
1 National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) -3 Susan...
83
1 National Institutes of Health (NIH) National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) -3 Expert Panel Report (EPR) -3 Susan K. Ross RN, AE-C Susan K. Ross RN, AE-C MDH Asthma Program MDH Asthma Program 651-201-5629 651-201-5629 [email protected] [email protected]
-
Upload
daniel-rees -
Category
Documents
-
view
221 -
download
1
Transcript of 1 National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) -3 Susan...

11
National Institutes of Health (NIH)National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline NAEPP 2007 Asthma Guideline
Expert Panel Report (EPR) -3Expert Panel Report (EPR) -3
Susan K. Ross RN, AE-CSusan K. Ross RN, AE-C MDH Asthma Program MDH Asthma Program
651-201-5629 651-201-5629 [email protected]@state.mn.us

22
National Institutes of HealthNational Institutes of HealthNational Asthma Education Prevention ProgramNational Asthma Education Prevention Program (NAEPP)(NAEPP)
http://www.nhlbi.nih.gov/guidelines/asthma/index.htmhttp://www.nhlbi.nih.gov/guidelines/asthma/index.htm
20072007Guidelines for the Diagnosis and Guidelines for the Diagnosis and Management of Asthma (EPR-3)Management of Asthma (EPR-3)
National Asthma Education
and Prevention Program

33
What is Asthma?What is Asthma?
““Asthma is a common chronic disorder of the Asthma is a common chronic disorder of the airways that involves a complex interaction airways that involves a complex interaction of airflow obstruction, bronchial of airflow obstruction, bronchial hyperresponsiveness and an underlying hyperresponsiveness and an underlying inflammation. This interaction can be highly inflammation. This interaction can be highly variable among patients and within patients variable among patients and within patients over time”.over time”.
EPR 3- Section 2, p 12.EPR 3- Section 2, p 12.

44
Characteristics of AsthmaCharacteristics of Asthma
• Airway Inflammation Airway Inflammation • Airway Obstruction (reversible) Airway Obstruction (reversible) • Hyperresponsiveness (irritability of airways)Hyperresponsiveness (irritability of airways)

55
Normal & Asthmatic BronchioleNormal & Asthmatic Bronchiole
66
Why Do We Need Asthma Guidelines?Why Do We Need Asthma Guidelines?

77
Asthma:Asthma:
– In 2008, it was estimated that 23.3 million Americans currently In 2008, it was estimated that 23.3 million Americans currently have asthma have asthma
– Is one of the most common chronic disorders in childhood, Is one of the most common chronic disorders in childhood, affecting an approx. 7.1 million children under 18 years (9.6%) affecting an approx. 7.1 million children under 18 years (9.6%) 11
– In 2007, 3,447 deaths were attributed to asthma, 152 deaths In 2007, 3,447 deaths were attributed to asthma, 152 deaths were children under the age of 15 were children under the age of 15 22
– Is the Is the thirdthird leading cause of hospitalization among children leading cause of hospitalization among children under the age of 15 under the age of 15 66
– Is one of the leading causes of school absenteeism Is one of the leading causes of school absenteeism 33 In 2008 In 2008 asthma accounted for approx. 14.4 million lost school daysasthma accounted for approx. 14.4 million lost school days44
– The annual health care costs of asthma is approx. $20.7 billion The annual health care costs of asthma is approx. $20.7 billion dollars dollars 55
From ALA website 11/2010 www.Lungusa.org 1 CDC: National Center for Health Statistics, National Health Interview Survey Raw Data, 20092 CDC. National Center for Health Statistics. Final Vital Statistics Report. Deaths: Final Data for 2007. April 17, 2009. Vol 58 No 19.3 CDC. National Center for Chronic Disease Prevention and Health Promotion. Healthy Youth! Health Topics: Asthma. August 14, 20094 CDC: National Center for Health Statistics, National Health Interview Survey Raw Data, 2008.5 NHLBI Chartbook, U.S. Department of Health and Human Services, National Institute of Health, 20096 CDC: National Center for Health Statistics, National Hospital Discharge Survey, 2006.

88
2007 - Guidelines for the Diagnosis 2007 - Guidelines for the Diagnosis && Management of AsthmaManagement of Asthma
Expert Review Panel (EPR-3)Expert Review Panel (EPR-3)

99
Asthma Guidelines:Asthma Guidelines: History History && Context Context
Initial guidelines released in 1991 and updated in 1997Initial guidelines released in 1991 and updated in 1997 Updated again in 2002 (EPR-2) with a focus on several Updated again in 2002 (EPR-2) with a focus on several
key questions about medications, monitoring and key questions about medications, monitoring and preventionprevention– Long-term management of asthma in childrenLong-term management of asthma in children– Combination therapyCombination therapy– Antibiotic useAntibiotic use– Written asthma action plans (AAP) and peak flow meters Written asthma action plans (AAP) and peak flow meters
(PFM)(PFM)– Effects of early treatment on the progression of asthmaEffects of early treatment on the progression of asthma

1010
Old Old && New Asthma Guidelines: New Asthma Guidelines:What has What has notnot changed changed
Initial asthma therapy is determined by assessment of asthma Initial asthma therapy is determined by assessment of asthma severityseverity– Ideally, before the patient is on a long-term controllerIdeally, before the patient is on a long-term controller
Stepping therapy up or down is based on how well asthma is Stepping therapy up or down is based on how well asthma is controlled or not controlledcontrolled or not controlled
Inhaled corticosteroids (ICS) are the preferred first-line therapy for Inhaled corticosteroids (ICS) are the preferred first-line therapy for asthmaasthma
Systemic steroids can still be used to treat asthma exacerbationsSystemic steroids can still be used to treat asthma exacerbations Peak flows and written asthma action plans are recommended for Peak flows and written asthma action plans are recommended for
asthma self managementasthma self management – Especially in moderate and severe persistent asthma, or for those Especially in moderate and severe persistent asthma, or for those
with a history of severe exacerbations or poorly controlled asthmawith a history of severe exacerbations or poorly controlled asthma

1111
Asthma Therapy GoalsAsthma Therapy Goals
““The goal of asthma therapy is to control asthma The goal of asthma therapy is to control asthma so patients can live active, full lives while so patients can live active, full lives while minimizing their risk of asthma exacerbations minimizing their risk of asthma exacerbations and other problems”and other problems”
Dr. William Busse, MD., chairman of the NAEPP EPR -3Dr. William Busse, MD., chairman of the NAEPP EPR -3

1212
2007 - Guidelines for the Diagnosis & 2007 - Guidelines for the Diagnosis & Management of Asthma (EPR-3)Management of Asthma (EPR-3)
– (Almost) no new medications(Almost) no new medications– Restructuring into “severity” and “control” Restructuring into “severity” and “control” – Domains of “impairment” and “risk”Domains of “impairment” and “risk”– Six treatment steps (step-up/step-down)Six treatment steps (step-up/step-down)– More careful thought into ongoing management issuesMore careful thought into ongoing management issues– Summarizes extensively-validated scientific evidence that Summarizes extensively-validated scientific evidence that
the guidelines, when followed, lead to a significant the guidelines, when followed, lead to a significant reduction in the frequency and severity of asthma reduction in the frequency and severity of asthma symptoms and improve quality of lifesymptoms and improve quality of life
1313
New Strategies of the EPR-3
1414
– Asthma is a chronic inflammatory disorder of the airways
– The immunohistopathologic features of asthma include inflammatory cell infiltration
– Airway inflammation contributes to airway hyperresponsiveness, airflow limitation, respiratory symptoms, and disease chronicity
– In some patients, persistent changes in airway structure occur, including sub-basement fibrosis, mucus hypersecretion, injury to epithelial cells, smooth muscle hypertrophy, and angiogenesis (remodeling)
Key Points: Definition, Pathophysiology Key Points: Definition, Pathophysiology && Pathogenesis Pathogenesis

1515
Key Points: cont..Key Points: cont..
– Gene-by-environment interactions are important to the expression of asthma
– Atopy, the genetic predisposition for the development of an immunoglobulin E (IgE)-mediated response to common aeroallergens, is the strongest identifiable predisposing factor for developing asthma
– Viral respiratory infections are one of the most important causes of asthma exacerbation and may also contribute to the development of asthma
EPR 3, Section 2: Page 11
1616
Causes – We Don’t Know…Yet!Causes – We Don’t Know…Yet!
– Asthma has dramatically risen worldwide over the past Asthma has dramatically risen worldwide over the past decades, particularly in developed countries, and experts decades, particularly in developed countries, and experts are puzzled over the cause of this increaseare puzzled over the cause of this increase
– Not all people with allergies have asthma, and not all cases Not all people with allergies have asthma, and not all cases of asthma can be explained by allergic responseof asthma can be explained by allergic response
– Asthma is most likely caused by a convergence of factors Asthma is most likely caused by a convergence of factors that can include genes that can include genes (probably several)(probably several) and various and various environmental and biologic triggers environmental and biologic triggers
– e.g., infections, dietary patterns, hormonal changes in women, and e.g., infections, dietary patterns, hormonal changes in women, and allergens allergens

