1 Pulmonary Function Tests Wanida Paoin. 2 Objectives Review basic pulmonary anatomy and lung...
48
1 Pulmonary Function Tests Wanida Paoin
-
Upload
caiden-fiveash -
Category
Documents
-
view
228 -
download
2
Transcript of 1 Pulmonary Function Tests Wanida Paoin. 2 Objectives Review basic pulmonary anatomy and lung...
1
Pulmonary Function Tests
Wanida Paoin
2
Objectives
Review basic pulmonary anatomy and lung volume.
Indication for PFTs. Technique and basic interpretation of
spirometry. Difference between obstructive and restrictive
lung disease. Clinically application
3
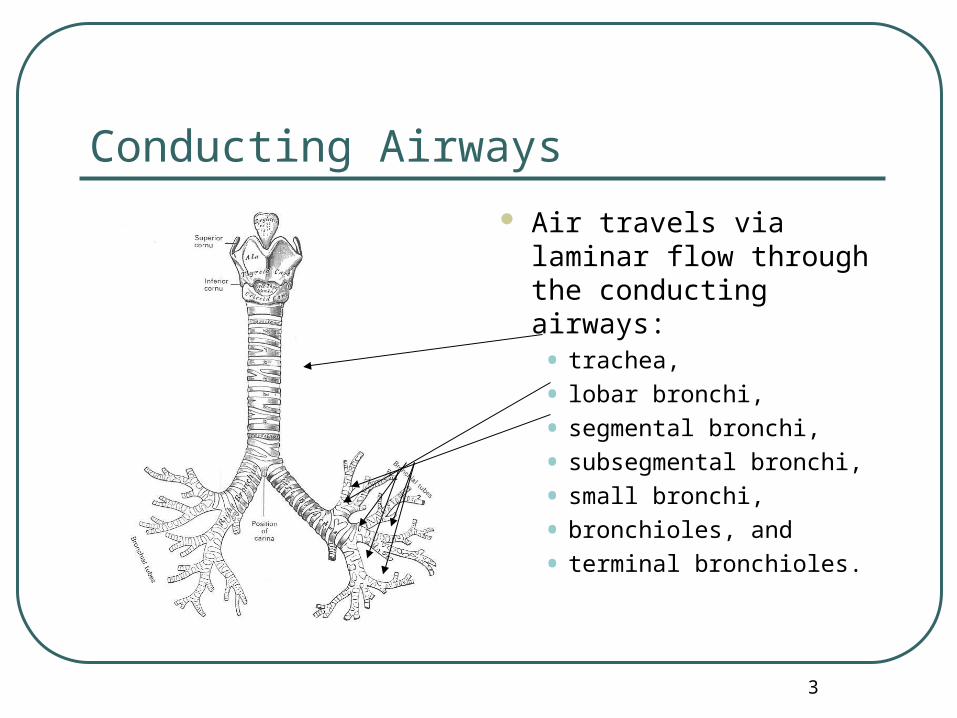
Conducting Airways
Air travels via laminar flow through the conducting airways:• trachea,
• lobar bronchi,
• segmental bronchi,
• subsegmental bronchi,
• small bronchi,
• bronchioles, and
• terminal bronchioles.
4
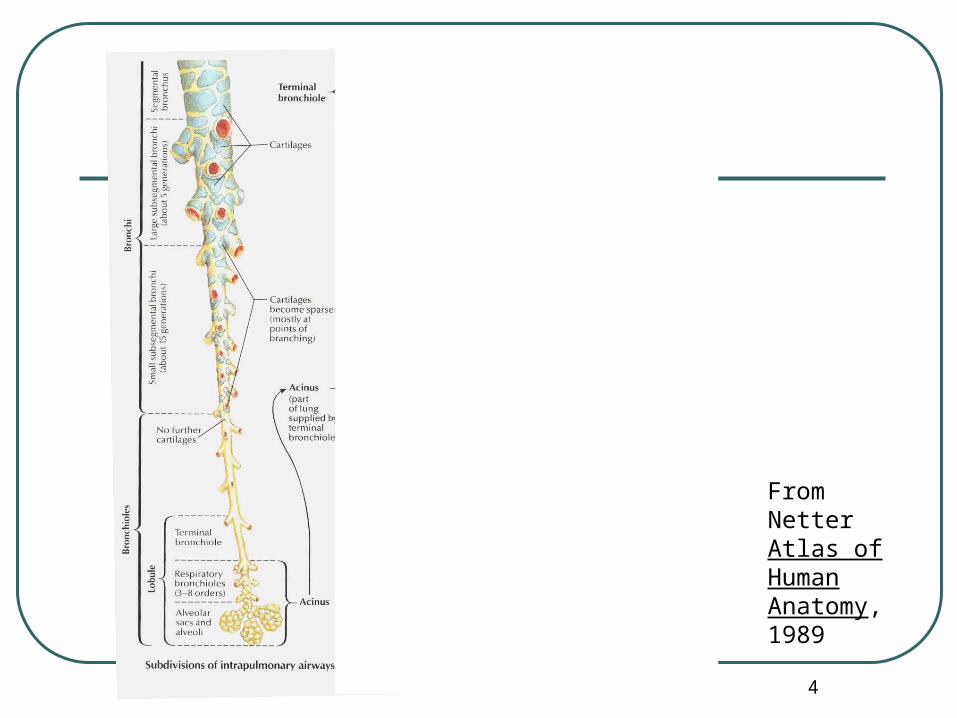
From Netter Atlas of Human Anatomy, 1989
5
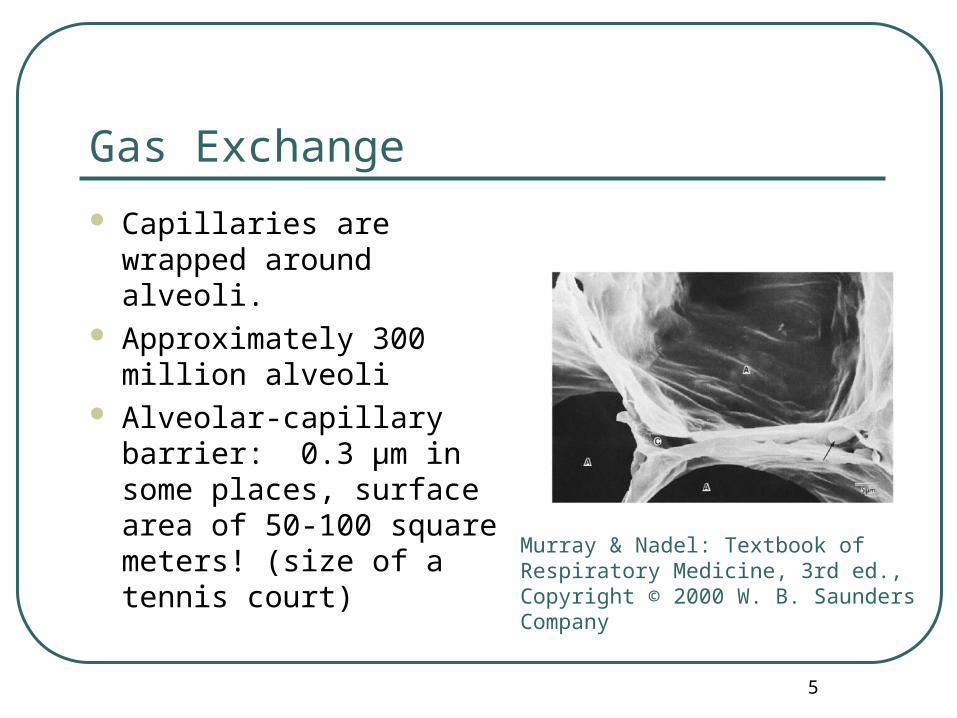
Gas Exchange
Capillaries are wrapped around alveoli.
