1 Medicaid Integrity Contractors & Medicaid RACs Are You Prepared? WV HFMA Spring Revenue Cycle...
30
1 Medicaid Integrity Contractors & Medicaid RACs Are You Prepared? WV HFMA Spring Revenue Cycle Meeting M. Jill Newberry, CPA, CPC Senior Manager Arnett Foster Toothman, P.L.L.C. [email protected] 800-642-3601
-
Upload
spencer-hayman -
Category
Documents
-
view
217 -
download
2
Transcript of 1 Medicaid Integrity Contractors & Medicaid RACs Are You Prepared? WV HFMA Spring Revenue Cycle...
1
Medicaid Integrity Contractors & Medicaid RACs
Are You Prepared?
WV HFMA Spring Revenue Cycle Meeting
M. Jill Newberry, CPA, CPCSenior Manager
Arnett Foster Toothman, [email protected]
800-642-3601
2
Medicaid Integrity Program (MIP)
Medicaid Integrity Program In February 2006, the Deficit Reduction Act (DRA) of 2005 was
signed into law and created the Medicaid Integrity Program (MIP) under section 1936 of the Social Security Act (the Act).
The MIP is the first comprehensive Federal strategy to prevent and reduce provider fraud, waste, and abuse in the $300 billion per year Medicaid program.
Three – Year Rollout (Ordered by DRA ’05) Underway -- CMS Region V/VII (OH), Region III/IV (WV, VA, KY) audits scheduled to begin November 2009
3
Medicaid Integrity Program (MIP)
Medicaid Integrity Program Not RAC: Rules, Players, Look-Back & Appeals Differ
MIG’s – Medicaid Integrity Group – established by CMS in July 2006 to implement MIP
MICs are Medicaid Integrity Contractors MIC’s are paid contract fee, no contingency fees Focus on overpayments, no underpayments No limit to record requests, no copying costs Works in concert with State Medicaid Agencies and State Law Enforcement Look-back period mirrors state standards
CMS has two broad responsibilities under the Medicaid Integrity Program: To hire contractors to review Medicaid provider activities, audit claims, identify
overpayments, and educate providers and others on Medicaid program integrity issues
To provide effective support and assistance to States in their efforts to combat Medicaid provider fraud and abuse

4
Medicaid Integrity Program (MIP)
Medicaid Integrity Program Involves Three Medicaid Integrity Contractors
Review, Audit & Education Annual Report to Congress Required Review MIC Works with CMS & Audit MICs
Analyzes Paid Claims Data, No pre-pay reviews No direct provider contact

5
Review MICs
Review Contractors Identifies “Aberrant” Claims, High-risk area and Potential
Vulnerabilities CMS: “Data driven approach ensures focused efforts” States can also recommend targets
Recommends leads & Provider targets to CMS and Audit MICs
Works with States & Feds to avoid duplicate audits

