difficult to treat TB. 43
44
2. TB therapies in the pre-antibiotic era 45
The high altitude sanatoria of the pre-antibiotic era sought to strengthen patients, at least for those 46
who were able to afford the fees of a sanatorium, with regimented daily regimes. It is important to 47
note that these sanatoria would not deliver a curative treatment but rather induce convalescence or 48
prolong patient survival [1, 2]. Three elements of these regimes that we recognise as biologically 49
active are better nutrition, daily sun exposure to boost vitamin D levels, and reducing the supply of 50
oxygen to the bacterial lesions. 51
52

Epidemiological studies have informed us that the burden of TB mortality, like many other 53
infectious diseases, falls disproportionally on the poor, the young, the frail and the weak. 54
Nutritional supplementation, historically achieved by increasing milk consumption, could directly 55
disrupt the infection-malnutrition cycle in favour of patient recovery [3]. Under nutrition is clearly a 56
predisposing factor for TB that remains to be solved as a public health issue [4, 5]. 57
58
The increased sun exposure prescribed for city dwellers of industrial Europe also has a modern 59
analogy in the form of vitamin D supplementation. The micronutrient vitamin D can boost anti-TB 60
immunity in pre-clinical models and is often found to be deficient in TB patients [6]. Again 61
however, systemic review of vitamin D supplementation as an interventional strategy has not 62
yielded evidence of a clinical benefit [4]. 63
64
This leaves the final element of altitude and the availability of oxygen on the outcome of infection. 65
Epidemiological studies in mountainous regions of the Americas and Himalayas have noted a 66
decrease in TB rates in high altitude populations [2, 7-11]. Although the effects of urbanisation and 67
poverty can negate the protective effects of living at high altitude, these observations provide strong 68
evidence for a protective role of hypoxia in TB biology. 69
70
Efforts to surgically bring the benefits of a high altitude retreat to the masses resulted in the short-71
lived lung collapse therapies, which peaked in usage immediately prior to the antibiotic age [12]. 72
Collapse of a lung was hypothesised to rest the organ allowing the body time to contain the 73
infection by fibrosis of the lesions and by starving the bacteria of oxygen [13]. Although successful 74
enough to be widely utilised as a treatment for an otherwise fatal condition, lung collapse surgeries 75
are inherently risky and were rendered obsolete with the appearance of antibiotic therapy. 76
77

Conversely, hyperoxia has been identified as a risk factor for TB disease. Analysis of a Taiwanese 78
comorbidity-controlled cohort of hyperbaric chamber users revealed an increased rate of TB 79
implying reactivation of subclinical TB infection by the hyperoxic treatment [14]. The 80
“summering” of sanatoria patients at sea level is anecdotally reported to cause relapse, even those 81
within the consolidation phase of immune control [1]. Experimentally, the pivotal experiments of 82
Rich & Follis and Sever & Youmans in the mid 20th
century demonstrated the host-protective effect 83
of hypoxia and a detrimental effect of hyperoxia in experimental TB infection (reviewed in [15]). 84
85
3. A “bacterial tumour”: Tuberculosis granulomas are structurally and molecularly similar to 86
tumours 87
Granulomas formed during TB are remarkably similar to solid tumours (Figure 1). Both lesions can 88
form in every organ system of the body, cause chronic diseases requiring lengthy treatment, and are 89
prone to relapse or reactivation. The lesions can even be difficult to differentiate by modern clinical 90
imaging techniques as both take the form of inflamed, metabolically active nodules in 91
fluorodeoxyglucose PET scans. This consumption of glucose to is caused by the engagement of 92
aerobic glycolysis in both lesions [16]. Cellular-level similarities such as a encapsulation of a 93
nodule, the development of a necrotic core during disease progression, an ineffective inflammatory 94
response that exacerbates disease [17, 18], and vascularisation are characteristic of both lesions 95
[19]. Below this cellular similarity are molecular similarities including hypoxia and hypoxia 96
induced factor (HIF) signalling [20], and the destruction of surrounding tissue by matrix 97
metalloproteinases [20, 21]. 98
99
Metabolic syndrome, encompassing diabetes and obesity, is an important co-morbidity of TB, 100
cancer, and other diseases driven by inflammation. Elevated blood glucose and cholesterol 101
associated with metabolic syndrome provide core cellular stressors in TB and tumours. Poorly 102
controlled diabetes impairs protective immunity and exacerbates immunopathology [22, 23], while 103

cholesterol can be preferentially utilised by mycobacteria as a carbon source, contributes to 104
mycobacterial evasion of host immunity, and encourages the survival of transformed cells in 105
tumours [24, 25]. Interestingly, control of either blood glucose by metformin or cholesterol 106
metabolism by statins has positive effects on immune control of TB [24, 26]. 107
108
T-cell immunity is essential for immune control of TB and tumours as evidenced by the impact of 109
HIV infection comorbidity. Two important shared aspects of immune dysfunction that are 110
characteristic of both diseases are the appearance of immune exhaustion and lack of lesion 111
penetration that reduces protective T-cell immunity (reviewed in [27]). The immune exhaustion 112
phenotype is characterised by the expression of surface molecules such as PD-L1 and cytokines 113
such as IL-10 that suppress immunity. Immune checkpoint inhibitors targeting CTLA-4 or the PD-114
1/PD-L1 axis have had remarkable success in stimulating protective immunity against a range of 115
tumours and a similar approach has been proposed for the treatment of TB where a similar 116
immunosuppressive profile can develop [28, 29]. Tumours and granuloma-resident mycobacteria 117
are both adept at feeding off inflammation. In respect to T cells, it is penetration of T cells into 118
tumour masses or into granuloma cores is an important correlate of protective immunity, as the 119
number of T cells distal to the lesion does not affect immune control [30-32]. 120
121
The conserved vascular pathologies of TB granulomas and tumours have also been well described, 122
and open the door to “Robin Hood” well-known vascular-targeting strategies from the cancer field 123
into HDTs for TB. At a molecular level, both lesions produce the vasoactive cytokines VEGF and 124
ANG-2 [33-35]. VEGF is the canonical pro-angiogenic signalling molecule and acts through the 125
cognate receptor VEGFR on endothelial cells to trigger endothelial proliferation and direct 126
migration. ANG-2 is also produced under similar conditions to VEGF and acts as a context-127
dependent antagonist of the TIE-2 receptor to antagonise the vascular-stabilizing effects of 128
physiological ANG-1/TIE-2 signalling [36]. These molecular similarities underpin the tumour-like 129

