1-In Vivo Cusp Fracture of Endodontically Treated Premolars Restored With MOD Amalgam or MOD Resin...
5
n vivo cusp fracture of endodontically treated premolars restored with M D amalgam or M D resin fillings E K Hansen Department of Technology Royal Dental College Copenhagen Denmark Hansen EK. n vivo cusp fracture of endodontically treated premolars restored with MOD amalgam or MOD resin fillings. Dent Mater 1988: 4: 169-173. Abstract - The frequency of cusp fracture of endodonticaUy treated premolars was investigated in a retrospective study. After endodontic therapy, the teeth were either restored with a MOD amalgam filling or with an enamel-bonded MOD resin filling. A very high frequency of cusp fracture was found in premolars restored with amalgam: nearly one-third fractured within 3 years after endodontic treatment. The frequency of cusp fracture differed among the 4 amalgam-restored teeth; the lower first premolar had a 15-year survival rate of 74 , in contrast to an average of 32 for the other 3 premolars. No resin- restored premolar fractured during the first 3 years, and the difference between amalgam and resin-restored teeth was highly significant at the 0-3 year interval. However, fracture of resin-restored premolars did happen in the following 3-10 year interval. From a periodontal point of view, a low frequency of cusp fracture carries great weight, and it is therefore concluded that an enamel- bonded resin filling may be a treatment option much preferred to amalgam in temporarily restoring endodontically treated premolars with MOD cavities. Key words: endodontic therapy restorative dentistry amalgam enamel-bonded resin tooth failure. E. Keith Hansen Helsing6rsgade 7 DK-3400 Hiller6d Denmark. Received April 27; accepted Ju ly 24 1987. Endodontic therapy causes a pro- nounced weakening of the tooth and a consequent high risk of cusp or crown fracture. Gher et al. (1) studied the clinical features associated with tooth fracture and found that 71 of the fractured teeth had been endodonti- cally treated. Tooth fracture is a severe problem because the fracture usually extends subgingivally and not infrequently re- sults in loss of periodontal attachment; the fracture may even be so vertical that the tooth has to be extracted. If the tooth can be saved, the main problem for the dentist is both technical and bio- logical in nature, i.e. the technical diffi- culties related to the impression-taking itself and, by impression-taking, the biological risk of further damaging the periodontal tissues (2). Even if the den- tist succeeds in fabricating a well- adapted restoration, the patient may face another problem. Many investiga- tors have reported that subgingivally placed restorations always result in an inflammatory periodontal response (3- 7). As a consequence of this, it has be- come accepted procedure to maintain restoration margins in the supragingival area whenever possible. However, in cases of cusp fracture, one nearly al- ways has to accept a subgingival restor- ation margin and thereby a pronounced possibility of permanent injury to the periodontal tissues. In order to prevent tooth fracture, the optimal restoration of endodonti- cally treated teeth is a full crown or a cast inlay that protects the cusps (8), but many dentists do not find it accept- able to fabricate the final restoration before periapical healing has been con- firmed with radiographs 6-12 months later. However, one of the cusps, or the crown in whole, may actually fracture during this observation period. Still an- other problem is that cast restorations are expensive and quite a few patients cannot afford them. In these cases, the dentist has but two choices: amalgam or com posite resin. This retrospective study was under- taken to examine whether, and to what extent, the use of an enamel-bonded restorative resin in MO D cavities of en- dodontically treated premolars had re- duced the frequency of tooth fracture when compared to endodontically treated premolars restored with a MOD amalgam filling. Material and method s The material was collected from May 1986 to February 1987 from 8 dentists working as general practitioners. The data were derived from clinical exam- inations and review of the patients' dental records and radiographs. The limiting criteria for acceptance of data were the following: (i) an MOD cavity in an endodontically treated pre- molar either restored with amalgam or restored with a composite resin after previous acid-etching of the enamel; (if) no weakening of any of the cusps caused by a Class V restoration; (iii) normal occlusion and articulation; and (iv) complete permanent dentition in the anterior and pre-molar region plus at least one molar in each quadrant in- volved in the occlusion. The following information was recorded: name of the 12 Dental Materials 4:4. 198 8
-
Upload
sara-faris -
Category
Documents
-
view
214 -
download
0
Transcript of 1-In Vivo Cusp Fracture of Endodontically Treated Premolars Restored With MOD Amalgam or MOD Resin...
7/21/2019 1-In Vivo Cusp Fracture of Endodontically Treated Premolars Restored With MOD Amalgam or MOD Resin Fillings
http://slidepdf.com/reader/full/1-in-vivo-cusp-fracture-of-endodontically-treated-premolars-restored-with-mod 1/5
I n v i v o c u s p f r a c t u r e o f
e n d o d o n t ic a l ly t r e a t e d
p r e m o l a r s r e s t o r e d w i t h M 0 Dam algam or M 0D res i n fillin gs
E . K . H a n s e n
Depar tment o f Techno logy, Roya l Denta lCo l lege, Copenhagen, Denmark
H a n s e n E K . In vivo c u s p f ra c t u r e o f e n d o d o n t i c a l l y t r e a t e d p r e m o l a r s r e s t o r e d
w i t h M O D a m a l g a m o r M O D r e s in fi ll in g s . D e n t M a t e r 1 9 88 : 4 : 1 69 - 17 3 .
A b s t r a c t - T h e f r e q u e n c y o f c u sp f r a c tu r e o f e n d o d o n t i c a U y t re a t e d p r e m o l a r s
w a s i n v e s t ig a t e d i n a r e t r o sp e c t i v e s tu d y . A f t e r e n d o d o n t i c t h e r a p y , t h e t e e t h
w e r e e i t h e r r e s t o r e d w i th a M O D a m a l g a m f il li n g o r w i th a n e n a m e l - b o n d e d
M O D r e s in f i ll in g . A v e r y h ig h f r e q u e n c y o f c u sp f r a c t u r e w a s f o u n d i n
p r e m o l a r s r e s t o r e d w i t h a m a l g a m : n e a r l y o n e - t h i r d f r a c t u r e d w i t h in 3 y e a r s
a f t e r e n d o d o n t i c t r e a t m e n t . T h e f r e q u e n c y o f c us p f ra c t u r e d i f f e re d a m o n g t h e
4 a m a l g a m - r e s t o r e d t e e t h ; t h e l o w e r fi rs t p r e m o l a r h a d a 1 5 - y e a r s u r v iv a l r a te
o f 7 4 % , i n c o n t r a s t to a n a v e r a g e o f 32 % f o r th e o t h e r 3 p r e m o l a r s . N o r e si n -
r e s t o r e d p r e m o l a r f r a c t u r e d d u r i n g t h e f i rs t 3 y e a r s , a n d t h e d i f fe r e n c e b e t w e e n
a m a l g a m a n d r e s i n - r e s t o r e d t e e t h w a s h i g h l y s ig n i fi c a n t a t t h e 0 - 3 y e a r i n te r v a l.
