1 - Olds - Approach to a Patient With Sensory Loss
76
CharismaT. Evangelista, MD, FPNA San Beda College of Medicine July 8, 2013
-
Upload
rose-ann-mecija -
Category
Documents
-
view
252 -
download
5
description
n
Transcript of 1 - Olds - Approach to a Patient With Sensory Loss

Charisma T. Evangelista, MD, FPNA San Beda College of Medicine July 8, 2013

¡ To review the somatosensory pathways
¡ To recall the technique of neurologic examination of the somatosensory system
¡ To be able to give a localization based on the pattern of sensory loss

I. Anatomic Considerations The Sensory Pathways – General Schema
II. The Sensory Syndromes A. Peripheral – peripheral nerve, roots, dorsal root ganglia B. Spinal Sensory Syndromes C. Brainstem D. Thalamus E. Parietal Lesions III. Approach to the Patient with Sensory Loss A. History-‐taking B. Techniques of Examination C. Final Reminders

IV. Etiologic Diagnoses V. Ancillary Diagnostics


¡ Pain ¡ Light touch ¡ Temperature – Warmth and cold ¡ Vibration sense ¡ Position sense ¡ Deep pressure


¡ Receptor → ¡ Peripheral Nerve → ¡ Spinal Root → ¡ Sensory Tract (Ascending tracts) → ¡ Thalamus → ¡ Sensory Cortex

Encapsulated receptors

Non-‐encapsulated receptors
¡ Merkel’s disk -‐ pressure
¡ Free nerve endings -‐ pain







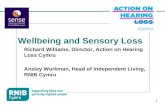
Insert pic of dermatomes
Dermatomes – represent the surface innervation of the sensory nerve roots.



¡ C3 – front of neck ¡ C6 – thumb ¡ C7 – middle finger ¡ C8 – little finger ¡ T4 – nipples ¡ T6 – xiphoid process ¡ T10 – umbilicus ¡ L1-‐ bikini line ¡ L4 – knee, big toe ¡ L5 – Shin ¡ S1 – little toe ¡ S2-‐ s3 -‐ genitalia
Back: ¡ C2 – back of the head ¡ C5 – tip of shoulder ¡ S2-‐S5 – buttocks





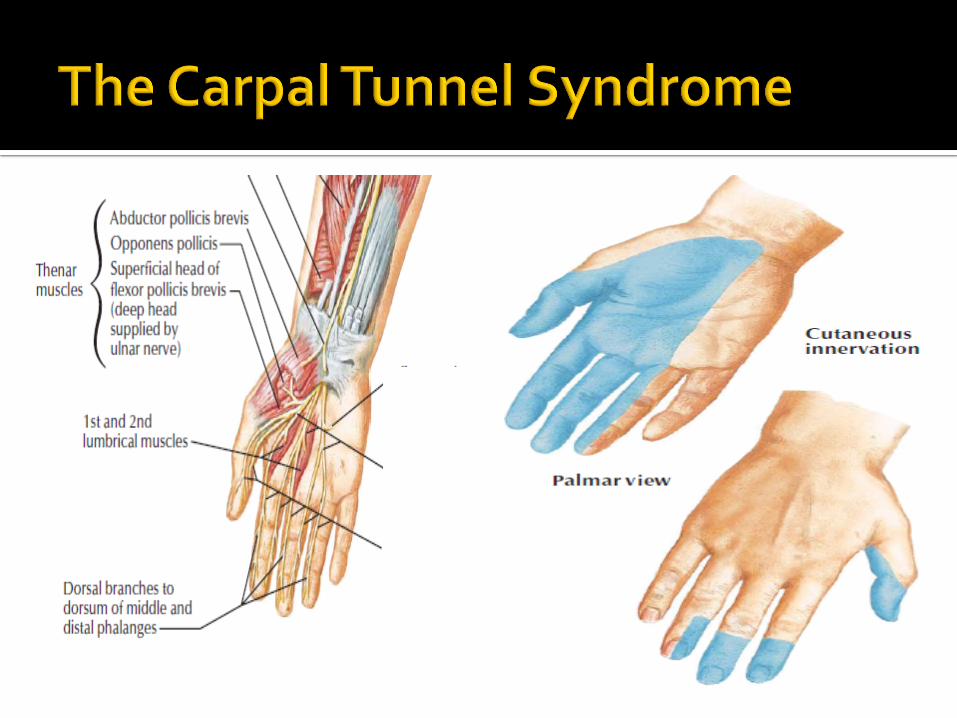
¡ Will vary depending on whether the nerve involved is predominantly muscular, cutaneous or mixed
¡ If a cutaneous nerve is involved, the area of sensory loss is always less than its anatomic distribution because of overlap from adjacent nerves.
¡ Deep pain and perception may be intact.