vasculature seen around mycobacterial granulomas: angiogenesis [19, 37-39], permeability and 130
inconsistent perfusion [34, 35], and haemostasis [40-42]. 131
132
4. Angiogenesis fuels the growth of mycobacterial granulomas 133
The observation that tumours must recruit vasculature to continue growing beyond a critical 134
threshold when oxygen can no longer permeate into their core has led to decades of research 135
targeting tumour angiogenesis as a universal cancer therapy [43]. The VEGF-VEGFR signalling 136
axis-driven is required for angiogenesis and inhibition of the axis by neutralising VEGF, blockading 137
the VEGF binding site on VEGFR, or inhibiting the tyrosine kinase activity of VEGFR indeed 138
slows the growth of many tumours in in vivo models, however efficacious translations to human 139
oncology has been limited. 140
141
Mycobacterial granulomas are known to be highly vascularised during the active stages of infection 142
across a range of host and bacterial species [19, 20, 34, 38]. In TB, extensive angiogenesis has been 143
observed in active granulomas but is mainly absent in the immune-controlled latent form of the 144
disease [19]. Furthermore, serum VEGF levels correlate with active disease and may even 145
constitute a biomarker for disease progression [33]. 146
147
Mycobacteria intrinsically induce VEGF expression by innate immune cells and subsequent 148
angiogenesis through recognition of cyclopropanated trehalose dimycolate, a cell wall component, 149
leading to activation of innate immune cells [44-46]. Furthermore, mycobacterial ESX-1-dependent 150
macrophage aggregation concentrates pro-angiogenic macrophages to direct the growth of blood 151
vessels towards nascent granulomas [38]. This requirement of multiple bacterial effectors, 152
conserved across species of mycobacteria, to elicit the angiogenic response suggests host 153
angiogenesis is an important core function of mycobacterial virulence. 154
155

The correlation between angiogenesis and bacterial growth state prompted us to investigate a 156
mechanistic link using the zebrafish-Mycobacterium marinum infection model [38]. Using small 157
molecule inhibitors of VEGFR, we found inhibition of angiogenesis reduced growth of M. 158
marinum, reduced bacterial dissemination away from primary granulomas, and increased survival 159
of drug-treated animals. VEGFR inhibition increased granuloma hypoxia in infected zebrafish but 160
was ineffective when granulomas formed in highly vascularised tissues in oxygen permeant tissues 161
of the embryo suggesting a mechanism of action dependent largely on the ability to induce hypoxia 162
within granuloma. Additional work by Walton et al. used a dominant negative VEGF isoform to 163
elegantly demonstrate the necessity of the VEGF ligand in the VEGF-VEGFR axis that promotes 164
mycobacterial growth [46]. 165
166
Interestingly, we observed an increased rate of granuloma conversion from a highly cellular 167
phenotype to cuffed acellular core with low-burden phenotype was observed following VEGFR 168
inhibition in zebrafish (Figure 2). This histological shift is reminiscent of the fibrotic walling off of 169
granulomas seen after lung collapse therapy and may represent a conserved aspect of natural host 170
containment of mycobacterial infection. 171
An important paper by Polena et al. utilised SCID mice to show 1) human macrophage-derived M. 172
tuberculosis granulomas recruit vasculature in vivo, and 2) reduced M. tuberculosis dissemination 173
in animals treated with VEGFR-blockading antibodies [39]. This important advance showed for the 174
first time that experimental M. tuberculosis infection of mammals could be controlled by targeting 175
infection-induced angiogenesis. 176
177
Complementary to the vascular-directed effects of anti-VEGF therapy, there is an emerging body of 178
literature addressing the non-angiogenic effects of VEGF blockers in mycobacterial infection. It has 179
become apparent from the cancer literature that immune cells are responsive to VEGF and respond 180
in an immunosuppressive manner. The VEGFR inhibitors pazopanib and VEGFR2 kinase inhibitor 181

I (SU 5408) were detected as protective in a macrophage-based in vitro infection screen, 182
independent of any effect on the vasculature [47]. A recent paper by Harding et al. has elegantly 183
demonstrated a role for granuloma-derived VEGF in promoting harmful granulomatous 184
inflammation in several mouse-M. tuberculosis models [48]. Together these papers provide 185
evidence that targeting the VEGF-VEGFR axis has a net positive effect on the outcome of 186
infection. 187
188
5. Case report evidence for the efficacy of anti-angiogenic drugs against TB 189
Anti-angiogenic therapies for cancer aim to induce sufficient tumour hypoxia to cause growth 190
arrest. Technologies have largely focused on inhibiting the VEGF-VEGFR axis by neutralising 191
VEGF, blockading the VEGF binding site on VEGFR, and inhibiting the tyrosine kinase activity of 192
VEGFR. Ocular inflammation-induced angiogenesis can cause loss of vision and is typically treated 193
by oral anti-inflammatories such as steroids or intravitreal injection of VEGF-neutralising agents 194
such as bevacizumab (Avastin) and ranibizumab. Ocular TB thus presents an important 195
manifestation of disseminated TB where TB treatment overlaps with anti-angiogenic therapy. 196
197
A total of 11 case reports have utilised VEGF neutralisation during TB. Injection of bevacizumab, 198
or the derivative ranibizumab, has been safely used as an adjunctive treatment to improve vision in 199
conjunction with antibiotics [49-52], to clear granuloma-associated angiogenesis after successful 200
antibiotic treatment [53, 54], as a component of treatment for paradoxical TB-associated immune 201
reconstitution inflammatory syndrome [55, 56], and even as monotherapy [57-59]. 202
203
The three monotherapy reports of VEGF neutralisation leading to ocular disease remission provide 204
the clearest evidence yet for an anti-TB effect of anti-angiogenic therapy in human TB. The 4 case 205
reports of anti-angiogenic therapy used as an adjunct to antibiotics demonstrate that adjunctive use 206
does not impair antibiotic efficacy, albeit only in the context of ocular infection. Together, these 207