6
Review MICs
Who are the Review Medicaid Integrity Contractors?
-- AdvanceMed (OH)-- Thomson Reuters (KY, VA, WV)

7
Audit MICs
Audit MICs Conducts Post-pay Audits of Medicaid Providers
FAFAS Standards (“yellow book”) Audits performed by “appropriate & qualified” professionals: physician
medical directors & RN reviewers Could involve medical record, bill data and other (?) provider records
Identifies Overpayments Can extrapolate sample reviews
Works with CMS MIG & state Medicaid offices to finalize results State Medicaid agencies that normally collect payments will recover
these payments as well Audit MIC reports can be shared with Federal or State Law Enforcement
Agencies
8
Audit MICs
Audit MICs Effective 10/26/09 - Health Integrity LLC
(formerly Booz Allen Hamilton)– (KY, VA, OH & WV)
9
Education MICs
Education MICs Works with CMS & Other MICs to Prevent Future Medicaid Fraud,
Waste & Abuse Interacts with all Medicaid Stakeholders
Providers Medicaid Agencies Medicare FI/MAC State & Federal Law Enforcement/State Auditor
Develops Training Materials, Awareness Campaigns & Conducts Provider Education
10
Education MICs
Education MICs Information experts Strategic Health Solutions confirmed for WV
11
NY State Inspector General – Jim Sheehan Comments
NY State IG Jim Sheehan provided some areas that providers can anticipate being audited by MICs:
Dead or alive – was patient alive at date service was rendered? IP at time of ambulatory service – IP’s at a hospital at the time home
health care or ambulance trips Hysterectomy on males Debridement requiring actual cutting Heart failure and shock – ambulatory surgery with no complication to
justify the IP stay Observation beds – popular because Medicaid rules differ by state and
differ from Medicare in most states Hiring excluded individuals – lack of thorough screening
12
Office of the Medicaid Inspector General – NY Free Stuff
Website – www.OMIG.State.NY.us Mandatory Compliance Program – hospitals, managed care, all
providers over $500,000/year Over 1300 provider audit reports detailing findings in specific
industry 66 Page work plan issued 4/20/09 – shared with other states, CMS,
OIG – new one due out this month! Listserv – put your name in, get email updates Updates on MIC, IPRO & Thomson Reuters NY Excluded Provider List.
13
How Does MIP Work?
1.CMS & Review MIC Identify Potential Projects/Targets2. CMS & Review MIC Outline Projects/Targets with State Medicaid, FI/MAC & State Agencies to avoid duplication3. Review MICs analyze Medicaid claims data to identify providers with potential overpayments. From the resulting lists of providers, CMS selects audit targets to assign to Audit MICs. 4. CMS forwards approved projects/targets to Audit MIC5. Audit MIC Notifies Provider Contact
At least two-week notice with list of accounts; extensions granted upon request for large projects – Expect no more than 45 days
Patient identifying data is limited (Medicaid SSI # & DOS) Audits will most often be done off-site – records required to be readied and available
accordingly – no copying costs Audit MIC will outline details in “entrance conference”

14
How Does MIP Work?
6. Audit MIC Performs Audit According to GAGAS7. Audit MIC Holds Exit Conference
Provider has chance to provide additional information8. Audit MIC Shares Draft Report with Provider, CMS & State)
Provider & State have chance to review and comment9. CMS Finalizes Report, Settles any differences and Determines Amount of
Overpayment10. CMS Issues Final Report to State and triggers 60 (calendar) day repayment
timeline11.State Issues Final Report to Provider
State handles appeals according to its rules State Recoups Overpayments according to its process
15
WV – BMS Office of Quality Program Integrity Director of Program Integrity – Tammy Hypes “MIP is still a work in progress” Spoke with Tammy Hypes 3/15 and she stated that the MIC
is not their focus at the moment. Other states have kicked off their MIC programs They are currently working with Health Integrity on behind
the scenes work such as getting their data aligned to prepare to perform data mining.

16
MIC Audits
Common areas under scrutiny: One day stays Provider eligibility Billing for services not provided Reimbursements for unapproved drugs Duplicate billing Providing services not medically necessary Providing services that may compromise the quality of care Excessive payments and “upcoding” for higher reimbursement of billed procedures Billing for services provided by unlicensed or untrained personnel Payments for unapproved transportation services Medicaid eligibility in multiple states Contingency fee payments to consultants and service providers Providing false certifications in the claims process
17
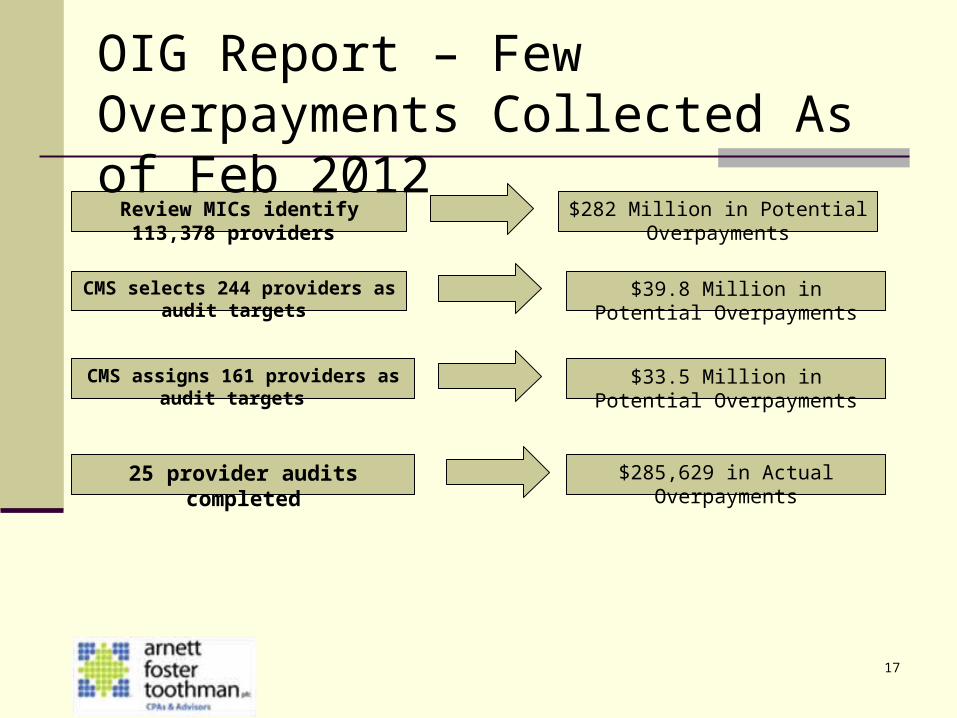
Review MICs identify 113,378 providers $282 Million in Potential Overpayments
CMS selects 244 providers as audit targets $39.8 Million in Potential Overpayments
CMS assigns 161 providers as audit targets $33.5 Million in Potential Overpayments
25 provider audits completed $285,629 in Actual Overpayments
OIG Report – Few Overpayments Collected As of Feb 2012