¡ Usually the sensory impairment is bilaterally symmetrical.
¡ In most types of polyneuropathy, the longest and largest fibers are the most affected, giving rise to a glove-‐and-‐stocking distribution of sensory loss.


¡ Usually all modalities of sensation are involved, but to varying degrees, with one modality impaired out of proportion to the others.
¡ May be accompanied by varying degrees of motor and reflex loss.

¡ Follows dermatomal distribution. ¡ If pain is present, it may be intensified by movement of the spine and radiate in proximal-‐distal fashion.

¡ Shooting or lancinating pains and burning sensations arise from diseases of the nerve roots, e.g. Sciatica, pain from the shoulder to the upper arm from cervical disc protrusion.
¡ Tendon and cutaneomuscular reflexes may be lost.
¡ Widespread disease may produce the same sensory defects as diseases of the posterior nerve roots.
¡ Proximal areas of the body also show pronounced sensory loss: face, oral mucosa, scalp, trunk, genitalia
¡ Tendon reflexes are also lost.
¡ +/-‐ dysautonomia ¡ Main causes: paraneoplastic, connective tissue diseases (Sjögren syndrome), toxic exposure, idiopathic inflammation.

1. Complete spinal sensory syndrome 2. Hemisection of the spinal cord (Brown-‐
Séquard Syndrome) 3. Syringomyelic Syndrome (Lesion of the
Central Gray MaHer) – or Central Cord Syndrome
4. Posterior (Dorsal) Column Syndrome 5. Anterior Myelopathy
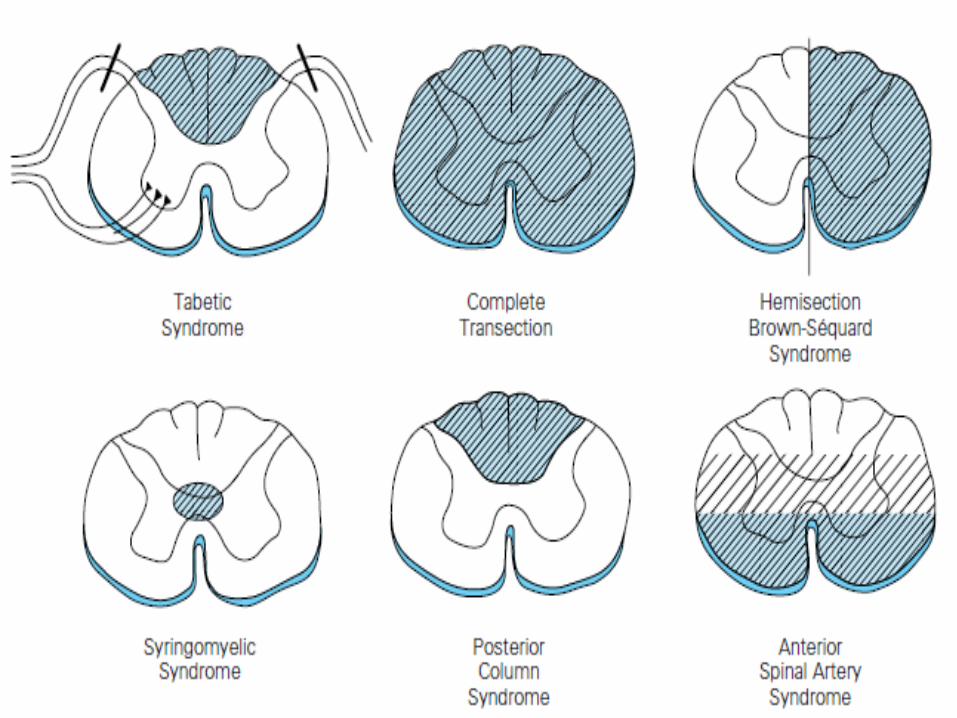

