1 Management of anti retroviral treatment in patients with cirrhosis Dominique Salmon Cochin...
36
1 Management of anti retroviral treatment in patients with cirrhosis Dominique Salmon Cochin Hospital June 23, 2006
-
Upload
buddy-bradley -
Category
Documents
-
view
215 -
download
0
Transcript of 1 Management of anti retroviral treatment in patients with cirrhosis Dominique Salmon Cochin...

1
Management of anti retroviral treatment in patients with cirrhosis
Dominique Salmon
Cochin Hospital
June 23, 2006

2
Background
• Beneficial impact of ARV on liver disease morbidity and mortality
• Hepatotoxicity more frequent in severe liver disease
• ARV clearance impaired in patients with severe liver disease
• Correlation between toxicity and plasma concentrations for some ARV
=> Specificity of ARV use in cirrhosis
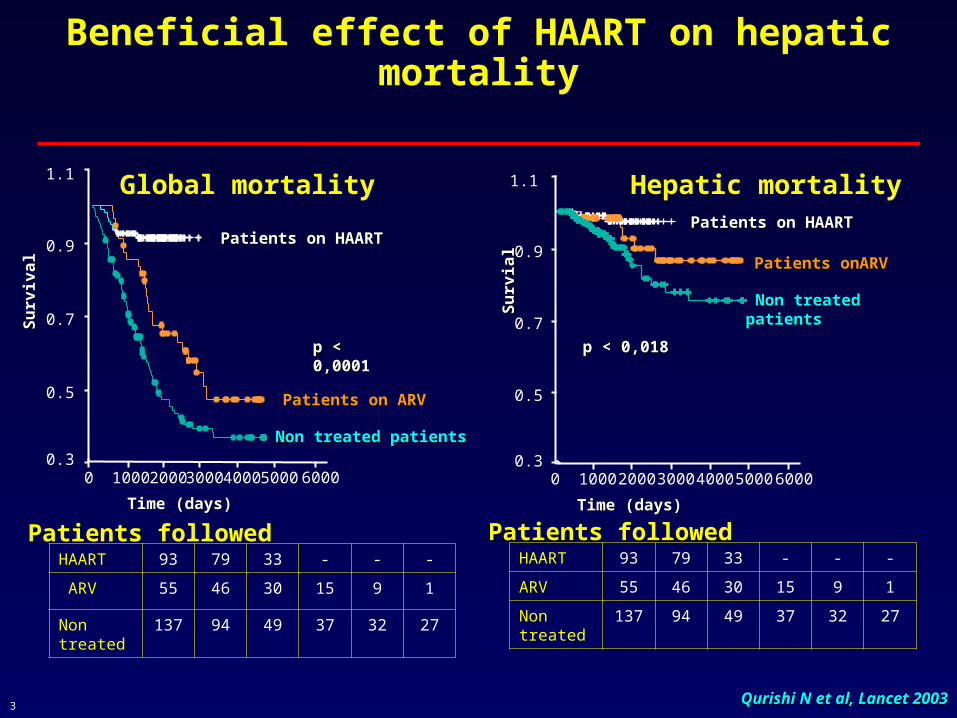
3 Qurishi N et al, Lancet 2003Qurishi N et al, Lancet 2003
Time (days)Time (days)
500040003000200010000
Su
rviv
al
Su
rviv
al
1.1
0.9
0.7
0.5
0.3
p < 0,0001p < 0,0001
Patients on HAARTPatients on HAART
Patients on ARVPatients on ARV
Non treated patientsNon treated patients
6000 6000500040003000200010000
1.1
0.9
0.7
0.5
0.3
p < 0,018p < 0,018
Patients on HAARTPatients on HAART
Patients onARVPatients onARV
Non treated patientsNon treated patientsSu
rvia
lS
urv
ial
Time (days)Time (days)
HAART 93 79 33 - - -
ARV 55 46 30 15 9 1
Non treated
137 94 49 37 32 27
Patients followedPatients followedHAART 93 79 33 - - -
ARV 55 46 30 15 9 1
Non treated
137 94 49 37 32 27
Patients followedPatients followed
Beneficial effect of HAART on hepatic mortality