18
Medicaid Integrity Program
http://www.cms.hhs.gov/MedicaidIntegrityProgram
http://www.cms.hhs.gov/ProviderAudits/Downloads/mipfactsheet.pdf

19
Medicaid RAC
The Affordable Care Act (ACA) requires Medicaid agencies to contract with Recovery Audit Contractors (RACs) to identify and recover overpayments and to identify underpayments.
States must also develop processes for entities to appeal RAC determinations, and coordinate RAC efforts with other Federal and state law enforcement agencies.
Most states have begun to develop comprehensive Medicaid RAC solutions to meet ACA requirements.
20
Medicaid RAC
West Virginia State Plan Amendment (SPA) Submitted 1/4/2011 SPA Approved 3/28/2011 The state is not seeking any exemptions from RAC audit scope A RAC RFP was issued in May 2012, with a response due date in July
2012. Claim types to be audited under the RFP scope are limited to medical, dental, and DME.
In September 2012, the state awarded the RAC contract covering medical, dental, and DME claims to HMS
A separate RAC RFP focusing exclusively on pharmacy claims was issued June 2012, and had a proposal due date of August 9; this pharmacy-only RAC RFP was subsequently canceled and will be re-bid
21
Medicaid RAC
Ohio SPA Submitted 12/22/2010 SPA Approved 3/22/2011 The state is not seeking any exemptions from RAC
audit scope A RAC RFP was issued January 2011 and closed
March 2011; RAC scope includes overpayment and underpayment identification, and quality and control of Medicaid services provided.
The RAC contract was awarded to CGI (May 2011)
22
Medicaid RAC
Ten of the most important elements of the rule that states, managed care organizations (MCOs), and other stakeholders should be aware of are:1. The deadline for states to implement their Medicaid RACs is now January 12, 2012. The
final rules are not effective until that time.2. States may exclude MCOs from review by Medicaid RACs, but are not required to do so.3. States must set limits on the number and frequency of medical records to be reviewed by
the Medicaid RACs subject to requests for exceptions made by the RACs.4. States must notify providers of underpayments that are identified by the Medicaid RACs,
and they must adequately incentivize RACs to detect underpayments. Medicare RAC underpayments, which made up 18% of corrections last year, will be used as a benchmark for Medicaid RACs. CMS will also look at the trends among the states.
5. CMS will allow states to establish “regional” Medicaid RACs.