1717
4 Components of Asthma Management 4 Components of Asthma Management
Component 1Component 1: Measures of Asthma Assessment & : Measures of Asthma Assessment & Monitoring Monitoring
Component 2Component 2:: Education for a Partnership in Education for a Partnership in Asthma Care Asthma Care
Component 3Component 3:: Control of Environmental Factors & Control of Environmental Factors & Comorbid Conditions that Affect Comorbid Conditions that Affect
Asthma Asthma
Component 4Component 4: Medications: Medications

1818
Component 1Component 1
Measures of Asthma Assessment Measures of Asthma Assessment && MonitoringMonitoring

1919
Key Points - Key Points - Overview: Measures of Asthma Assessment Overview: Measures of Asthma Assessment && MonitoringMonitoring
Assessment and monitoring are closely linked to the concepts of Assessment and monitoring are closely linked to the concepts of severity, controlseverity, control, and , and responsivenessresponsiveness to treatment: to treatment:
– SeveritySeverity - - intensity of the disease process. Severity is intensity of the disease process. Severity is measured most easily and directly in a patient not receiving measured most easily and directly in a patient not receiving long-term-control therapy.long-term-control therapy.
– Control Control - - degree to which asthma degree to which asthma (symptoms, functional (symptoms, functional impairments, and risks of untoward events)impairments, and risks of untoward events) are minimized and the are minimized and the goals of therapy are met.goals of therapy are met.
– ResponsivenessResponsiveness - - the ease with which asthma control is the ease with which asthma control is achieved by therapy. achieved by therapy.
EPR -3 , Pg. 36,EPR -3 , Pg. 36,

2020
Key Points – Key Points – cont. cont. Domains Domains
ImpairmentImpairment (Present): (Present): – Frequency and intensity of symptoms Frequency and intensity of symptoms – Functional limitations (quality of life)Functional limitations (quality of life)
RiskRisk (Future):(Future):– Likelihood of asthma exacerbations orLikelihood of asthma exacerbations or– Progressive loss of lung function (reduced lung growth) Progressive loss of lung function (reduced lung growth) – Risk of adverse effects from medicationRisk of adverse effects from medication
EPR -3, Pg. 38-80, 277-345EPR -3, Pg. 38-80, 277-345
Assess Severity and Control based on:
2121
Key Points - Key Points - cont. cont. SeveritySeverity && ControlControl
If the patient is If the patient is notnot currently on a long-term controller at the currently on a long-term controller at the first visit:first visit:– Assess asthma severity to determine the appropriate Assess asthma severity to determine the appropriate
medication & treatment planmedication & treatment plan Once therapy is initiated, the emphasis is changed to the Once therapy is initiated, the emphasis is changed to the
assessment of assessment of asthma controlasthma control– The level of asthma control will guide decisions either to The level of asthma control will guide decisions either to
maintain or adjust therapymaintain or adjust therapy
Are used as follows for managing asthma:Are used as follows for managing asthma:

2222
Assessing Impairment Assessing Impairment (Present) Domain(Present) Domain
Assess by taking a careful, directed history and lung function measurement
Assess Quality of Life using standardized questionnaires– Asthma Control Test (ACT)– Childhood Asthma Control Test– Asthma Control Questionnaire– Asthma Therapy Assessment Questionnaire (ATAQ)
control index Some patients may perceive the severity of airflow
obstruction poorly

2323
Assessing Risk (Future)Assessing Risk (Future)DomainDomain
– Of adverse events in the future, especially of Of adverse events in the future, especially of exacerbations and of progressive, exacerbations and of progressive, irreversibleirreversible loss of loss of pulmonary function—is more problematic (airway pulmonary function—is more problematic (airway remodeling) remodeling)
– The test most used for assessing the risk of future The test most used for assessing the risk of future adverse events is adverse events is spirometryspirometry

2424
Measures of Assessment Measures of Assessment && Monitoring Monitoring
DiagnosisDiagnosis

2525
Key Points – Diagnosis of AsthmaKey Points – Diagnosis of Asthma
To establish a diagnosis of asthma the clinician should To establish a diagnosis of asthma the clinician should determine thatdetermine that::
– Episodic symptoms of airflow obstruction or airway Episodic symptoms of airflow obstruction or airway hyperresponsiveness are presenthyperresponsiveness are present
– Airflow obstruction is at least partially reversibleAirflow obstruction is at least partially reversible– Alternative diagnoses are excludedAlternative diagnoses are excluded
2626
Key Points – Methods to Establish Diagnosis Key Points – Methods to Establish Diagnosis
Recommended methods to establish the diagnosis areRecommended methods to establish the diagnosis are: :
– Detailed medical historyDetailed medical history– Physical exam focusing on the upper respiratory tract, Physical exam focusing on the upper respiratory tract,
chest, and skinchest, and skin– Spirometry to demonstrate obstruction and assess Spirometry to demonstrate obstruction and assess
reversibility, including in children 5 years of age or reversibility, including in children 5 years of age or olderolder
– Additional studies to exclude alternate diagnosesAdditional studies to exclude alternate diagnoses

2727
Key Indicators: Diagnosis of AsthmaKey Indicators: Diagnosis of Asthma
Has/does the patient:Has/does the patient:– had an attack or recurrent attacks of wheezing?had an attack or recurrent attacks of wheezing?– have a troublesome cough at night?have a troublesome cough at night?– wheeze or cough after exercise?wheeze or cough after exercise?– experience wheezing, chest tightness, or cough after experience wheezing, chest tightness, or cough after
exposure to airborne allergens or pollutants?exposure to airborne allergens or pollutants?– colds ‘go to the chest’ or take more than 10 days to clear colds ‘go to the chest’ or take more than 10 days to clear
up?up?– symptoms improved by appropriate asthma treatment?symptoms improved by appropriate asthma treatment?
Adapted from the GINA guidelines 2008
2828
Characterization Characterization && Classification of Classification of AsthmaAsthma
SeveritySeverity

2929
Key Points - Initial Assessment: Key Points - Initial Assessment: SeveritySeverity
Once a diagnosis is established:Once a diagnosis is established:– Identify precipitating factors (triggers)Identify precipitating factors (triggers)– Identify comorbidities that aggravate asthmaIdentify comorbidities that aggravate asthma– Assess the patient’s knowledge and skills for self-Assess the patient’s knowledge and skills for self-
managementmanagement– Classify severity using impairment and risk domainsClassify severity using impairment and risk domains
Pulmonary function testing (spirometry) to assess Pulmonary function testing (spirometry) to assess severityseverity
EPR -3, Sec. 3, pg. 47EPR -3, Sec. 3, pg. 47

3030
Assessment of Asthma SeverityAssessment of Asthma Severity
Previous GuidelinesPrevious Guidelines Frequency of daytime Frequency of daytime
symptomssymptoms Frequency of nighttime Frequency of nighttime
symptomssymptoms Lung functionLung function
2007 Guidelines2007 Guidelines ImpairmentImpairment
– Frequency of daytime /nighttime Frequency of daytime /nighttime symptomssymptoms
– Quality of life assessmentsQuality of life assessments– Frequency of SABA useFrequency of SABA use– Interference with normal activityInterference with normal activity– Lung function (FEVLung function (FEV11/FVC) /FVC)
RiskRisk– Exacerbations (frequency and Exacerbations (frequency and
severity)severity)
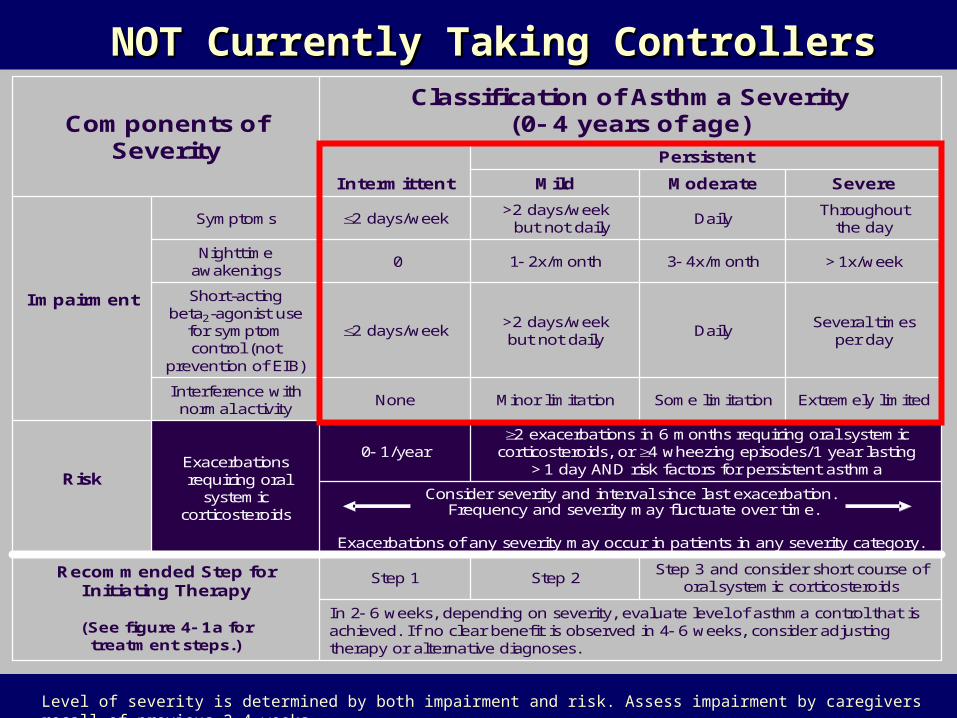
NOT Currently Taking ControllersNOT Currently Taking Controllers
Level of severity is determined by both impairment and risk. Assess impairment by caregivers recall of previous 2-4 weeks.
Step 3 and consider short course of oral systemic corticosteroids
Step 2Step 1Recommended Step for Initiating Therapy
(See figure 4 1a fortreatment steps.)
In 2 6 weeks, depending on severity, evaluate level of asthma control that is achieved. If no clear benefit is observed in 4 6 weeks, consider adjusting therapy or alternative diagnoses.
Extremely limitedSome limitationMinor limitationNoneInterference with normal activity
Several timesper day
Daily>2 days/weekbut not daily
2 days/week
Short-actingbeta2-agonist use
for symptom control (not
prevention of EIB)
Consider severity and interval since last exacerbation.Frequency and severity may fluctuate over time.
Exacerbations of any severity may occur in patients in any severity category.
Exacerbationsrequiring oral
systemic corticosteroids
Risk
Impairment
>1x/week3 4x/month1 2x/month0Nighttime
awakenings
Classification of Asthma Severity(0 4 years of age)
Persistent
Components ofSeverity
2 exacerbations in 6 months requiring oral systemic corticosteroids, or 4 wheezing episodes/1 year lasting
>1 day AND risk factors for persistent asthma0 1/year
Throughoutthe day
Daily>2 days/week
but not daily2 days/weekSymptoms
SevereModerateMildIntermittent