Global mortality Hepatic mortality
4
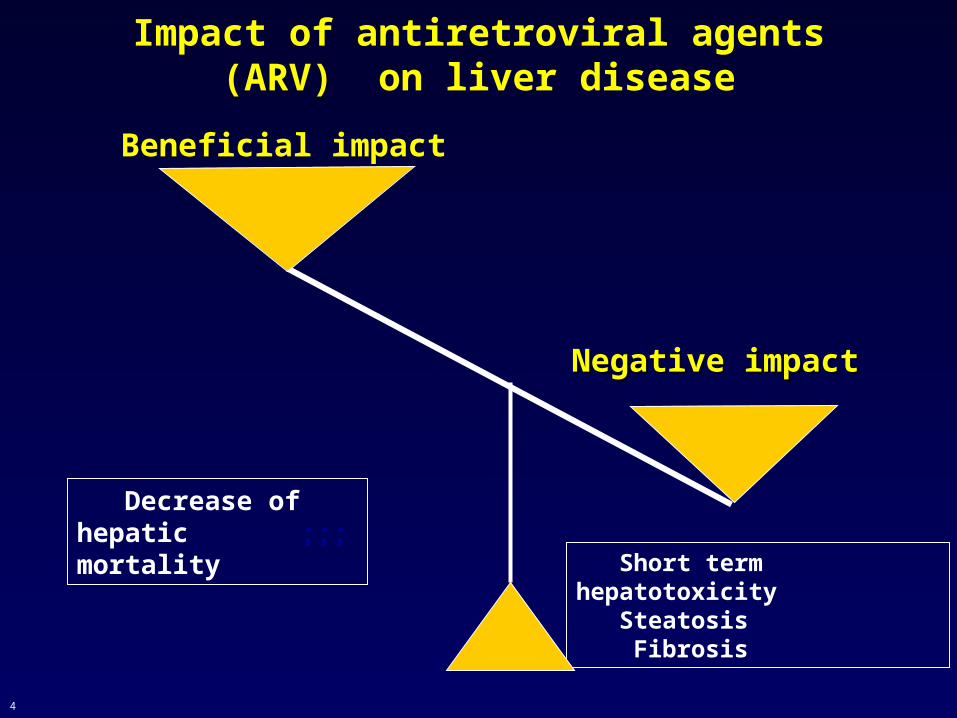
Negative impactNegative impact
Beneficial impact
Short term hepatotoxicity Steatosis Fibrosis
Decrease of hepatic ;;;mortality
Impact of antiretroviral agents (ARV) on liver disease
5
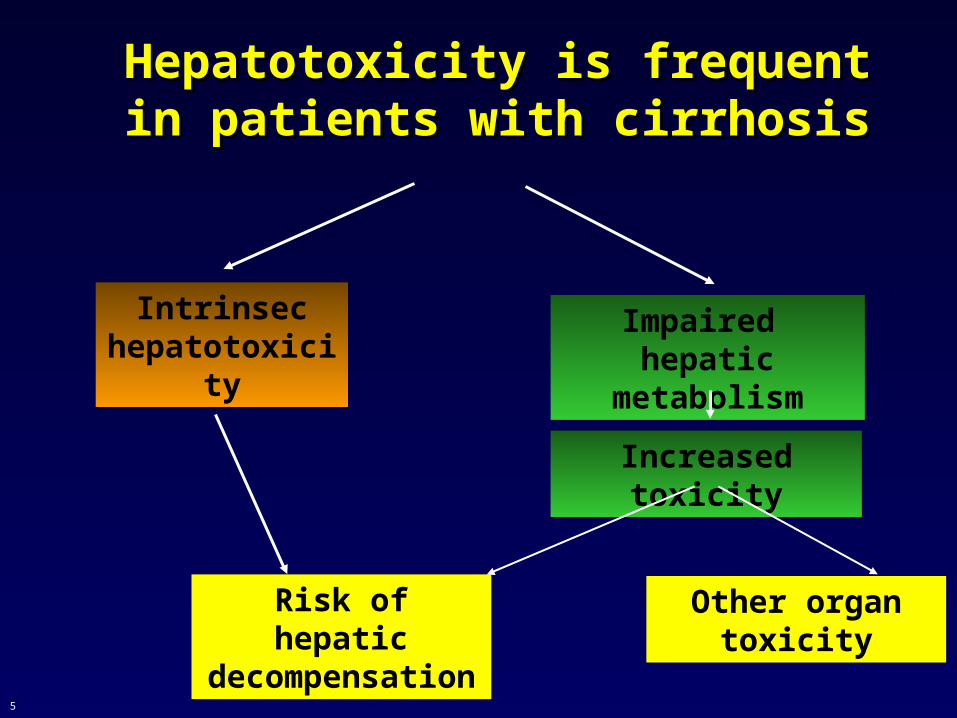
Hepatotoxicity is frequent in Hepatotoxicity is frequent in patients with cirrhosispatients with cirrhosis
Intrinsec hepatotoxicity
Impaired hepatic metabolism
Risk of hepatic decompensation
Increased toxicity
Other organ toxicity
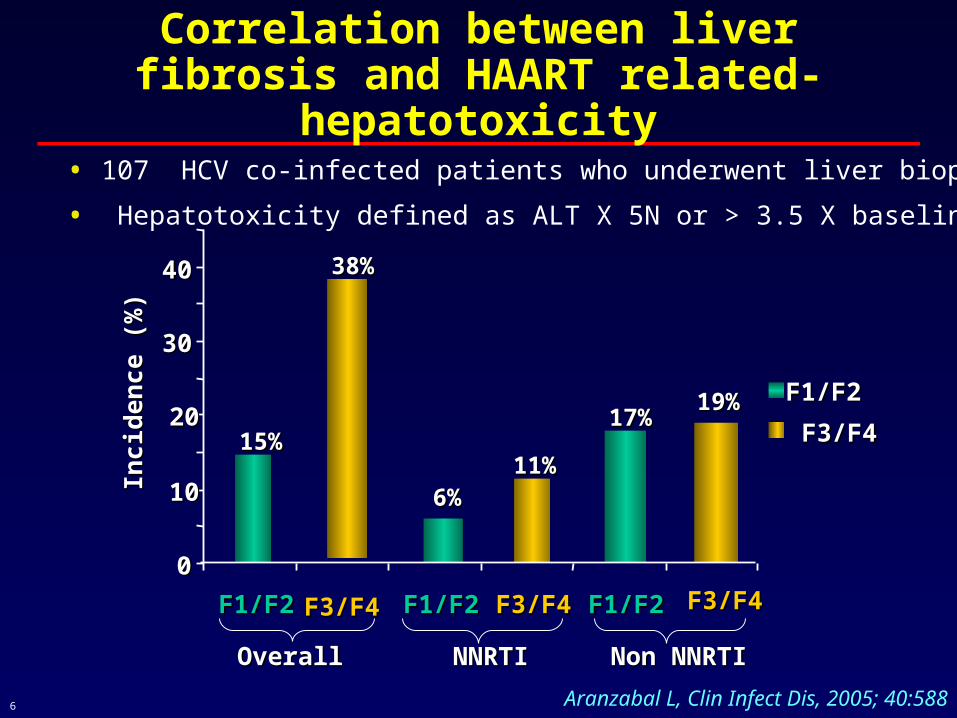
6 Aranzabal L, Clin Infect Dis, 2005; 40:588
15%15%
38%38%
6%6%11%11%
17%17%19%19%
00
1010
2020
3030
4040
F1/F2F1/F2 F1/F2F1/F2 F3/F4F3/F4 F1/F2F1/F2
Inci
den
ce (
%)
Inci
den
ce (
%)
F1/F2F1/F2
OverallOverall NNRTINNRTI Non NNRTINon NNRTI
Correlation between liver fibrosis and HAART related-hepatotoxicity
F3/F4F3/F4 F3/F4F3/F4
• 107 HCV co-infected patients who underwent liver biopsy
• Hepatotoxicity defined as ALT X 5N or > 3.5 X baseline
F3/F4F3/F4
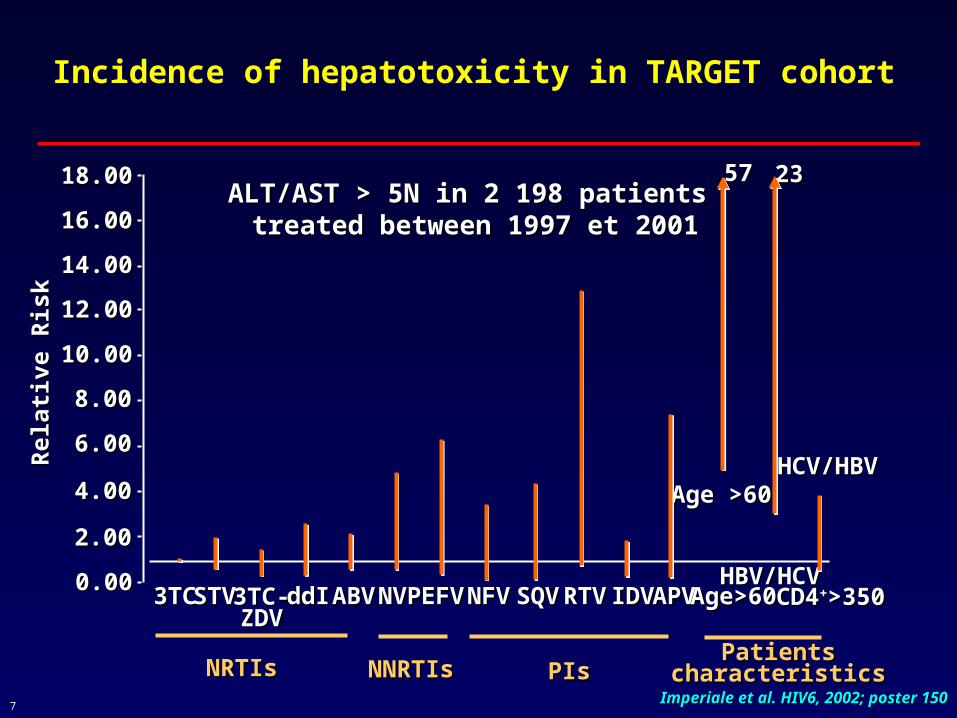
7 Imperiale et al. HIV6, 2002; poster 150Imperiale et al. HIV6, 2002; poster 150
ALT/AST > 5N in 2 198 patients ALT/AST > 5N in 2 198 patients treated between 1997 et 2001treated between 1997 et 2001
18.0018.00
16.0016.00
14.0014.00
12.0012.00
10.0010.00
8.008.00
6.006.00
4.004.00
2.002.00
0.000.00
Rel
ativ
e R
isk
Rel
ativ
e R
isk
3TC3TC STVSTV 3TC-3TC-ZDVZDV
ddIddI ABVABV NVPNVP EFVEFV NFVNFV SQVSQV RTVRTV IDVIDV APVAPV Age>60Age>60 CD4CD4++>350>350HBV/HCVHBV/HCV
HCV/HBVHCV/HBVAge >60Age >60
