
1. prostaglandins in labour dr rabi
39
PROSTAGLANDINS IN LABOUR DR. RABI NARAYAN SATAPATHY ASST.PROFESSOR DEPT. OF OBST.& GYNAECOLOGY SCB MEDICAL COLLEGE, CUTTACK MOB-09861281510 [email protected]
-
Upload
rabi-satpathy -
Category
Health & Medicine
-
view
355 -
download
5
Transcript of 1. prostaglandins in labour dr rabi

PROSTAGLANDINS IN LABOUR
DR. RABI NARAYAN SATAPATHY
ASST.PROFESSOR
DEPT. OF OBST.& GYNAECOLOGY
SCB MEDICAL COLLEGE, CUTTACK
MOB-09861281510

The role of all technological advances is to reduce human suffering.
In relation to obstetrics it can be achieved by:
• Reducing Maternal morbidity and mortality.
• Reducing perinatal mortality and morbidity
• Relievingpain of a parturient mother and thereby reducing her suffering

Historical developments in the development of Prostaglandins
1930 – KURZORK & LEIB DISCOVERED BIOLOGICAL ASPECTS OF PG’S
1935 – VON EULER COINED THE TERM PROSTAGLANDIN BELIEVING IT TO ORIGINATE FROM THE PROSTATE
1959 – ELAISON PROVED THAT PG ORIGINATED IN THE SEMINAL VESICLE
1964 – BERGSTRON ELUCIDATED THE STRUCTURE
1966 – DR. SULTAN KARIM REPORTED PRESENCE OF PG IN THE AMNIOTIC FLUID
- USED SEMEN TO AUGMENT LABOUR
1970 – DR. KARIM I.V. PGF2α FOR 1ST AND 2ND TRIMESTER ABORTIONS

Prostaglandins in Reproduction
Parturition
Birth
Ovulation
Fertilization & implantation
Pregnancy
Fetal placental hemodynamics
PPH
Lactation
Toxaemia
Ductus Aretriosus patency
Spontaneous abortion
Preterm labour
Sperm transport
PDA closure
Umbilical cord closure dysmenorrhoea
Leutolysis
menstruation
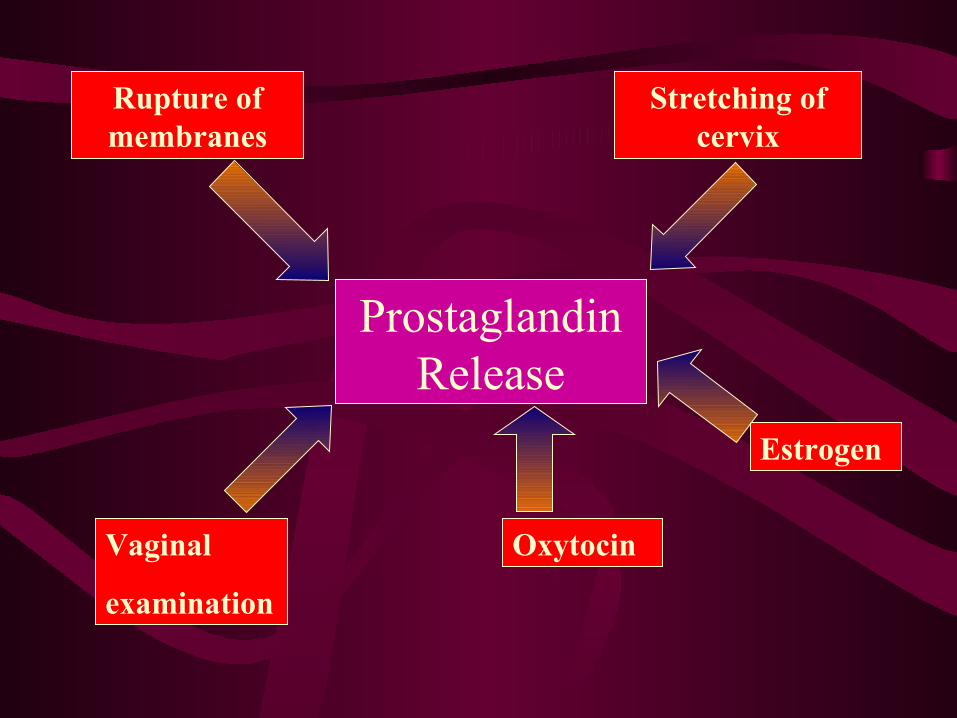
Prostaglandin Release
Rupture of membranes
Stretching of cervix
Vaginal
examination
Oxytocin
Estrogen