reports provide some evidence of the efficacy of anti-angiogenic therapy in human TB and 208
demonstrate safety of anti-angiogenic therapy during active ocular TB. 209
210
6. Molecular level protective effects of hypoxia 211
6.1. Effects on the bacterium 212
The most obvious effect of hypoxia is that the lack of oxygen starves the mycobacteria and stops 213
proliferation. Indeed, low oxygen pressures do halt the growth of M. tuberculosis in vitro, causing 214
the bacteria to enter a relatively metabolically dormant lifestyle that is also observed in 215
experimental models and clinically in non-progressing latent infection [60]. Hypoxia causes the 216
build-up NADH, an indicator of cellular stress, in mycobacteria. This metabolic block exposes the 217
bacterial electron transport chain as an antibiotic target in the absence of cellular division [61]. 218
219
M. tuberculosis responds to hypoxic conditions through activation of the DosR regulon (well-220
reviewed in [62]). Expression of DosR regulon genes is exquisitely correlated with hypoxia in vivo 221
and is maximal in the hypoxic granulomas characteristic of the latent TB classification [60]. 222
Mutants lacking components of the DosR regulon are unable to established latent infection in 223
animal models that form granulomas with significant hypoxia but remain relatively virulent in 224
mouse models that do not recapitulate a hypoxic infection environment [63, 64]. Thus induction of 225
granuloma hypoxia is likely to drive a non-replicative bacterial state that can be at least partially 226
controlled by host immunity. 227
228
The intrinsic resistance of dormant mycobacteria to antibiotics compounds the hypoxia-induced 229
shift of mycobacteria to a dormant phenotype. It is conceivable that in drug-sensitive TB cases, 230
adjunctive hypoxia-inducing therapy could counterproductively promote drug resistance by 231
intrinsically limiting the sensitivity of TB to antibiotics. 232
233

6.2. Host protective effects of hypoxia 234
Granuloma hypoxia may also stimulate host immunity to mycobacterial infection. Complementary 235
to the findings of reduced TB incidence in humans living at altitude, whole blood restriction of 236
mycobacterial growth was increased in donors living at high altitude [65]. Furthermore, 237
macrophages cultured in low oxygen show increased bactericidal activity compared with 238
macrophages cultured in atmospheric oxygen [66-68]. Recent analyses of host-mycobacterium 239
interactions have revealed how exposure to hypoxia may augment anti-TB immunity at the 240
molecular level. 241
242
IFNgamma activation is required for optimal macrophage killing of mycobacteria and loss of 243
IFNgamma signalling is responsible for the heritable cluster of diseases termed Mendelian 244
Susceptibility to Mycobacterial Diseases in humans [69]. HIF1alpha signalling has recently been 245
demonstrated to potentiate IFNgamma-dependent immunity against TB [70]. Important anti-TB 246
HIF1alpha-dependent immune pathways include effectors that modulate further immune activation 247
such as PGE2, and directly bactericidal compounds such as nitric oxide [70, 71]. While HIF1alpha-248
dependent immune pathways have been shown to be directly induced by mycobacterial infection 249
[71], we have found anti-angiogenic therapy increases HIF1alpha activation in mycobacterial 250
granulomas in vivo [38]. 251
252
Another recently appreciated anti-mycobacterial killing mechanism is activation of the Warburg 253
effect in mycobacteria-infected macrophages resulting in a switch to glycolysis at the expense of 254
oxidative phosphorylation [72]. This metabolic shift produces sufficient ATP to fuel antibacterial 255
effector activity, glucose-derived metabolites that are toxic to M. tuberculosis under hypoxic 256
conditions, and, in a positive feedback loop, stabilises HIF1alpha to further enhance cellular 257
immunity [73]. 258
259

Together, this potentiation of anti-mycobacterial immunity by hypoxia and HIF1alpha signalling 260
demonstrate a molecular pathway linking anti-angiogenic therapy to reduced mycobacterial burden. 261
262
7. Host-detrimental effects of hypoxia 263
While HIF1alpha activation leads to an enhancement of anti-mycobacterial immunity, it also 264
drastically induces the production of tissue-destructive matrix metalloproteinases (MMPs) [20, 74]. 265
MMPs are produced as part of inflammatory responses and are central to the pathogenesis of many 266
inflammatory diseases when over produced, and their production in mycobacterial infection aids 267
granuloma formation by remodelling infected tissue [21, 75]. The collagenase activity of MMPs 268
aids the growth and dissemination of mycobacteria, facilitating the escape of mycobacteria away 269
from areas of growth-limiting hypoxia. This effect could be analogous to the pro-metastatic effects 270
of hypoxia on tumours (Figure 1). 271
272
The switch to glycolysis is a double-edged sword as prolonged engagement of glycolysis leads to 273
the accumulation of intracellular lipid droplets and the transformation of macrophages into foam 274
cells laden with triacylglycerols (Figure 1). Foam cells are deficient in anti-bacterial function and 275
are thought to provide a ready carbon source for mycobacterial growth in the granuloma core [76]. 276
277
Hypoxia may inhibit the function of T cells and exclude T cells from mycobacterial granulomas. It 278
is evident from the cancer literature that hypoxia-induced cytokine profiles create a 279
microenvironment conducive to Treg retention at the expense of anti-tumour effector T cell types 280
[77]. It is unknown if a similar mechanism functions in TB granulomas. 281
282
It has also been shown that inhibition of lymphangiogenesis by VEGFC reduces systemic T cell 283
responses to infection [78]. If a VEGF family-targeting therapeutic is used to induce hypoxia in TB 284
granulomas, it is conceivable that it could affect inflammatory lymphangiogenesis and the priming 285

of adaptive immune responses. An important distinction between lung collapse or high altitude 286
environmental hypoxia and anti-angiogenic therapy is that the former methods of inducing hypoxia 287
do not prevent blood flow to the granuloma. Hypoxia induced by anti-angiogenic therapy may thus 288
have compounding effects on protective adaptive immunity. 289
290
Mycobacterial granulomas are naturally resistant to penetration by antibiotics, and this is a major 291
therapeutic hurdle for antibiotic delivery [79]. There is thus a valid concern that anti-angiogenesis 292
therapy will create avascular granulomas that could be impenetrable to antibiotics. Vascular 293
normalisation experiments provide a contrasting intervention that decreases granuloma hypoxia by 294
facilitating circulation to the granuloma neovascular network. Work in the rabbit TB model by 295
Datta et al. utilised a short duration of treatment with the monoclonal antibody bevacizumab to 296
neutralise infection-induced VEGF and normalise the granuloma vasculature resulting in better 297
delivery of a small molecule dye to the granuloma core [34]. Xu et al. next demonstrated that 298
inhibiting matrix metalloprotease activity normalised the vasculature and improved antibiotic 299
delivery to mouse granulomas [80]. These two studies highlight the importance of vascular 300
perfusion to delivering antibiotics into granulomas and suggest anti-angiogenic therapies could 301
hinder antibiotic delivery. 302
303
8. Necessary elements of a preclinical model to test the hypothesis 304
TB is a disease that exacerbates economic inequity at personal and international levels. Despite the 305
efficacious application of anti-VEGF biologics to small numbers of ocular TB patients, I believe 306
small molecule VEGFR inhibitors are the most feasible intervention to advance. From an 307
economics standpoint, small molecules can be chemically synthesised as generic drugs as patents 308
expire. Importantly, small molecule VEGFR inhibitors have been formulated for delivery by tablets 309
and capsules extending their delivery range into areas lacking sufficient infrastructure to handle 310
biologics. 311