23235757
NRTIsNRTIs NNRTIsNNRTIs PIsPIsPatientsPatients
characteristicscharacteristics
Incidence of hepatotoxicity in TARGET cohort

8
Steatosis and HIV/HCV co-infection
• Frequent :
- 40 to 67 % of the patients
- Severe in 7 %
- Microvesicular
- Macrovesicular
Sulkowsky, AIDS, 2005; BaniSadr, AIDS 2006; Castéra et al., Lemoine et al., Marks et al, Agarwal et al, Sulkowsky, AIDS, 2005; BaniSadr, AIDS 2006; Castéra et al., Lemoine et al., Marks et al, Agarwal et al, AASLD, 2004AASLD, 2004

9
Risk factors of steatosis in HIV/HCV co-infection
• BMI
• Genotype 3
• Caucasian race
• Fibrosis score
• Hyperglycemia/insulin resistance
• Lipodystrophy
• D4T use
• Cumulative time on PI
(1) Castera, 2004; (2) Sulkowski, 2005; (3) Bani-Sadr, 2006
Role of HAART
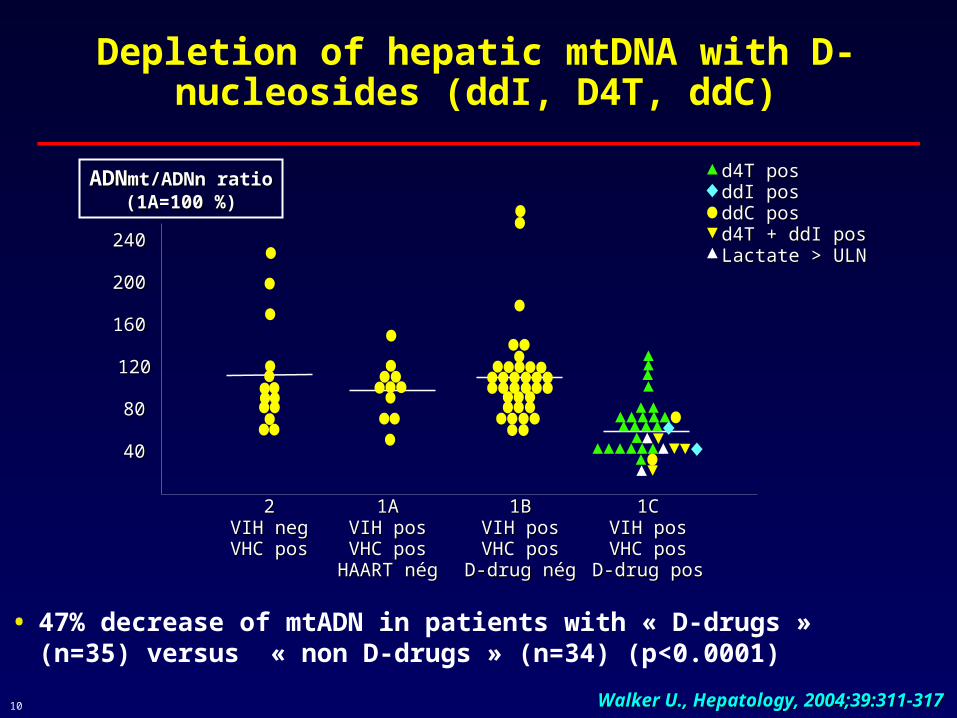
10
Depletion of hepatic mtDNA with D-nucleosides (ddI, D4T, ddC)
• 47% decrease of mtADN in patients with « D-drugs » (n=35) versus « non D-drugs » (n=34) (p<0.0001)
240240
200200
160160
120120
8080
4040
22VIH negVIH negVHC posVHC pos
1A1AVIH posVIH posVHC posVHC pos
HAART négHAART nég
1B1BVIH posVIH posVHC posVHC pos
D-drug négD-drug nég
1C1CVIH posVIH posVHC posVHC pos
D-drug posD-drug pos
ADNADNmt/ADNn ratiomt/ADNn ratio(1A=100 %)(1A=100 %)
d4T posd4T posddI posddI posddC posddC posd4T + ddI posd4T + ddI posLactate > ULNLactate > ULN
Walker U., Hepatology, 2004;39:311-317Walker U., Hepatology, 2004;39:311-317
11
Pharmacokinetics of ARV in cirrhotic
patients

12
Impaired hepatic metabolism in cirrhosis
protein synthesis => increase of free form
hepatic metabolism (CYP 450, UGP..)
