1. Identifying women with GDM is important because appropriate therapy can decrease fetal and...
39
Insulin Treatment of Patients with Gestational Diabetes Mellitus (GDM) F . Hadaegh MD. Prevention of Metabolic Disorders Research Center 1
-
Upload
reynold-jenkins -
Category
Documents
-
view
216 -
download
0
Transcript of 1. Identifying women with GDM is important because appropriate therapy can decrease fetal and...

1
Insulin Treatment of Patients with Gestational Diabetes Mellitus (GDM)
F . Hadaegh MD.
Prevention of Metabolic Disorders Research Center

2
Rational for GDM Treatment
Identifying women with GDM is important because appropriate therapy can decrease fetal and maternal morbidity, particularly macrosomia .
An effective treatment regimen :
-Dietary therapy
-SMBG
-Insulin if target blood glucose values are not met with diet alone.

3
Nutritional Therapy
By a registered dietitian upon diagnosis and be placed on an appropriate diet
The goals of medical nutritional therapy
Achieve normoglycemia
Prevent ketosis
Provide adequate weight gain Contribute to fetal well-being

4
Major Components in MNT of GDM
Caloric allotment
Carbohydrate intake
and calorie distribution

5
Calorie Allotment
Calorie allotment (ideal body weight):
30 kcal per kg current weight per day in pregnant BMI 22 to 25 kg/m2
24 kcal per kg current weight per day in overweight pregnant women (BMI 26 to 29 kg/m2).
12 to 15 kcal per kg current weight per day for morbidly obese pregnant women (BMI >30 kg/m2).
40 kcal per kg current weight per day in pregnant women who are less than BMI 22kg/m2

6
Carbohydrate Intake Carbohydrate intake (33 to 40 %)percent of
calories Protein (about 20 percent) Fat (about 40 percent) With this calorie distribution, 75 to 80 percent of
women with GDM will achieve normoglycemia. PPG are directly dependent upon the
carbohydrate content of a meal Complex carbohydrates, (starches and
vegetables) are more nutrient dense and PPG less than simple sugars.
Noncaloric sweeteners, such as aspartame, may be used in moderation.

7
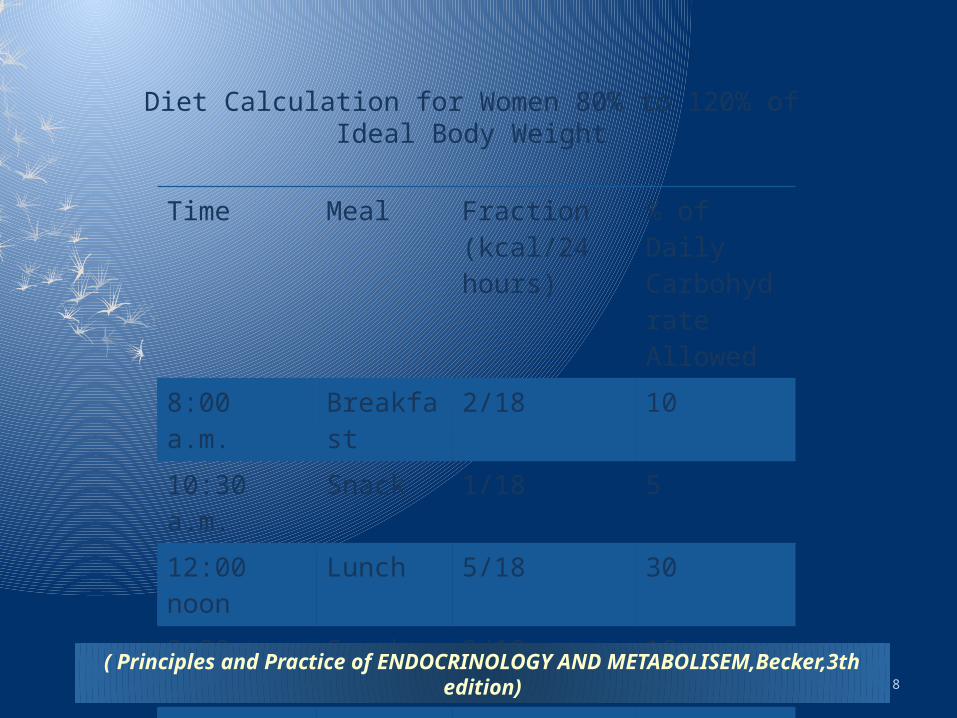
Calorie Distribution
3 meals and 3 snacks; however, in overweight and obese women the snacks are often eliminated
The breakfast meal should be small (10 %total calories) to help maintain PP euglycemia;
CHO at breakfast is also limited since insulin resistance is greatest in the morning.
Lunch (30 percent of total calories )
Dinner (30 percent of total calories )
Snacks (Leftover calories) (30%of total calories) are distributed, as needed, as snacks.
8
Time Meal Fraction (kcal/24 hours)
% of Daily Carbohydrate Allowed
8:00 a.m. Breakfast 2/18 10
10:30 a.m. Snack 1/18 5
12:00 noon Lunch 5/18 30
3:00 p.m. Snack 2/18 10
5:00 p.m. Dinner 5/18 30
8:00 p.m. Snack 2/18 5
11:00 p.m. Snack 1/18 10
Diet Calculation for Women 80% to 120% of Ideal Body Weight
( Principles and Practice of ENDOCRINOLOGY AND METABOLISEM,Becker,3th edition)