H o w e v e r , f r a c t u r e o f re s i n - r e s to r e d p r e m o l a r s d i d h a p p e n i n t h e f o ll o w i n g 3 - 1 0
y e a r i n t e r v a l. F r o m a p e r i o d o n t a l p o i n t o f v i e w , a lo w f r e q u e n c y o f c u sp
f r a c t u re c a r r i e s g r e a t w e i g h t , a n d i t i s t h e r e f o r e c o n c l u d e d t h a t a n e n a m e l -
b o n d e d r e s i n f il li n g m a y b e a t r e a t m e n t o p t i o n m u c h p r e f e r r e d t o a m a l g a m i n
t e m p o r a r i l y r e s t o r in g e n d o d o n t i c a l l y t r e a t e d p r e m o l a r s w i th M O D c a v i ti e s.
Key words: endodont i c therapy, restorative
dentistry, amalgam, enamel-bonded resin, tooth
failure.
E. Kei th Hansen, Helsing6rsgade 7, DK-3400Hi l ler6d, Denmark.
Received Apri l 27; accepted July 24, 1987.
E n d o d o n t i c t h e r a p y c a u s e s a p r o -
n o u n c e d w e a k e n i n g o f t h e t o o t h a n d a
c o n s e q u e n t h i g h r i s k o f c u sp o r c r o w n
f r a c t u r e . G h e r e t a l . ( 1 ) s t u d i e d t h e
c l i n ic a l f e a t u r e s a s s o c i a t e d w i t h t o o t h
f r a c t u re a n d f o u n d t h a t 7 1 % o f t h e
f r a c t u r e d t e e t h h a d b e e n e n d o d o n t i -
c a l l y t r e a t e d .
T o o t h f r a c t u r e i s a s e v e r e p r o b l e m
b e c a u s e t h e f r a c t u r e u s u a l l y e x t e n d s
s u b g i n g i v a l l y a n d n o t i n f r e q u e n t l y r e -
s u l t s i n l o s s o f p e r i o d o n t a l a t t a c h m e n t ;
t h e f r a c t u r e m a y e v e n b e s o v e r t i c a l
t h a t t h e t o o t h h a s t o b e e x t r a c t e d . I f t h e
t o o t h c a n b e s a v e d , t h e m a i n p r o b l e m
f o r t h e d e n t i s t i s b o t h t e c h n i c a l a n d b i o -
l o g i c a l i n n a t u r e , i . e . t h e t e c h n i c a l d i f fi -
c u l ti e s r e l a t e d t o t h e i m p r e s s i o n - t a k i n g
i t se l f a n d , b y i m p r e s s i o n - t a k i n g , t h e
b i o l o g i c a l r i sk o f f u r t h e r d a m a g i n g t h e
p e r i o d o n t a l t is s u e s (2 ) . E v e n i f t h e d e n -
t i s t s u c c e e d s i n f a b r i c a t i n g a w e l l -
a d a p t e d r e s t o r a t i o n , t h e p a t i e n t m a y
f a c e a n o t h e r p r o b l e m . M a n y i n v e s t i g a -
t o r s h a v e r e p o r t e d t h a t s u b g i n g i v a l l y
p l a c e d r e s t o r a t i o n s a l w a y s r e s u l t i n a n
i n f l a m m a t o r y p e r i o d o n t a l r e s p o n s e ( 3 -
7 ) . A s a c o n s e q u e n c e o f t h i s , i t h a s b e -
c o m e a c c e p t e d p r o c e d u r e t o m a i n t a i n
r e s t o r a t i o n m a r g i n s i n t h e s u p r a g i n g i v a l
a r e a w h e n e v e r p o s s ib l e . H o w e v e r , i n
c a s e s o f c u s p f r a c t u r e , o n e n e a r l y a l -
w a y s h a s t o a c c e p t a s u b g i n g i v a l r e s t o r -
a t io n m a r g i n a n d t h e r e b y a p r o n o u n c e d
p o s s i b il i ty o f p e r m a n e n t i n j u r y t o t h e
p e r i o d o n t a l t is s u e s.
I n o r d e r t o p r e v e n t t o o t h f r a c t u r e ,
t h e o p t i m a l r e s to r a t i o n o f e n d o d o n t i -
c a l l y t r e a t e d t e e t h i s a f u ll c r o w n o r a
c a s t i n l a y t h a t p r o t e c t s t h e c u s p s ( 8 ) ,
b u t m a n y d e n t i s ts d o n o t f i n d i t a c c e p t -
a b l e t o f a b r i c a t e t h e f i n a l r e s t o r a t i o n
b e f o r e p e r i a p i c a l h e a l in g h a s b e e n c o n -
f i r m e d w i t h r a d i o g r a p h s 6 - 1 2 m o n t h s
l a t e r. H o w e v e r , o n e o f t h e c u s p s , o r t h e
c r o w n i n w h o l e , m a y a c t u a l l y f ra c t u r e
d u r i n g t h i s o b s e r v a t i o n p e r i o d . S t i ll a n -
o t h e r p r o b l e m i s t h a t c a s t r e s t o r a t i o n s
a r e e x p e n s i v e a n d q u i t e a f e w p a t i e n t s
c a n n o t a f f o r d t h e m . I n t h e s e c a s e s, t h e
d e n t i s t h a s b u t t w o c h o i c e s : a m a l g a m
o r c o m p o s i t e r e s i n .
T h i s r e t r o s p e c t i v e s t u d y w a s u n d e r -
t a k e n t o e x a m i n e w h e t h e r , a n d t o w h a t
e x t e n t , t h e u s e o f a n e n a m e l - b o n d e d
r e s t o r a t iv e r e s i n i n M O D c a v i ti e s o f e n -
d o d o n t i c a l ly t r e a t e d p r e m o l a r s h a d r e -
d u c e d t h e f r e q u e n c y o f to o t h f r a c t u r e
w h e n c o m p a r e d t o e n d o d o n ti c a ll y
t r e a t e d p r e m o l a r s r e s t o r e d w i t h a
M O D a m a l g a m f i ll in g .