hepatic flow => decrease hepatic clearance
Increase of C max, AUC

13
Protease inhibitors
14
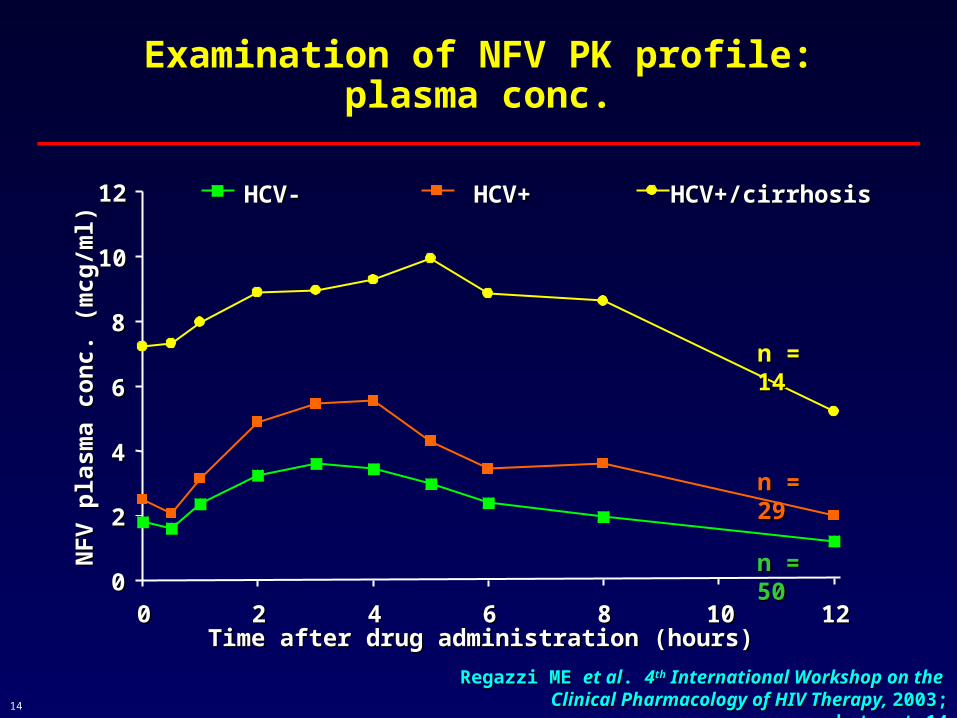
Examination of NFV PK profile:plasma conc.
Regazzi ME Regazzi ME et alet al. . 44thth International Workshop on the International Workshop on the Clinical Pharmacology of HIV Therapy, Clinical Pharmacology of HIV Therapy, 2003; abstract 2003; abstract
1414
00
22
44
66
88
1010
1212
00 22 44 66 88 1010 1212Time after drug administration (hours)Time after drug administration (hours)
NF
V p
lasm
a co
nc.
(m
cg/m
l)N
FV
pla
sma
con
c. (
mcg
/ml)
HCV-HCV- HCV+HCV+ HCV+/cirrhosisHCV+/cirrhosis
n = 14n = 14
n = 29n = 29
n = 50n = 50

15
Lopinavir Total and Unbound AUC12, Individual and Mean ± SD,
Study Day 14L
op
inav
ir A
UC
12 ( g
•h/m
L)
0
50
100
150
200
250
Un
bo
un
d L
op
inav
ir A
UC
12 ( g
•hr/
mL
)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Control Mild+Moderate
Control
Mild HI
Moderate HI
Control Mild+ModerateTotal LPV Unbound LPV
Arribas et al.; EACS 2003, #F2/6
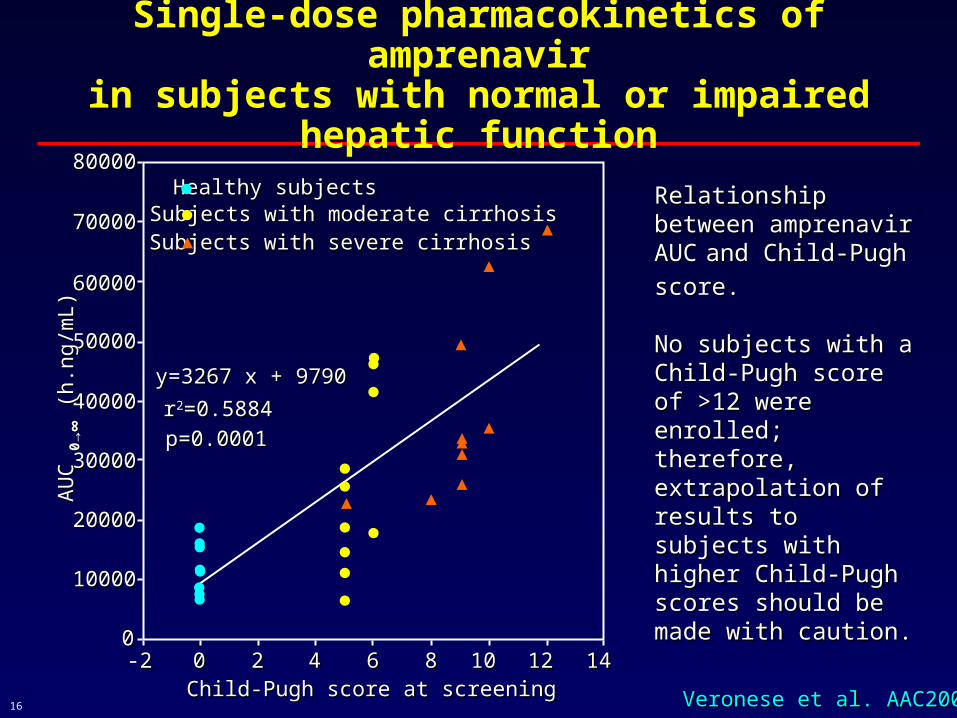
16 Veronese et al. AAC2000Veronese et al. AAC2000
Relationship between Relationship between amprenavir AUCamprenavir AUC
and and
Child-Pugh score. Child-Pugh score.
No subjects with a Child-No subjects with a Child-Pugh score of >12 were Pugh score of >12 were enrolled; therefore, enrolled; therefore, extrapolation of results to extrapolation of results to subjects with higher subjects with higher Child-Pugh scores Child-Pugh scores should be made with should be made with caution.caution.