NOT Currently Taking ControllersNOT Currently Taking Controllers
Extremely limitedSome limitationMinor limitationNoneInterference withnormal activity
Step 1and consider short course oforal systemic corticosteroids
Step 3, medium-dose ICS option
In 2 6 weeks, evaluate level of asthma control that is achieved, and adjust therapy accordingly.
Step 3, medium-dose ICS option, or step 4
Risk
Exacerbationsrequiring oral
systemic corticosteroids
• FEV1/FVC <75%• FEV1/FVC = 75 80%• FEV1/FVC >80%• FEV1/FVC >85%
• FEV1 <60% predicted
• FEV1 = 60 80% predicted
• FEV1 = >80% predicted
• FEV1 >80% predicted
Lung function
2/year (see note)0 1/year (see note)
• Normal FEV1between exacerbations
Several timesper dayDaily>2 days/week
but not daily2 days/week
Short-actingbeta2-agonist use for symptom control (not
prevention of EIB)
Consider severity and interval since last exacerbation.Frequency and severity may fluctuate over time for patients in any severity category.
Step 2
Classification of Asthma Severity(5 11 years of age)
Impairment
Recommended Step for Initiating Therapy
(See figure 4 1b fortreatment steps.)
Persistent
Components of Severity
Relative annual risk of exacerbations may be related to FEV1.
Often 7x/week>1x/week butnot nightly3 4x/month2x/monthNighttime
awakenings
Throughoutthe day
Daily>2 days/week but not daily
2 days/weekSymptoms
SevereModerateMildIntermittent
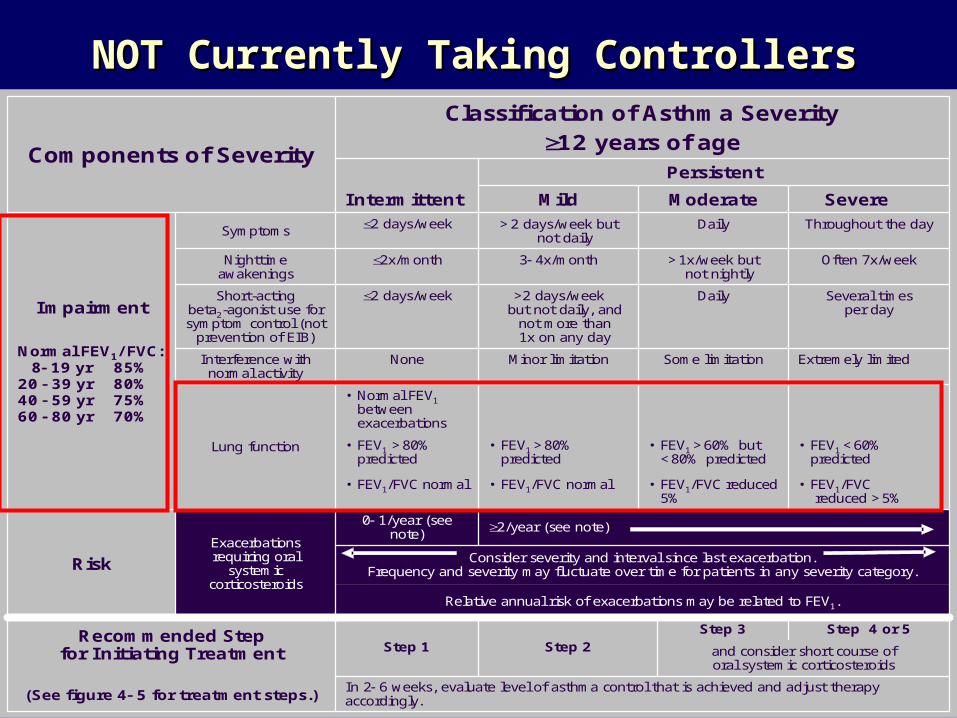
and consider short course oforal systemic corticosteroids
Step 4 or 5Step 3Step 2Step 1
Recommended Stepfor Initiating Treatment
(See figure 4 5 for treatment steps.)In 2 6 weeks, evaluate level of asthma control that is achieved and adjust therapy accordingly.
• Normal FEV1between exacerbations
Extremely limitedSome limitationMinor limitationNoneInterference with normal activity
Several timesper day
Daily>2 days/weekbut not daily, and
not more than1x on any day
2 days/weekShort-actingbeta2-agonist use for symptom control (not
prevention of EIB)
2/year (see note)0 1/year (see note)
• FEV1 <60% predicted
• FEV1 >60% but <80% predicted
• FEV1 >80% predicted
• FEV1 >80% predicted
• FEV1/FVCreduced >5%
• FEV1/FVC reduced 5%
• FEV1/FVC normal• FEV1/FVC normal
Risk
Relative annual risk of exacerbations may be related to FEV1.
Classification of Asthma Severity12 years of age
Consider severity and interval since last exacerbation.Frequency and severity may fluctuate over time for patients in any severity category.
Impairment
Normal FEV1/ FVC:8 19 yr 85%
20 39 yr 80%40 59 yr 75%60 80 yr 70%
PersistentComponents of Severity
Exacerbationsrequiring oral
systemic corticosteroids
Lung function
Often 7x/week>1x/week butnot nightly
3 4x/month2x/monthNighttime awakenings
Throughout the dayDaily>2 days/week but not daily
2 days/weekSymptoms
SevereModerateMildIntermittent
NOT Currently Taking ControllersNOT Currently Taking Controllers

Classifying Severity AFTER Control Classifying Severity AFTER Control is Achieved – All Ages is Achieved – All Ages
Lowest level Lowest level of treatment of treatment required to required to maintain maintain controlcontrol
Classification of Asthma SeverityClassification of Asthma Severity
IntermittentIntermittent PersistentPersistent
Step 1Step 1
MildMild ModerateModerate SevereSevere
Step 2Step 2 Step 3 Step 3 or 4or 4
Step 5 Step 5 or 6or 6
(already on controller)(already on controller)
3535
Periodic Assessment Periodic Assessment && Monitoring Monitoring
Asthma ControlAsthma Control

3636
Key Points – Key Points – Asthma Control (Goals of Therapy)Asthma Control (Goals of Therapy)
Reducing Reducing impairmentimpairment– Prevent chronic & troublesome symptomsPrevent chronic & troublesome symptoms– Prevent frequent use (Prevent frequent use (< < 2 days /wk) of inhaled SABA for 2 days /wk) of inhaled SABA for
symptomssymptoms– Maintain (near) “normal” pulmonary functionMaintain (near) “normal” pulmonary function– Maintain normal activity levels (including exercise and Maintain normal activity levels (including exercise and
other physical activity and attendance at work or school)other physical activity and attendance at work or school)– Meet patients’ and families’ expectations of and Meet patients’ and families’ expectations of and
satisfaction with asthma caresatisfaction with asthma care
EPR- 3, p. 50EPR- 3, p. 50