Approximately 300 million alveoli
Alveolar-capillary barrier: 0.3 μm in some places, surface area of 50-100 square meters! (size of a tennis court)
Murray & Nadel: Textbook of Respiratory Medicine, 3rd ed., Copyright © 2000 W. B. Saunders Company
6
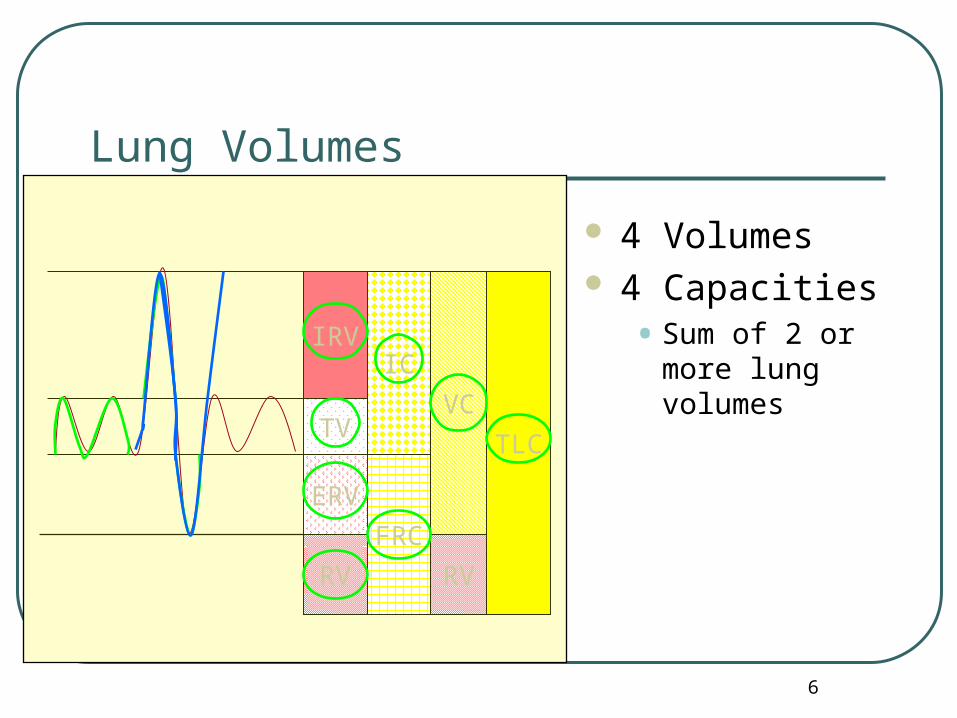
Lung Volumes
IRV
ERV
4 Volumes 4 Capacities
• Sum of 2 or more lung volumes
RV
IC
FRC
VC
TLC
RV
TV

7
Pulmonary Function Tests
• Pulse oximetry • Blood gases • End tidal CO2
• Spirometry• Peak expiratory flow rate • Bronchial challenge testing
• Exercise tests • Respiratory muscle pressure measurement• Lung volumes by helium dilution or body
plethysmography• Diffusing capacity
8
Pulmonary Function Tests
Evaluates 1 or more major aspects of the respiratory system• Lung volumes
• Airway function
• Gas exchange
9
Indications
Detect disease Evaluate extent and monitor course of
disease Evaluate treatment Measure effects of exposures Assess risk for surgical procedures Assess bronchial hyperreactivity
10
Evaluate extent and monitor course of disease
Obstructive disease - asthma - FB - subglottic, tracheal stenosis - tracheomalacia - vascular ring - vocal cord paralysis

11
Evaluate extent and monitor course of disease
Restictive disease - external compression: thoracic cage abnormality, pleural effusion, pneumothorax, obesity, scoliosis - unexpanded lung: interstitial fibrosis, pulmonary edema - neuromuscular disease: poliomyelitis, myasthenia grevis
12
Importance
Patients and physicians have inaccurate perceptions of severity of airflow obstruction and/or severity of lung disease by physical exam