9
Gestational Diabetes: The Need for a Common GroundE Albert Reece A 2003 Cochrane review showed no difference
in the prevalence of birth weights 4000 g or C/S in women with GDM who were randomly assigned to primary dietary therapy or no specific treatment.
The authors concluded that insufficient evidence exists to recommend dietary therapy in patients with altered glucose metabolism .
( www.thelancet.com Vol 373 May 23, 2009)

10
Exercise
Exercise appears to improve glycemic control primarily from increased tissue sensitivity to insulin.
In one small randomized trial, six weeks of a cardiovascular fitness program using arm ergometry three times a week for 20 to 30 minutes per session resulted in normalization of glucose tolerance .
The value of exercise in women with GDM requires further exploration to determine the potential range of benefits
ADA encourages a program of moderate exercise as part of the treatment plan for women with GDM and no medical or obstetrical contraindications to this level of physical activity

11
Gestational Diabetes: The Need for a Common GroundE Albert Reece Women who spent 20 h per week watching TV
and did not do any vigorous activity had a higher risk of developing the condition than women who spent <2 h per week watching TV and did physical activity.
Women with GDM who exercised regularly during pregnancy were less likely than those who did not exercise to deliver a large-for-gestational-age infant(LGA)
( www.thelancet.com Vol 373 May 23, 2009)

12
Glucose Goal INSULIN : on two or more occasions within a two-week
interval despite dietary therapy FBS≥ 90 mg/dL - 1hPP ≥ 120 mg/dL.
The main purpose of drug intervention at these levels is to minimize the incidence of macrosomia, and its associated risks of shoulder dystocia, birth trauma, and possibly childhood obesity and metabolic syndrome.(FBS<90 and 1hPP <120).
By comparison, ACOG recommend insulin to reduce the risk of macrosomia when FBS≥ 95 mg/dL or 1hPP >130 to 140 mg/dL or 2hPP ≥ 120 mg/dL.
The Hyperglycemia and Adverse Pregnancy Outcome trial (HAPO) showed that a FBS 105 mg/dL was associated with a risk of macrosomic 5 fold greater than that with a FBS <75 mg/dL (25 versus 5 percent).

13
ACOG(18) American Diabetes
Association (19)
Fourth International Workshop-
Conference (1)
Canadian Diabetes
Association (20)
Fasting (mg/dl) 60-90 <105 <95 -
Premeal (mg/dl) 60-105 - - 95
Postmeal (mg/dl)
1 h <130-140 <155 <140 <140
2 h <120 <130 <120 <120
Mean (mg/dl) 100 - - -
Nighttime (mg/dl) 60-90 - - -
Recommended glycemic thresholds
Data are means ±1 SD

14
Gestational Diabetes: The Need for a Common GroundE Albert Reece The fifth international workshop -conference on
gestational diabetes recommended the following blood glucose concentrations:
FPG of 90–99 mg/dL; 1-h PPG <140 mg/dL; and 2-h PPG below <120–127 mg/dL.
(www.thelancet.com Vol 373 May 23, 2009)

15
Timing and Frequency Check FBS on awakening and 1hpp because the degree of fasting
glycemia alone does not predict the need for insulin therapy. The value of PP versus preprandial measurement was illustrated in
a study that randomly assigned patients to have their diabetes managed according to results of preprandial or postprandial monitoring (one hour after meals) of blood glucose concentrations:
1hpp was associated with the following benefits as compared to preprandial monitoring:
Better glycemic control (HbA1c value 6.5 versus 8.1 percent) A lower incidence of LGA infants (12 versus 42 percent) A lower rate of C/S for cephalopelvic disproportion (12 versus 36
percent) Assessment of blood glucose can be performed either one or two
hours postprandially, the optimum time has not been determined It is suggested for determination of blood glucose one hour after
meals.