8000080000
7000070000
6000060000
5000050000
4000040000
3000030000
2000020000
1000010000
00-2-2 00 22 44 66 88 1010 1212 1414
Child-Pugh score at screeningChild-Pugh score at screening
AU
C
AU
C 00 →
∞→
∞ (
h.ng
/mL)
(h.
ng/m
L)
Healthy subjects Healthy subjects Subjects with moderate cirrhosisSubjects with moderate cirrhosisSubjects with severe cirrhosisSubjects with severe cirrhosis
y=3267 x + 9790y=3267 x + 9790
rr22=0.5884=0.5884
p=0.0001p=0.0001
●●●●●●●●
●
●●●●
●●
●
●●
●
▲▲ ▲
▲▲▲
▲
▲
▲
▲▲
●
Single-dose pharmacokinetics of amprenavirin subjects with normal or impaired
hepatic function
17
Normal hepatic function Normal hepatic function 1,200 mg BID1,200 mg BID
Child-Pugh scores 5 - 8 Child-Pugh scores 5 - 8 450 mg BID450 mg BID
Child-Pugh scores 9 - 14 Child-Pugh scores 9 - 14 300 mg BID300 mg BID
Veronese et al. AAC2000Veronese et al. AAC2000
Single-dose pharmacokinetics of amprenavirin subjects with normal or impaired
hepatic function
18
NNRTI
19
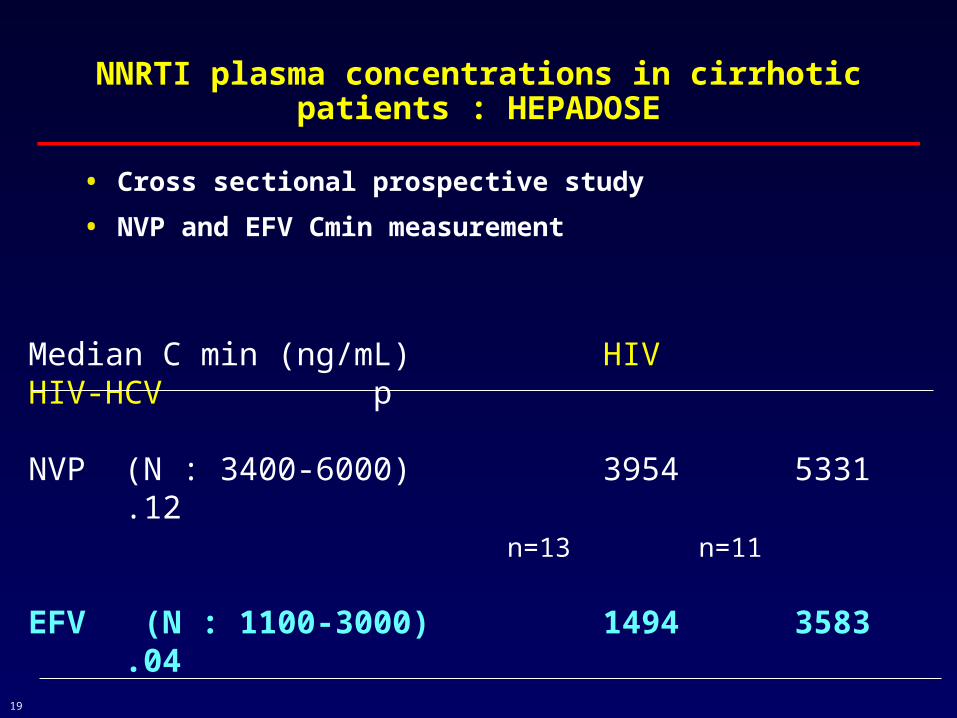
NNRTI plasma concentrations in cirrhotic patients : HEPADOSE
• Cross sectional prospective study
• NVP and EFV Cmin measurement
Median C min (ng/mL) HIV HIV-HCV p
NVP (N : 3400-6000) 3954 5331 .12 n=13 n=11
EFV (N : 1100-3000) 1494 3583 .04
n=8 n=12
20
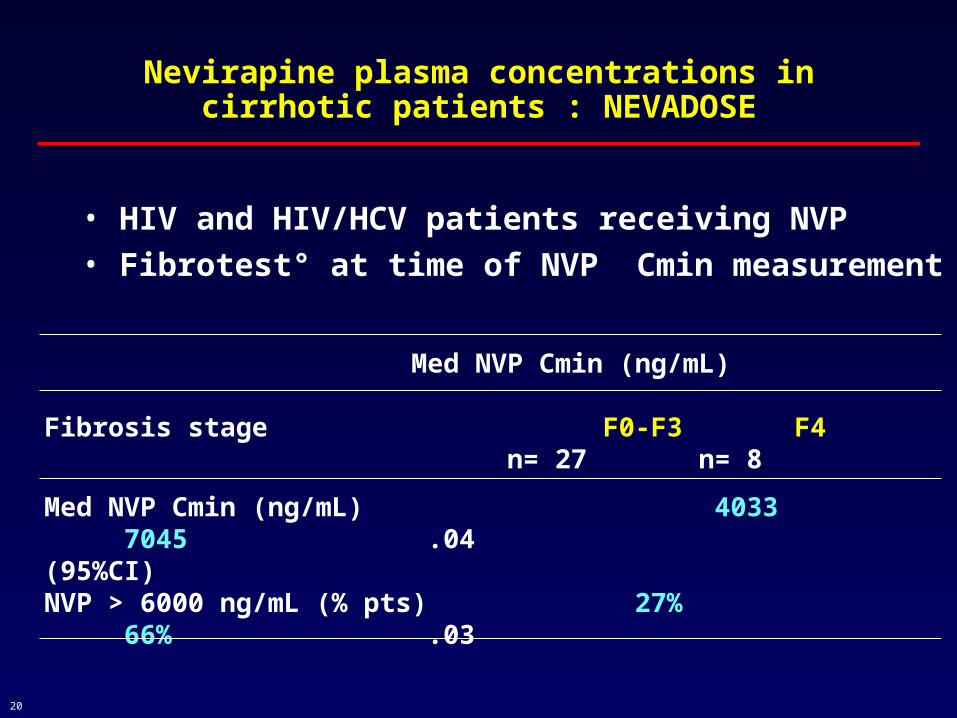
Nevirapine plasma concentrations in cirrhotic patients : NEVADOSE
Med NVP Cmin (ng/mL) 4033 7045 .04 (95%CI) NVP > 6000 ng/mL (% pts) 27% 66% .03