OXYTOCIN INDUCED
High amplitude
Higher frequency
Higher intensity
Quicker onset
Stops when infusion discontinued
PROSTAGLANDIN INDUCED
Low amplitude
Low frequency
Lower intensity
Continues even after discontinuing treatment
UTERINE CONTRACTIONS
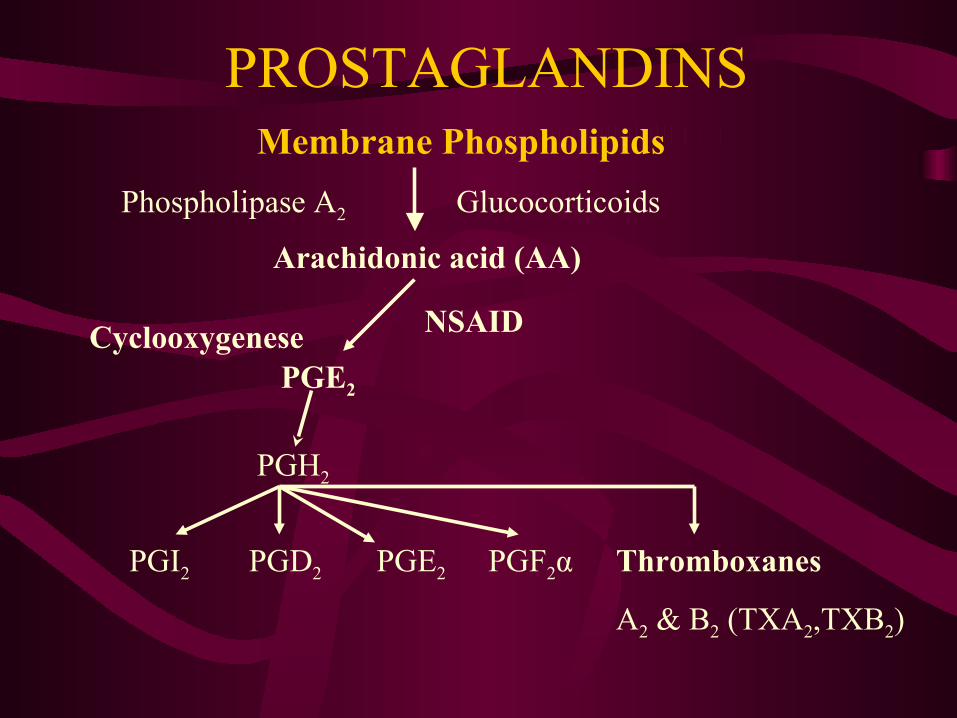
PROSTAGLANDINSMembrane Phospholipids
Arachidonic acid (AA)
NSAID
PGE2
PGH2
Cyclooxygenese
PGI2 PGD2 PGE2 PGF2α Thromboxanes
A2 & B2 (TXA2,TXB2)
GlucocorticoidsPhospholipase A2