M a t e r ia l a n d m e t h o d s
T h e m a t e r i a l w a s c o l le c t e d fr o m M a y
1 9 8 6 t o F e b r u a r y 1 9 8 7 f r o m 8 d e n t i s t s
w o r k i n g a s g e n e r a l p r a c t i t i o n e r s . T h e
d a t a w e r e d e r i v e d f r o m c l in i c a l e x a m -
i n a t i o n s a n d r e v i e w o f t h e p a t i e n t s '
d e n t a l r e c o r d s a n d r a d i o g r a p h s .
T h e l i m i t i n g c r i t e r i a f o r a c c e p t a n c e
o f d a t a w e r e t h e f o l lo w i n g : ( i) a n M O D
c a v i ty in a n e n d o d o n t i c a l l y tr e a t e d p r e -
m o l a r e i t h e r r e s t o r e d w i t h a m a l g a m o r
r e s t o r e d w i t h a c o m p o s i t e r e s i n a f t e r
p r e v i o u s a c i d - e t c h i n g o f t h e e n a m e l ;
( i f ) n o w e a k e n i n g o f a n y o f t h e c u s p s
c a u s e d b y a C l a s s V r e s t o r a t i o n ; ( i i i )
n o r m a l o c c l u s io n a n d a r t i c u la t i o n ; a n d
( i v ) c o m p l e t e p e r m a n e n t d e n t i t i o n i n
t h e a n t e r i o r a n d p r e - m o l a r r e g i o n p l u s
a t le a s t o n e m o l a r i n e a c h q u a d r a n t i n -
v o l v e d i n t h e o c c l u s i o n . T h e f o l l o w i n g
i n f o r m a t i o n w a s re c o r d e d : n a m e o f t h e
12 DentalMaterials4:4. 1988
7/21/2019 1-In Vivo Cusp Fracture of Endodontically Treated Premolars Restored With MOD Amalgam or MOD Resin Fillings
http://slidepdf.com/reader/full/1-in-vivo-cusp-fracture-of-endodontically-treated-premolars-restored-with-mod 2/5
1 7 0 H a n s e n
individual tooth, date of endodont ic
therapy, restorative material, and date
of control. For restorations with a com-
posite resin: type of cavity preparation
(bevel or butt-joint), use of an i nterme-
diate layer of low-viscous resin, and ap-
plication technique (bulk or incre-
ment). In cases of fracture, the dentists
were asked to record the date of regis-
tration of fracture, whether the fracture
involved the facial cusp, the lingual
cusp, or the crown as a whole, and also
whether the fracture resulted in extrac-
tion of the tooth. Informa tion was ob-
tained on 222 endodontic ally treated
premolars restored with either a MOD
amalgam or an enamel -bonded MOD
resin filling. It should be emphasized
that the restorative resins in this study
were applied after previous acid-etch-
ing of the ena mel, but without use of a
dentin- bonding agent.
Trial time of the endodontically
treated premolars was defined as the
time elapsing between the date of en-
dodontic therapy and (a) the date of
fracture; (b) the date of last contact ; (c)
the date of withdrawal; or (d) the
date of final registration. Total trial
time was arranged into intervals of one
year and, for each interval, the effec-
tive numb er of teeth exposed to risk of
fracture was calculated. The cumula-
tive survival rate was then calculated
using life table analysis (9, 10). Ana-
lyses of differences between the cum-
ulative survival rate of each of the 4
premolars and of differences between
MOD amalgam and MOD resin restor-
ations were tested at the 5% level of
significance by means of Chi-square
tests (10).
Resu l ts
Table 1 shows the num ber of endo don-
tically treated premolars restored with
Table 1. Number of endodontically treatedpremolars restored with a MOD amalgam orwith an enamel-bonded MOD resin filling.Number of fractures are shown in paren-theses.
Tooth MOD restorationsnumber*
Amalgam Resin
14, 24 48 (27) 23 (2)15, 25 70 (45) 11 (3)34, 44 13 (3) 2 (0)35, 45 50 (27) 4 (0)
Total 181 (102) 40 (5)
* = Viohl's two-digit system.
10 0
8 O
L UI- -
r
6o
U .I
40
g(. 9
20
%
9 ".
' , . ' \
\ - . .\ \ " - %
\ \ " ' . .
\ \ " ' ., . . . . . . . . . .
I I I I I I I _ Y E A R S A F T E R
2 /. 6 8 10 121 4
TREATMENT
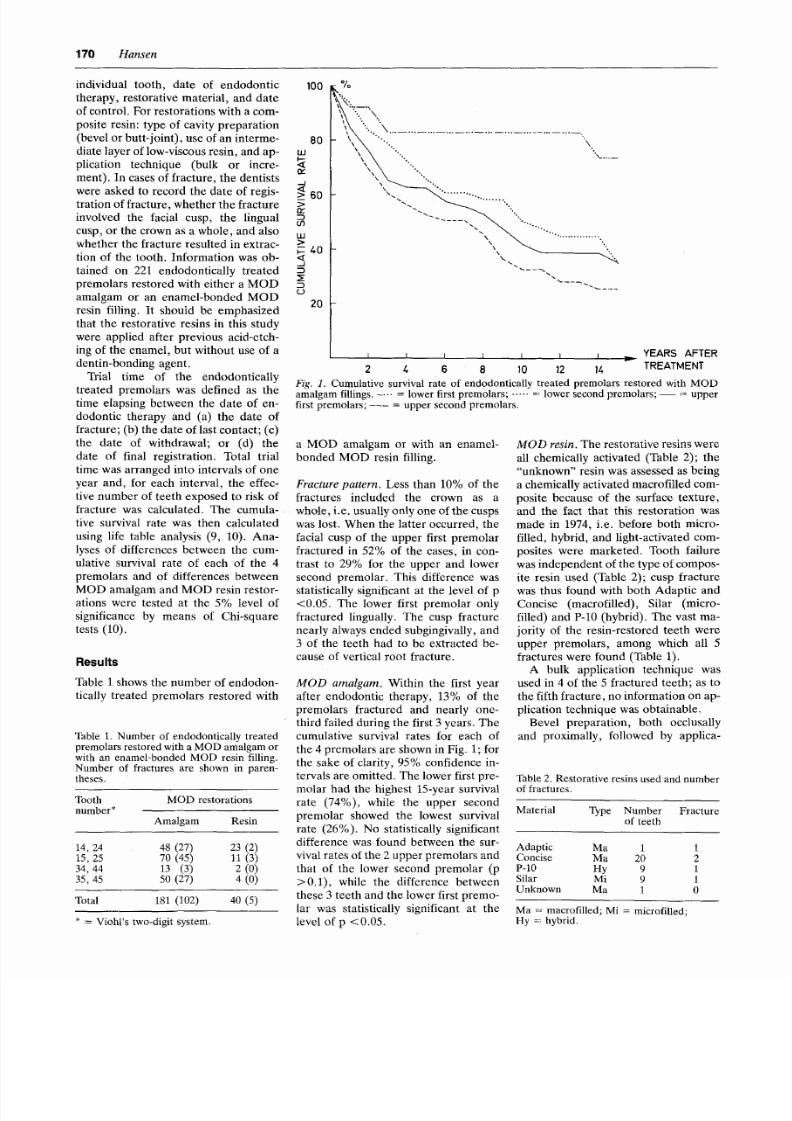
Fig. 1. Cumulative survival rate of endodontically treated premolars restored with MODamalgam fillings. - . . . . lower first premolars; . . . . . . lower second premolars; - - = upperfirst premolars; . . . . upper second premolars.