• HIV and HIV/HCV patients receiving NVP• Fibrotest° at time of NVP Cmin measurement
Med NVP Cmin (ng/mL) Fibrosis stage F0-F3 F4
n= 27 n= 8

21
NRTI = few datas
22
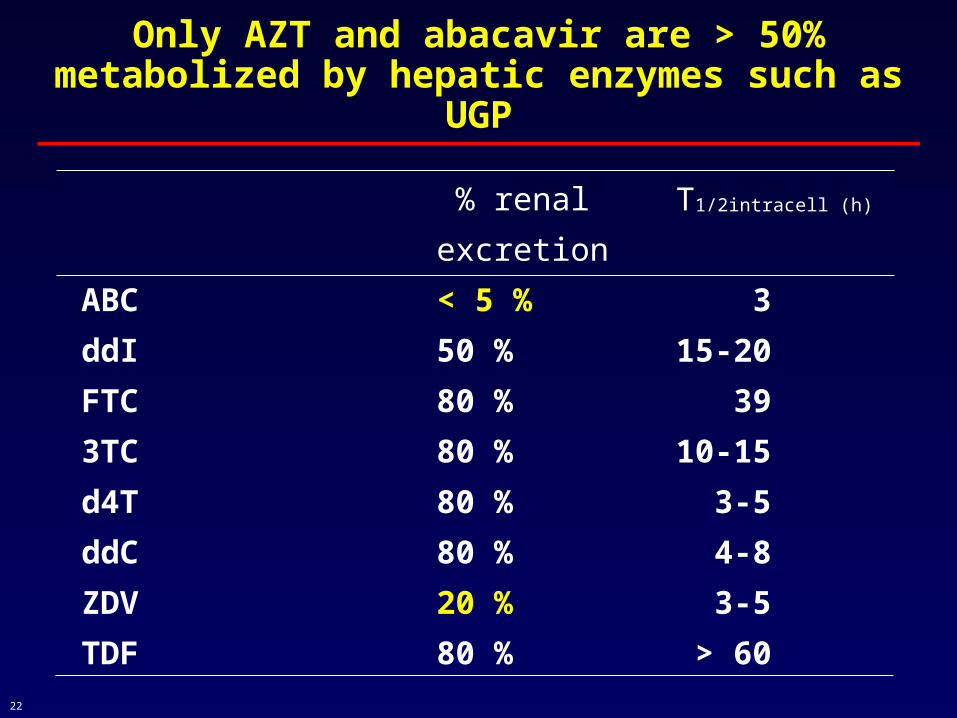
Only AZT and abacavir are > 50% metabolized by hepatic enzymes such as UGP
% renal T1/2intracell (h)
excretion
ABC < 5 % 3
ddI 50 % 15-20
FTC 80 % 39
3TC 80 % 10-15
d4T 80 % 3-5
ddC 80 % 4-8
ZDV 20 % 3-5
TDF 80 % > 60

23
Zidovudine pharmacokinetics in patients with liver cirrhosis
Clearances
ml/min
Clo Clfgzdv
Healthy 2562 ± 813 1540 ± 540
Cirrhosis 686 ± 243** 236 ± 73**
Clo
-ml/m
in/k
gC
lo-m
l/min
/kg
Child-Pugh scoresChild-Pugh scores
00
1010
2020
3030
4040
5050
6060
7070
HH 66 77 88 99 1010 1111 1212 1313
CirrhosisCirrhosis healthyhealthy
Taburet et al., CPT 1990 ; 47 : 731Taburet et al., CPT 1990 ; 47 : 731
24
Abacavir pharmacokinetics in patients with liver cirrhosis
• Single oral dose of 600 mg abacavir
• 9 HIV+ subjects with mild cirrhosis (Child Pugh score 5-6) were compared to 9 controls
• 89% in abacavir AUC
• 59% in abacavir T1/2 (p<0.0001)
• => Dose reduction to 150mg/d recommended in patients with cirrhosis Raffi et al, ICAAC,2004Raffi et al, ICAAC,2004
25
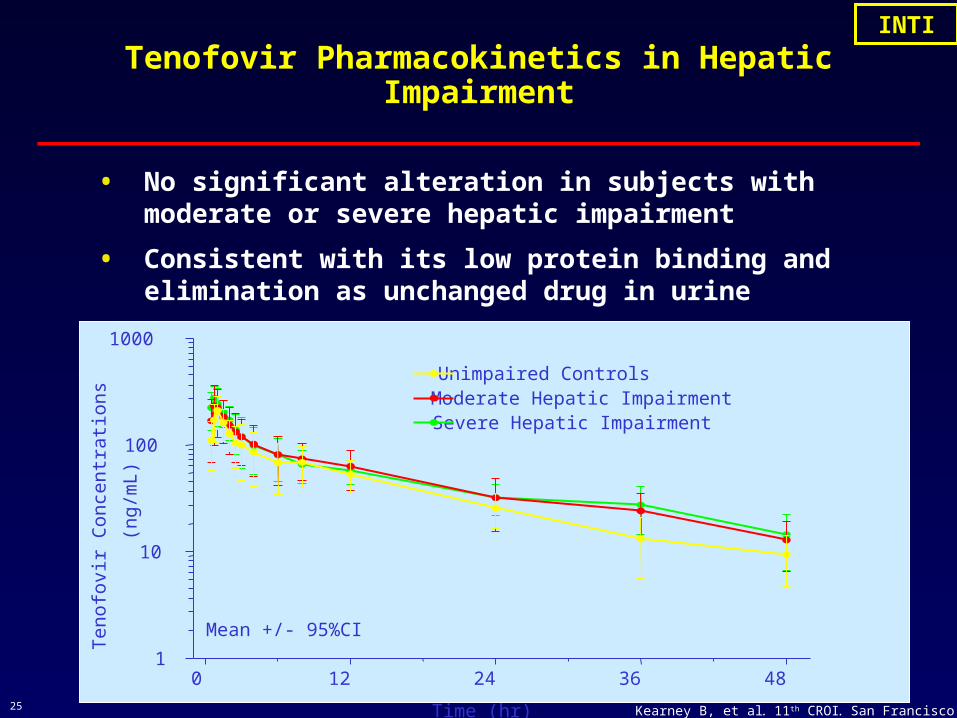
Tenofovir Pharmacokinetics in Hepatic Impairment
• No significant alteration in subjects with moderate or severe hepatic impairment
• Consistent with its low protein binding and elimination as unchanged drug in urine
Kearney B, et al. 11th CROI. San Francisco 2004, #600.