Provides objective evidence in identifying patterns of disease
13
Spirometry
Measurement of the pattern of air movement into and out of the lungs during controlled ventilatory maneuvers.
Silhouette of Hutchinson Performing Spirometry, From Chest, 2002
14
Limitation
They do not act alone. They act only to support
or exclude a diagnosis.
15
Mechanical Properties
Compliance• Describes the stiffness of the lungs
• volume / pressure
Elastic recoil• The tendency of the lung to return to it’s
resting state
• A lung that is fully stretched has more elastic recoil and thus larger maximal flows
16
Resistive Properties
Determined by airway caliber Affected by
• Lung volume
• Bronchial smooth muscles
• Airway collapsibility
17
Factors That Affect Lung Volumes
Age Sex Height Weight Race Disease
18
Special Considerations
Ability to perform spirometry dependent on developmental age of child, personality, and interest of the child.
Patients need a calm, relaxed environment and good coaching. Patience is key.
Even with the best of environments and coaching, a child may not be able to perform spirometry.
19
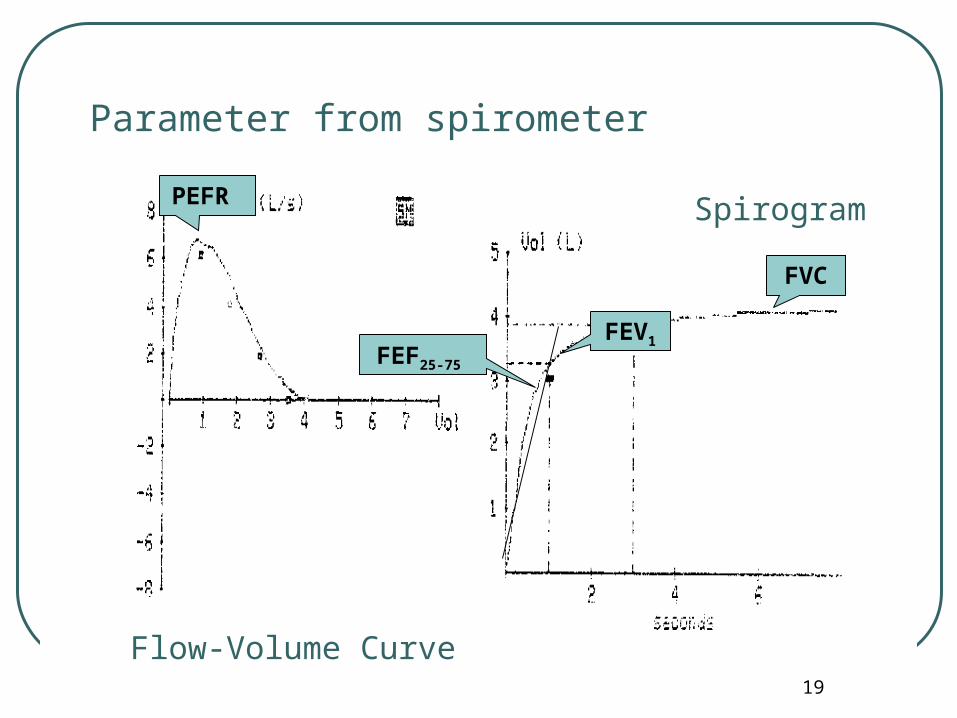
Parameter from spirometer
Flow-Volume Curve
Spirogram
FVC
FEV1FEF25-75
PEFR
20
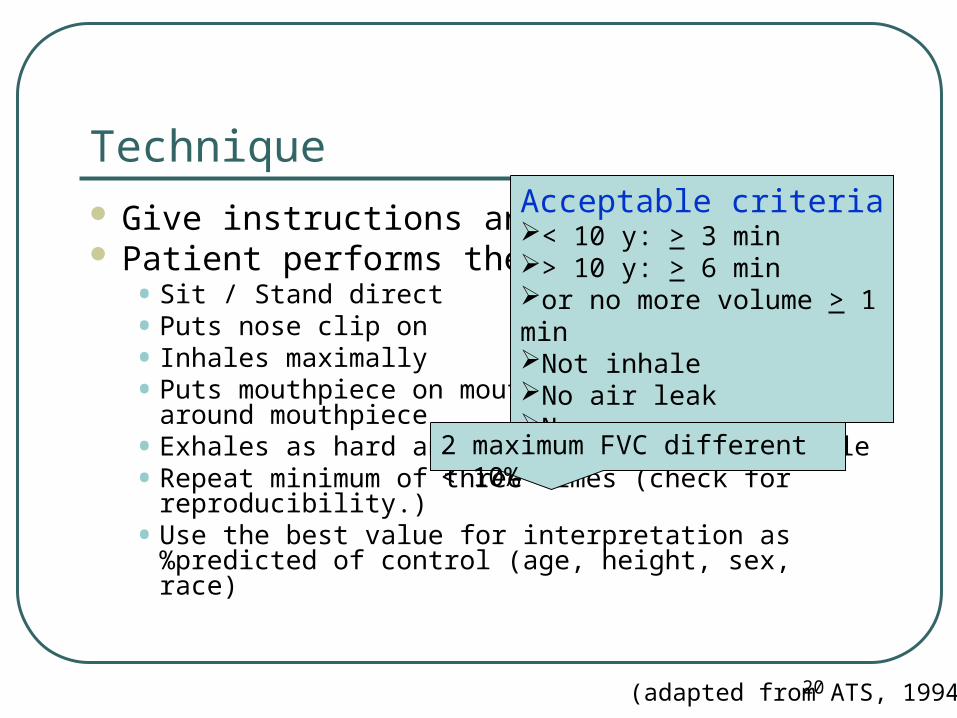
Technique Give instructions and demonstrate Patient performs the maneuver
•Sit / Stand direct•Puts nose clip on• Inhales maximally•Puts mouthpiece on mouth and closes lips
around mouthpiece•Exhales as hard and fast and long as possible•Repeat minimum of three times (check for