PG synthesis

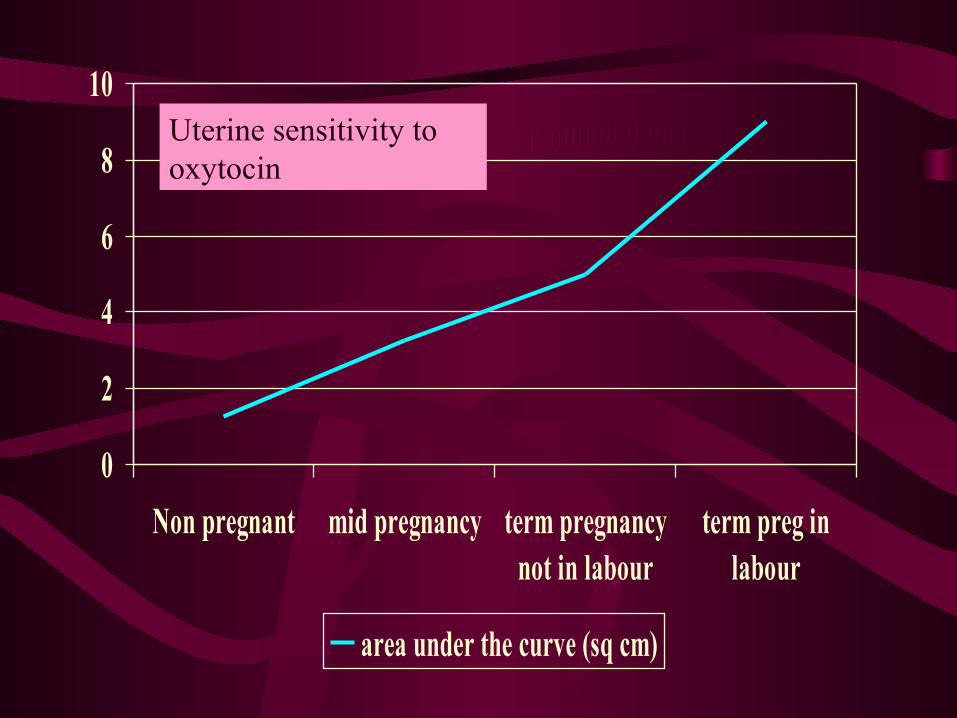
0
2
4
6
8
10
Non pregnant mid pregnancy term pregnancynot in labour
term preg inlabour
area under the curve (sq cm)
Uterine sensitivity to oxytocin

10
50
90
not inlabour
earlystage 1
latestage 1
II stage III stage
oxytocinpg/ml

0
12
24
2 cm 4 cm 6 cm 8 cm 10 cm
PGF2PGE2
Amniotic fluid PG during labour

Indicatons for the use of Cerviprime gel
• Post term
• Hypertension / Toxaemia
• Chronic hypertension
• Oligohydramnios
• Intrauterine growth restriction
• Diabetes
• Reduced fetal movements
• Suspected placental insufficiency