¡ Loss of ALL forms of sensation below a level that corresponds to that lesion.
¡ The subacute evolution of a transverse
spinal cord lesion may show a discrepancy between the level of the lesion and that of the sensory loss.

¡ Affectation of the pain and thermal sensation on the side contralateral to the lesion
¡ Ipsilateral proprioceptive affectation
¡ Associated spastic motor paralysis on the ipsilateral side

CTLS




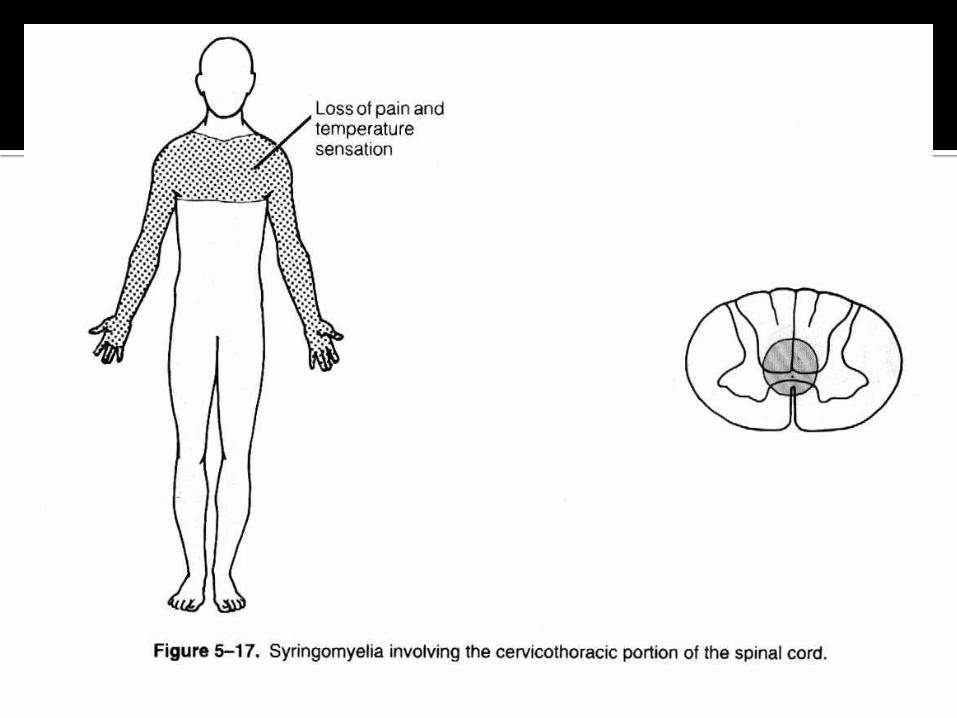
¡ Abolition of pain and temperature on one or both sides over several segments (in dermatomal distribution) but with sparing of tactile sensation (dissociated sensory loss)
¡ There may be varying degrees of segmental amyotrophy and reflex loss.
¡ If the lesion has spread to the white matter, corticospinal, spinothalamic, and posterior column signs will be conjoined.
¡ Most common etiologies: developmental syringomyelia (especially in the cervical region), intramedullary tumors (ependymomas), trauma, hemorrhage


¡ Paresthesias may be common complaints. ¡ Vibration and position senses are more affected.
¡ Usual causes: multiple sclerosis, vitamin B12
Deficiency, tabes dorsalis, HIV and HTLV-‐1 infection.