a MOD amalgam or with an enamel-
bonded MOD resin filling.
F r a c t u r e p a t t e r n . Less than 10% of the
fractures included the crown as a
whole, i.e. usually only one of the cusps
was lost. When the latter occurred, the
facial cusp of the upper first premolar
fractured in 52% of the cases, in con-
trast to 29% for the upper and lower
second premolar. This difference was
statistically significant at the level of p
<0.05. The lower first premolar only
fractured lingually. The cusp fracture
nearly always ended subgingivally, and
3 of the teeth had to be extracted be-
cause of vertical root fracture.
M O D a m a l g a m . Within the first year
after endodontic therapy, 13% of the
premolars fractured and nearly one-
third failed during the first 3 years. Th e
cumulative survival rates for each of
the 4 premolars are shown in Fig. 1; for
the sake of clarity, 95% confidence in-
tervals are omitted. The lower first pre-
molar had the highest 15-year survival
rate (74%), while the upper second
premolar showed the lowest survival
rate (26%). No statistically significant
difference was found between the sur-
vival rates of the 2 upper premolars an d
that of the lower second premolar (p
>0.1), while the difference between
these 3 teeth and the lower first premo-
lar was statistically significant at the
level of p < 0.05.
M O D r e s i n . The restorative resins were
all chemically activated (Table 2); the
"unknown" resin was assessed as being
a chemically activated macrofilled com-
posite because of the surface texture,
and the fact that this restoration was
made in 1974, i.e. before both micro-
filled, hybrid, and light-activated com-
posites were marketed. Tooth failure
was independen t of the type of compos-
ite resin used (Table 2); cusp fracture
was thus found with both Adaptic and
Concise (macrofilled), Silar (micro-
filled) and P-10 (hybrid). The vast ma-
jority of the resin-restored teeth were
upper premolars, among which all 5
fractures were found (Table 1).
A bulk application technique was
used in 4 of the 5 fractured teeth; as to
the fifth fracture, no inf ormation on ap-
plication technique was obtaina ble.
Bevel preparation, both occlusally
and proximally, followed by applica-
Table 2. Restorative resins used and numberof fractures.
Material Type Number Fractureof teeth
Adaptic Ma 1 lConcise Ma 20 2P-10 Hy 9 1Silar Mi 9 1Unknown Ma 1 0
Ma = macrofilled; Mi = microfilled;Hy = hybrid.

7/21/2019 1-In Vivo Cusp Fracture of Endodontically Treated Premolars Restored With MOD Amalgam or MOD Resin Fillings
http://slidepdf.com/reader/full/1-in-vivo-cusp-fracture-of-endodontically-treated-premolars-restored-with-mod 3/5
F r e q u e n c y o f c u s p f r a c t u r e i n v i v o 171
t i o n o f a l o w - v i s c o u s r e s i n , w a s u s e d i n
3 0 o f t h e 4 0 r e s i n - r e s t o r e d p r e m o l a r s ;
n o i n f o r m a t i o n o n b e v e l / b u t t - jo i n t an d
l o w - v i s c o u s r e s i n w a s o b t a i n a b l e f o r t h e
r e m a i n i n g 1 0 fi l li n g s . F o u r o f t h e 5 f r a c -
t u r e s w e r e f o u n d i n t e e th w i t h b e v e l e d
c a v i t y m a r g i n s .
A m a l g a m v s . r e s i n . A s m e n t i o n e d e a r -
l i e r , t h e c u m u l a t i v e s u r v i v a l r a t e o f
a m a l g a m - r e s t o r e d l o w e r f ir st p r e m o l a r s
w a s s i g n i f i c a n t l y h i g h e r t h a n t h e s u r v i -
v a l ra t e s o f t h e 3 o t h e r p r e m o l a r s ( F i g .
1 ) . L o w e r f i r s t p r e m o l a r s a r e t h e r e f o r e
n o t i n c l u d e d i n t h e s t a t i st i c a l a n a l y s i s o f
d i f fe r e n c e s b e t w e e n t h e s u r v i v a l r a t e o f
M O D a m a l g a m a n d M O D r e si n -r e -
s t o r e d t e e t h . A s e p a r a t e a n a l y s i s o f
l o w e r f i r st p r e m o l a r s i s m e a n i n g l e s s b e -
c a u s e o f th e s m a l l n u m b e r o f o b s e r v a -
t i o n s ( T a b l e 1 ) .
T h e p o o l e d c u m u l a t i v e s u r v i v a l r a t eo f t h e u p p e r f i r st p r e m o l a r s , t h e u p p e r
s e c o n d p r e m o l a r s a n d t h e l o w e r se c o n d
p r e m o l a r s i s s h o w n i n F ig . 2 .