0 12 24 36 481
10
100
1000
Unimpaired ControlsModerate Hepatic ImpairmentSevere Hepatic Impairment
Time (hr)
Ten
ofov
ir C
once
ntr
atio
ns
(ng/
mL)
Mean +/- 95%CI
INTIINTI

26 Peytavin, CROI, 2001Peytavin, CROI, 2001
AE
GI
Nephro
Cut
Metab
AE
Gastrointestinal
Nephrolithiasis
Cutaneous
Metabolic
RTV/IDV (mg bid)
100/400
400/400
100/600
100/800
r2 =0.47r2=0.90
r2 =0.99r2 =0.90
00
500500
10001000
15001500
20002000
00 1010 2020 3030 4040
Adverse Effects (%)Adverse Effects (%)
IDV
Cm
in (
ng
/ml)
IDV
Cm
in (
ng
/ml)
Correlation between plasma Cmin and adverse events : indinavir
27
0
10
20
30
40
50
60
janv-02 D 15 D 38 D47 D45 D60
Stop Efavirenz
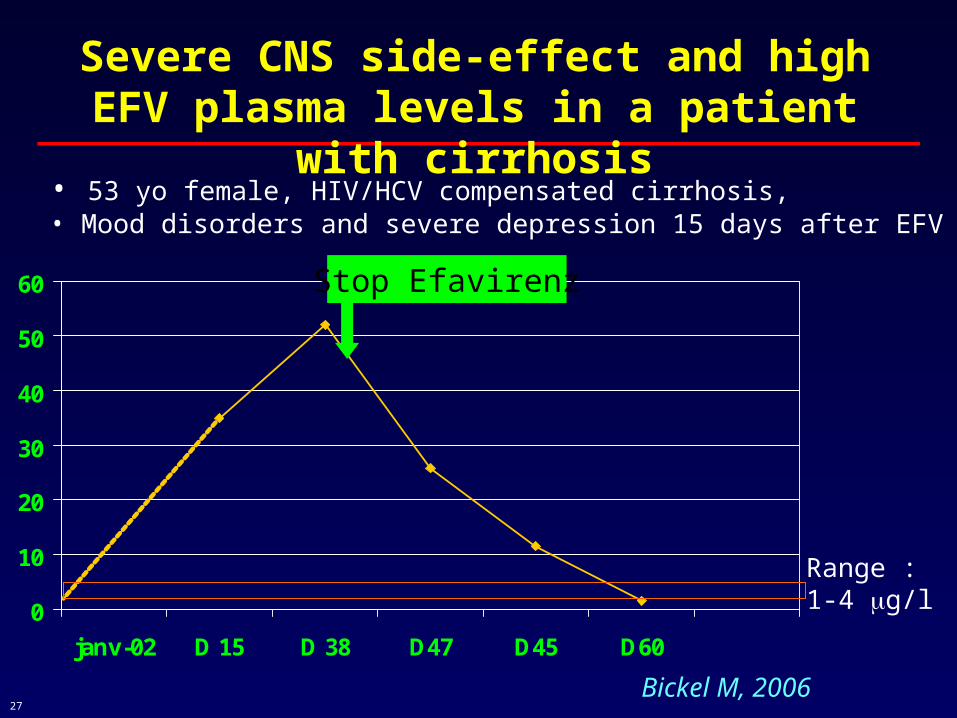
Severe CNS side-effect and high EFV plasma levels in a patient with cirrhosis
Bickel M, 2006
• 53 yo female, HIV/HCV compensated cirrhosis, • Mood disorders and severe depression 15 days after EFV initiation
Range : 1-4 g/l

28
However,
• Major intra and inter individual variability
• Genetic polymorphisms
• Compensatory mechanisms in severe liver disease

29
Conclusion (1)
• ARV are beneficial in patients with cirrhosis
• Normal dosage can be initially prescribed in
patients with moderate hepatic impairement
• Early TDM is warranted in patients with
cirrhosis
- for NNRTI, PI, AZT, abacavir….
- mainly if Child Pugh score > B
30
Conclusion (2)How to prevent steatosis ?
• Select HAART regimen with safe metabolic
• avoid : D4T, ddI, triple NUC regimen
• Select PI such as atazanavir
• Treat metabolic disturbances
• Avoid high BMI
• Treat HCV and HBV

31
Risk factors of steatosis in HIC/HCV co-infectionodds ratio (OR)
Castera, 2004 Sulkowski, 2005 Bani-Sadr , 2006
BMI X 2.8 1.13
Hyperglycemia/insulin resistance
X 2.8
Lypodistropphy X
D4T use
Cumulative time on PI
3.4
1.2
Genotype 3 X 3.2
Caucasian race 4.6
Fibrosis score X 1.43
32
Abacavir and Hepatic Impairment
• Mild hepatic impairment: the data is very limited; due to the potential increases in exposure in some patients, close monitoring is required.