MUSCLE
MUCOSA
PROTEOGLYCAN
FIBROBLASTS


Instillation of PGE2 Gel

Cervical priming
COLLAGEN DEGRADATION
COLLAGEN IS RESISTANT TO MOST PROTEINASES
I COLLAGENASE
II LEUCOCYTE ELASTASE

Fibroblast activation
Vasacular permiability
Tissue hydration
Destabilization of Proteoglycans
Collagen dsegradation
PGE2Cervical ripening
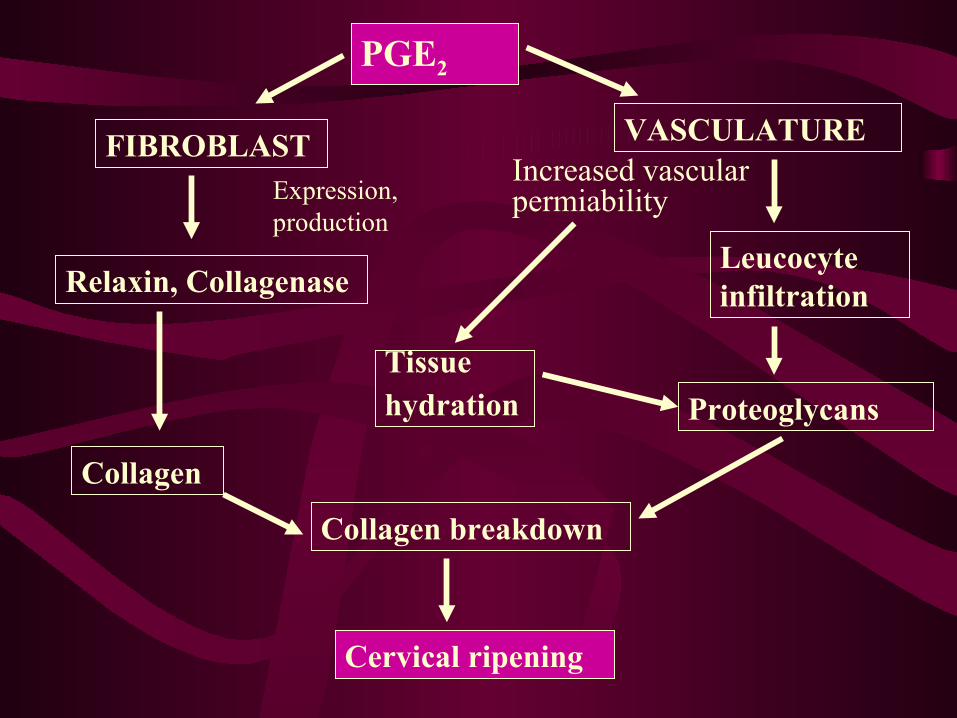
PGE2
FIBROBLAST VASCULATURE
Relaxin, CollagenaseLeucocyte infiltration
Tissue hydration
Collagen
Collagen breakdown
Cervical ripening
Proteoglycans
Expression, production
Increased vascular permiability

Progressive cervical dilatation

Cervical changes during labourNulliparous cervix near term
During labour - effacement
Fully dilated

Cerviprime to improve Bishop scoreAuthors year No. of
PtsBishop scoreBefore After
Bernstein 1987 42 3.2 7.7
ICMR study
1988 221 <3.0 >6.0
Bhide 1992 68 2.8 8.5
Patki & Daftary
1992 80 2.7 6.0

Cerviprime for labour outcomeAuthors Year No. of Pts Vaginal
delivery (%)
Legarht 1988 57 84.2
ICMR Study
1988 221 80.5
Bhide 1991 40 97.0
Patki & Daftary
1992 80 92.5

Prostaglandin induction of Labour (1993-94)
S No.
Author Place % Vag Del.
% C sec.
Avg Dur of lab(hrs)
Primi Multi
1 Patki Mumbai 92.5 7.5 7.3 7.3
2 Bhide Mumbai 90 10 16.4
3 Dubey Kanpur 92.2 7.1 14.6 8.2
4 Mehta Jaipur 100 - 8.0 6.0
5 R. Jina Gorakhpur 95 5 8.13 7.06
6 Sasikala Pondicherry 91.4 8.6 7.4 7.4
7 Daftary G. S. Mumbai 80 20 10.6 8.4
8 Handa P.R. Jamshedpur 85.7 14.3 12 10

Prostaglandin induction of Labour (1995-96)
S No.
Author Place % Vag Del.
% C sec.
Avg Dur of lab(hrs)
Primi Multi
1 S. Gupta Jaipur 79.7 21.3 12.6
2 S. Bhattacharya Calcutta 62.4 37.6 8.2 8.2
3 Sandhu Amritsar 85 15 10.35 6.08
4 S. Kore Mumbai 88 12 11.4 7.6
5 Mukherjee Allhabad 84 16 16.3 10.3
6 Vaneetkuma Jammu 81 19 12.0 -
7 A. Sone Simla 93 7 10 7.4

