1 PAT 2009 with clinical signs and blood alcohol concentrations. ‘Make the Connection’ Prof....
22
1 PAT 2009 with clinical signs and blood alcohol concentrations. ‘Make the Connection’ Prof. Robin Touquet & Adrian Brown RMN St Mary’s Hospital, Imperial College HCT, Paddington, London, England.
-
Upload
kai-gravley -
Category
Documents
-
view
213 -
download
0
Transcript of 1 PAT 2009 with clinical signs and blood alcohol concentrations. ‘Make the Connection’ Prof....

1
PAT 2009with clinical signs and blood alcohol concentrations.
‘Make the Connection’
Prof. Robin Touquet & Adrian Brown RMNSt Mary’s Hospital, Imperial College HCT,
Paddington, London, England.

2
Early Identification of Alcohol Misuse
History – Paddington Alcohol Test (PAT)
Examination – “SAFE Moves, ABCD”
Special Investigation – Blood Alcohol Concentration (BAC)
Leads to - Brief Advice (B.A.)(by all staff) + offer of referral
- Brief Intervention (B.I.) (by Alcohol Nurse Specialist)
3
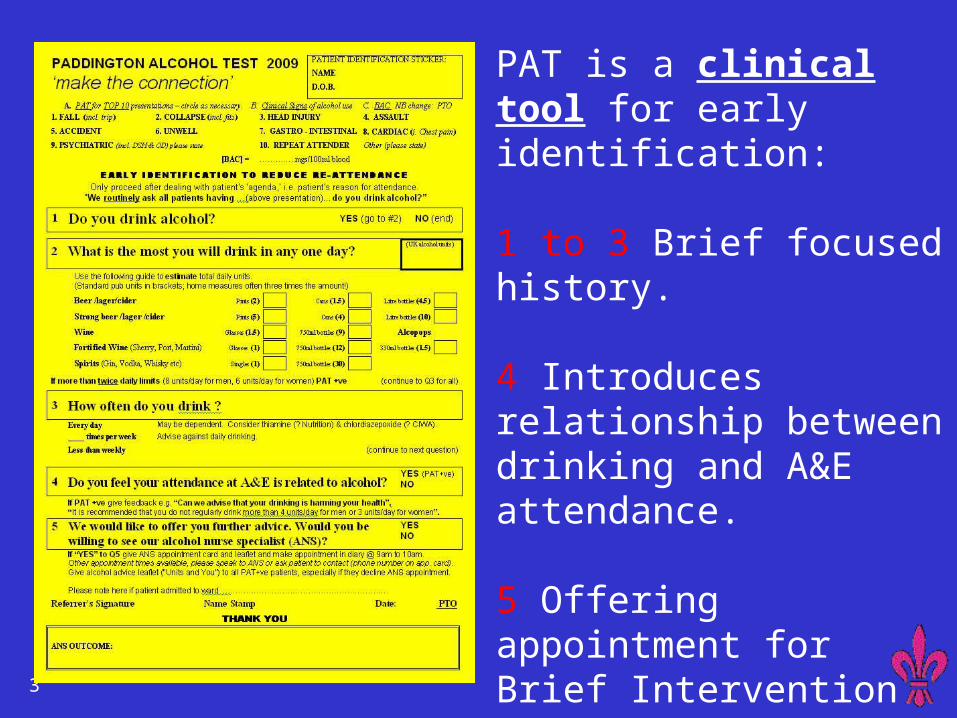
PAT is a clinical tool for early identification:
1 to 3 Brief focused history.
4 Introduces relationship between drinking and A&E attendance.
5 Offering appointment for Brief Intervention (B.I.)

4
Back of PAT 2009
SAFE Moves
5
All new A&E SHOs
1 hour Education Alcohol Misuse DAY 2! Early detection in natural history of misuse - noting clinical signs of alcohol
- use of PAT & Alcohol Health Work
- ? BAC if not ‘PAT-able’
Every SHO gives RT 5 PATs 1st 2/52 - once you ‘give me 5’, symphony will suffice
for patients who do not accept referral
Each month feedback presented as a league table of referrals