3737
Key Points – contKey Points – cont. .
Reducing Reducing RiskRisk– Prevent recurrent exacerbations of asthma and minimize Prevent recurrent exacerbations of asthma and minimize
the need for ER visits and hospitalizationsthe need for ER visits and hospitalizations– Prevent progressive loss of lung function - Prevent progressive loss of lung function - for children, for children,
prevent reduced lung growthprevent reduced lung growth– Provide optimal pharmacotherapy with minimal or no Provide optimal pharmacotherapy with minimal or no
adverse effectsadverse effects Periodic assessments at 1-6 month intervalsPeriodic assessments at 1-6 month intervals Patient self-assessment (w/clinician)Patient self-assessment (w/clinician) Spirometry testingSpirometry testing
EP-3 EP-3 , sec. 3, p. 53, sec. 3, p. 53

3838
Key Points cont. - Written AAP’s Key Points cont. - Written AAP’s && PFM PFM
Provide to all patients a written AAP based on signs and Provide to all patients a written AAP based on signs and symptoms and/or PEFsymptoms and/or PEF– Written AAPs are particularly recommended for patients Written AAPs are particularly recommended for patients
who have moderate or severe persistent asthma, a history who have moderate or severe persistent asthma, a history of severe exacerbations or poorly controlled asthmaof severe exacerbations or poorly controlled asthma..
Whether PF monitoring, symptom monitoring (available data Whether PF monitoring, symptom monitoring (available data show similar benefits for each), or a combo of approaches is show similar benefits for each), or a combo of approaches is used, self- monitoring is important to the effective self-used, self- monitoring is important to the effective self-management of asthma.management of asthma.
EPR -3 Sec. 3, P.53EPR -3 Sec. 3, P.53

3939
Peak Flow MonitoringPeak Flow Monitoring
Long-term daily PF monitoring can be helpful toLong-term daily PF monitoring can be helpful to::
– Detect early changes in asthma control that require Detect early changes in asthma control that require adjustments in treatment:adjustments in treatment:
– Evaluate responses to changes in treatmentEvaluate responses to changes in treatment– Provide a quantitative measure of impairmentProvide a quantitative measure of impairment
EPR-3 , Sec. 3, P.54EPR-3 , Sec. 3, P.54

4040
Asthma Control = Asthma GoalsAsthma Control = Asthma Goals
Definition of asthma control is the same as asthma Definition of asthma control is the same as asthma goalsgoals reducing impairment and riskreducing impairment and risk
Monitoring quality of life, any:Monitoring quality of life, any:– work or school missed because of asthma?work or school missed because of asthma?– reduction in usual activities?reduction in usual activities?– disturbances in sleep due to asthma?disturbances in sleep due to asthma?– Change in caregivers activities due to a child's Change in caregivers activities due to a child's
asthma?asthma?
4141
Responsiveness - Questions for Assessing Asthma Control
Ask the patient:– Has your asthma awakened you at night or early morning?– Have you needed more quick-relief medication (SABA) than
usual?– Have you needed any urgent medical care for your asthma,
such as unscheduled visits to your provider, an UC clinic, or the ER?
– Are you participating in your usual and desired activities?– If you are measuring your peak flow, has it been below your personal best?
Adapted from Global Initiative for Asthma: Pocket Guide for Asthma Management & Prevention.” 1995
4242
Actions to consider:– Assess whether the medications are being taken as
prescribed– Assess whether the medications are being inhaled with
correct technique– Assess lung function with spirometry and compare to
previous measurement– Adjust medications, as needed; either step up if control is
inadequate or step down if control is maximized, to achieve the best control with the lowest dose of medication
Adapted from Global Initiative for Asthma: Pocket Guide for Asthma Management & Prevention.” 1995
Responsiveness - Actions
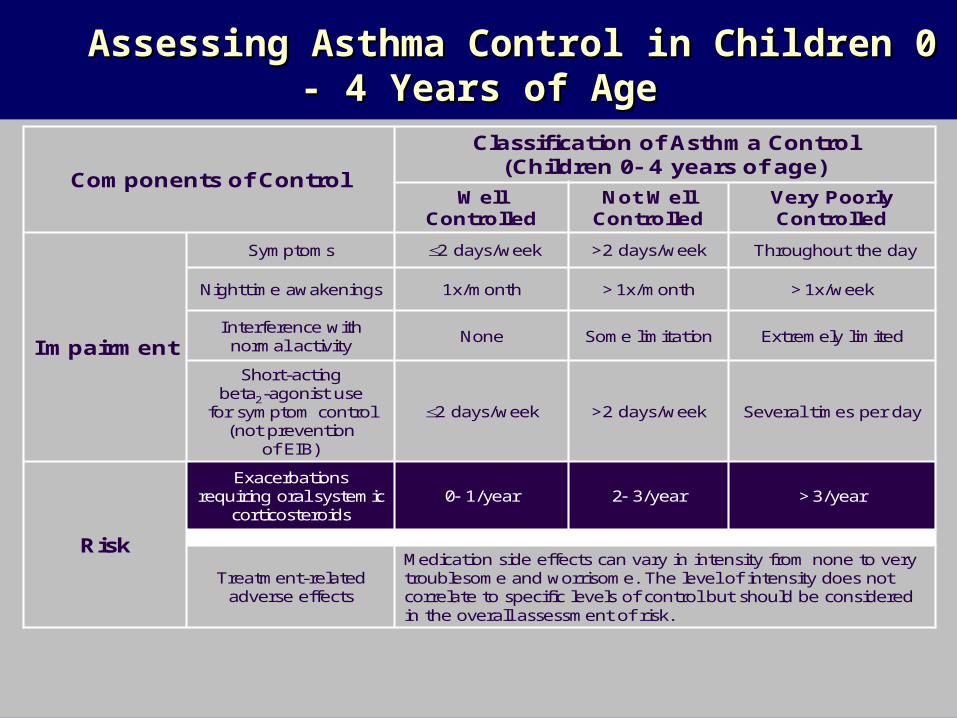
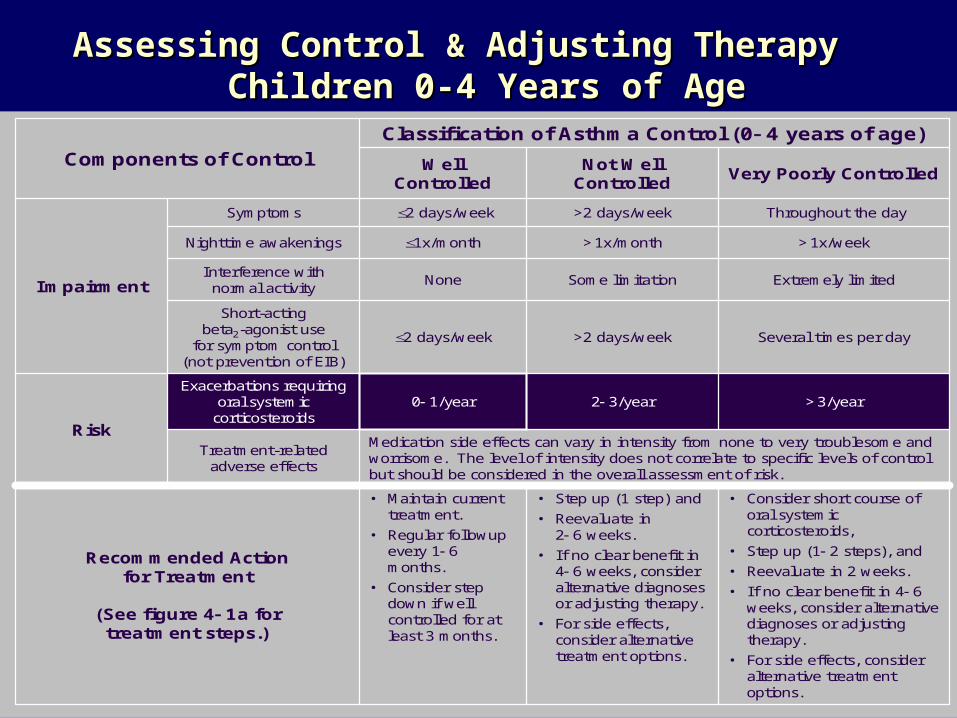
Assessing Asthma Control in Children 0 - 4 Years of AgeAssessing Asthma Control in Children 0 - 4 Years of Age
>3/year2 3/year0 1/yearExacerbations
requiring oral systemic corticosteroids
Risk
Several times per day>2 days/week2 days/week
Short-actingbeta2-agonist use
for symptom control (not prevention
of EIB)
Extremely limitedSome limitationNoneInterference with normal activity
Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be consideredin the overall assessment of risk.
Classification of Asthma Control(Children 0 4 years of age)
Impairment
Components of Control
Treatment-related adverse effects
>1x/week>1x/month1x/monthNighttime awakenings
Throughout the day>2 days/week2 days/weekSymptoms
Very Poorly Controlled
Not Well Controlled
Well Controlled