C h i - s q u a r e a n a l y s i s i n a 2 x 2 c o n -
t i n g e n c y t a b l e r e q u i r e s t h a t t h e e x -
p e c t e d f r e q u e n c y i n e a c h c e l l n o t b e t o o
s m a l l ; th e i n t e r v a ls a n a l y z e d w e r e
t h e r e f o r e r e s t r i c t e d t o 0 - 3 y e a r s , 3 - 6
y e a r s , a n d 6 -- 10 y e a r s . A n a l y s i s b e y o n d
1 0 y e a r s w a s n o t m a d e b e c a u s e o n l y 8
r e s i n r e s t o r a t i o n s w e r e o l d e r t h a n 1 0
y e a r s , a n d o n l y 4 r e s t o r a t i o n s w e r e o l -
d e r t h a n 1 1 y e a r s . T h e a n a l y s i s ( T a b l e
3 ) s h o w e d a h i g h l y s i g n i f ic a n t d i ff e r -e n c e b e t w e e n t h e s u r v i v a l r a t e o f a m a l -
g a m a n d r e s i n - r e s t o r e d p r e m o l a r s a t p
< 0 . 0 0 1 ; t h e m a i n r e a s o n w a s t h a t n o
r e s i n - r e s to r e d t o o t h f r a c t u r e d d u r i n g
t h e f i r st 3 y e a r s . T h e r e s i n - r e s t o r e d p r e -
m o l a r s h a d a s l i g h t ly b e t t e r s u r v i v a l
r a t e d u r i n g t h e 3 ~ 5 a n d 6 - 1 0 y e a r in t e r -
v a l s ( F i g . 2 ; T a b l e 3 ) , b u t t h i s d i f f e r -
e n c e w a s n o t s t a t i s t ic a l l y s i g n i f ic a n t ( p
> 0 . 0 5 ) .
Discussion
L i k e a l l r e t r o s p e c t i v e s t u d i e s , t h i s i n -
v e s t i g a ti o n h a s a n i n h e r e n t d i s a d v a n -
t a g e i n t h a t t h e d a t a o b t a i n e d f r o m r e -
v i e w o f t h e p a t i e n t s ' r e c o r d s o n l y p a r -
t ia l ly a n s w e r e d t h e q u e s t io n s a s k e d .
M a n y e s s e n t i a l d e t a i ls m a y b e l o s t i n a
r e t r o s p e c t i v e s t u d y b e c a u s e m o s t p a -
t i e n t r e c o r d s d o n o t c o n t a i n a l l t h e i n -
f o r m a t i o n n e e d e d f o r a c a r e fu l i n v e s ti -g a t i o n . T h i s p r o b l e m d o e s n o t p r e v e n t
a d i s c u s s i o n o f t h e p o s s i b l e c a u s e s o f
t h e d i f f e r e n t s u r v i v a l r a t e s o f a m a l g a m
a n d r e s i n - r e s t o r e d p r e m o l a r s , b u t t h e
r e s u l t s o f t h i s s t u d y s h o u l d b e c a u -
t i o u s l y i n t e r p r e t e d , e s p e c i a l l y s i n c e t h e
n u m b e r o f r e s i n - re s t o r e d t e e t h w a s
r a t h e r s m a l l .
L a b o r a t o r y s t u d i e s h a v e s h o w n t h a t a
n o n - b o n d e d i n t r a c o r o n a l r e s t o r a t i o n
d o e s n o t s t re n g t h e n t h e t o o t h , a n d t h a t
t h e f r a c t u r e r e s i s ta n c e o f p r e m o l a r s
w i t h M O D c a v i t ie s r e s t o r e d w i th a m a l -
g a m o r w i th a n o n - b o n d e d c o m p o s i ter e s i n is s i m i l a r t o t h a t o f p r e m o l a r s w i t h
a n u n f i l l e d M O D c a v i t y ( 8 , 1 1 , 1 2 ).
S e v e r a l a u t h o r s h a v e p u b l i s h e d p a p e r s
o n t h e r e i n f o r c i n g ef f e ct o f a n e n a m e l -
b o n d e d c o m p o s i t e r e s t o r a t i o n w i t h o u t
p r e v i o u s a p p l i c a t i o n o f a d e n t i n - b o n d -
i n g a g e n t , a s in v e s t i g a t e d in t h e p r e s e n t
s t u d y , b u t t h e r e s u l t s a r e c o n t r a d i c t o r y .
R e e l & M i t c h e l l ( 1 3 ) , E a k l e ( 1 4 ) a n d
S t a m p a l i a e t a l . ( 1 5 ) d i d n o t f i n d a s ig -
n i f i c a n t i n c r e a s e i n t h e f r a c t u r e r e s i s -
t a n c e , i n c o n t r a s t w i t h S i m o n s e n e t a l ,
( 1 1 ), D o u g l a s ( 1 2 ) a n d M a c k e n z i e ( 1 6) ,
w h o a ll f o u n d t h a t p r e m o l a r s w i th e n -a m e l - b o n d e d c o m p o s i t e r e s t o r a t i o n s
w e r e s t r o n g e r t h a n t h o s e e i t h e r re -
s t o r e d w i t h a m a l g a m o r l e f t u n r e s t o r e d .
H o w e v e r , m e t h o d s u s e d i n v i t ro t o
m e a s u r e t h e f r a c t u r e r e s i s ta n c e o f t e e t h
w i th a n M O D p r e p a r a t i o n m a y n o t r e -
p r o d u c e w h a t a c t u a l l y h a p p e n s i n v i v o .
I n t h e p r e s e n t i n v e s t ig a t i o n o n l y 3 o f
t h e 1 0 7 f r a c t u r e s w e r e s o v e r t i c a l t h a t
t h e t o o t h h a d t o b e e x t r a c t e d . T h i s l o w
f r e q u e n c y o f v e r t i c a l fr a c t u r e i s n o t i n
a c c o r d a n c e w i t h th e i n v i t ro r e s u l t s p r e -
s e n t e d b y S t a m p a l i a e t a l. ( 1 5 ) ; t h e s e
a u t h o r s f o u n d t h a t a l l e x c e p t o n e o f 22
f r a c t u r e s o c c u r r e d a s a m i d d l e s p l i t o f
t h e t o o t h t h r o u g h t h e p u l p a l f lo o r o f
t h e c a v i ty p r e p a r a t i o n . T h e d i s c r e p a n c y
b e t w e e n t h e r e s u l t s o f t h e p r e s e n t s t u d y
a n d t h e r e s u l t s p u b l i sh e d b y S t a m p a l i a
e t a l . ( 15 ) m a y v e r y w e l l b e c a u s e d b y
t h e d i f f e r e n t d i m e n s i o n s o f t h e M O D
c a v i t ie s . A f u r t h e r p o s s i b l e e x p l a n a t i o nh a s b e e n g i v e n b y C r a i g ( 1 7 ) , w h o
p o i n t e d o u t t h a t i n v i t ro t e s t i n g o f a r i -
g i d ly s u p p o r t e d t o o t h i g n o r e s t h e r e -
s il ie n c y o f t h e p e r i o d o n t a l l i g a m e n t .