6
1 year Resuscitation Room positive BACs - Prevalence by Y90 coding
0
20
40
60
80
100
120
No. ofpatients
Collapse
GI Bleed
NCCP
DSH
Trauma
Other
20-39 40-59 60-79 80-99 100-119 120-199 200-239 240+ mg/100ml Y90.1 Y90.2 Y90.3 Y90.4 Y90.5 Y90.6 Y90.7 Y90.8 Note. DSH denotes deliberate self harm, and NCCP denotes Non Cardiac Chest Pain
From “Resuscitation Room blood alcohol concentrations: one year cohort study” Touquet et al, Emergency Medicine Journal 2008: 25: 752-6
110/291 (38%)> 240 mg/100ml

7
Symbiosis to counter ‘clinical Symbiosis to counter ‘clinical inertia’inertia’
Alcohol Nurse Specialist – ‘stress reducer’ for staff:
seeing patients perceived as ‘difficult’ - B.I. (20 mins +)
Consultant Alcohol Support
ensuring referrals, supporting education/audit/feed-back for giving simple B.A. (1/2 -2 min)

8
Role of the Alcohol Nurse Specialist
Brief intervention following referral – both by appointment and in real time if on observation/admission ward; liaison with local services.
Education,e.g. for brief advice (by all staff) with resulting
referral rate increase, withdrawal, detox. regimes, etc.
Audit – improving practice.
Feedback – patient outcomes. CHANGING ATTITUDES.
ANS attends every weekday 8am including CDU & DAAU

9
30 months in A&E(initial research done in resusc only)
174,764 adult attendances at A&E 52% 84,024 had PAT possible condition
1% (1,714) “apparently drunk”
2.0%(1,812*) diagnosed “alcohol problem” 2.6%(2,191) referred to ANS 5,384 had BAC carried out on
2,315 BAC < 10 mg/100ml) ie NEGATIVE
2,554 BAC > 120 mg/100ml 31% (804) referred to ANS

10
Reminder:PAT possible conditions
as recorded on A&E database
Apparently Drunk Falls Collapsed adult Fits Head Injury Assault Abdominal Pain Chest pain
Mental Illness Deliberate self harm Overdose & Poisoning Behaving strangely
Unwell Adult Limb problems Wounds

11
Outcome of ANS referrals(PAT possible conditions)
31% of referrals to ANS have positive BAC (679 out of 2179)
12% have BAC <10 (259 out of 2179)

12
Outcome of ANS referrals(where BAC done)
NB among BACs <10, 54 previous contact, 168 referred to ANS
13
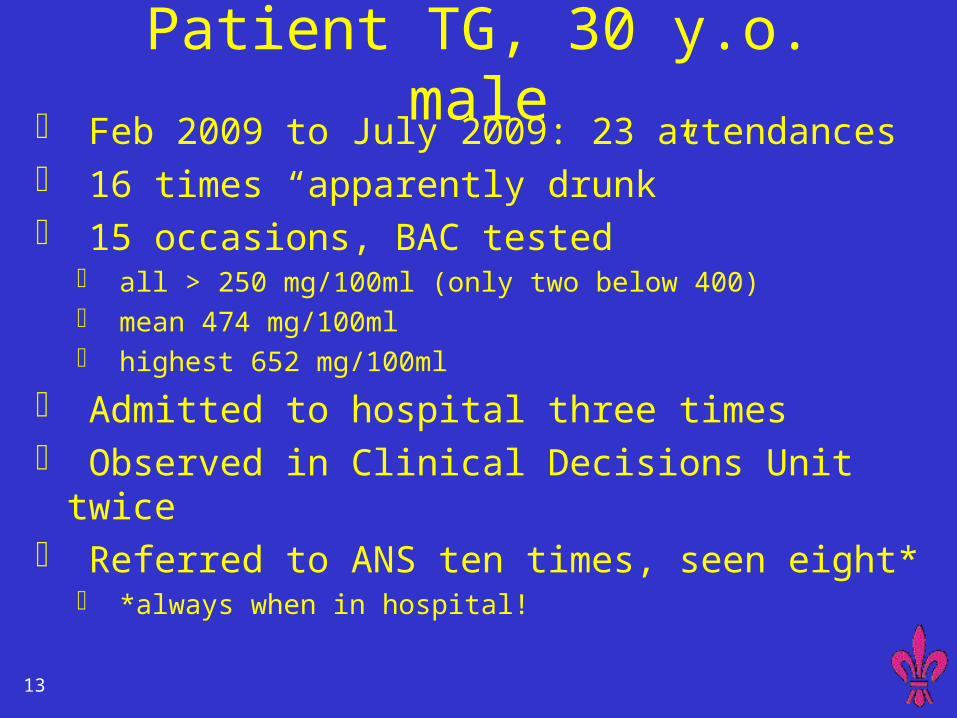
Patient TG, 30 y.o. male Feb 2009 to July 2009: 23 attendances 16 times “apparently drunk” 15 occasions, BAC tested
all > 250 mg/100ml (only two below 400) mean 474 mg/100ml highest 652 mg/100ml
Admitted to hospital three times Observed in Clinical Decisions Unit twice Referred to ANS ten times, seen eight*
*always when in hospital!
14
Patient EF, 51 y.o. male Never previously attended A&E Head injury after bicycle accident Initially reluctant to admit he’d been drinking BAC tested
Did not want to stay in hospital, discharging doctor advised him of BAC score and he then accepted referral to ANS.
Attended ANS appointment 2 days later Admitted his drinking had been a problem, and
agreed to referral to community services.