Assessing Asthma Control in Children 5 - 11 Years of AgeAssessing Asthma Control in Children 5 - 11 Years of Age
Impairment
2/year (see note)0 1/yearExacerbations requiring oral systemic corticosteroids
Lung function
<60% predicted/personal best
60 80% predicted/personal best
>80% predicted/personal best
FEV1 or peak flow
Evaluation requires long-term followup.
Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk.
Treatment-related adverse effects
Consider severity and interval since last exacerbation
Risk
Several times per day>2 days/week2 days/week
Short-actingbeta2-agonist use
for symptom control(not prevention of EIB)
Extremely limitedSome limitationNoneInterference withnormal activity
Classification of Asthma Control(Children 5 11 years of age)Components of Control
Reduction in lung growth
<75%75 80%>80% FEV1/FVC
2x/week2x/month1x/monthNighttimeawakenings
Throughout the day>2 days/week or multiple times on
2 days/week
2 days/week but not more than
once on each daySymptoms
Very Poorly Controlled
Not Well Controlled
Well Controlled
Consider severity and interval since last exacerbation
Evaluation requires long-term followup care
Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk.
Treatment-related adverse effects
Progressive loss of lung functionRisk
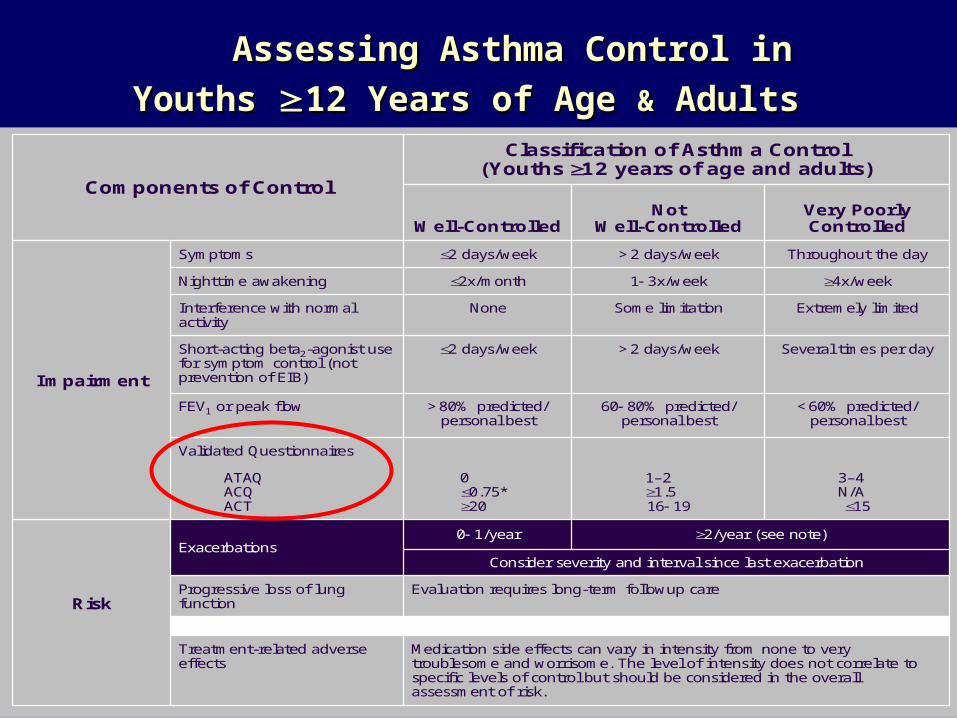
Validated Questionnaires
2/year (see note)
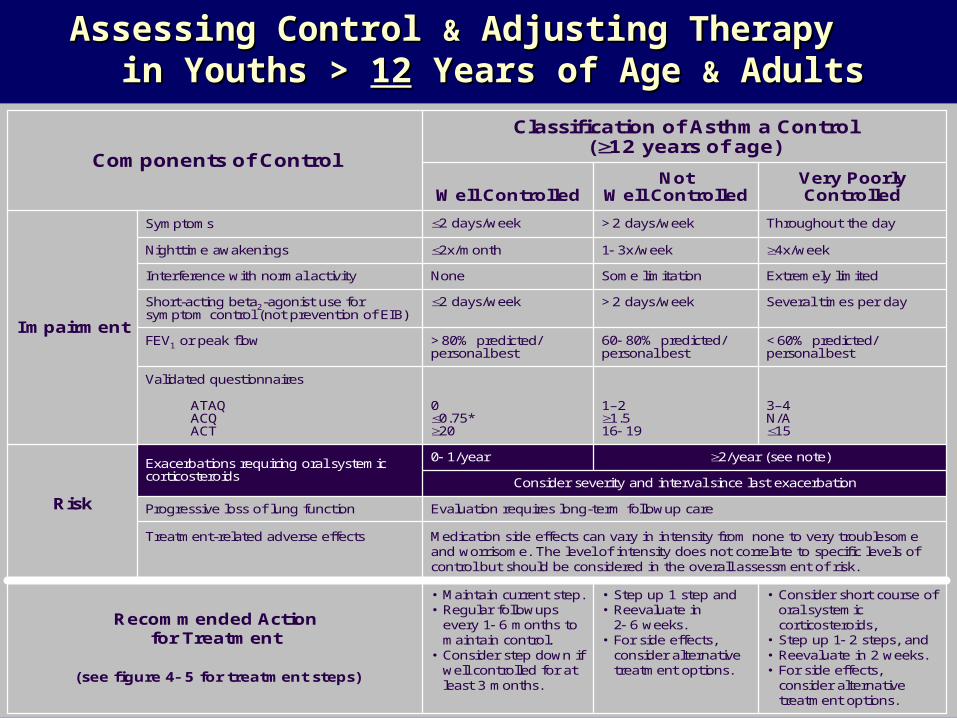
Throughout the day>2 days/week2 days/weekSymptoms
Impairment
3–4N/A15
1–21.516 19
00.75*20
ATAQACQACT
<60% predicted/personal best
60 80% predicted/personal best
>80% predicted/personal best
FEV1 or peak flow
Several times per day>2 days/week2 days/weekShort-acting beta2-agonist use for symptom control (not prevention of EIB)
0 1/yearExacerbations
Classification of Asthma Control(Youths 12 years of age and adults)
Components of Control
Extremely limitedSome limitationNoneInterference with normal activity
4x/week1 3x/week2x/monthNighttime awakening
Very PoorlyControlled
NotWell-ControlledWell-Controlled
Assessing Asthma Control in Youths Assessing Asthma Control in Youths 12 Years of Age 12 Years of Age && Adults Adults

4646
Component 2Component 2
Education for a Partnership in Education for a Partnership in Asthma CareAsthma Care

4747
Key Points - EducationKey Points - Education
Self management education is essential and should be Self management education is essential and should be integrated into all aspects of care; requires repetition and integrated into all aspects of care; requires repetition and reinforcementreinforcement
Provide Provide allall patients with a patients with a writtenwritten asthma action plan that asthma action plan that includes 2 aspects:includes 2 aspects:– Daily managementDaily management– How to recognize & handle worsening asthma symptomsHow to recognize & handle worsening asthma symptoms
Regular review of the status of patients asthma controlRegular review of the status of patients asthma control– Teach and reinforce at every opportunityTeach and reinforce at every opportunity
Develop an active partnership with the patient and familyDevelop an active partnership with the patient and family
EPR – 3, Section 3, Pg. 93EPR – 3, Section 3, Pg. 93

4848
Key Points – Education cont.Key Points – Education cont.
Encourage adherence by:Encourage adherence by:– Choosing a tx regimen that achieves outcomes and Choosing a tx regimen that achieves outcomes and
addresses preferences important to the addresses preferences important to the patientpatient– Review the success of tx plan and make changes as Review the success of tx plan and make changes as
neededneeded Tailor the plan to needs of each patientTailor the plan to needs of each patient Encourage community based interventionsEncourage community based interventions Asthma education provided by trained health Asthma education provided by trained health
professionals should be reimbursed and considered an professionals should be reimbursed and considered an integral part of effective asthma care ! integral part of effective asthma care ! (AE-C)(AE-C)

4949
Key Educational MessagesKey Educational Messages
– Significance of diagnosisSignificance of diagnosis– Inflammation as the underlying cause Inflammation as the underlying cause – Controllers vs. quick-relieversControllers vs. quick-relievers– How to use medication delivery devicesHow to use medication delivery devices– Triggers, including 2Triggers, including 2ndnd hand smoke hand smoke– Home monitoring/ self-managementHome monitoring/ self-management– How/when to contact the providerHow/when to contact the provider– Need for continuous, on-going interaction w/the clinician Need for continuous, on-going interaction w/the clinician
to step up/down therapyto step up/down therapy– Annual influenza vaccine Annual influenza vaccine

5050
Other Educational Points of Care Other Educational Points of Care
ER Department and hospital based ER Department and hospital based Medication therapy management (Pharmacist)Medication therapy management (Pharmacist) Community basedCommunity based Home based for caregivers including home based Home based for caregivers including home based
allergen/ environmental assessmentallergen/ environmental assessment Computer based technology Computer based technology Case management for high-risk patientsCase management for high-risk patients