reproducibility.)•Use the best value for interpretation as
%predicted of control (age, height, sex, race)
(adapted from ATS, 1994)
Acceptable criteria< 10 y: > 3 min > 10 y: > 6 minor no more volume > 1 minNot inhaleNo air leakNo pause
2 maximum FVC different < 10%

21
FVC
Forced vital capacity (FVC):• Total volume of air that can
be exhaled forcefully from TLC
• The majority of FVC can be exhaled in <3 seconds in normal people, but often is much more prolonged in obstructive diseases
22
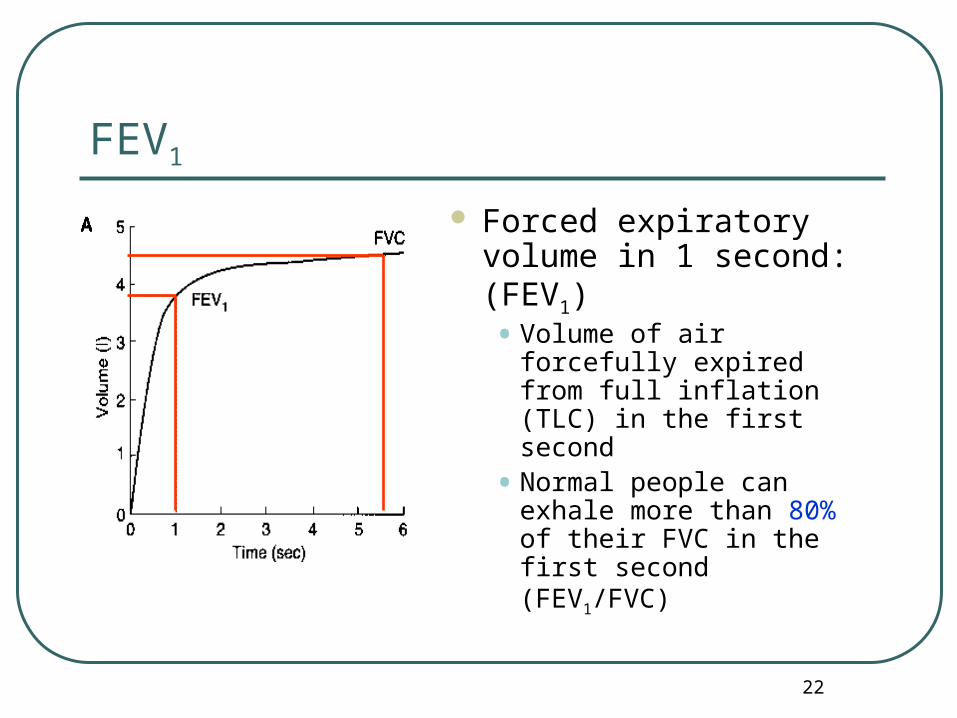
Forced expiratory volume in 1 second: (FEV1)• Volume of air forcefully
expired from full inflation (TLC) in the first second
• Normal people can exhale more than 80% of their FVC in the first second (FEV1/FVC)
FEV1
23
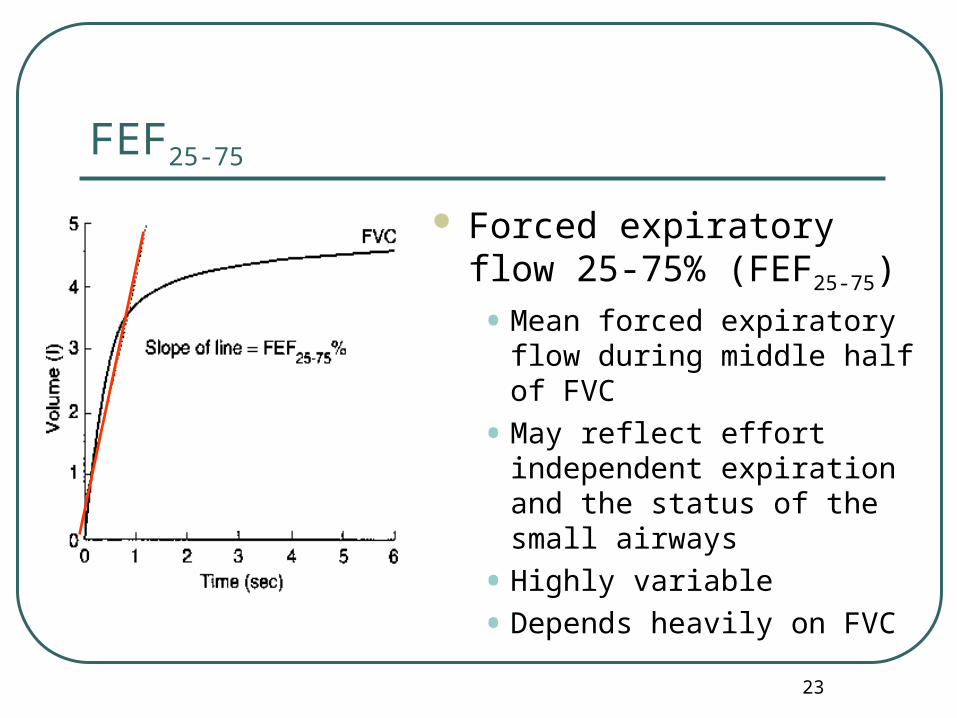
Forced expiratory flow 25-75% (FEF25-75)
• Mean forced expiratory flow during middle half of FVC
• May reflect effort independent expiration and the status of the small airways
• Highly variable
• Depends heavily on FVC
FEF25-75
24
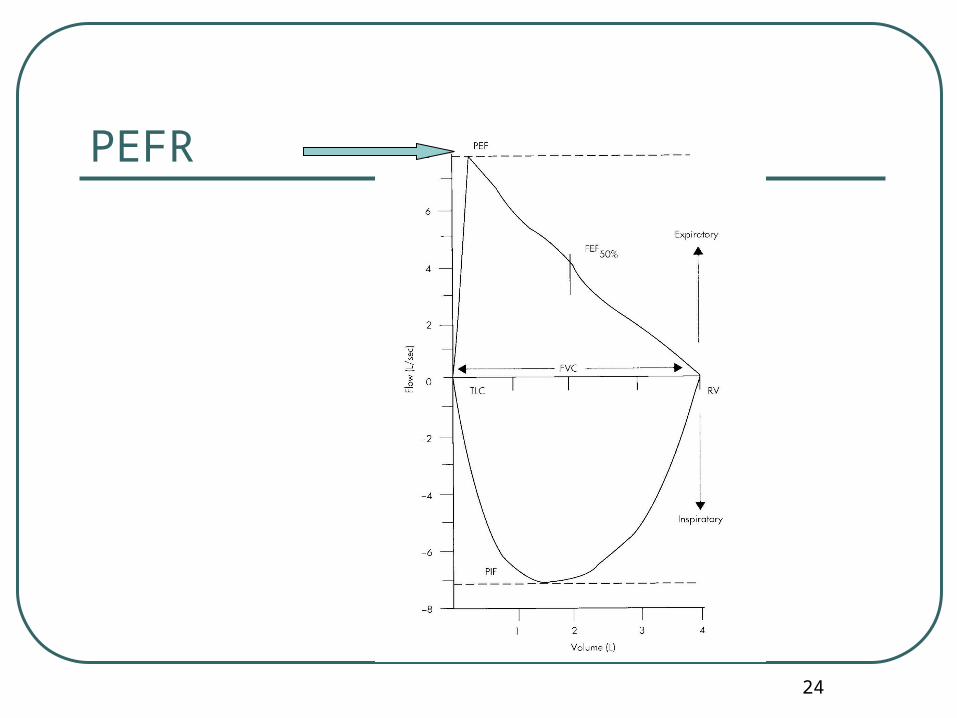
PEFR
25
PEFR
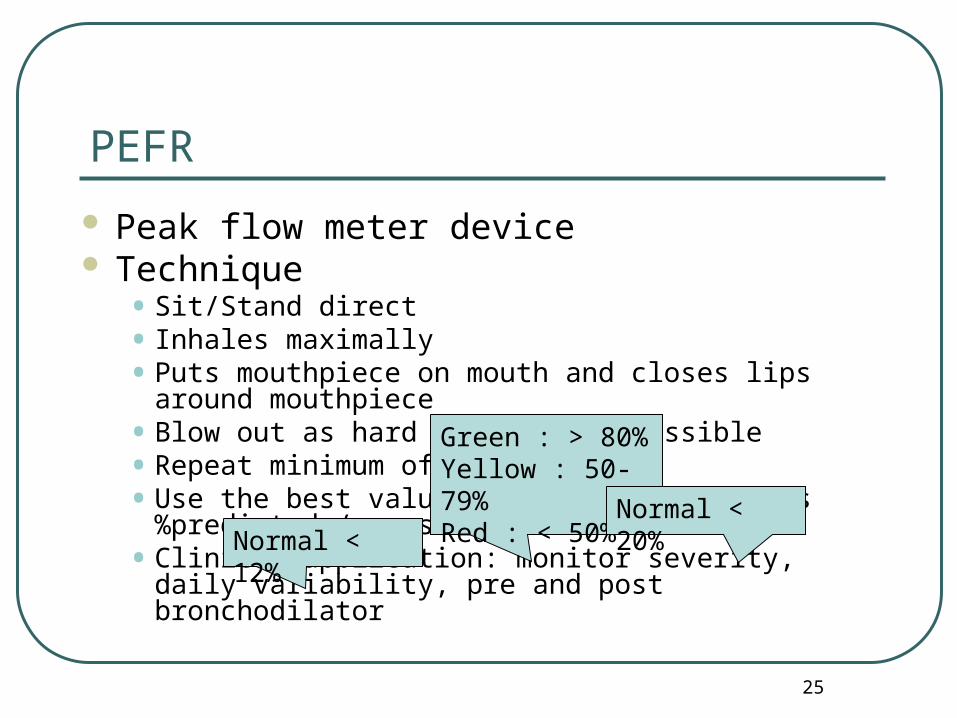
Peak flow meter device Technique
•Sit/Stand direct• Inhales maximally•Puts mouthpiece on mouth and closes lips
around mouthpiece•Blow out as hard and fast as possible•Repeat minimum of three times •Use the best value for interpretation as
%predicted / personal best •Clinical application: monitor severity, daily
variability, pre and post bronchodilator
Green : > 80%Yellow : 50-79%Red : < 50%
Normal < 20%Normal <
12%
26
Categories of Disease