• Moderate: No data are available in patients with moderate or severe hepatic impariment. Plasma concentrations are expected to substantially increase in these patients. Therefore the use of abacavir in patients with moderate hepatic impariment is not recommended unless judged necessary and requires close monitoring of these patients
• Severe: For patients with severe hepatic impairment, Ziagen is contraindicated.
European SmPC: Ziagen
INTIINTI
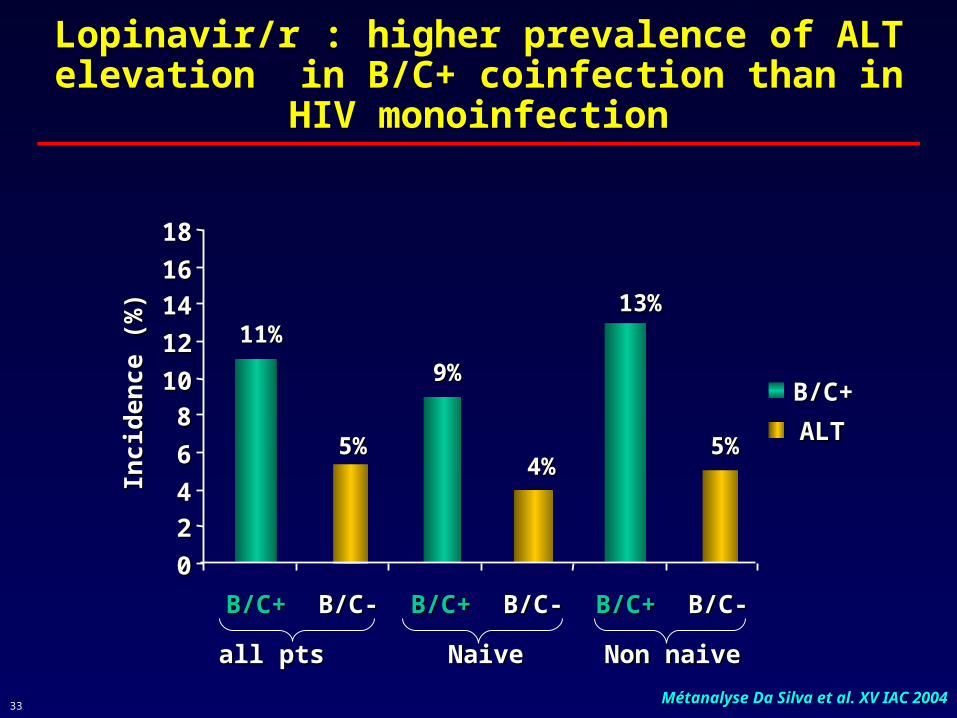
33 Métanalyse Da Silva et al. XV IAC 2004Métanalyse Da Silva et al. XV IAC 2004
11%11%
5%5%
9%9%
4%4%
13%13%
5%5%
00
2244
66
881010
1212
14141616
1818
B/C+B/C+ B/C-B/C- B/C+B/C+ B/C-B/C- B/C+B/C+ B/C-B/C-
Inci
den
ce (
%)
Inci
den
ce (
%)
B/C+B/C+
ALTALT
all ptsall pts NaiveNaive Non naiveNon naive
Lopinavir/r : higher prevalence of ALT elevation in B/C+ coinfection than in HIV monoinfection
34
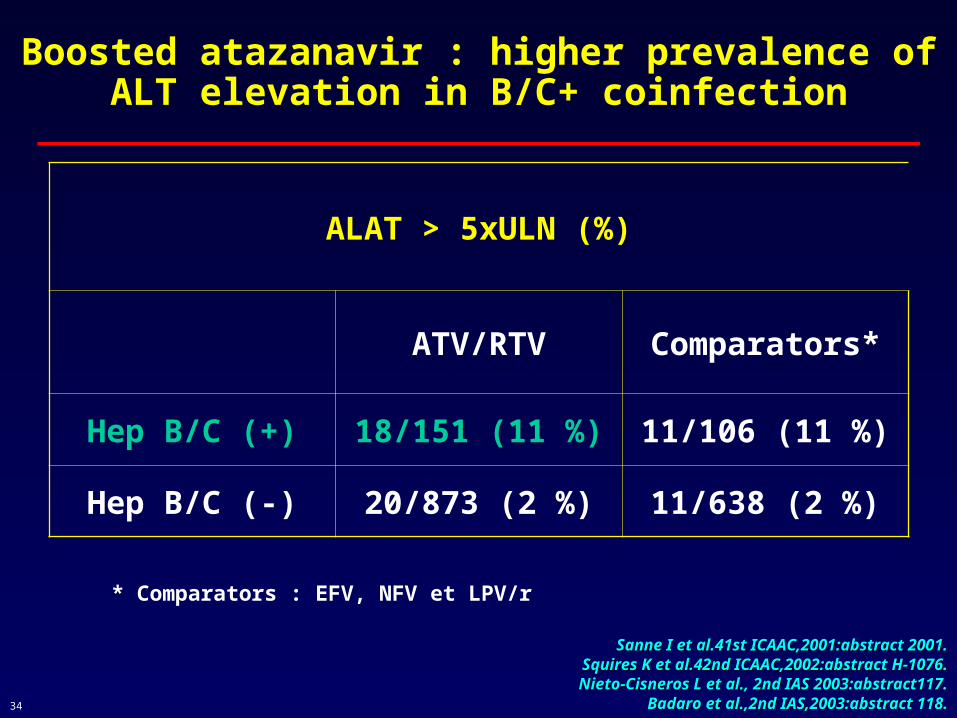
Boosted atazanavir : higher prevalence of ALT elevation in B/C+ coinfection
* Comparators : EFV, NFV et LPV/r
Sanne I et al.41st ICAAC,2001:abstract 2001.Sanne I et al.41st ICAAC,2001:abstract 2001.Squires K et al.42nd ICAAC,2002:abstract H-1076.Squires K et al.42nd ICAAC,2002:abstract H-1076.Nieto-Cisneros L et al., 2nd IAS 2003:abstract117.Nieto-Cisneros L et al., 2nd IAS 2003:abstract117.
Badaro et al.,2nd IAS,2003:abstract 118.Badaro et al.,2nd IAS,2003:abstract 118.
ALAT > 5xULN (%)
ATV/RTV Comparators*
Hep B/C (+) 18/151 (11 %) 11/106 (11 %)
Hep B/C (-) 20/873 (2 %) 11/638 (2 %)
35
1 - Impact of antiretroviral agents (ARV) on liver disease
2 - Pharmacokinetics of ARV in cirrhotic patients
3 - Correlation between high concentrations and toxicity
36
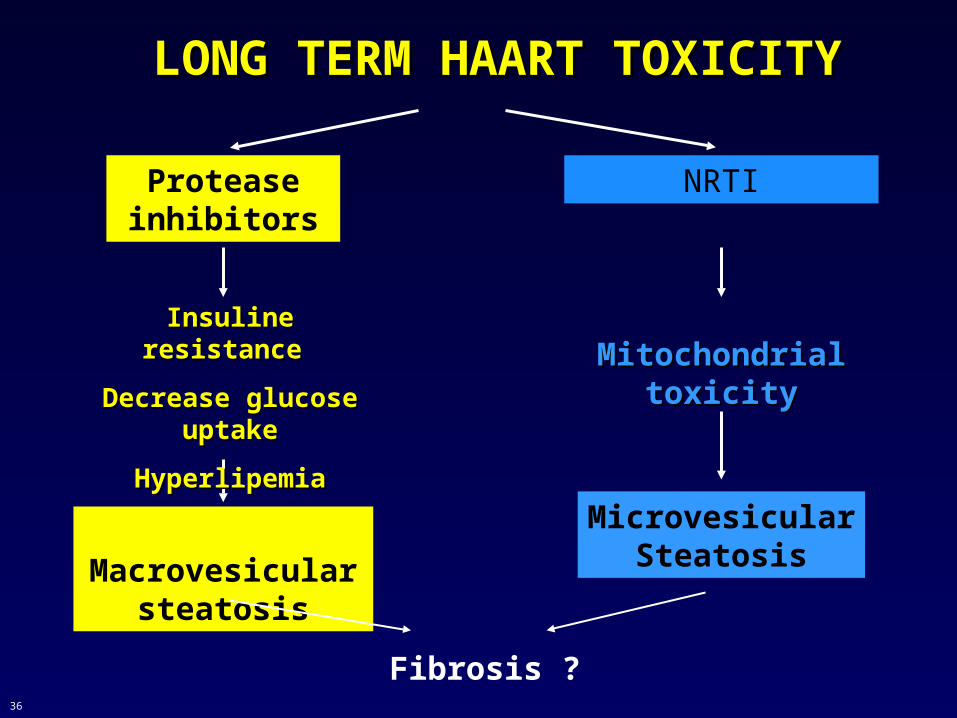
LONG TERM HAART TOXICITYLONG TERM HAART TOXICITY
Protease inhibitors
NRTI
Macrovesicular steatosis
MicrovesicularSteatosis
Fibrosis ?
Insuline resistance Insuline resistance
Decrease glucose Decrease glucose uptakeuptake
HyperlipemiaHyperlipemia
MitochondrialMitochondrialtoxicitytoxicity