Contraindicatons for the use of Cerviprime gel
1. Patients hypersensitive to PG’S
2. Patients in whom Oxytocics are contraindicated• Previous LSCS
• Major CPD• Pre-existing fetal distress• Grande multipara
• Previous difficult or traumatic labour
1. Patients with ruptured membranes
2. Non-vertex presentation

Oxytocin PGE2
FUNDUS + +
ISTHMUS + -
+ STIMULATION - INHIBITION

Comparison of PG vs. Pitocin for Induction of labour
Distribution of casesOxytocin PGE2
Total cases 200 200
Indications
Post datism 25 60
P.R.O.M. 75 80
P.I.H. 40 30
Meconium stained liquor
50 15
I.U.G.R 10 15

Effect on Bishop score after single
Intracervical Gel or oxytocin drip after 4 hours
Oxytocin PGE2
Initial Bishop score 2.71± 0.96 2.65± 1.04
Follow up Bishop score 3.86± 1.45 5.02± 1.58
Mean change in Bishop score
1.15 2.37

Mean duration of stages of labour
Oxytocin PGE2
1ST STAGE 10.4 (2-14 HRS)
7.3 (1.5-12 HRS)
2ND STAGE 25.5 MIN 26.7 MIN
3RD STAGE 5 MIN 7 MIN

Comparison of PG vs. Pitocin Mode of delivery
Oxytocin PGE2Normal vaginal delivery
70 (35%) 125 (62.5%)
Instrumental vaginal delivery
90 (45%) 60 (30%)
L.S.C.S. 40 (20%) 15 (7.5%)

Prostaglandins – Induction of labour
SUMMARY:
• A survey of 15 Indian studies 1993 – 1996
• Parts of the country covered – 12 cities
• Average incidence of vaginal delivery 86.6%
• Average incidence of C. sections – 13.4%
• Average induction – Del. Interval – Primi 10.8 hrs
• Average induction – Del. Interval – multi 7.6 hrs

Pitocin induction of labourSummary:• Survey of six Indian studies• Average incidence of vaginal deliveries – 72.8%• Average incidence of C. section – 27.2%• Average induction – delivery time: 16.2 hrs in
primi• Average induction – delivery time: 9.6 hrs in
Multi• Incidence of low APGAR scores 1.5 – 2 times
higher

Comparison of PG vs. Pitocin for InductionS no
Authors drug % success
LSCS % incidence
Ind-Del interval hrs
Perinatal outcome low apgar
1 Gupta et al, Jaipur, 1995
PGO
73.355.5
13.344.4
16.427.9
4.4%13.3%
2 Muhkerjee, Allhabad,1996
PGO
72.750
16.340
16.322.5
--
3 Sandhu et al,Amritsar,1995
PGO
1015
9.510.4
--
4 Patki et al, Mumbai,1993
PGO
7520
7.810.9
5%7.5%
5 Dubey, kanpur, 1994
PGO
7.112.5
14.616.2
NIL4.7%
6 k. Gupta,Agra, 1994
PGO
12%20%
5.66.3
8.3%8.3%

Time lag due to oral administration leads to longer
induction – delivery interval as compared to I.V. Oxytocin
(Lange 1986)

Oral PGE2 – less GI symptoms & more effective than PGF2α and
has become the standard for induction and acceleration of
labour

PG’S are effective even in unripe
cervices due to the direct
softening effect on the cervix as
compared to Oxytocin

Prostaglandins in the induction of labour have been shown to be
devoid of deleterious effects on the physical and psychomotor development of the Neonate

Prostaglandin formulations in Obstetric practice
PROSTAGLANDINS
CERVICAL RIPENING
Cerviprime gel
FETAL DEATH
Prostodin injection
Cerviprime Gel +
Oxytocic
LABOUR
INDUCTION
Primiprost tablet
LABOUR
AUGMENTATION
Primiprost Tablets
THIRD STAGE COMPLICATIONS
Prostodin injections


