Obstructive Restrictive Mixed
27
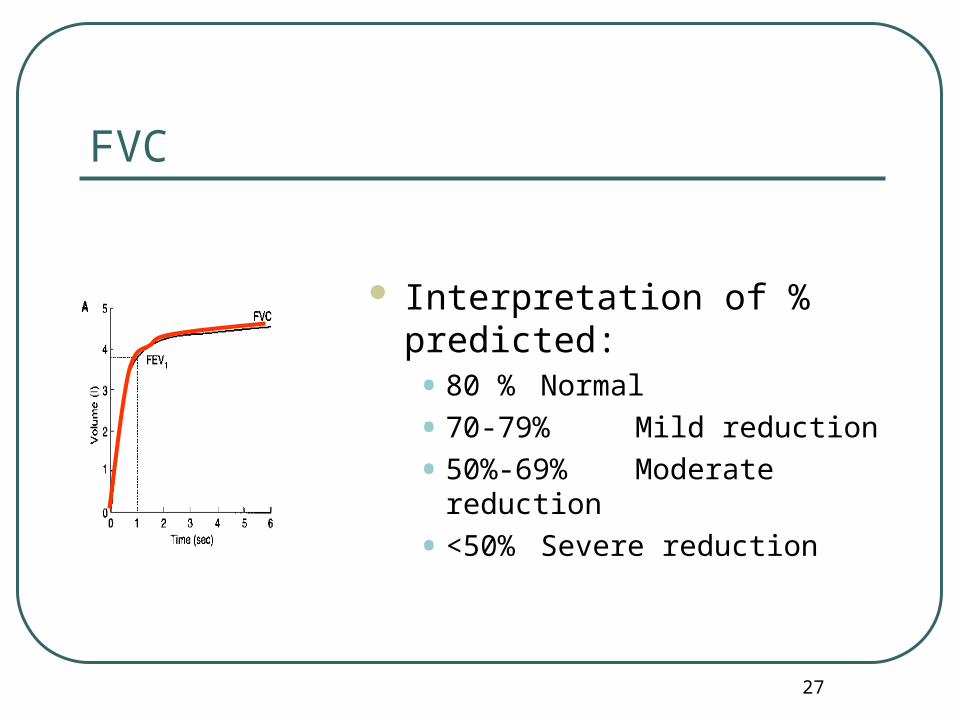
FVC
Interpretation of % predicted:• 80 % Normal
• 70-79% Mild reduction
• 50%-69% Moderate reduction
• <50% Severe reduction

28
FEV1
Interpretation of % predicted:• >80% Normal
• 65-79% Mild obstruction
• 50-64% Moderate obstruction
• <49% Severe obstruction
29
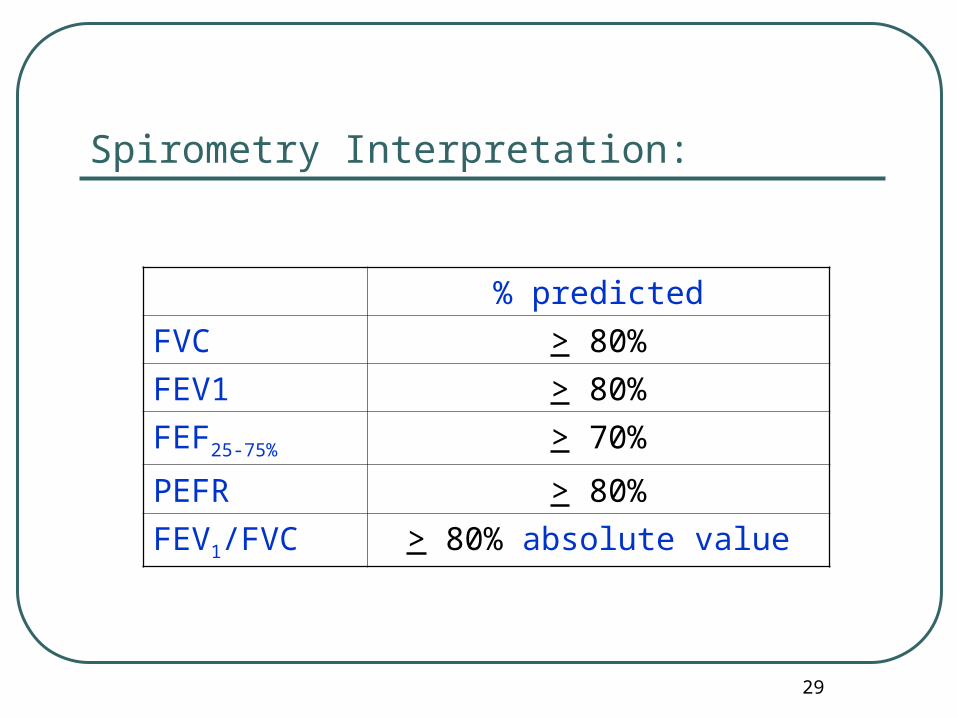
Spirometry Interpretation:
% predicted
FVC > 80%
FEV1 > 80%
FEF25-75% > 70%
PEFR > 80%
FEV1/FVC > 80% absolute value

30
Spirometry in Obstructive Disease
Slow rise in upstroke May not reach
plateau
31
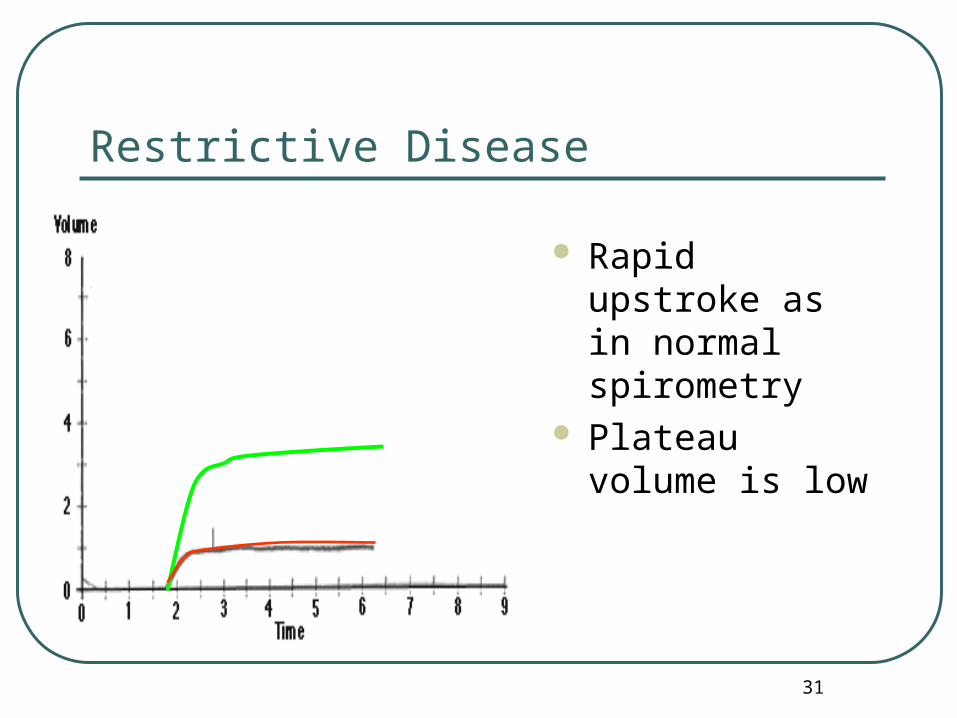
Restrictive Disease
Rapid upstroke as in normal spirometry
Plateau volume is low
32
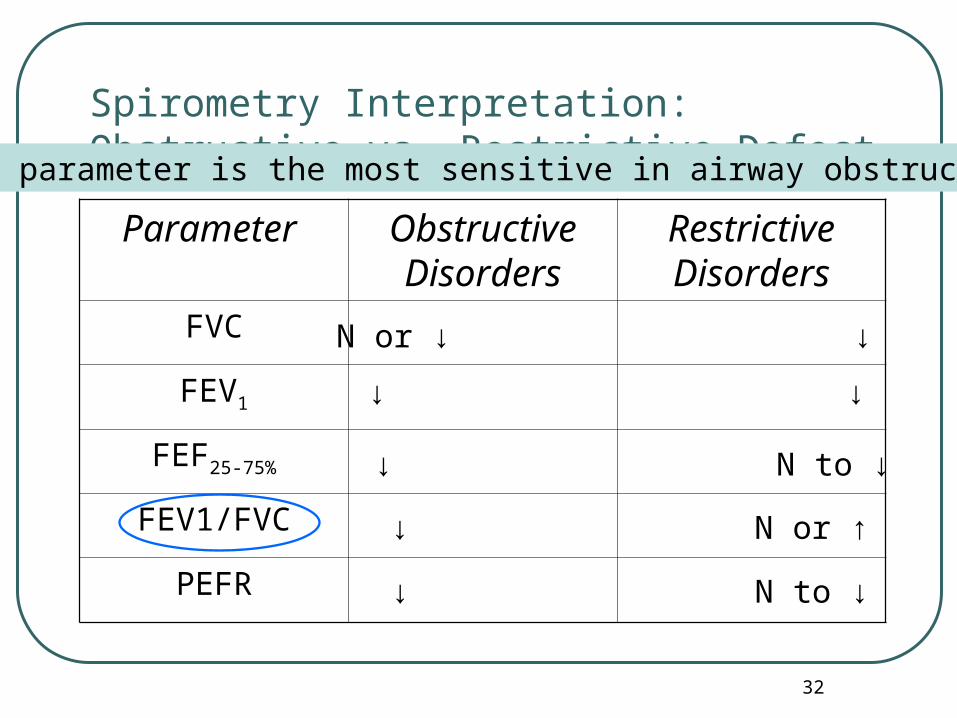
Spirometry Interpretation: Obstructive vs. Restrictive Defect
Parameter Obstructive Disorders
Restrictive Disorders
FVC
FEV1
FEF25-75%
FEV1/FVC
PEFR
N or ↓ ↓
↓ ↓
↓ N to ↓
↓ N or ↑
↓ N to ↓
What parameter is the most sensitive in airway obstruction?
33
Spirometry Interpretation: Obstructive Disorders
• Characterized by a limitation of expiratory airflow
Examples:
• Asthma
• Bronchiectasis
• COPD
• Cystic Fibrosis
Restrictive Disorders• Characterized by
reduced lung volumes/decreased lung compliance
Examples:
• Interstitial Fibrosis
• Kyphoscoliosis
• Obesity
• Lung Resection
• Neuromuscular diseases
• Cystic Fibrosis
34
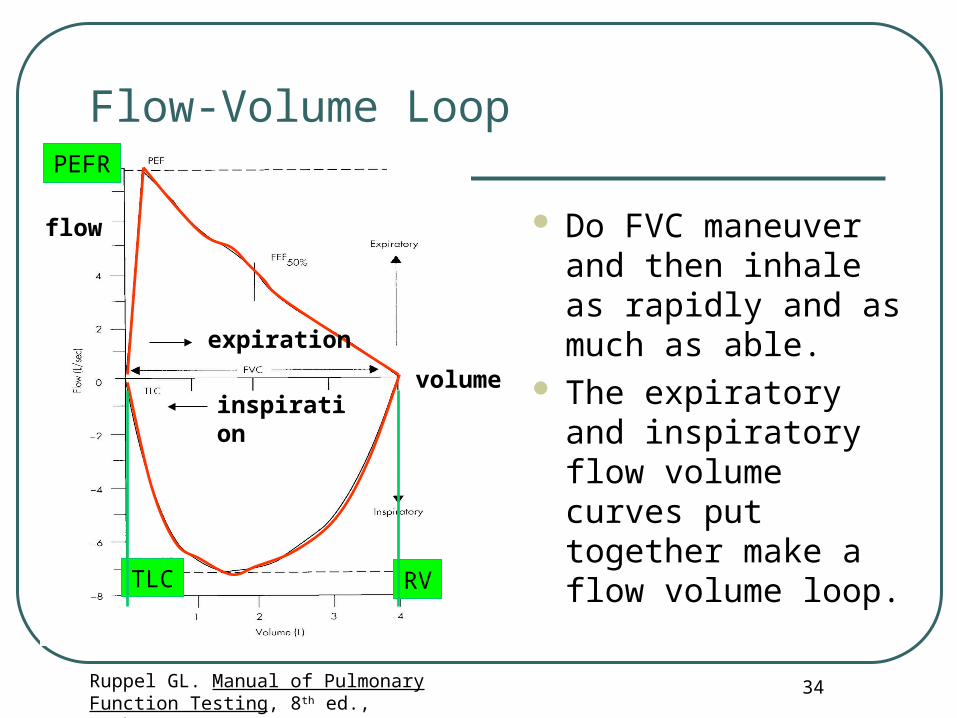
Flow-Volume Loop
Ruppel GL. Manual of Pulmonary Function Testing, 8th ed., Mosby 2003
Do FVC maneuver and then inhale as rapidly and as much as able.