5151
Maintaining the PartnershipMaintaining the Partnership
Promote open communication w/patient and family by Promote open communication w/patient and family by addressing at each visitaddressing at each visit::
– Ask what concerns they have and what they want Ask what concerns they have and what they want addressed during the visitaddressed during the visit
– Review short – term goals agreed to at the initial visitReview short – term goals agreed to at the initial visit– Review written AAP and steps to take – adjust as neededReview written AAP and steps to take – adjust as needed– Encourage parents to take a copy of AAP to the school or Encourage parents to take a copy of AAP to the school or
childcare setting or childcare setting or sendsend a copy to the school nurse a copy to the school nurse– Teach and reinforce key educational messagesTeach and reinforce key educational messages– Provide simple, brief, written materials that reinforce the Provide simple, brief, written materials that reinforce the
actions and skills taughtactions and skills taught
5252
Component 3Component 3
Control of Environmental Factors Control of Environmental Factors && Comorbid Conditions that Affect AsthmaComorbid Conditions that Affect Asthma

5353
Key Points – Environmental FactorsKey Points – Environmental Factors
All patients with asthma shouldAll patients with asthma should::– Reduce, if possible, exposure to allergens & irritants they are Reduce, if possible, exposure to allergens & irritants they are
sensitive toosensitive too– Understand effective allergen avoidance is multifaceted and Understand effective allergen avoidance is multifaceted and
individual steps alone are ineffectiveindividual steps alone are ineffective– Avoid exertion outdoors when levels of air pollution are highAvoid exertion outdoors when levels of air pollution are high– Avoid use of nonselective beta-blockersAvoid use of nonselective beta-blockers– Avoid sulfite-containing and otherAvoid sulfite-containing and other foods they are sensitive to foods they are sensitive to– Avoid use of humidifiers (generally)Avoid use of humidifiers (generally)

5454
Key Points – Environmental ContKey Points – Environmental Cont..
Clinicians shouldClinicians should::– Evaluate a patient for other chronic co-morbid conditions Evaluate a patient for other chronic co-morbid conditions
when asthma cannot be well controlledwhen asthma cannot be well controlled– Encourage their asthma patients to receive a yearly Encourage their asthma patients to receive a yearly
influenza vaccination (inactivated)influenza vaccination (inactivated)– Consider allergen immunotherapy when appropriateConsider allergen immunotherapy when appropriate– Ask about possible occupational exposures, particularly Ask about possible occupational exposures, particularly
those who have new-onset disease (work related asthma)those who have new-onset disease (work related asthma)

5555
Component 4Component 4
MedicationsMedications
5656
Key Points - MedicationsKey Points - Medications
2 general classes:2 general classes:– Long-term control medicationsLong-term control medications– Quick-Relief medicationsQuick-Relief medications
Controller medicationsController medications::– Corticosteroids Corticosteroids – Long Acting Beta Agonists (LABA’s)Long Acting Beta Agonists (LABA’s)– Leukotriene modifiers (LTRA)Leukotriene modifiers (LTRA)– Cromolyn & NedocromilCromolyn & Nedocromil– Methylxanthines:Methylxanthines: ( (Sustained-release theophylline) Sustained-release theophylline)

5757
Key Points – Medications contKey Points – Medications cont..
Quick- relief medicationsQuick- relief medications– Short acting bronchodilators (SABA’s)Short acting bronchodilators (SABA’s)– Systemic corticosteroidsSystemic corticosteroids– AnticholinergicsAnticholinergics

5858
Key Points: Safety of ICS’sKey Points: Safety of ICS’s
– ICS’s are the most effective long-term therapy available, are ICS’s are the most effective long-term therapy available, are well tolerated & safe at recommended doseswell tolerated & safe at recommended doses
– The potential but small risk of adverse events from the use The potential but small risk of adverse events from the use of ICS treatment is well balanced by their efficacyof ICS treatment is well balanced by their efficacy
– The dose-response curve for ICS treatment begins to flatten The dose-response curve for ICS treatment begins to flatten at low to medium dosesat low to medium doses
– Most benefit is achieved with relatively low doses, whereas Most benefit is achieved with relatively low doses, whereas the risk of adverse effects increases with dosethe risk of adverse effects increases with dose
5959
Key Points: Key Points: Reducing Potential Adverse Effects Reducing Potential Adverse Effects
Spacers or valved holding chambers (VHCs) used with non-breath-Spacers or valved holding chambers (VHCs) used with non-breath-activated MDIs reduce local side effectsactivated MDIs reduce local side effects– There is little or no data on use of spacers with hydrofluoroalkane There is little or no data on use of spacers with hydrofluoroalkane
(HFA) MDIs(HFA) MDIs Patients should rinse their mouths (rinse and spit) after (ICS) Patients should rinse their mouths (rinse and spit) after (ICS)
inhalationinhalation Use the lowest dose of ICS that maintains asthma control: Use the lowest dose of ICS that maintains asthma control:
– Evaluate patient adherence and inhaler technique as well as Evaluate patient adherence and inhaler technique as well as environmental factors before increasing the dose of ICSenvironmental factors before increasing the dose of ICS
To achieve or maintain control of asthma, add a LABA to a low or To achieve or maintain control of asthma, add a LABA to a low or medium dose of ICS rather than using a higher dose of ICS medium dose of ICS rather than using a higher dose of ICS
Monitor linear growth in childrenMonitor linear growth in children

6060
Key Points:Key Points:Safety of Long-Acting BetaSafety of Long-Acting Beta22-Agonists -Agonists (LABA’s)(LABA’s)
– Adding a LABA to the tx of patients whose asthma is not well Adding a LABA to the tx of patients whose asthma is not well controlled on low- or medium-dose ICS improves lung function, controlled on low- or medium-dose ICS improves lung function, decreases symptoms, and reduces exacerbations and use of SABA decreases symptoms, and reduces exacerbations and use of SABA for quick relief in most patientsfor quick relief in most patients
– The FDA determined that a Black Box warning was warranted on all The FDA determined that a Black Box warning was warranted on all preparations containing a LABApreparations containing a LABA
– For patients who have asthma not sufficiently controlled with ICS For patients who have asthma not sufficiently controlled with ICS alone, the option to increase the ICS dose should be given alone, the option to increase the ICS dose should be given equal equal weightweight to the option of the addition of a LABA to ICS to the option of the addition of a LABA to ICS
– It is not currently recommended that LABA be used for treatment of It is not currently recommended that LABA be used for treatment of acute symptoms or exacerbationsacute symptoms or exacerbations
– LABAs are not to be used as monotherapy for long-term controlLABAs are not to be used as monotherapy for long-term control
6161
FDA Recommendations for LABA’sFDA Recommendations for LABA’sFebruary 2010February 2010
– Are contraindicated without the use of an asthma controller Are contraindicated without the use of an asthma controller medication such as an ICSmedication such as an ICS
– Single-ingredient LABAs should only be used in combination Single-ingredient LABAs should only be used in combination with an asthma controller medication; they should not be with an asthma controller medication; they should not be used aloneused alone
– Should only be used long-term in patients whose asthma Should only be used long-term in patients whose asthma cannot be adequately controlled on asthma controller cannot be adequately controlled on asthma controller medicationsmedications
6262
FDA Recommendations for LABA’s Cont.FDA Recommendations for LABA’s Cont.
– Should be used for the shortest duration of time required to Should be used for the shortest duration of time required to achieve control of asthma symptoms and discontinued, if achieve control of asthma symptoms and discontinued, if possible, once asthma control is achievedpossible, once asthma control is achieved
– Patients should then be maintained on an asthma controller Patients should then be maintained on an asthma controller medicationmedication
– Pediatric and adolescent patients who require the addition Pediatric and adolescent patients who require the addition of a LABA to an ICS should use a combination product of a LABA to an ICS should use a combination product containing both an ICS and a LABA, to ensure compliance containing both an ICS and a LABA, to ensure compliance with both medicationswith both medications

6363
Key Points: Key Points: Safety of Short -Acting BetaSafety of Short -Acting Beta22-Agonists (SABA’s)-Agonists (SABA’s)
– SABAs are the most effective medication for relieving SABAs are the most effective medication for relieving acute bronchospasm acute bronchospasm
– Increasing use of SABA treatment or using SABA >2 days Increasing use of SABA treatment or using SABA >2 days a week for symptom relief (not prevention of EIB) a week for symptom relief (not prevention of EIB) indicates inadequate control of asthmaindicates inadequate control of asthma
– Regularly scheduled, daily, chronic use of SABA is Regularly scheduled, daily, chronic use of SABA is notnot recommendedrecommended

6464
Section 4 Section 4
Managing Asthma Long Term Managing Asthma Long Term ““The Stepwise Approach”The Stepwise Approach”
6565
Key Points: Managing Asthma Long TermKey Points: Managing Asthma Long Term
The goal of therapy is to control asthma by:The goal of therapy is to control asthma by:– Reducing impairmentReducing impairment– Reducing riskReducing risk
A stepwise approach to medication therapy is A stepwise approach to medication therapy is recommended to gain and maintain asthma controlrecommended to gain and maintain asthma control
Monitoring and follow-up is essentialMonitoring and follow-up is essential