23
Medicaid RAC
6. Medicaid RACs must notify providers of overpayment findings within 60 calendar days.
7. CMS will be developing performance metrics with states to determine the accuracy of RAC reviews.
8. CMS will allow states to determine at what stage of the audit process RACs will receive the contingency fee. States should specify in their RAC contracts the time frame in which the state expects the Medicaid RAC to return the contingency fee in cases in which a determination is reversed at any level of the appeals process.
9. If a state is interested in “bundling” its Medicaid RAC procurement with other services (for example: third party liability) that are currently being performed by an existing contractor, the state must execute a separate task order outlining the requirements of RAC program for the existing contractor.
10. Medicaid RACs are not required to collect overpayments, only to identify them. States have the flexibility to coordinate the collection of overpayments.
24
Medicaid RAC
Per HMS website: We conduct face-to-face meetings and conference calls with hospitals and provider associations, and
individual providers. We work with multiple contacts at your facility to make sure that everyone has a common understanding of the process and objectives.
A 24/7 state-of-the-art web-based portal to help you navigate the overpayment identification and recovery process — without the burden of paper
A full-time Provider Services team to guide you through the audit process. Our team is focused exclusively on responding to your inquiries, and has the experience required to promptly and accurately respond to your questions regarding the review and recovery process.
Regular updates on findings. We regularly participate in state hospital and provider association meetings and publish information about trends and issues identified on our website. We also publish quarterly newsletters and conduct webinars to keep you up to date.
A highly skilled Clinical Review team. Registered nurses, certified coding professionals, and physicians experienced in the review of medical records work together to review claims and make fair determinations based on your state’s policy and regulations.
Guidance on how to correct overpayment errors in the future. Provider education is important to us. Our determination letters include detailed clinical rationales so you’re 100% clear on why a claim is denied, and how to prevent the overpayment on future claims.
25
Medicaid RAC
FAQ: Are state’s required to give providers advance notice about the audit areas on which the Medicaid RAC’s might focus similar to when the Medicare
RAC first started?
Answer: CMS is not requiring states to publicize the audit areas on which their Medicaid RACs will focus. States have a certain degree of flexibility to design their Medicaid RAC programs to meet their specific needs.
However, we believe that states should promote transparency in their RAC programs. Encouraging RACs to give advance notice to providers of audit areas on preparation of review is an example of how states can facilitate transparency.
26
Medicaid RAC
The final rule at 42 CFR § 455.506(e) provides that a state must set limits on the number
and frequency of records to be reviewed by it’s RAC. The state has the flexibility to set the limits.
The final rule at 42 CFR § 455.508(f) specifies that a Medicaid RAC must not review claims that are more than 3 years from the date the claim was filed unless it receives approval from the state
Medicaid RACs operate at the direction of the State. States have the discretion to determine
what areas of their Medicaid program to target based on the program integrity landscape in the State.
States should provide the Medicaid RACs with the most accurate data available in order to ensure the most accurate audit results.
CMS expects States to work with their Medicaid RACs to identify vulnerabilities within each State’s Medicaid Program.
27
Medicaid RAC
Molina will present general workshops during April, 2013. Various contractors will be at the meetings to present on various topics including
Medicaid RAC, Appeal and Reconsideration processes PERM, Re-enrollment
Invites for these workshops have not gone out yet as of Friday March 15. Check your inbox and/or find it in your organization and sign up!
All services covered by Medicaid are available for the RAC to review.
WV – won’t put any information out on any websites until they are sure they will focus on it.
New False Claims Review Criteria for States – March 15, 2013:https://oig.hhs.gov/fraud/docs/falseclaimsact/guidelines-sfca.pdf

28
Medicaid RAC – Locations for Workshops
LOCATION DATE TIME
Martinsburg – April 15, 2013 9:00 am – 1:00 pmHoliday Inn
Morgantown – April 16, 2013 9:00 am – 1:00 pmWaterfront Hotel
Wheeling – April 17, 2013 9:00 am – 1:00 pmOglebay Park Pine Room
Flatwoods – April 22, 2013 9:00 am – 1:00 pmDays Inn Hotel
LOCATION DATE TIME
Huntington – April 23, 2013 9:00 am – 1:00 pmBig Sandy Arena Beckley – April 24, 2013 9:00 am – 1:00 pmTamarack Charleston– April 25, 2013 9:00 am – 1:00 pmMarriott Town Center – Pavilion

29
Medicaid RAC
Areas most likely to be targeted: Medical necessity claims DME claims Units of therapy claims Cardiac claims Other high dollar claims Drug units
30
Medicaid RAC
What can you do now? Stay on top of the general Medicaid billing rules, not just RACs and appeals Conduct real-time, open chart audits to ensure accurate and compliant documentation It may be beneficial for a provider to have someone on the front end at registration that is
qualifying and screening potential Medicaid recipients Measurement of accuracy and exchange of information are important for long-term success and
accountability Ensure processes are in place for real time management of the bed placement and
appropriate documentation are crucial to getting the rules right on the front end There must be some type of structure that brings together the finance, clinical, and
utilization review functions All roles related to billing compliance should serve on the billing/compliance RAC
committee or any other type of centralized committee. Basically this will be utilizing current processes for Medicare RAC but be sure to have a
process in place to keep the requests and responses separate.