The expiratory and inspiratory flow volume curves put together make a flow volume loop.RVTLC
PEFR
flow
volume
expiration
inspiration
35
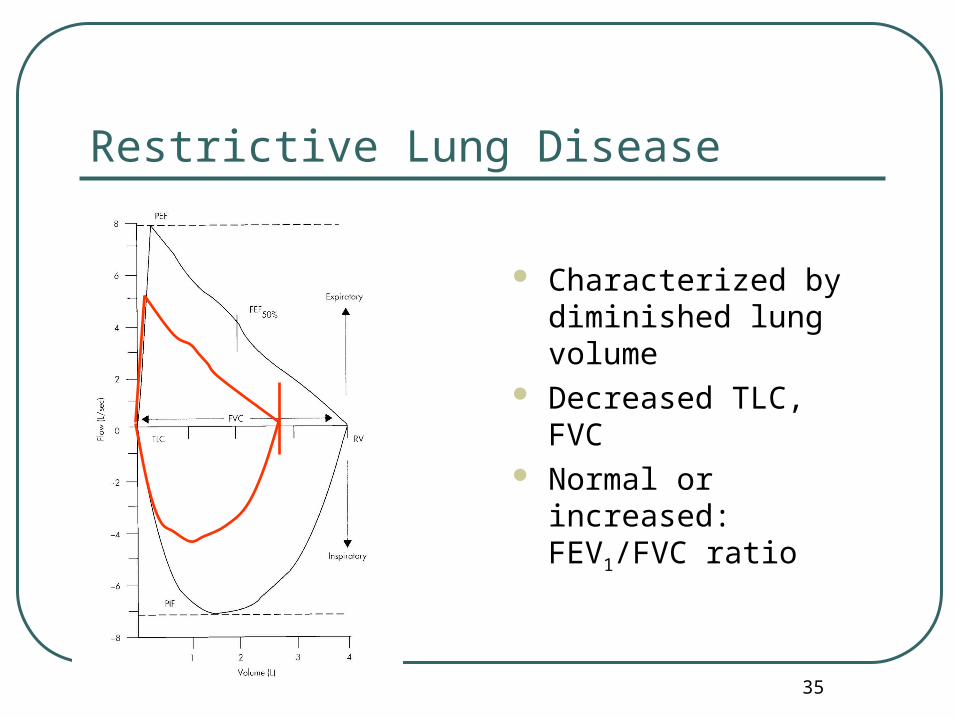
Restrictive Lung Disease
Characterized by diminished lung volume
Decreased TLC, FVC Normal or increased:
FEV1/FVC ratio
36
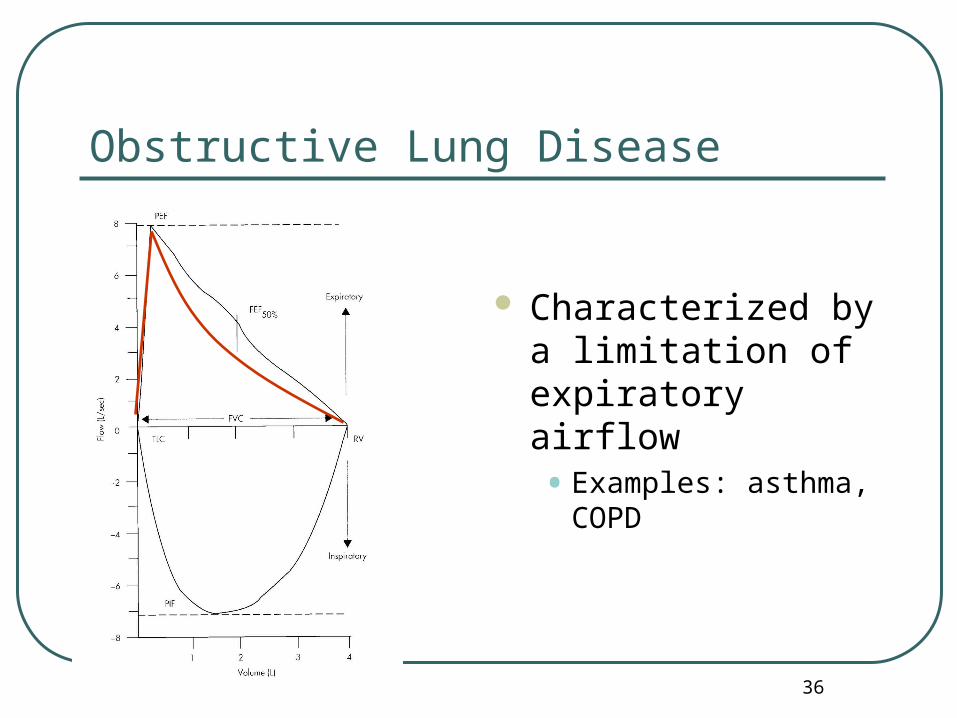
Obstructive Lung Disease
Characterized by a limitation of expiratory airflow• Examples: asthma,
COPD
37
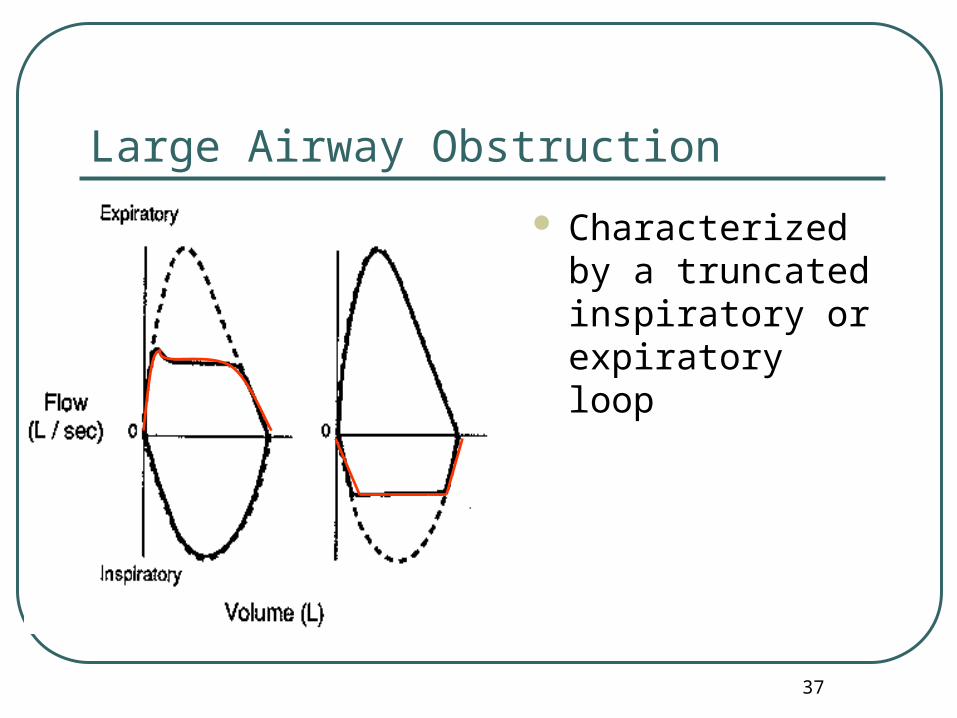
Large Airway Obstruction
Characterized by a truncated inspiratory or expiratory loop
38(Rudolph and Rudolph, 2003)
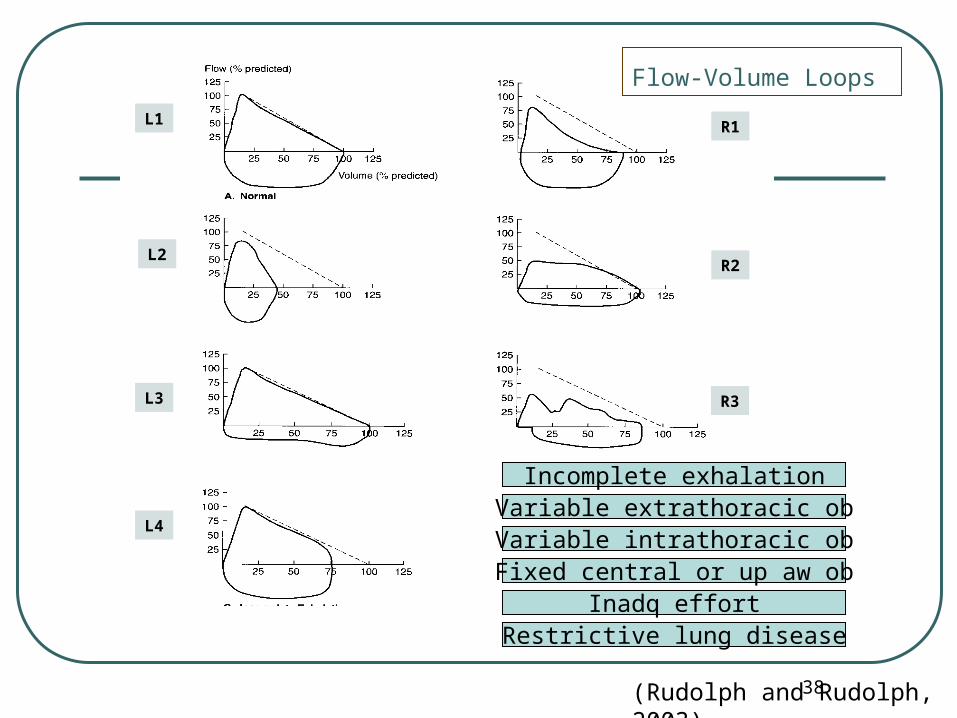
Flow-Volume Loops
Variable intrathoracic obFixed central or up aw ob
Inadq effort
Incomplete exhalationVariable extrathoracic ob
Restrictive lung disease
L1
L2
L3
L4
R2
R3
R1
39
Spirometry: Pre and Post Bronchodilator
Obtain spirogram and flow-volume loop. Pre and 15 minutes after administration of
the bronchodilator Salbutamol MDI 4 puffs via valve spacer
• Slow inhale
• Breath hold 5-10 sec.