312
Mouse models of TB infection are the gold standard small animal models for testing new therapies. 313
The ideal mouse TB model would replicate: 314
1. Angiogenic and hypoxic granulomas 315
2. A natural ability to control or sterilise infection 316
3. The pharmacokinetics of antibiotic delivery into granulomas 317
318
Most mouse strains do not develop hypoxic granulomas following mycobacterial infection like that 319
seen in the zebrafish-M. marinum model and in human TB infection [37, 81]. This has recently 320
changed with the characterisation of the C3HeB/FeJ mouse strain that recapitulates necrotic 321
granulomas with areas of hypoxia following pulmonary infection with M. tuberculosis [82-84]. The 322
reproduction of hypoxic granulomas is essential to determine if hypoxia-inducing anti-angiogenic 323
therapies are effective in treating M. tuberculosis infection in mammals [81]. Although granuloma 324
angiogenesis has not been directly described in this strain, it is likely to recapitulate this phenotype 325
as mycobacterial infection-induced angiogenesis is highly conserved across species pairings. 326
327
With respect to human-like immune control, the CC001/UncJ mouse strain was identified from a 328
screen of mouse strains as more able to reduce M. tuberculosis burden between 3 and 6 weeks post 329
infection [85]. The ability of a mouse model to restrain TB infection is unusual and suggests an 330
effective immune response against M. tuberculosis that could be leveraged to examine the effect of 331
hypoxia-inducing therapy in the background of successful immune-mediated control of infection. 332
333
As addressed in section 7, anti-angiogenesis therapy could reduce antibiotic penetration into 334
granulomas. Testing of anti-angiogenic therapy in conjunction with conventional antibiotics will 335
determine if anti-angiogenic therapy should be used to treat antibiotic-sensitive TB or only as a 336
“last line” therapy for antibiotic resistant infections. 337

338
9. Conclusion 339
While hypoxia in cancer has been suggested to ultimately lead to more aggressive malignancies, 340
hypoxia in mycobacterial infection may fit a converse paradigm where lack of oxygen slows 341
bacterial growth and improves anti-TB immunity. The observations and the findings discussed here 342
demonstrate potential adjunctive, host-directed therapies and may open new avenues to treating 343
recalcitrant TB infections, including multi-drug resistant disease. However concerns of the wider 344
effects of these treatments on antibiotic susceptibility call for further pre-clinical testing and 345
compassionate use of anti-angiogenic therapies in antibiotic resistant infections. 346
347
While induction of hypoxia appears to be effective in slowing the growth of mycobacteria in vivo, 348
this approach is probably not sterilising given the low “cure” rate (5-10%) compared with 349
“improved” status (~50%) measured for collapse therapy patients [12], and the highly variable 350
improvement rate of sanatoria from 90% to 5% declining with initial severity of disease and with an 351
average 9 year fitness rate of 60% [1]. These observations could be due to the conversion of active 352
lesions to more latent lesions with a reduced but not sterile load of mycobacteria. While this is 353
certainly preferable to the high mortality rate seen in the pre-antibiotic era it is unsatisfactory 354
compared to the 86% cure rate for drug susceptible TB recorded by the WHO 355
(http://www.who.int/gho/tb/epidemic/treatment/en/). Where hypoxia-inducing therapies may find a 356
niche is in the treatment of MDR TB (50% cure rate) and XDR TB (23% cure rate). 357
358
10. Acknowledgements 359
I would like to thanks Drs Mark Cronan and David Tobin, and all members of the Tobin lab and 360
Tuberculosis Research Program at the Centenary Institute for discussions that helped shape this 361
hypothesis. I believe Dr Cronan coined the phrase “bacterial tumour” that shaped so much of my 362
research into TB-associated angiogenesis. 363

364

References 365 1 Amrein, O. (1929) The High Altitude Treatment of Pulmonary Tuberculosis. Br Med J. 366 2, 1188-1191 367 2 Murray, J. F. (2014) Tuberculosis and high altitude. Worth a try in extensively drug-368 resistant tuberculosis? Am J Respir Crit Care Med. 189, 390-393 369 3 Riva, M. A. (2014) From milk to rifampicin and back again: history of failures and 370 successes in the treatment for tuberculosis. J Antibiot (Tokyo). 67, 661-665 371 4 Grobler, L., Nagpal, S., Sudarsanam, T. D. and Sinclair, D. (2016) Nutritional 372 supplements for people being treated for active tuberculosis. Cochrane Database Syst Rev, 373 CD006086 374 5 Sinha, P., Davis, J., Saag, L., Wanke, C., Salgame, P., Mesick, J., Horsburgh, C. R. and 375 Hochberg, N. S. (2019) Undernutrition and Tuberculosis: Public Health Implications. J Infect 376 Dis. 219, 1356-1363 377 6 Grobler, L., Nagpal, S., Sudarsanam, T. D. and Sinclair, D. (2016) Nutritional 378 supplements for people being treated for active tuberculosis. Cochrane Database Syst Rev, 379 CD006086 380 7 Olender, S., Saito, M., Apgar, J., Gillenwater, K., Bautista, C. T., Lescano, A. G., Moro, P., 381 Caviedes, L., Hsieh, E. J. and Gilman, R. H. (2003) Low prevalence and increased household 382 clustering of Mycobacterium tuberculosis infection in high altitude villages in Peru. The 383 American journal of tropical medicine and hygiene. 68, 721-727 384 8 Perez-Padilla, R. and Franco-Marina, F. (2004) The impact of altitude on mortality from 385 tuberculosis and pneumonia. The international journal of tuberculosis and lung disease : the 386 official journal of the International Union against Tuberculosis and Lung Disease. 8, 1315-387 1320 388 9 Saito, M., Pan, W. K., Gilman, R. H., Bautista, C. T., Bamrah, S., Martin, C. A., Tsiouris, S. J., 389 Arguello, D. F. and Martinez-Carrasco, G. (2006) Comparison of altitude effect on 390 Mycobacterium tuberculosis infection between rural and urban communities in Peru. The 391 American journal of tropical medicine and hygiene. 75, 49-54 392 10 Tanrikulu, A. C., Acemoglu, H., Palanci, Y. and Dagli, C. E. (2008) Tuberculosis in 393 Turkey: high altitude and other socio-economic risk factors. Public Health. 122, 613-619 394 11 Vargas, M. H., Furuya, M. E. and Perez-Guzman, C. (2004) Effect of altitude on the 395 frequency of pulmonary tuberculosis. The international journal of tuberculosis and lung 396 disease : the official journal of the International Union against Tuberculosis and Lung Disease. 397 8, 1321-1324 398 12 Singer, J. J. (1936) Collapse Therapy in Pulmonary Tuberculosis. Cal West Med. 45, 399 120-125 400 13 Coryllos, P. N. (1933) How do rest and collapse treatment cure pulmonary 401 tuberculosis? Journal of the American Medical Association. 100, 480-482 402 14 Wang, K. Y., Lin, Y. S., Sy, C. L., Huang, W. C. and Chen, L. W. (2018) Hyperbaric oxygen 403 therapy increases the risk of tuberculosis disease. The international journal of tuberculosis 404 and lung disease : the official journal of the International Union against Tuberculosis and Lung 405 Disease. 22, 637-640 406 15 Goodwin, R. A. and Des Prez, R. M. (1983) Apical localization of pulmonary 407 tuberculosis, chronic pulmonary histoplasmosis, and progressive massive fibrosis of the lung. 408 Chest. 83, 801-805 409 16 Ankrah, A. O., van der Werf, T. S., de Vries, E. F., Dierckx, R. A., Sathekge, M. M. and 410 Glaudemans, A. W. (2016) PET/CT imaging of Mycobacterium tuberculosis infection. Clin 411 Transl Imaging. 4, 131-144 412 17 Ramakrishnan, L. (2012) Revisiting the role of the granuloma in tuberculosis. Nat Rev 413 Immunol. 12, 352-366 414

