1 Review of Antiretroviral Therapy in Adults HAIVN Harvard Medical School AIDS Initiative in...
17
1 Review of Antiretroviral Therapy in Adults HAIVN Harvard Medical School AIDS Initiative in Vietnam
Transcript of 1 Review of Antiretroviral Therapy in Adults HAIVN Harvard Medical School AIDS Initiative in...

1
Review of Antiretroviral Therapy in Adults
HAIVNHarvard Medical School AIDS
Initiative in Vietnam

2
Learning Objectives
By the end of this session, participants should be able to:
Explain the criteria for starting ART Identify the first line ARV regimens Describe the common side effects
caused by NRTIs and NNRTIs Describe the protocol for performing
routine follow-up with ARV patients

3
Drug Classes of Antiretrovirals (ARV)
1. Nucleoside Reverse Transcriptase Inhibitors
(NRTI)
2. Non-nucleoside Reverse Transcriptase
Inhibitors (NNRTI)
3. Protease Inhibitors (PI)
4. Fusion/Entry Inhibitors
5. Integrase Inhibitors

4
ARV Drugs Currently Available in the World and Vietnam
Nucleoside/Nucleotide RTI
AZT / Zidovudine
d4T / Stavudine
3TC / Lamivudine
ddI / didanosine
ABC / Abacavir
TDF / Tenofovir
FTC /Emtricitabine
Non-nucleoside RTI
NVP /Nevirapine
DLV / Delavirdine
EFV / Efavirenz
ETR / Etravirine
Protease inhibitors
SQV / Saquinavir
RTV / Ritonavir
IDV / Indinavir
NFV / Nelfinavir
APV / Amprenavir
LPVr / Lopinavir + ritonavir
ATV / Atazanavir
Fos-Amprenavir
DRV / Darunavir
TPV / Tipranavir
Integrase inhibitors
RAL / Raltegravir
Fusion/Entry inhibitors
MVC / Mariviroc
ENF / Enfuvirtide
5
Goals of ARV Therapy
Inhibit HIV replication• As low as possible (undetectable)• For as long as possible
Allow recovery of the immune system Prevent opportunistic infection Improve survival, health and quality
of life

6
When to Start ART?
ARV therapy is never an emergency Patients with high CD4 are not at risk
for OIs and can delay ARV treatment Decide when to start ARV based on:
Risks Benefits
• Allergy• Side Effects• Adherence• Costs
• Improve immune function • Improve quality of life• Decrease risk for OIs
7
When to Start ARV in Vietnam
Patients with: CD4 ≤ 350 cells/mm³ irrespective of
clinical stage Clinical stage 3 or 4 irrespective of CD4
cell count
Modification and Supplement to the Guidelines for Diagnosis and Treatment of HIV/AIDS, MOH November 2011
8
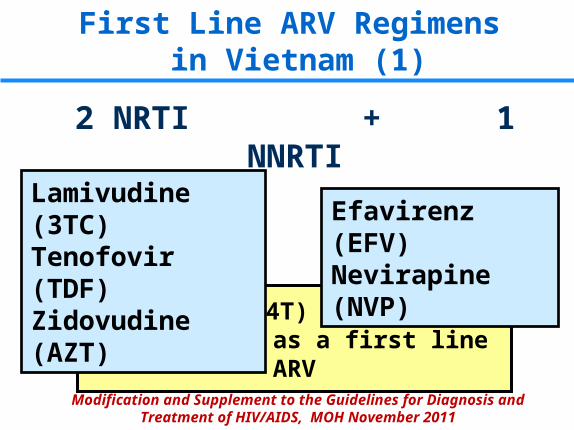
First Line ARV Regimens in Vietnam (1)
2 NRTI + 1 NNRTI
Stavudine (D4T) is no longer recommended as a first line ARV
Lamivudine (3TC)Tenofovir (TDF)Zidovudine (AZT)
Efavirenz (EFV)Nevirapine (NVP)
Modification and Supplement to the Guidelines for Diagnosis and Treatment of HIV/AIDS, MOH November 2011
9
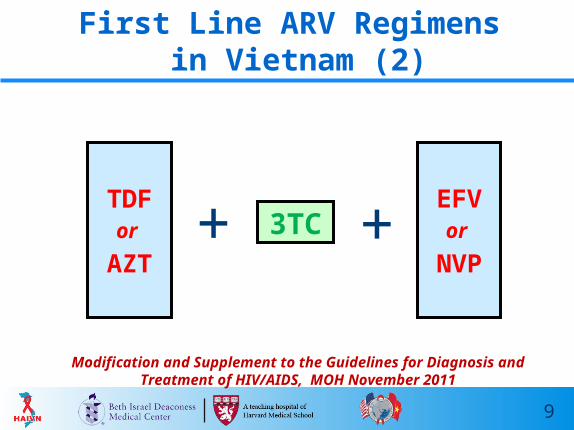
First Line ARV Regimens in Vietnam (2)
3TCEFVor
NVP+
Modification and Supplement to the Guidelines for Diagnosis and Treatment of HIV/AIDS, MOH November 2011
+TDFor
AZT

10
First Line ARV Regimens in Vietnam (3)
Priority Regimens Alternative Regimens
TDF/3TC/EFVTDF/3TC/NVP
AZT/3TC/EFVAZT/3TC/NVP
Modification and Supplement to the Guidelines for Diagnosis and Treatment of HIV/AIDS, MOH November 2011

11
Side Effects of 1st Line ARVs
11
Class Drug Common Side Effects
NRTI
d4T• Peripheral neuropathy• Lipoatrophy• Lactic acidosis
AZT• Headache, nausea• Anemia
TDF • Renal Dysfunction
NNRTIEFV
• Rash• CNS symptoms• Teratogenicity
NVP• Rash• Hepatotoxicity

12
Monitoring Patients on ART

13
Monitoring: How Often?
Month 1 Month 2 Month 3+
Once per week every 2 weeksOnce per month
orevery 2 months
If the clinical situation is stable:
14
What to Monitor? (1)
Adherence Monitoring
Assess missed doses
Provide counseling about adherence, prevention, and healthy living
Clinical Monitoring Weight,
temperature WHO Clinical Stage ARV side effects or
toxicity Signs of IRIS

15
What to Monitor? (2)
Laboratory Monitoring:
Test Frequency
CBC Every 6 monthsAlso after 1st month if on AZT
ALT Every 6 monthsAlso after 1st month if on NVP
CD4 Every 6 months
Lipids and Glucose
Every year
Creatinine Every 6 months if on TDF

16
Key Points
Patients with clinical stage 3 or 4 or CD4 ≤ 350 should start ART
Two priority first ARV regimens in Vietnam:• TDF + 3TC + EFV• TDF + 3TC + NVP
All ART patients need routine clinical and laboratory monitoring

17
Thank You!
Questions?