A l s o , i t d o e s n o t s e e m v e r y l i k e ly , co n -
s i d e ri n g t h e c o m p l e x o c c l u s a l f u n c t io n ,
t h a t i n v i v o l o a d i n g o f t h e c u s p s c a n b e
c o m p l e t e ly r e p r o d u c e d i n v i t ro w i t h t h e
t e s t m e t h o d s u s e d ( 1 1 -1 6 ) .
T h e m o s t a s t o n i s h i n g f i n d i n g i n t h e
p r e s e n t s t u d y W a s t h e v e r y h i g h f r e -
q u e n c y o f c u s p f r a c t u r e o f t h e a m a l -
g a m - r e s t o r e d p r e m o l a r s , w h e r e n e a r l y
o n e - t h i r d f r a c t u r e d w i t h in 3 y e a r s a f t e re n d o d o n t i c t r e a t m e n t ( T a b l e 3 ) . T h e s e
f r a c t u r e s , m o s t o f t e n s u b g i n g i v a l , m a y
r e s u lt i n p e r m a n e n t i n j u r y to t h e p e r i o -
d o n t a l t i s s u e s n o t o n l y b e c a u s e o f t h e
f r a c t u r e i t s e l f , b u t a l s o b e c a u s e e v e n a
w e l l - a d a p t e d r e s t o r a t i o n w i l l h a r d l y
e v e r b e s u r r o u n d e d b y t h e sa m e
h e a l t h y p e r i o d o n t a l t is s u e s a s th e n a t u -
r a l t o o t h s u r f a c e i t s e l f (3 - 7 ) .
T h e f re q u e n c y o f fr a c t u r e d i f fe r e d
a m o n g t h e 4 a m a l g a m - r e s t o r e d p re m o -
l a r s (F i g . 1 ) . T h e h i g h 1 5 - y e a r s u rv i v a l
r a t e o f t h e l o w e r f i rs t p r e m o l a r ( 7 4 % )
c o m p a r e d t o a n a v e r a g e o f 3 2 % f o r t h eo t h e r t h r e e p r e m o l a r s ( F i g s . 1 a n d 2 ) is
p r o b a b l y r e l a t e d t o b o t h t h e a n a t o m i c a l
f o r m a n d t h e l o c a t io n o f t h e t o o t h . A s
t o t h e l a t t e r , L e i n f e l d e r ( 1 8 ) h a s p r e -
s e n t e d a w e a r f a c t o r o f c o m p o s i t e r e si n
a s a f u n c t i o n o f l o c a t i o n : t h e l o w e r f i r st
p r e m o l a r w a s g i v e n a w e a r f a c t o r o f
1 x , t h e u p p e r f ir s t p r e m o l a r 3 x , a n d
t h e tw o s e c o n d p r e m o l a r s 4 x . T h e s e
w e a r f a c t o r s , b e i n g a f u n c t i o n o f l o -
c a t i o n , a r e i n f a ir l y g o o d a g r e e m e n t
w i t h t h e d i f f e r e n t f r e q u e n c i e s o f c u s p
f r a c tu r e o f t h e 4 p r e m o l a r s f o u n d i n t h e
p r e s e n t s t u d y ( F i g . 1 ) .
Table 3 . C hi - square analys is o f surv ival r a t es ( cusp/crown f r ac ture) of endod ont i ca l ly t r ea t ed perm olar s r es tor ed wi th M OD amalgam f il li ngsor wi th enam el -bond ed MO D res in f il li ngs.
Years af tert r e a t m e n t
M O D a m a l g a m r e s to r a t io n s M O D r e si n r e s to r a t io n s
1~ dx Ux l'x l'~-d ~ lx d~ u~ 1'~ l' x -d~ ;(2
0-3 168 53 9 163.5 110.5 38 0 1 37.5 37.5 16.5093-6 106 17 11 100.5 83.5 37 3 5 34.5 31.5 1.3756-10 78 19 9 73.5 54.5 29 2 19 19.5 17.5 2.144
Total Chi-squ are 20.028
1• = intac t at beg inning of interval ; d x = fai l lures dur ing interva l ; ux = withdrawn and los t cases dur ing interval ; 1 'x = effective num bersexposed to r i sk of f r ac ture .
12"
7/21/2019 1-In Vivo Cusp Fracture of Endodontically Treated Premolars Restored With MOD Amalgam or MOD Resin Fillings
http://slidepdf.com/reader/full/1-in-vivo-cusp-fracture-of-endodontically-treated-premolars-restored-with-mod 4/5
172 H a n s e n
100
80
IL l
t Y
<
> 6 0
W>
~ 40<
IE
20
I I I
2 4 6 8
YEARS AFTERI I t
10 12 14 TREATMENT
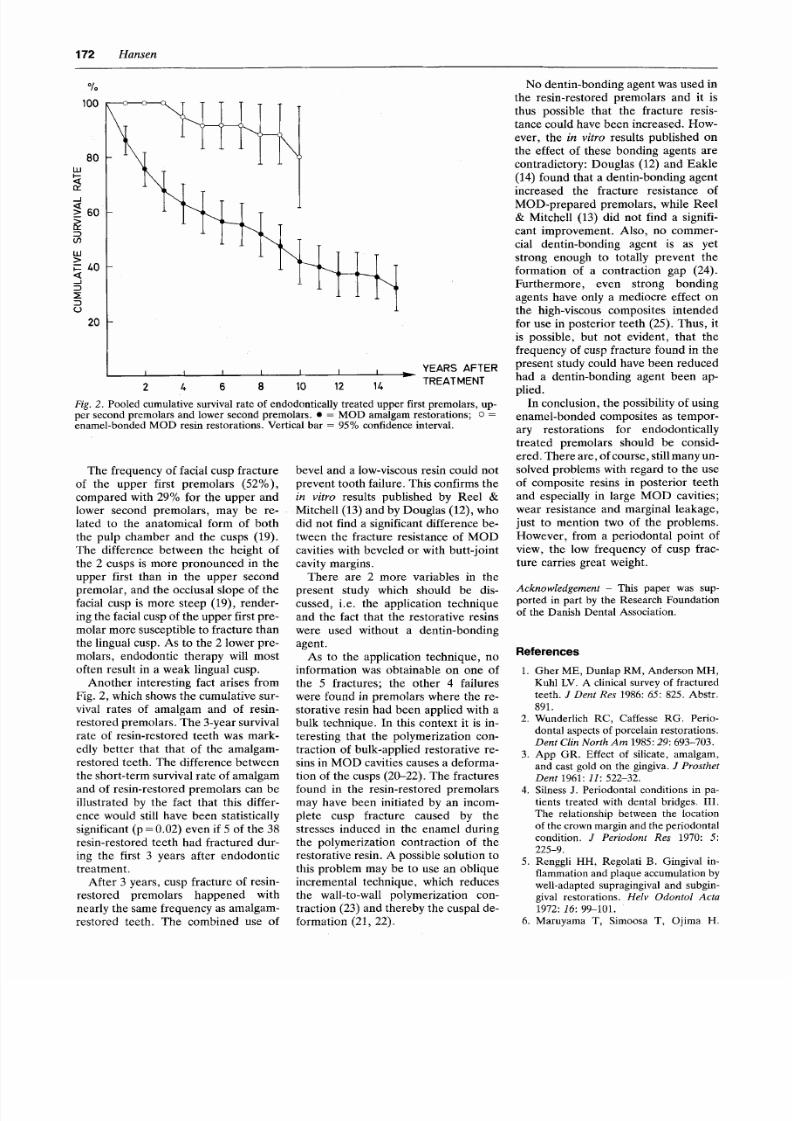
Fig . 2 . Pooled cumulative survival rate of endodontically treated upper first premolars, up-per second premolars and lower second premolars. 9 = MOD amalgam restorations; o =enamel-bonded MOD resin restorations. Vertical bar = 95% confidence interval.