18 Ernst, J. D. (2012) The immunological life cycle of tuberculosis. Nat Rev Immunol. 12, 415 581-591 416 19 Ulrichs, T., Kosmiadi, G. A., Jorg, S., Pradl, L., Titukhina, M., Mishenko, V., Gushina, N. and 417 Kaufmann, S. H. (2005) Differential organization of the local immune response in patients 418 with active cavitary tuberculosis or with nonprogressive tuberculoma. J Infect Dis. 192, 89-97 419 20 Belton, M., Brilha, S., Manavaki, R., Mauri, F., Nijran, K., Hong, Y. T., Patel, N. H., Dembek, 420 M., Tezera, L., Green, J., Moores, R., Aigbirhio, F., Al-Nahhas, A., Fryer, T. D., Elkington, P. T. and 421 Friedland, J. S. (2016) Hypoxia and tissue destruction in pulmonary TB. Thorax 422 21 Volkman, H. E., Pozos, T. C., Zheng, J., Davis, J. M., Rawls, J. F. and Ramakrishnan, L. 423 (2010) Tuberculous granuloma induction via interaction of a bacterial secreted protein with 424 host epithelium. Science. 327, 466-469 425 22 Martinez, N. and Kornfeld, H. (2014) Diabetes and immunity to tuberculosis. Eur J 426 Immunol. 44, 617-626 427 23 Hua, F., Yu, J. J. and Hu, Z. W. (2016) Diabetes and cancer, common threads and missing 428 links. Cancer letters. 374, 54-61 429 24 Parihar, S. P., Guler, R., Khutlang, R., Lang, D. M., Hurdayal, R., Mhlanga, M. M., Suzuki, 430 H., Marais, A. D. and Brombacher, F. (2014) Statin therapy reduces the mycobacterium 431 tuberculosis burden in human macrophages and in mice by enhancing autophagy and 432 phagosome maturation. J Infect Dis. 209, 754-763 433 25 Galluzzi, L., Kepp, O., Vander Heiden, M. G. and Kroemer, G. (2013) Metabolic targets 434 for cancer therapy. Nat Rev Drug Discov. 12, 829-846 435 26 Singhal, A., Jie, L., Kumar, P., Hong, G. S., Leow, M. K., Paleja, B., Tsenova, L., Kurepina, N., 436 Chen, J., Zolezzi, F., Kreiswirth, B., Poidinger, M., Chee, C., Kaplan, G., Wang, Y. T. and De Libero, 437 G. (2014) Metformin as adjunct antituberculosis therapy. Science translational medicine. 6, 438 263ra159 439 27 Khan, N., Vidyarthi, A., Amir, M., Mushtaq, K. and Agrewala, J. N. (2017) T-cell 440 exhaustion in tuberculosis: pitfalls and prospects. Crit Rev Microbiol. 43, 133-141 441 28 Zumla, A., Rao, M., Dodoo, E. and Maeurer, M. (2016) Potential of immunomodulatory 442 agents as adjunct host-directed therapies for multidrug-resistant tuberculosis. BMC Med. 14, 443 89 444 29 Ostuni, R., Kratochvill, F., Murray, P. J. and Natoli, G. (2015) Macrophages and cancer: 445 from mechanisms to therapeutic implications. Trends Immunol. 36, 229-239 446 30 Egen, J. G., Rothfuchs, A. G., Feng, C. G., Horwitz, M. A., Sher, A. and Germain, R. N. 447 (2011) Intravital imaging reveals limited antigen presentation and T cell effector function in 448 mycobacterial granulomas. Immunity. 34, 807-819 449 31 Srivastava, S. and Ernst, J. D. (2013) Cutting edge: Direct recognition of infected cells by 450 CD4 T cells is required for control of intracellular Mycobacterium tuberculosis in vivo. J 451 Immunol. 191, 1016-1020 452 32 Ernst, J. D., Cornelius, A., Desvignes, L., Tavs, J. and Norris, B. A. (2018) Limited 453 Antimycobacterial Efficacy of Epitope Peptide Administration Despite Enhanced Antigen-454 Specific CD4 T-Cell Activation. J Infect Dis. 218, 1653-1662 455 33 Matsuyama, W., Hashiguchi, T., Matsumuro, K., Iwami, F., Hirotsu, Y., Kawabata, M., 456 Arimura, K. and Osame, M. (2000) Increased serum level of vascular endothelial growth factor 457 in pulmonary tuberculosis. Am J Respir Crit Care Med. 162, 1120-1122 458 34 Datta, M., Via, L. E., Kamoun, W. S., Liu, C., Chen, W., Seano, G., Weiner, D. M., Schimel, D., 459 England, K., Martin, J. D., Gao, X., Xu, L., Barry, C. E., 3rd and Jain, R. K. (2015) Anti-vascular 460 endothelial growth factor treatment normalizes tuberculosis granuloma vasculature and 461 improves small molecule delivery. Proc Natl Acad Sci U S A. 112, 1827-1832 462 35 Oehlers, S. H., Cronan, M. R., Beerman, R. W., Johnson, M. G., Huang, J., Kontos, C. D., 463 Stout, J. E. and Tobin, D. M. (2017) Infection-induced vascular permeability aids mycobacterial 464 growth. J Infect Dis. 215, 813-817 465