• 5-10 sec pause between each puff. Reversibility: FEV1 / PEFR > 12% Improve flow-volume loop.
40
PEFR
Inhales maximally Exhales as hard and fast and short as possible Repeat minimum of three times Use the best value for interpretation as
%predicted of control / personal best Highly effort dependent Diurnal variation (normal < 20%) Different value in each devices
41
Exercise challenge test
Perform spirometry Exercise 6-8 min (tread mill) till HR
160-180/min Repeat spirometry at 5, 10, 15,
20, 30 min EIB: FEV1 10-15%, or wheezing

42
Respiratory muscle testing
Measure maximum inspiratory P. (PImax, MIP) or negative inspiratory force (NIF)
Maximum inhale via pressure manometer Normal < -60 cmH2O Useful for evaluation neuromuscular dis:
myasthenia grevis, Guillian-Barre syndrome, diaphragmatic paralysis, pre-extubation
Other parameter: FVC, PEFR
43
Clinical Applications
44
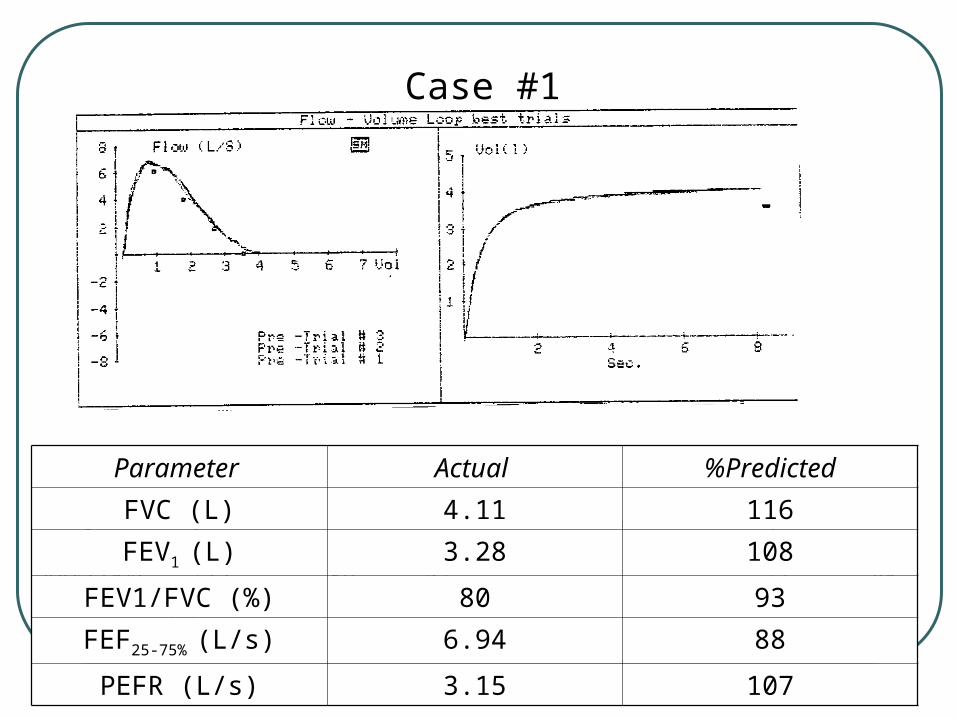
Case #1
Parameter Actual %Predicted
FVC (L) 4.11 116
FEV1 (L) 3.28 108