6666
Treatment: Treatment: Principles of “Stepwise” Therapy Principles of “Stepwise” Therapy
““The goal of asthma therapy is to maintain long-The goal of asthma therapy is to maintain long-term control of asthma with the least amount of term control of asthma with the least amount of medication and hence minimal risk for adverse medication and hence minimal risk for adverse
effects”effects”..
EPR -3, Section 4, P. 284EPR -3, Section 4, P. 284

6767
Principles of Step Therapy to Maintain Principles of Step Therapy to Maintain ControlControl
Step upStep up medication dose if symptoms are not controlled medication dose if symptoms are not controlled If very poorly controlled, consider an increase by 2 steps, If very poorly controlled, consider an increase by 2 steps,
add oral corticosteroids, or bothadd oral corticosteroids, or both Before increasing medication therapy, evaluate:Before increasing medication therapy, evaluate:
– Exposure to environmental triggers Exposure to environmental triggers – Adherence to therapyAdherence to therapy– For proper device techniqueFor proper device technique– Co-morbiditiesCo-morbidities
6868
Follow-up AppointmentsFollow-up Appointments
Visits every 2-6 weeks until asthma control is achievedVisits every 2-6 weeks until asthma control is achieved When control is achieved, follow-up every 3-6 monthsWhen control is achieved, follow-up every 3-6 months Step-down in therapyStep-down in therapy::
– When asthma is well-controlled for at least 3 monthsWhen asthma is well-controlled for at least 3 months Patients may relapse with total discontinuation or Patients may relapse with total discontinuation or
reduction of inhaled corticosteroidsreduction of inhaled corticosteroids
• Consider short course of oral systemic corticosteroids,
• Step up (1 2 steps), and
• Reevaluate in 2 weeks.
• If no clear benefit in 4 6 weeks, consider alternative diagnoses or adjusting therapy.
• For side effects, consider alternative treatment options.
• Step up (1 step) and
• Reevaluate in2 6 weeks.
• If no clear benefit in 4 6 weeks, consider alternative diagnoses or adjusting therapy.
• For side effects, consider alternative treatment options.
• Maintain current treatment.
• Regular followupevery 1 6 months.
• Consider step down if well controlled for at least 3 months.
Recommended Actionfor Treatment
(See figure 4 1a fortreatment steps.)
>3/year2 3/year0 1/yearExacerbations requiring
oral systemic corticosteroids
Risk
Several times per day>2 days/week2 days/week
Short-actingbeta2-agonist use
for symptom control (not prevention of EIB)
Extremely limitedSome limitationNoneInterference with normal activity
Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk.
Classification of Asthma Control (0 4 years of age)
Impairment
Components of Control
Treatment-related adverse effects
>1x/week>1x/month1x/monthNighttime awakenings
Throughout the day>2 days/week2 days/weekSymptoms
Very Poorly ControlledNot Well
ControlledWell
Controlled
Assessing Control Assessing Control && Adjusting Therapy Adjusting Therapy Children 0-4 Years of AgeChildren 0-4 Years of Age

IntermittentAsthma
Persistent Asthma: Daily MedicationConsult asthma specialist if step 3 care or higher is required.
Consider consultation at step 2
Step 1
PreferredSABA PRN
Step 2
PreferredLow dose ICSAlternative Montelukast or Cromolyn
Step 3
PreferredMedium Dose ICS
Step 4
PreferredMedium Dose ICS
AND
Either:Montelukast or LABA
Step 5
PreferredHigh Dose ICS
AND
Either:Montelukast or LABA
Step 6
PreferredHighDose ICS
AND
Either:Montelukast or LABA
ANDOral corticosteroid
Patient Education and Environmental Control at Each Step
Stepwise Approach for Managing Asthma in Children 0-4 Years of Age
Quick-relief medication for ALL patients -SABA as needed for symptoms.With VURI: SABA every 4-6 hours up to 24 hours. Consider short course of corticosteroids with (or hx of) severe exacerbation
Step down if
possible
(and asthma is well
controlled at least 3
months)
Assess control
Step up if needed
(first check adherence, environmental control)

Assessing Control Assessing Control && Adjusting Therapy Adjusting Therapy Children 5-11 Years of AgeChildren 5-11 Years of Age
Consider severity and interval since last exacerbation
• Consider short course of oral systemic corticosteroids,
• Step up 1 2 steps, and• Reevaluate in 2 weeks.• For side effects, consider
alternative treatment options.
• Step up at least 1 step and
• Reevaluate in 2 6 weeks.
• For side effects: consider alternative treatment options.
• Maintain current step.• Regular followup
every 1 6 months.• Consider step down if
well controlled for at least 3 months.
Recommended Actionfor Treatment
(See figure 4 1b fortreatment steps.)
Lung function
<60% predicted/personal best
60 80% predicted/personal best
>80% predicted/personal best
• FEV1 or peak flow
Evaluation requires long-term followup.
Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk.
Treatment-related adverse effects
2/year (see note)0 1/yearExacerbations requiring oral systemic
corticosteroids
Risk
Several times per day>2 days/week2 days/week
Short-actingbeta2-agonist use
for symptom control(not prevention of EIB)
Extremely limitedSome limitationNoneInterference with normal activity
Classification of Asthma Control (5 11 years of age)
Impairment
Components of Control
Reduction inlung growth
<75% 75 80% >80% • FEV1/FVC
2x/week2x/month1x/monthNighttimeawakenings
Throughout the day>2 days/week or multiple times on
2 days/week
2 days/week but not more than once on each
daySymptoms
Very Poorly ControlledNot Well
ControlledWell
Controlled

IntermittentAsthma
Persistent Asthma: Daily MedicationConsult asthma specialist if step 4 care or higher is required.
Consider consultation at step 3
Patient Education and Environmental Control at Each Step
Stepwise Approach for managing asthma in children 5-11 years of age
Quick-relief medication for ALL patientsSABA as needed for symptoms.Short course of oral corticosteroids maybe needed.
Step down if possible
(and asthma is well
controlled at least 3
months)
Assess control
Step up if needed
(first check adherence, environmental control,
and comorbid
conditions)
Preferred
SABA PRN
Step 1
Preferred
Low dose ICS
AlternativeLTRA, CromolynNedocromil orTheophylline
Step 2Preferred
EitherLow Dose ICS + LABA, LTRA, or Theophylline
OR
Medium Dose ICS
Step 3 Preferred
Medium Dose ICS + LABA
AlternativeMedium dose ICS + either LTRA, or Theophylline
Step 4 Preferred
High Dose ICS + LABA
AlternativeHigh dose ICS + either LTRA, or Theophylline
Step 5Preferred
High Dose ICS + LABA + oral corticosteroid
AlternativeHigh dose ICS + either LTRA, or Theophylline + oral corticosteroid
Step 6
Assessing Control Assessing Control && Adjusting Therapy Adjusting Therapy in Youths > in Youths > 1212 Years of Age Years of Age && Adults Adults
2/year (see note)0 1/year
• Consider short course of oral systemic corticosteroids,
• Step up 1 2 steps, and• Reevaluate in 2 weeks.• For side effects,
consider alternative treatment options.
• Step up 1 step and• Reevaluate in
2 6 weeks.• For side effects,
consider alternative treatment options.
• Maintain current step.• Regular followups
every 1 6 months to maintain control.
• Consider step down if well controlled for at least 3 months.
Recommended Actionfor Treatment
(see figure 4 5 for treatment steps)
Evaluation requires long-term followup care
Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk.
Treatment-related adverse effects
Progressive loss of lung functionRisk
Validated questionnaires
Throughout the day>2 days/week2 days/weekSymptoms
Impairment
3–4N/A15
1–21.516 19
00.75*20
ATAQACQACT
<60% predicted/personal best
60 80% predicted/personal best
>80% predicted/personal best
FEV1 or peak flow
Several times per day>2 days/week2 days/weekShort-acting beta2-agonist use for symptom control (not prevention of EIB)
Consider severity and interval since last exacerbation
Exacerbations requiring oral systemic corticosteroids
Classification of Asthma Control(12 years of age)
Components of Control
Extremely limitedSome limitationNoneInterference with normal activity
4x/week1 3x/week2x/monthNighttime awakenings
Very PoorlyControlled
NotWell ControlledWell Controlled