36 Huang, H., Bhat, A., Woodnutt, G. and Lappe, R. (2010) Targeting the ANGPT-TIE2 466 pathway in malignancy. Nature reviews. Cancer. 10, 575-585 467 37 Tsai, M. C., Chakravarty, S., Zhu, G., Xu, J., Tanaka, K., Koch, C., Tufariello, J., Flynn, J. and 468 Chan, J. (2006) Characterization of the tuberculous granuloma in murine and human lungs: 469 cellular composition and relative tissue oxygen tension. Cell Microbiol. 8, 218-232 470 38 Oehlers, S. H., Cronan, M. R., Scott, N. R., Thomas, M. I., Okuda, K. S., Walton, E. M., 471 Beerman, R. W., Crosier, P. S. and Tobin, D. M. (2015) Interception of host angiogenic 472 signalling limits mycobacterial growth. Nature. 517, 612-615 473 39 Polena, H., Boudou, F., Tilleul, S., Dubois-Colas, N., Lecointe, C., Rakotosamimanana, N., 474 Pelizzola, M., Andriamandimby, S. F., Raharimanga, V., Charles, P., Herrmann, J. L., Ricciardi-475 Castagnoli, P., Rasolofo, V., Gicquel, B. and Tailleux, L. (2016) Mycobacterium tuberculosis 476 exploits the formation of new blood vessels for its dissemination. Scientific reports. 6, 33162 477 40 Robson, S. C., White, N. W., Aronson, I., Woollgar, R., Goodman, H. and Jacobs, P. (1996) 478 Acute-phase response and the hypercoagulable state in pulmonary tuberculosis. Br J 479 Haematol. 93, 943-949 480 41 Fox, K. A., Kirwan, D. E., Whittington, A. M., Krishnan, N., Robertson, B. D., Gilman, R. H., 481 Lopez, J. W., Singh, S., Porter, J. C. and Friedland, J. S. (2018) Platelets Regulate Pulmonary 482 Inflammation and Tissue Destruction in Tuberculosis. Am J Respir Crit Care Med. 198, 245-483 255 484 42 Hortle, E., Johnson, K. E., Johansen, M. D., Nguyen, T., Shavit, J. A., Britton, W. J., Tobin, D. 485 M. and Oehlers, S. H. (2019) Thrombocyte inhibition restores protective immunity to 486 mycobacterial infection in zebrafish. J Infect Dis 487 43 Folkman, J. (2002) Role of angiogenesis in tumor growth and metastasis. Seminars in 488 oncology. 29, 15-18 489 44 Saita, N., Fujiwara, N., Yano, I., Soejima, K. and Kobayashi, K. (2000) Trehalose 6,6'-490 dimycolate (cord factor) of Mycobacterium tuberculosis induces corneal angiogenesis in rats. 491 Infect Immun. 68, 5991-5997 492 45 Sakaguchi, I., Ikeda, N., Nakayama, M., Kato, Y., Yano, I. and Kaneda, K. (2000) Trehalose 493 6,6'-dimycolate (Cord factor) enhances neovascularization through vascular endothelial 494 growth factor production by neutrophils and macrophages. Infect Immun. 68, 2043-2052 495 46 Walton, E. M., Cronan, M. R., Cambier, C. J., Rossi, A., Marass, M., Foglia, M. D., Brewer, 496 W. J., Poss, K. D., Stainier, D. Y. R., Bertozzi, C. R. and Tobin, D. M. (2018) Cyclopropane 497 Modification of Trehalose Dimycolate Drives Granuloma Angiogenesis and Mycobacterial 498 Growth through Vegf Signaling. Cell Host Microbe. 24, 514-525 e516 499 47 Korbee, C. J., Heemskerk, M. T., Kocev, D., van Strijen, E., Rabiee, O., Franken, K., Wilson, 500 L., Savage, N. D. L., Dzeroski, S., Haks, M. C. and Ottenhoff, T. H. M. (2018) Combined chemical 501 genetics and data-driven bioinformatics approach identifies receptor tyrosine kinase 502 inhibitors as host-directed antimicrobials. Nat Commun. 9, 358 503 48 Harding, J. S., Herbath, M., Chen, Y., Rayasam, A., Ritter, A., Csoka, B., Hasko, G., Michael, 504 I. P., Fabry, Z., Nagy, A. and Sandor, M. (2019) VEGF-A from Granuloma Macrophages 505 Regulates Granulomatous Inflammation by a Non-angiogenic Pathway during Mycobacterial 506 Infection. Cell Rep. 27, 2119-2131 e2116 507 49 Babu, K., Murthy, P. R. and Murthy, K. R. (2010) Intravitreal bevacizumab as an adjunct 508 in a patient with presumed vascularised choroidal tubercular granuloma. Eye (London, 509 England). 24, 397-399 510 50 Lee Kim, E., Rodger, D. C. and Rao, N. A. (2017) Choroidal neovascularization secondary 511 to tuberculosis: Presentation and management. American journal of ophthalmology case 512 reports. 5, 124-129 513 51 Taguchi, M., Sakurai, Y., Kanda, T. and Takeuchi, M. (2017) Anti-VEGF therapy for 514 central retinal vein occlusion caused by tuberculosis-associated uveitis: a case report. 515 International medical case reports journal. 10, 139-141 516

