1 Intubation and Anatomy of the Airway. 2 3 4 Compression to the cricoid cartilage can be applied...
25
1 Intubation and Anatomy of the Airway
-
Upload
bonnie-lawson -
Category
Documents
-
view
215 -
download
0
Transcript of 1 Intubation and Anatomy of the Airway. 2 3 4 Compression to the cricoid cartilage can be applied...

1
Intubation and Anatomy of the Airway

2

3

4
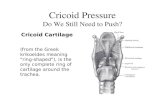
Compression to the cricoid cartilage can be applied in rapid sequence induction in order to compress the esophagus to prevent aspiration in cases of regurgitation but be wary in cases of vomiting as it may cause perforation of the esophagus

5

6

7

For supporting ventilation in patien t with some pathologic disease
: Upper airway obstruction
: Respiratory failure
: Loss of conciousness or a Glasgow coma scale of less then 8

For supporting ventilation durin g general anesthesia
Type of surgery
: Operative site near the airway
: Abdominal or thoracic surgery

: Prone or lateral position
: Long period of surgery
: Patient has risk of pulmonary aspiration
: Difficult mask ventilation

--- : Congenital anomalies > Pierre Robin syndrome , Down’s syndrom
e -- : Infection in airway > Retrophary
ngeal abscess, Epiglottitis : Tumor in oral cavity or larynx
Conditions that are associated with difficult intubation

Enlarge thyroid gland
trachea shift to la teral or compress
ed tracheal lumen
Condition that associated with difficult intubation (con’t)

: Maxillofacial ,cervical or laryngeal trauma : Temperomandibular joint dysfunction : Burn scar at face and neck
: Morbidly obese or pregnancy
Condition that associated with difficult intubation (con’t)

14
is to identify any possible problems with
maintaining, protecting, and providing a patent
airway during anesthesia.
The evaluation is performed with the aid of a
physical examination and a review of the
patients history and previous anesthetic
records.

15
1-2-3’ test is used to asses several factors that may affect decisions concerning the patient’s airway management.
‘1-2-3’ TEST COMPONENTS:
TMJ MOBILITY MOUTH OPENING
THYROMENTAL DISTANCE
1-2-3’ TEST

16
FIRST COMPONENT :ISTEMPOROMANDIBULAR JOINT
(TMJ) MOBILITYIt`s used to identify and restricted
mobility of the temporomandibular joint (TMJ). Ask the patient to sit up with his head in the neutral position and open his mouth as wide as possible.The condyle should rotate forward freely such that the space created between the tragus of the ear and the mandibular condyle is approximately one fingerbreadth in width.
1-2-3’ TEST

17
SECOND COMPONENT :ISMouth Opening and tongue protrusion:
Incisor gap : normal -> more than 3 cms or the patient's mouth should allow at least 2 fingers between the teeth, on the other hand, It will be difficult to insert the laryngoscope blade on less than 2 fingers
1-2-3’ TEST

18
SECOND COMPONENT :ISMouth Opening and tongue protrusion:
With the patient's tongue maximally protruded, the structures visualized should include:
•The pharyngeal arches.• Uvula.• Soft palate.• Hard palate.• Tonsillar beds.• Posterior pharyngeal wall.
Technical difficulties with intubation should be anticipated when only the tongue and soft palate are visualized in a patient during this above maneuver.
1-2-3’ TEST

19
SECOND COMPONENT :ISMouth Opening and tongue protrusion:
Mallampati ClassificationActually, the amount of the posterior pharynx
you can visualize is important and correlates with the difficulty of intubation.
Visualization of the pharynx is obscured by a large tongue (relative to the size of the mouth), which also interferes with visualization of the larynx on laryngoscopy.
1-2-3’ TEST

20
SECOND COMPONENT : MOUTH OPENING AND TONGUE PROTRUSION
Mallampati classification is used to predict the ease of intubation
It is determined by looking at the anatomy of the oral cavity; specifically, it is based on the visibility of the base of uvula, faucial pillars(the arches in front of and behind the tonsils) and soft palate. Some suggest that phonation is best to be used to better asses the mallampati score
Modified Mallampati Scoring is as follows:Class 1: Full visibility of tonsils, uvula and soft palateClass 2: Visibility of hard and soft palate, upper portion of tonsils and uvulaClass 3: Soft and hard palate and base of the uvula are visibleClass 4: Only Hard Palate visible
1-2-3’ TEST

Uvula
Class 3,4 -> may be difficult intubation

- grade 3,4 > risk for difficult intubation
Laryngoscopic view

23

24
THIRD COMPONENT :ISTHE THYROMENTAL
DISTANCE :
It is measured from the lower border of the chin.
Adults who have less than 3 fingerbreadths between their mentum and thyroid notch may have either an anterior larynx or a small mandible, which will make intubation difficult.
1-2-3’ TEST

25
THIRD COMPONENT :ISTHE THYROMENTAL
DISTANCE :Next, evaluate the mobility of the cervical spine.
This is performed by asking the patient to flex and extend their neck. They should be able to perform this without discomfort. Disease of the C-spine (RA, OA, previous injury or surgical fusion) may limit neck extension, which may create difficulties during attempts to intubate. This is certainly true if the atlanto-occipital joint is involved, as restriction of this joints mobility may impair one's ability to visualize the larynx.
1-2-3’ TEST