IntermittentAsthma
Persistent Asthma: Daily MedicationConsult asthma specialist if step 4 care or higher is required.
Consider consultation at step 3
Step 1
Preferred:SABA PRN
Step 2
Preferred:Low dose ICS
Alternative: Cromolyn, LTRA, Nedocromil or Theophylline
Step 3Preferred:
Low-dose ICS + LABA OR – Medium dose ICS
Alternative: Low-dose ICS + either LTRA, Theophylline, or Zileuton
Step 4
Preferred:Medium Dose ICS + LABA
Alternative:Medium-dose ICS + either LTRA, Theophylline, or Zileuton
Step 5
PreferredHigh Dose ICS + LABA
AND
Consider Omalizumab for patients who have allergies
Step 6
PreferredHigh dose ICS + LABA + oral corticosteroid
AND
Consider Omalizumab for patients who have allergies
Each Step: Patient Education and Environmental Control and management of comorbiditiesSteps 2 – 4: Consider subcutaneous allergen immunotherapy for patients who have allergic asthma
Stepwise Approach for Managing Asthma in Youths >12 Years of Age & Adults
•Quick-relief medication for ALL patients -SABA as needed for symptoms: up to 3 tx @ 20 minute intervals prn. Short course of o systemic corticosteroids may be needed.• Use of SABA >2 days a week for symptom relief (not prevention of EIB) generally indicates inadequate control & the need to step up treatment.
Step down if
possible
(and asthma is well
controlled at least 3
months)
Assess control
Step up if needed
(first check adherence, environmental control & comorbid conditions)

7575
Section 5Section 5
Managing Exacerbations of AsthmaManaging Exacerbations of Asthma
7676
Key Points –Key Points –Managing Exacerbations Managing Exacerbations
Early treatment of asthma exacerbations is the best strategy Early treatment of asthma exacerbations is the best strategy for management:for management:
Patient education includes a written asthma action plan (AAP) to Patient education includes a written asthma action plan (AAP) to guide patient self management of exacerbations‑guide patient self management of exacerbations‑– especially for patients who have moderate or severe persistent especially for patients who have moderate or severe persistent
asthma and any patient who has a history of severe asthma and any patient who has a history of severe exacerbationsexacerbations
A peak flow based plan for patients who have difficulty perceiving ‑ ‑A peak flow based plan for patients who have difficulty perceiving ‑ ‑airflow obstruction and worsening asthma is recommendedairflow obstruction and worsening asthma is recommended
EPR -3 Pg. 373EPR -3 Pg. 373
7777
Key Points – cont.Key Points – cont.
– Recognition of early signs of worsening asthma & taking Recognition of early signs of worsening asthma & taking prompt actionprompt action
– Appropriate intensification of therapy, often including a Appropriate intensification of therapy, often including a short course of oral corticosteroidsshort course of oral corticosteroids
– Removal or avoidance of the environmental factors Removal or avoidance of the environmental factors contributing to the exacerbationcontributing to the exacerbation
– Prompt communication between patient and clinician about Prompt communication between patient and clinician about any serious deterioration in symptoms or peak flow, any serious deterioration in symptoms or peak flow, decreased responsiveness to SABAs, or decreased duration decreased responsiveness to SABAs, or decreased duration of effectof effect

7878
Exacerbations Defined - RISKExacerbations Defined - RISK
Are acute or subacute episodes of progressively worsening Are acute or subacute episodes of progressively worsening shortness of breath, cough, wheezing, and chest tightness?shortness of breath, cough, wheezing, and chest tightness?
— — or some combination of these symptoms or some combination of these symptoms Are characterized by decreases in expiratory airflow that can Are characterized by decreases in expiratory airflow that can
be documented and quantified by spirometry or peak be documented and quantified by spirometry or peak expiratory flowexpiratory flow– These objective measures more reliably indicate the These objective measures more reliably indicate the
severity of an exacerbation than does the severity of severity of an exacerbation than does the severity of symptomssymptoms

Classifying Severity of Asthma Exacerbations in the UC or ER SettingClassifying Severity of Asthma Exacerbations in the UC or ER Setting
SeveritySeverity Symptoms & Signs Initial PEF (or FEV1)
Clinical Course
Mild
Dyspnea only with activity (assess tachypnea in young children)
PEF 70 percent predicted or personal best
Usually cared for at home Prompt relief with inhaled SABA Possible short course of oral systemic
corticosteroids
Moderate Dyspnea interferes with or limits usual activity
PEF 4069 percent predicted or personal best
Usually requires office or ED visit Relief from freq. inhaled SABA Oral systemic corticosteroids; some
symptoms last 1–2 days after treatment is begun
Severe
Dyspnea at rest; interferes with conversation
PEF <40 percent predicted or personal best
Usually requires ED visit and likely hospitalization
Partial relief from frequent inhaled SABA
PO systemic corticosteroids; some symptoms last >3 days after treatment is begun
Adjunctive therapies are helpful
Subset: Life threatening Too dyspneic to speak;
perspiring
PEF <25 percent predicted or personal best
Requires ED/hospitalization; possible ICU
Minimal or no relief w/ frequent inhaled SABA
Intravenous corticosteroids Adjunctive therapies are helpful

Assess Severity
Patients at high risk for a fatal attack (see figure 5–2a) require immediate medical attention after initial treatment.
Symptoms and signs suggestive of a more serious exacerbation such as marked breathlessness, inability to speak more than short phrases, use of accessory muscles, or drowsiness (see figure 5–3) should result in initial treatment while immediately consulting with a clinician.
Less severe signs and symptoms can be treated initially with assessment of response to therapy and further steps as listed below.
If available, measure PEF—values of 50–79% predicted or personal best indicate the need for quick-relief mediation. Depending on the response to treatment, contact with a clinician may also be indicated. Values below 50% indicate the need for immediate medical care.
Initial Treatment
Inhaled SABA: up to two treatments 20 minutes apart of 2–6 puffs by metered-dose inhaler (MDI) or nebulizer treatments.
Note: Medication delivery is highly variable. Children and individuals who have exacerbations of lesser severity may need fewer puffs than suggested above.
Good Response
No wheezing or dyspnea(assess tachypnea in young children).
PEF 80% predicted or personal best.
Contact clinician for followup instructions and further management.
May continue inhaled SABA every 3–4 hours for 24–48 hours.
Consider short course of oral systemic corticosteroids.
Incomplete Response
Persistent wheezing and dyspnea (tachypnea).
PEF 50–79% predicted or personal best.
Add oral systemic corticosteroid.
Continue inhaled SABA.
Contact clinician urgently (this day) for further instruction.
Poor Response
Marked wheezing and dyspnea.
PEF <50% predicted or personal best.
Add oral systemic corticosteroid.
Repeat inhaled SABA immediately.
If distress is severe and nonresponsive to initial treatment:
—Call your doctor AND—PROCEED TO ED;—Consider calling 9–1–1
(ambulance transport).
To ED.
Managing Asthma Exacerbations at Home
8181
What the EPR -3 Does What the EPR -3 Does NOTNOT Recommend Recommend
– Drinking large volumes of liquids or breathing warm, Drinking large volumes of liquids or breathing warm, moist air moist air (e.g., the mist from a hot shower)(e.g., the mist from a hot shower)
– Using over-the-counter products such as antihistamines Using over-the-counter products such as antihistamines or cold remediesor cold remedies
– Although pursed-lip and other forms of controlled Although pursed-lip and other forms of controlled breathing may help to maintain calm during respiratory breathing may help to maintain calm during respiratory distress, these methods do distress, these methods do not not bring about improvement bring about improvement in lung functionin lung function
EPR -3 , P.384EPR -3 , P.384

8282
Many Thanks To -Many Thanks To -
Colleagues who shared their power point presentations and/or provided feedback on the foundation for this presentation:
– Dr. Gail M Brottman MD, Director, Dr. Gail M Brottman MD, Director, Pediatric Pulmonary Medicine, HCMC Pediatric Pulmonary Medicine, HCMC
– Dr. Don Uden, Pharm. D., Professor, Dr. Don Uden, Pharm. D., Professor, University of Minnesota, College of University of Minnesota, College of Pharmacy Pharmacy
– Dr. Barbara P. Yawn, MD, MSc, Dr. Barbara P. Yawn, MD, MSc, Director of Research, Olmsted Medical Director of Research, Olmsted Medical ClinicClinic
– Dr. Mamta Reddy, MD, ChiefDr. Mamta Reddy, MD, Chief Allergy/ Immunology, Bronx Lebanon Hospital Center, NYAllergy/ Immunology, Bronx Lebanon Hospital Center, NY– Mary Bielski, RN, LSN, CNS, Mary Bielski, RN, LSN, CNS,
Nursing Service Manager, Minneapolis Public Schools Nursing Service Manager, Minneapolis Public Schools

8383
Minnesota Department of HealthMinnesota Department of HealthAsthma ProgramAsthma Program
www.health.state.mn.us/asthmawww.health.state.mn.us/asthma

















![(750B) 30]046-242-1529 046-244-5629 (500B) (500B) (700B ... · (750b) 30]046-242-1529 046-244-5629 (500b) (500b) (700b) (1,800b) 046-229-4129 1130—1500 (l.o.iÇ.oo) 1730—2330](https://static.fdocuments.us/doc/165x107/5f9026deeaa0d031143b4e8b/750b-30046-242-1529-046-244-5629-500b-500b-700b-750b-30046-242-1529.jpg)