52 Yuksel, E. and Ozdek, S. (2013) Unusual presentation of ocular tuberculosis: multiple 517 chorioretinitis, retinal vasculitis and ischaemic central retinal vein occlusion. Clinical & 518 experimental optometry. 96, 428-429 519 53 Julian, K., Terrada, C., Fardeau, C., Cassoux, N., Francais, C., LeHoang, P. and Bodaghi, B. 520 (2011) Intravitreal bevacizumab as first local treatment for uveitis-related choroidal 521 neovascularization: long-term results. Acta ophthalmologica. 89, 179-184 522 54 Lodhi, S. A., Saifuddin, K. and Devulapally, S. (2017) Inflammatory choroidal 523 neovascular membrane after healed tuberculous choroidal granuloma. GMS ophthalmology 524 cases. 7, Doc06 525 55 Jain, S., Bajgai, P., Tigari, B., Sharma, K., Sharma, A., Gupta, V. and Singh, R. (2016) 526 Bevacizumab for paradoxical worsening treatment adjunct in HIV patient with choroidal 527 tuberculoma. Journal of ophthalmic inflammation and infection. 6, 42 528 56 Ruiz-Cruz, M., Espinosa, E., Romero, K. and Reyes-Teran, G. (2011) Bevacizumab 529 reverts serous retinal detachment caused by tuberculosis-associated immune reconstitution 530 inflammatory syndrome. AIDS (London, England). 25, 1241-1243 531 57 Bansal, R., Beke, N., Sharma, A. and Gupta, A. (2013) Intravitreal bevacizumab as an 532 adjunct in the management of a vascular choroidal granuloma. BMJ case reports. 2013 533 58 Invernizzi, A., Franzetti, F., Viola, F., Meroni, L. and Staurenghi, G. (2015) Optic nerve 534 head tubercular granuloma successfully treated with anti-VEGF intravitreal injections in 535 addition to systemic therapy. European journal of ophthalmology. 25, 270-272 536 59 Jain, S., Agarwal, A. and Gupta, V. (2019) Resolution of Large Choroidal Tuberculoma 537 following Monotherapy with Intravitreal Ranibizumab. Ocular immunology and inflammation, 538 1-4 539 60 Hudock, T. A., Foreman, T. W., Bandyopadhyay, N., Gautam, U. S., Veatch, A. V., LoBato, 540 D. N., Gentry, K. M., Golden, N. A., Cavigli, A., Mueller, M., Hwang, S. A., Hunter, R. L., Alvarez, X., 541 Lackner, A. A., Bader, J. S., Mehra, S. and Kaushal, D. (2017) Hypoxia Sensing and Persistence 542 Genes Are Expressed during the Intragranulomatous Survival of Mycobacterium tuberculosis. 543 Am J Respir Cell Mol Biol. 56, 637-647 544 61 Rao, S. P., Alonso, S., Rand, L., Dick, T. and Pethe, K. (2008) The protonmotive force is 545 required for maintaining ATP homeostasis and viability of hypoxic, nonreplicating 546 Mycobacterium tuberculosis. Proc Natl Acad Sci U S A. 105, 11945-11950 547 62 Prosser, G., Brandenburg, J., Reiling, N., Barry, C. E., 3rd, Wilkinson, R. J. and Wilkinson, 548 K. A. (2017) The bacillary and macrophage response to hypoxia in tuberculosis and the 549 consequences for T cell antigen recognition. Microbes Infect. 19, 177-192 550 63 Rustad, T. R., Sherrid, A. M., Minch, K. J. and Sherman, D. R. (2009) Hypoxia: a window 551 into Mycobacterium tuberculosis latency. Cell Microbiol. 11, 1151-1159 552 64 Mehra, S., Foreman, T. W., Didier, P. J., Ahsan, M. H., Hudock, T. A., Kissee, R., Golden, N. 553 A., Gautam, U. S., Johnson, A. M., Alvarez, X., Russell-Lodrigue, K. E., Doyle, L. A., Roy, C. J., 554 Blanchard, J. L., Khader, S. A., Lackner, A. A., Sherman, D. R. and Kaushal, D. (2015) The DosR 555 Regulon Modulates Adaptive Immunity and is Essential for M. tuberculosis Persistence. Am J 556 Respir Crit Care Med 557 65 Eisen, S., Pealing, L., Aldridge, R. W., Siedner, M. J., Necochea, A., Leybell, I., Valencia, T., 558 Herrera, B., Wiles, S., Friedland, J. S., Gilman, R. H. and Evans, C. A. (2013) Effects of ascent to 559 high altitude on human antimycobacterial immunity. PLoS ONE. 8, e74220 560 66 Meylan, P. R., Richman, D. D. and Kornbluth, R. S. (1992) Reduced intracellular growth 561 of mycobacteria in human macrophages cultivated at physiologic oxygen pressure. Am Rev 562 Respir Dis. 145, 947-953 563 67 Nickel, D., Busch, M., Mayer, D., Hagemann, B., Knoll, V. and Stenger, S. (2012) Hypoxia 564 triggers the expression of human beta defensin 2 and antimicrobial activity against 565 Mycobacterium tuberculosis in human macrophages. J Immunol. 188, 4001-4007 566