FEV1/FVC (%) 80 93
FEF25-75% (L/s) 6.94 88
PEFR (L/s) 3.15 107
Case #1
45
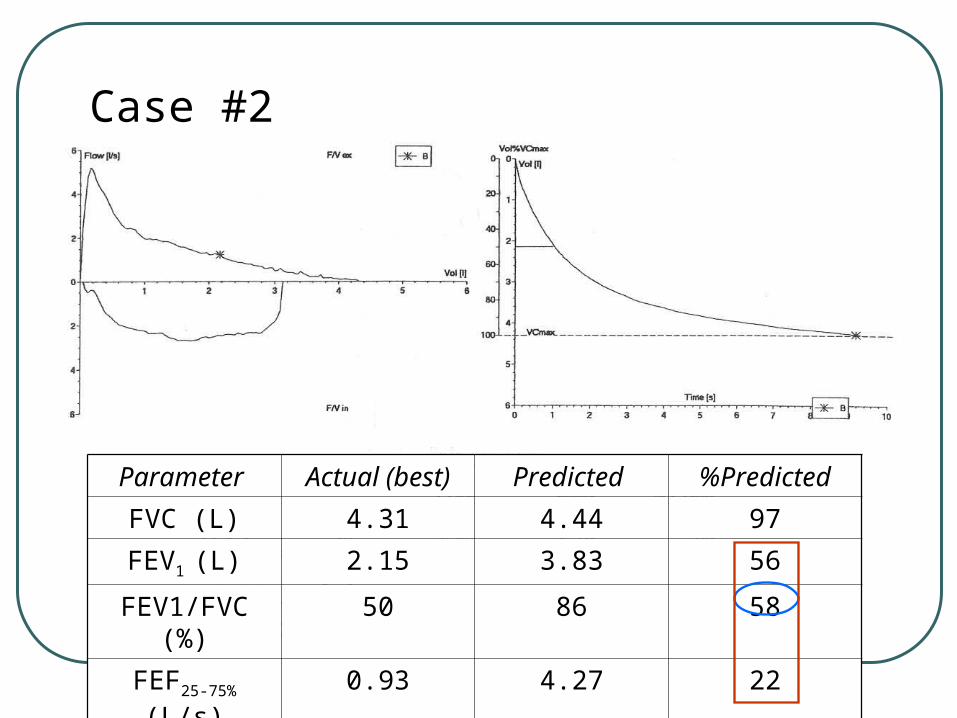
Case #2
Parameter Actual (best) Predicted %Predicted
FVC (L) 4.31 4.44 97
FEV1 (L) 2.15 3.83 56
FEV1/FVC (%)
50 86 58
FEF25-75% (L/s) 0.93 4.27 22
PEFR (L/s) 5.23 8.01 65
46
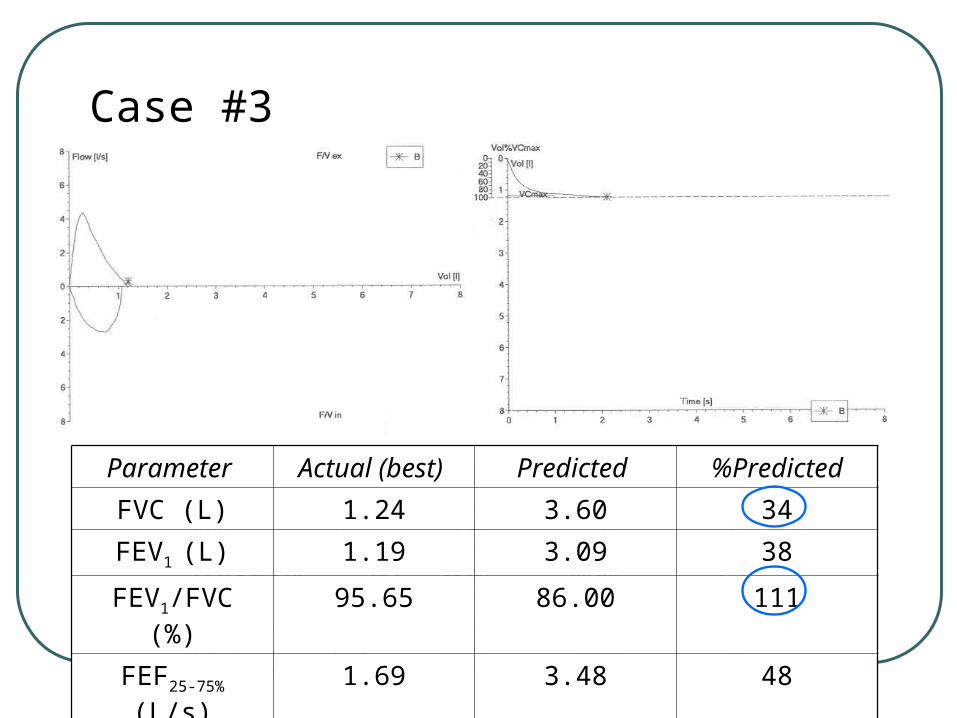
Case #3
Parameter Actual (best) Predicted %Predicted
FVC (L) 1.24 3.60 34
FEV1 (L) 1.19 3.09 38
FEV1/FVC (%) 95.65 86.00 111
FEF25-75% (L/s) 1.69 3.48 48
PEFR (L/s) 4.37 6.70 65
47
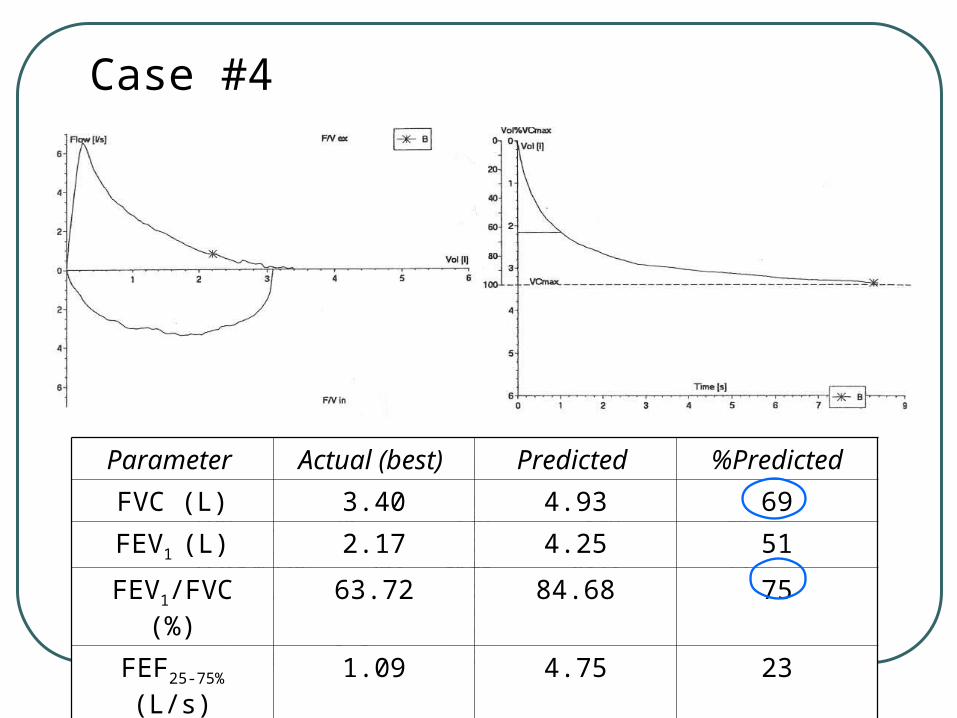
Case #4
Parameter Actual (best) Predicted %Predicted
FVC (L) 3.40 4.93 69
FEV1 (L) 2.17 4.25 51
FEV1/FVC (%) 63.72 84.68 75
FEF25-75% (L/s) 1.09 4.75 23
PEFR (L/s) 6.65 9.00 73
48
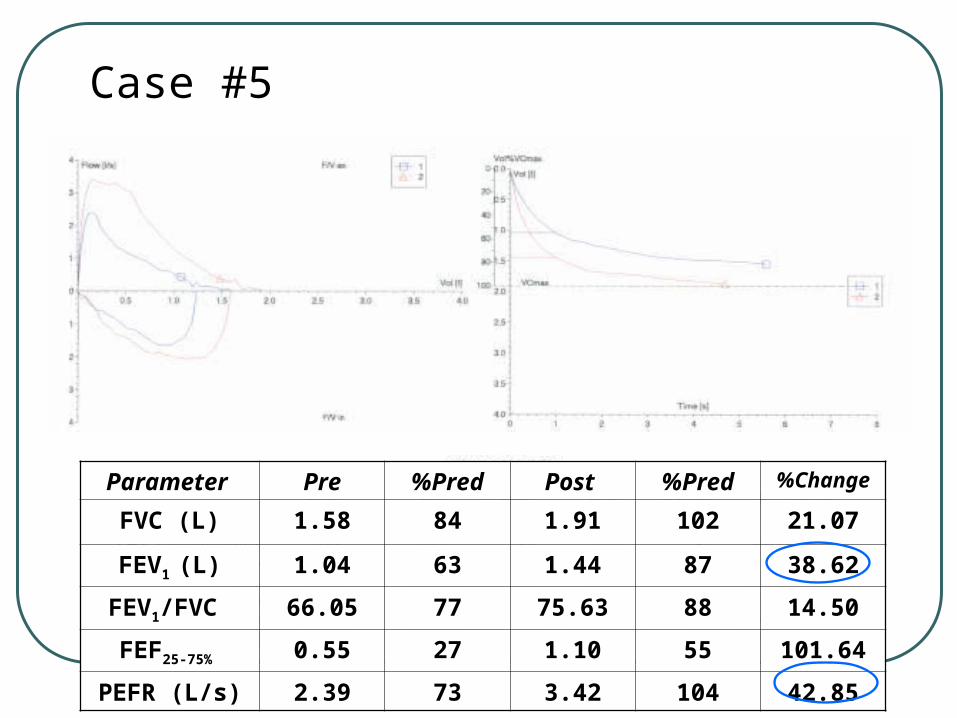
Case #5
Parameter Pre %Pred Post %Pred %Change
FVC (L) 1.58 84 1.91 102 21.07
FEV1 (L) 1.04 63 1.44 87 38.62
FEV1/FVC 66.05 77 75.63 88 14.50
FEF25-75% 0.55 27 1.10 55 101.64
PEFR (L/s) 2.39 73 3.42 104 42.85