The frequency of facial cusp fracture
of the upper first premolars (52%),
compared with 29% for the upper and
lower second premolars, may be re-
lated to the anatomical form of both
the pulp chamber and the cusps (19).
The difference between the height of
the 2 cusps is more pronounced in the
upper first than in the upper second
premolar, and the occlusal slope of the
facial cusp is more steep (19), render-
ing the facial cusp of the upp er first pre-
molar more susceptible to fracture than
the lingual cusp. As to the 2 lower pre-
molars, endodontic therapy will most
often result in a weak lingual cusp.
Another interesting fact arises from
Fig. 2, which shows the cu mulat ive sur-
vival rates of amalgam and of resin-
restored premolars. The 3-year survival
rate of resin-restored teeth was mark-
edly better that that of the amalgam-
restored teeth. The difference between
the short-term survival rate of amalgam
and of resin-restored premolars can be
illustrated by the fact that this differ-
ence would still have been statistically
significant (p = 0.02) e ven if 5 of the 38
resin-restored teeth had fractured dur-
ing the first 3 years after endodontic
treatment.
After 3 years, cusp fracture of resin-
restored premolars happened with
nearly the same frequency as amalgam-
restored teeth. The combined use of
bevel and a low-viscous resin could no t
prevent tooth failure. This confirms the
i n v i t r o results published by Reel &
Mitchell (13) and by Douglas (12), who
did not find a significant difference be-
tween the fracture resistance of MOD
cavities with beveled or with butt-joint
cavity margins.
There are 2 more variables in the
present study which should be dis-
cussed, i.e. the application technique
and the fact that the restorative resins
were used without a dentin-bonding
agent.
As to the application technique, no
information was obtainable on one of
the 5 fractures; the other 4 failures
were found in premolars where the re-
storative resin had bee n applied with a
bulk technique. In this context it is in-
teresting that the polymerization con-
traction of bulk-applied restorative re-
sins in MOD cavities causes a defo rma-
tion of the cusps (20-22). The fractures
found in the resin-restored premolars
may have been initiated by an incom-
plete cusp fracture caused by the
stresses induced in the enamel during
the polymerization contraction of the
restorative resin. A possible solution to
this problem may be to use an oblique
incremental technique, which reduces
the wall-to-wall polymerization con-
traction (23) and thereby the cuspal de-
formation (21, 22).
No den tin-bond ing agent was used in
the resin-restored premolars and it is
thus possible that the fracture resis-
tance could have bee n increased. How-
ever, the i n v i t r o results published on
the effect of these bonding agents are
contradictory: Douglas (12) a nd Eakl e
(14) found that a den tin-bon ding agent
increased the fracture resistance of
MOD-prepared premolars, while Reel
& Mitchell (13) did not find a signifi-
cant improvement. Also, no commer-
cial dent in-bondi ng agent is as yet
strong enough to totally prevent the
formation of a contraction gap (24).
Furthermore, even strong bonding
agents have only a mediocre effect on
the high-viscous composites intended
for use in posterior teeth (25). Thus, it
is possible, but not evident, that the
frequency of cusp fracture found in the
present study could have bee n reduced
had a dent in-bond ing agent been ap-
plied.
In conclusi on, the possibility of using
enamel-bonded composites as tempor-
ary restorations for endodontically
treated premolars should be Consid-
ered. There are, of course, still many un-
solved problems with regard to the use
of composite resins in posterior teeth
and especially in large MOD cavities;
wear resistance and marginal leakage,
just to mention two of the problems.
However, from a periodontal point of
view, the low frequency of cusp frac-
ture carries great weight.
A c k n o w l e d g e m e n t - This paper was sup-ported in part by the Research Foundationof the Danish Dental Association.
R e f e r e n c e s
1. Gher ME, Dunlap RM, Anderson MH,Kuhl LV. A clinical survey of fracturedteeth. J D e n t R e s 1986:6 5 : 825. Abstr.891.
2. Wunderlich RC, Caffesse RG. Perio-dontal aspects of porcelain restorations.
D e n t C l in N o r t h A m 1985:29 : 693-703.3. App GR. Effect of silicate, amalgam,
and cast gold on the gingiva. J P r o s t h e t
D e n t 1961: 11 : 522-32.4. Silness J. Periodontal conditions in pa-
tients treated with dental bridges. III.The relationship between the locationof the crown margin and the periodontalcondition. J P e r i o d o n t R e s 1970: 5:225-9.
5. Renggli HH, Regolati B. Gingival in-flammation and plaque accumulation bywell-adapted supragingival and subgin-gival restorations. H e l v O d o n t o l A c t a
1972: 16 : 99-101.6. Maruyama T, Simoosa T, Ojima H.