68 Matta, S. K. and Kumar, D. (2016) Hypoxia and classical activation limits 567 Mycobacterium tuberculosis survival by Akt-dependent glycolytic shift in macrophages. Cell 568 Death Discov. 2, 16022 569 69 Fortin, A., Abel, L., Casanova, J. L. and Gros, P. (2007) Host genetics of mycobacterial 570 diseases in mice and men: forward genetic studies of BCG-osis and tuberculosis. Annual 571 review of genomics and human genetics. 8, 163-192 572 70 Braverman, J., Sogi, K. M., Benjamin, D., Nomura, D. K. and Stanley, S. A. (2016) HIF-573 1alpha Is an Essential Mediator of IFN-gamma-Dependent Immunity to Mycobacterium 574 tuberculosis. J. Immunol. 575 71 Elks, P. M., Brizee, S., van der Vaart, M., Walmsley, S. R., van Eeden, F. J., Renshaw, S. A. 576 and Meijer, A. H. (2013) Hypoxia Inducible Factor Signaling Modulates Susceptibility to 577 Mycobacterial Infection via a Nitric Oxide Dependent Mechanism. PLoS Pathog. 9, e1003789 578 72 Shi, L., Eugenin, E. A. and Subbian, S. (2016) Immunometabolism in Tuberculosis. 579 Frontiers in immunology. 7, 150 580 73 Phong, W. Y., Lin, W., Rao, S. P., Dick, T., Alonso, S. and Pethe, K. (2013) Characterization 581 of phosphofructokinase activity in Mycobacterium tuberculosis reveals that a functional 582 glycolytic carbon flow is necessary to limit the accumulation of toxic metabolic intermediates 583 under hypoxia. PLoS ONE. 8, e56037 584 74 Ong, C. W. M., Fox, K., Ettorre, A., Elkington, P. T. and Friedland, J. S. (2018) Hypoxia 585 increases neutrophil-driven matrix destruction after exposure to Mycobacterium 586 tuberculosis. Scientific reports. 8, 11475 587 75 Kubler, A., Luna, B., Larsson, C., Ammerman, N. C., Andrade, B. B., Orandle, M., Bock, K. 588 W., Xu, Z., Bagci, U., Mollura, D. J., Marshall, J., Burns, J., Winglee, K., Ahidjo, B. A., Cheung, L. S., 589 Klunk, M., Jain, S. K., Kumar, N. P., Babu, S., Sher, A., Friedland, J. S., Elkington, P. T. and Bishai, 590 W. R. (2015) Mycobacterium tuberculosis dysregulates MMP/TIMP balance to drive rapid 591 cavitation and unrestrained bacterial proliferation. The Journal of pathology. 235, 431-444 592 76 Cardona, P., Allain, S., Altare, F., Kim, M. and Russell, D. G. (2009) Foamy macrophages 593 and the progression of the human tuberculosis granuloma. Nature Immunology. 10, 943-948 594 77 McNamee, E. N., Korns Johnson, D., Homann, D. and Clambey, E. T. (2013) Hypoxia and 595 hypoxia-inducible factors as regulators of T cell development, differentiation, and function. 596 Immunol Res. 55, 58-70 597 78 Harding, J., Ritter, A., Rayasam, A., Fabry, Z. and Sandor, M. (2015) Lymphangiogenesis 598 Is Induced by Mycobacterial Granulomas via Vascular Endothelial Growth Factor Receptor-3 599 and Supports Systemic T-Cell Responses against Mycobacterial Antigen. Am J Pathol. 185, 600 432-445 601 79 Dartois, V. (2014) The path of anti-tuberculosis drugs: from blood to lesions to 602 mycobacterial cells. Nat Rev Microbiol. 12, 159-167 603 80 Xu, Y., Wang, L., Zimmerman, M. D., Chen, K. Y., Huang, L., Fu, D. J., Kaya, F., Rakhilin, N., 604 Nazarova, E. V., Bu, P., Dartois, V., Russell, D. G. and Shen, X. (2018) Matrix metalloproteinase 605 inhibitors enhance the efficacy of frontline drugs against Mycobacterium tuberculosis. PLoS 606 Pathog. 14, e1006974 607 81 Via, L. E., Lin, P. L., Ray, S. M., Carrillo, J., Allen, S. S., Eum, S. Y., Taylor, K., Klein, E., 608 Manjunatha, U., Gonzales, J., Lee, E. G., Park, S. K., Raleigh, J. A., Cho, S. N., McMurray, D. N., 609 Flynn, J. L. and Barry, C. E., 3rd. (2008) Tuberculous granulomas are hypoxic in guinea pigs, 610 rabbits, and nonhuman primates. Infect Immun. 76, 2333-2340 611 82 Kramnik, I., Demant, P. and Bloom, B. B. (1998) Susceptibility to tuberculosis as a 612 complex genetic trait: analysis using recombinant congenic strains of mice. Novartis 613 Foundation symposium. 217, 120-131; discussion 132-127 614 83 Driver, E. R., Ryan, G. J., Hoff, D. R., Irwin, S. M., Basaraba, R. J., Kramnik, I. and Lenaerts, 615 A. J. (2012) Evaluation of a mouse model of necrotic granuloma formation using C3HeB/FeJ 616

mice for testing of drugs against Mycobacterium tuberculosis. Antimicrob Agents Chemother. 617 56, 3181-3195 618 84 Harper, J., Skerry, C., Davis, S. L., Tasneen, R., Weir, M., Kramnik, I., Bishai, W. R., 619 Pomper, M. G., Nuermberger, E. L. and Jain, S. K. (2012) Mouse model of necrotic tuberculosis 620 granulomas develops hypoxic lesions. J Infect Dis. 205, 595-602 621 85 Smith, C. M., Proulx, M. K., Olive, A. J., Laddy, D., Mishra, B. B., Moss, C., Gutierrez, N. M., 622 Bellerose, M. M., Barreira-Silva, P., Phuah, J. Y., Baker, R. E., Behar, S. M., Kornfeld, H., Evans, T. 623 G., Beamer, G. and Sassetti, C. M. (2016) Tuberculosis Susceptibility and Vaccine Protection 624 Are Independently Controlled by Host Genotype. mBio. 7 625 626

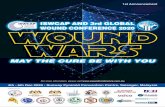
Figure legends 627 Figure 1: The “bacterial tumour”: similarities between the TB granuloma and solid tumours. 628 (Top left) Both lesions are hypoxic and drive the formation of a leaky and haemostatic vasculature 629 through the production of VEGF and ANG-2. The lack of sufficient perfusion prevents the 630 penetration of drugs into each lesion resulting in phenotypic insensitivity. Activation of haemostasis 631 is a common strategy to subvert the immune response. The hypoxic conditions activate a HIF1-632 mediated transcriptional program that also feed into metabolism and tissue destruction. 633 (Top right) There are shared immunological markers of disease prognosis. A robust type 1 immune 634 response with spatial penetration of lymphocytes is associated with lesion apoptosis and immune 635 containment. A skewing to a type 2 response with insufficient lymphocyte penetration is associated 636 with poor immune control and a worse prognosis. 637 (Bottom right) Matrix metalloprotease (MMP)-mediated remodelling and destruction of the 638 surrounding stromal tissue is essential to facilitate lesion spread from primary foci through 639 surrounding tissue and eventually facilitating haematogenous spread. MMP activity is increased by 640 hypoxia and the HIF1-mediated transcriptional program. 641 (Bottom left) Metabolic syndrome-associated diseases diabetes and dyslipidaemia are important 642 comorbidities for both diseases. At a molecular level, these comorbidities feed lesions with glucose 643 and lipid. In the TB granuloma this results in loss of effective immune control and fuels bacterial 644 growth, while in cancer the malignant cells use the nutrients. 645 646 Figure 2: VEGFR inhibition drives a granuloma maturation phenotype in zebrafish 647 (A) Representative image of an organised cellular zebrafish-M. marinum granuloma. 648 (B) Representative image of an organised necrotic zebrafish-M. marinum granuloma. 649 (C) Quantification of granuloma necrosis in 6 week-post infection zebrafish adults treated with 1 650 µM pazopanib as indicated. Each dot represents a single granuloma. 651

TB dissemination
Cancer metastasis
MMP-mediated matrix destruction
Vascular dysfunction: weak perfusion
Drug insensitivity
M1 Th1
M2 Th2
Good prognosis Lesion apoptosis
Poor prognosis Immune evasion
Hypoxia / HIF1alpha
O2
Vascular dysfunction: thrombosis
TNF, IFNgamma
IL-10, PD-L1
Aerobic glycolysis Diabetes Dyslipidemia Citrate / acetyl CoA
Lipid accumulation
Granuloma caseation
Tumour survival