15
BAC level vs PAT test Where PAT completed, self report <15 units per day but BAC score suggests more !
Maximum units per day, reported on PAT
mg/ 100ml

16
PAY OFFFor every two patients referred to
the Alcohol Nurse Specialist
There will be one less reattendance within the next 12 months.
Screening and referral for B.I.
Lancet 2004;364:1334-9

17

18
When to order a BAC? - always with a sugar (grey bottle)
1. If in Resuscitation Room.- Collapse
- Trauma - Self-harm & overdose - G.I. & Abdominal - Chest pain 2. If giving IV B vitamins (pabrinex) for chronic alcohol misuse
with poor diet - ? Signs of Wernicke’s
3. If clinical signs of withdrawal - patient in majors (on trolley needing bloods being taken)
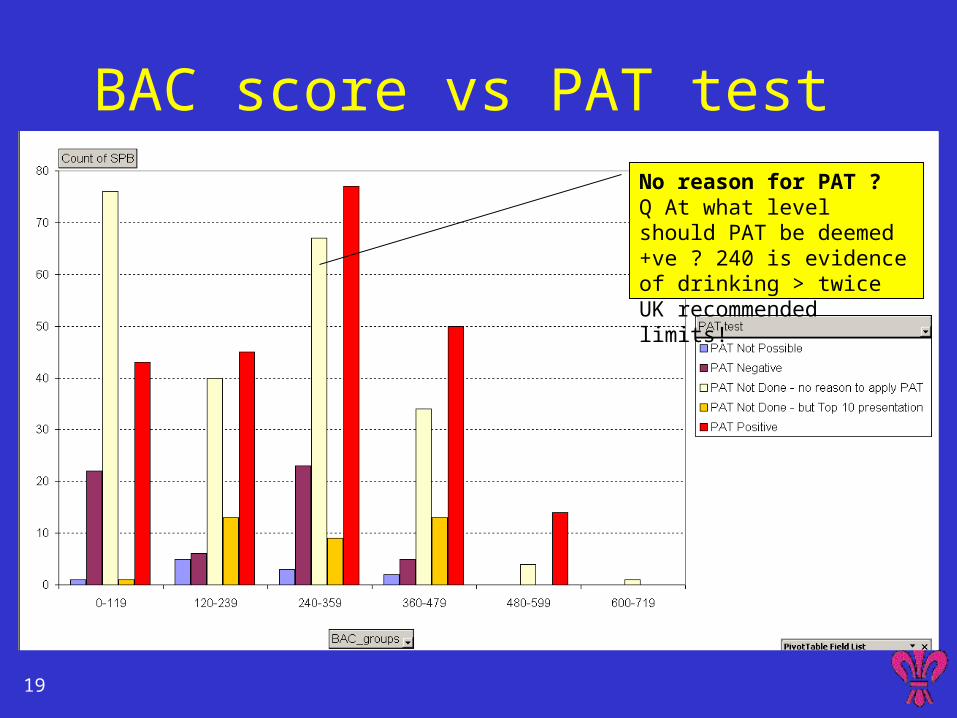
19
BAC score vs PAT test No reason for PAT ?Q At what level should PAT be deemed +ve ? 240 is evidence of drinking > twice UK recommended limits!

20
BAC score vs Referral to ANS Unfortunately the majority in the “hazardous” range are not referred, but there is evidence that these patients leave (intoxicated) before result is known.
Increasing likelihood that referral will be made.

21
BAC score vs Age group Younger adults (20-40) tend toward higher consumption,

22
BAC score vs gender