7/21/2019 1-In Vivo Cusp Fracture of Endodontically Treated Premolars Restored With MOD Amalgam or MOD Resin Fillings
http://slidepdf.com/reader/full/1-in-vivo-cusp-fracture-of-endodontically-treated-premolars-restored-with-mod 5/5
Frequency of cusp fracture i n v i v o 1 7 3
M o rp h o l o g y o f g i n g i v a l c a p i ll a r i e s a d j a -
c e n t t o c o m p l e t e c r o w n s . J Prosthet
Dent 1976: 35: 1 7 9 -8 4 .
7 . Va l d e rh a u g J . Pe r i o d o n t a l c o n d i t i o n s
a n d c a r i o u s l e s i o n s fo l l o wi n g t h e i n se r -
t i o n o f f i x e d p ro s t h e se s : a 1 0 -y e a r fo l -
l o w-u p s t u d y . Int Dent J 1980: 30: 2 9 6 -
304.
8 . H o o d J A A . M e t h o d s to i m p r o v e f r a c-t u r e r e s i s t a n c e o f te e t h . I n : V a n h e r l e G ,
S m i t h D C , e d s . Posterior composite re-
sin dental restorative materials. T h e
Ne t h e r l a n d s : Pe t e r Sz u l c , 19 8 5: 4 4 3 -5 0 .
9 . C u t l e r S J , E d e r e r E M a x i m u m u t i li z a -
t i o n o f t h e l i f e t a b l e m e t h o d i n a n a l y z in g
su rv i v a l . J Chronic Dis 1958: 8 : 699-
712 .
1 0 . Tb y l s t ru p A, R 6 1 1i ng I . Th e l i f e t a b l e
me t h o d i n c l i n i c a l d e n t a l r e se a rc h .
Community Dent Oral Epidemiol 1975:
3 : 5 -1 0 .
1 1. S i m o n s e n R J , B a r o u g h E , G e l b M .
C u s p f r a c t u r e r e s i s t a n c e f r o m c o m p o s i t e
re s i n i n C l a s s I I r e s t o ra t i o n s . J Dent Res
1983: 62: 2 5 4 . Ab s t r . 7 6 1 .1 2. D o u g l a s W H . M e t h o d s t o i m p r o v e f ra c -
t u r e r e s i s t a n c e o f t e e t h . I n : V a n h e r l e G ,
S m i t h D C , e d s . Posterior composite re-
sin dental restorative materials. T h e
Ne t h e r l a n d s : Pe t e r Sz u l c , 1 9 8 5 : 4 3 3 -4 1 .
1 3 . R e e l DC , M i t c h e l l R J . F ra c t u re re s i s -
t a n c e o f t e e t h r e s t o r e d w i t h C l a s s I I
c o m p o s i t e r e s t o r a t i o n s . J Dent Res
9 1984: 63: 2 7 6 . Ab s t r . 9 5 0 .
1 4. E a k l e W S . F r a c t u r e r e s i s t a n c e o f t e e t h
r e s t o r e d w i t h C l a s s I I b o n d e d c o m p o s i t ere s i n . J Dent Res 1986: 65: 1 4 9 -5 3 .
1 5 . S t a m p a l i a LL , N i c h o I l s J I , B ru d v i k JS ,
J o n e s D W . F r a c t u r e r e s i s t a n c e o f t e e t h
w i t h r e s i n - b o n d e d r e s t o r a t i o n s . J Pros-
thet Dent 1986: 55: 6 9 4 -8 .
1 6. M a c k e n z i e D E T h e r e i n f o r c i n g e f f e ct o f
me s i o -o e c l u so d i s t a l a c i d -e t c h c o mp o s i t e
r e s t o r a t i o n s o n w e a k e n e d p o s t e r i o r
t e e t h . Br Dent J 1986: 161: 4 1 0 ~ .
1 7. C r a i g R G . O p e n d i s c u s s io n o f D o u g l a s /
H o o d p a p e r s . I n : V a n h e r l e G , S m i t h
D C , e d s . Posterior composite resin den-
tal restorative materials. T h e N e t h e r -
l a n d s : Pe t e r Sz u l c , 1 9 8 5 : 4 5 1 -2 .
1 8. L e i n f e l d e r K E C o m p o s i t e r e s i n s. Dent
Clin North Am 1985: 29: 3 5 9 -7 1 .1 9 . C a r l se n O. Ta n d mo rfo l o g i sk e sk i t s e r .
C o p e n h a g e n : M u n k s g a a r d , 1 9 8 6 .
2 0 . C a u s t o n B E , M i l l e r B , S e f t o n J . T h e
d e r f o r m a t i o n o f c u s p s b y b o n d e d p o s -
t e r i o r c o m p o s i t e r e s t o r a t i o n s : a n in vitro
s t u d y . Br Dent J 1985: 159: 3 9 7 -4 0 0 .
2 1 . J e n s e n M E , C h a n D C N . P o l y m e r i z a -
t i o n c o n t r a c t i o n a n d m i c r o l e a k a g e . I n :
V a n h e r l e G , S m i t h D C , e d s. Posterior
composite resin dental restorative mate-
rials. T h e N e t h e r l a n d s : P e t e r S z u l c ,1985: 243-62 .
2 2 . M c C u l l o c k A J , S m i t h B G N . In vitro
s t u d i e s o f c u s p a l m o v e m e n t p r o d u c e d
b y a d h e s i v e r e s t o r a t i v e m a t e r i a l s . Br
Dent J 1986: 161: 4 0 5 -9 .
2 3 . H a n s e n E K . E f f e c t o f c a v i ty d e p t h a n d
a p p l i c a ti o n t e c h n i q u e o n m a r g i n a l a d a p -
t a t i o n o f r e s i n s i n d e n t i n c a v i t ie s . J Dent
Res 1986: 65: 1319-21 .
2 4 . H a n s e n EK , A s m u s s e n E . C o m p a r a t i v e
s t u d y o f d e n t i n a d h e s i v e s . Scand J Dent
Res 1985: 93: 2 8 0 -7 .
2 5 . H a n s e n E K . E f f e c t o f t h r e e d e n t i n a d -
h e s i v e s o n m a r g i n a l a d a p t a t i o n o f t w o
l i g h t -c u re d c o mp o s i t e s . Scand J Dent
Res 1986: 94: 8 2 -6 .