¡ Loss of pain and temperature sensation below the level of the lesion but with relative or absolute sparing of proprioceptive sensation.
¡ Spastic paralysis is a prominent feature (since the corticospinal tracts and the ventral gray matter also lie within the distribution of the anterior spinal artery)
¡ Causes: Infarction of the spinal cord in the territory of the ASA

¡ Medullary lesions – may cause crossed sensory disturbance
¡ Upper medulla, pons, midbrain – the crossed trigeminothalamic and lateral spinothalamic tracts run together; lesions at this level may cause loss of pain and temp on the opposite half of the face and the body
¡ Cranial nerve palsies, cerebellar ataxia, and motor paralysis are almost invariably associated.


¡ Loss or diminu+on of all forms of sensa+on on the opposite side of the body
¡ Spontaneous pain or discomfort may appear on the affected side of the body (thalamic pain)
¡ There may be hypalgesia with hyperpathia (due to an elevated pain threshold)
¡ Causes: Vascular (strokes), less oTen tumors

¡ Disturbance of discriminative sensory functions without impairment of the primary modalities of sensation (unless the lesion is extensive and deep)
¡ Sensory inattention, extinction and neglect

¡ Examination may sometimes include overtly hysterical findings like ipsilateral reduced hearing, sight, smell and taste
¡ Impaired vibration over half the skull and sternum
¡ Anesthesia not conforming to the distribution of a root or cutaneous nerve

“Namamanhid ang _____ ko.”
¡ Ask the patient about their symptoms – this may pose a problem as the symptoms may be unlike anything the patient has experienced before
¡ Ask how the sensory disturbance was first noted

Generally Accepted Definitions of Commonly Used Terms Regarding the Sensory System and Abnormalities of Sensation Allodynia* Increase in sensibility to pain, pain in response to a stimulus not normally
painful
Alloesthesia Perception of a stimulus at a site other than where it was delivered.
Analgesia Absence of sensibility of pain
Astereognosis Absence of spatial tactile sensibility; inability to identify objects by feel
Anesthesia Absence of all sensation
Dysesthesias Unpleasant or painful sensations, either spontaneous or after a normally nonpainful stimulus
Hypalgesia Decrease in sensibility to pain
Hyperalgesia* Increase in sensibility to pain, pain in response to a stimulus not normally painful
Hyperpathia* Increase in sensibility to pain, pain in response to a stimulus not normally painful
Pallesthesia Vibration sense
Paresthesias Abnormal spontaneous sensations experienced in the absence of stimulation

If the complaint is arm numbness... ¡ Symptoms constant or intermittent? ¡ Relationship to activities ¡ Any involvement of the arm, face, leg ¡ Any problems with speech or vision ¡ Neck pain? ¡ Hand/arm weakness ¡ Any history of injury ¡ Any involvment of the opposite hand
If the complaint is numbness of the feet... ¡ Whether symptoms are constant or intermittent
¡ If intermittent, any relation to posture, activity or movement
¡ Any associated pain in the back, legs, or feet ¡ Any weakness of the legs or feet ¡ Any history of back injury, disc herniation, or back surgery

¡ Symmetry of symptoms ¡ Any bowel, bladder, or sexual dysfunction ¡ Any history of underlying systemic disease ¡ Any weight loss ¡ Drinking habits ¡ Smoking history ¡ Any history to suggest toxin exposure, vocational, or
recreational ¡ Dietary history ¡ Medication history, including vitamins ¡ Family history of similar symptoms ¡ Family history of diabetes, pernicious anemia or
peripheral neuropathy

A. Tools
1. Pin
2. Wisp of cotton
3. Tuning fork (128 or 256 Hz)

1. Testing touch sensation
¡ For screening purposes test only the dorsum of the hands and feet (DeMyer)
¡ Test each area as required by the history (DeMyer)
2. Testing temperature sensation
¡ Use the tuning fork versus finger or hot and cold tubes (DeMyer)
¡ Remember you are testing temperature discrimination, not how much heat/cold the patient can tolerate! (DeMyer)

3. Testing pain sensation
¡ Use of a pin, with both blunt and sharp ends (DeMyer).
¡ Alternate blunt and sharp ends. ¡ Make 3 successive pricks. ¡ Ask the patient to respond “dull” or “sharp.” ¡ Have the patient close his eyes. ¡ Start with a normal area. ¡ Avoid the thick skin of the palms and the soles.

4. Testing proprioception
¡ Support the part to be tested. ¡ Wiggle the digit up and down, stopping in one
direction randomly. ¡ Make the patient watch first, before asking
him/her to close his eyes. ¡ Patient should not move the other digits. ¡ You may give three alternatives (up, down, or
neutral, to reduce the chances of guessing)

5. Testing for loss of vibration sense (pallanesthesia)
¡ Start with the patient’s eyes open. ¡ Strike the tuning fork and apply to the
patient’s finger-‐ and/or toenails. ¡ If the patient cannot feel the vibration at the
nails for as long as you can, apply the fork to proximal bony prominences.

50%
100 % sensory deficit to pain, t empe r a t u r e and light touch f r o m T 1 0 downwards

C. Final reminders ¡ The sensory examination is difficult and tedious.
¡ The patient should be alert and attentive, full cooperation is necessary.
¡ Objective evidences: withdrawal of the part stimulated, wincing, blinking, and changes in countenance; pupillary dilation, tachycardia and perspiration may accompany painful stimulation.

¡ Obtain patient confidence ¡ Areas under examination should be uncovered but it is best to expose various parts of the body as little as possible.
¡ Compare homologous areas. ¡ Examination depends on the history. ¡ Positive and negative symptoms may occur together!
¡ In patients with limited cooperation, the abnormal area may be surveyed first.

¡ There are 2 screening patterns: side to side (usually compares the major dermatomes and peripheral nerve distributions), and distal to proximal (when peripheral neuropathy is a differential).
¡ Sensory changes due to suggestion are notoriously frequent in emotionally labile individuals, but suggestion can produce non0rganic findings in patients with organic disease.

¡ Uncooperative vs. overly cooperative ¡ Some areas of the body are more sensitive than the others: antecubital fossae, supraclavicular fossae, neck
¡ Obstacles: low intellectual endowment, language difficulties, or a clouded sensorium
¡ With altered mental status: pain may be tested grossly by pricking or pinching the skin
¡ In a child: it may be best to delay sensory testing until the end of the examination


¡ V – Vascular – occlusion, hemorrhage, vasculitis ¡ I – Infectious – tabes dorsalis, HIV, abscesses,
granulomas ¡ T – Traumatic, Toxic – gross trauma, radiation, drugs,
vertebral fractures, skull fractures ¡ A – Autoimmune – SLE ¡ M – Metabolic – DM, Uremia ¡ I – Inflammatory – Guillain-‐Barre Syndrome ¡ N – Neoplastic, Nutritional – Leukemias, Vitamin B12
deficiency, Spinal cord tumors ¡ D – Degenerative, Developmental (including
Congenital), Demyelinating – Multiple sclerosis, HSMN, Disc herniations

¡ Electrophysiologic testing – EMG-‐NCV, Somatosensory evoked potentials
¡ Imaging tests – MRI, CT scan
¡ Blood chemistry
¡ Fecalysis
¡ Vitamin B12 assays

Thank you.