16
Glucose Monitoring
Check BS at least 4 times daily (fasting and one-hour after the first bite of each meal)
SMBG is important for women managed with MNT alone, as well as those on anti-hyperglycemic agents.
Daily measurement allows recognition of women who should begin an anti-hyperglycemic agent and appears to decrease the risk of macrosomia
Although many providers decrease the frequency SMBG in women with good glycemic control, there are no data on the duration of good control sufficient to reduce the frequency of SMBG or the appropriate frequency of testing in GDM that is well controlled with MNT.

17
Meters
Almost all blood glucose meters give direct plasma readings from the capillary whole blood sample, presumably by partitioning off the red blood cells and sampling only the plasma in the sample.
Some present the results as plasma glucose concentration by multiplying the whole blood result by 1.12. (100 1.12=112 mg/dl)
The patient and clinician should know how the glucose concentration is being measured and reported

18
Glycosylated Hemoglobin (A1C)
A helpful test in assessing glycemic control during pregnancy
Measure HbA1c every two to four weeks to provide the patient with feedback and to ascertain that blood glucose monitoring is accurately reflecting maternal glycemic control.
It should be noted that A1C values tend to be lower in pregnant compared to nonpregnant women because the average blood glucose concentration is about 20 percent lower in pregnant women

19
HbA1C
The association between Hb1C and pregnancy outcome and macrosemia in GDM patients is poor.
In preexisting DM the HbA1C correlates with congenital anomalies and spontaneous abortion.
(DIABETES CARE, VOLUME 30, SUPPLEMENT 2, JULY 2007).
20
Monitoring for Ketones Monitor urinary ketones in women with GDM is nor
recommended. Ketonuria is not associated with an adverse effect on cognitive
development of the fetus. Ketonemia with elevated glucose levels may have an
adverse effect of cognitive development Diabetic ketoacidosis is rare in women with gestational diabetes. In general, women with diabetes should test their urine for
ketones if the BS 240 mg/dl ,during periods of illness or stress, or if there are symptoms compatible with ketoacidosis such as nausea, vomiting, and abdominal pain.
The present of ketones in the urine does not always mean that the person has impending ketoacidosis.
Ketonuria indicates that the person is in a catabolic state and is breaking down fat, and can occur in anyone who has a negative caloric balance. Ketonemia does not accompany ketonuria in this setting .

21
Insulin
15 percent of women with GDM are placed on insulin
In addition, randomized trials have suggested that restricting insulin administration to the subgroup of women with indirect evidence of fetal hyperinsulinemia (e.g., ultrasound showing abdominal circumference >75th percentile early in the third trimester) allows targeted treatment of those at highest risk of delivering a macrosomic infant and avoids treatment of those at low risk .
Some of these women have no or mild hyperglycemia.
22
Insulin Dose
A total insulin dose ranging from 0.7 to 2 units per kilogram (present pregnant weight) to achieve glucose control.
The dose and type of insulin used is calculated based upon the specific abnormality of blood glucose noted during monitoring:
23
Insulin Therapy …..
FBS is high, an intermediate-acting insulin, such as NPH insulin, is given before bedtime. (an initial dose of 0.2 unit/kg body weight)
If PP glucose concentrations are high, insulin aspart or insulin lispro before meals at a dose calculated to be 1.5 units per 10 grams CHO in the breakfast meal and 1 unit per 10 grams CHO in the lunch and dinner meals.
If both preprandial and postprandial blood glucose concentrations are high or if the woman's postprandial glucose levels can only be blunted if starvation ketosis occurs, then we suggest initiating a four injection per day regimen.
It suggests total dose of 0.7 unit/kg up to week 18 , 0.8 unit/kg for weeks 18 to 26, 0.9 unit/kg for weeks 26 to 36, and 1. unit/kg for weeks 36 to term.
In a morbidly obese woman, the initial doses of insulin may need to be increased to 1.5 to 2. units/kg to overcome the combined insulin resistance of pregnancy and obesity.

24
MSI in GDM
The insulin is divided as:
50 percent as NPH insulin [given in three equal doses before breakfast, before dinner( IS IT POSSIBLE IN IRANIAN POPULATION?) and before bedtime]
50 percent as three preprandial rapid-acting insulin injections. This regimen improved glycemic control and perinatal outcome compared to a twice-daily regimen.
The titration of insulin dose to blood glucose levels is based upon SMBG
4glucose measurements each day are needed to optimize therapy and ensure a smooth increase of insulin as insulin requirements increase with pregnancy progression.
Twin gestations have an approximate doubling of the insulin requirement throughout pregnancy.
25
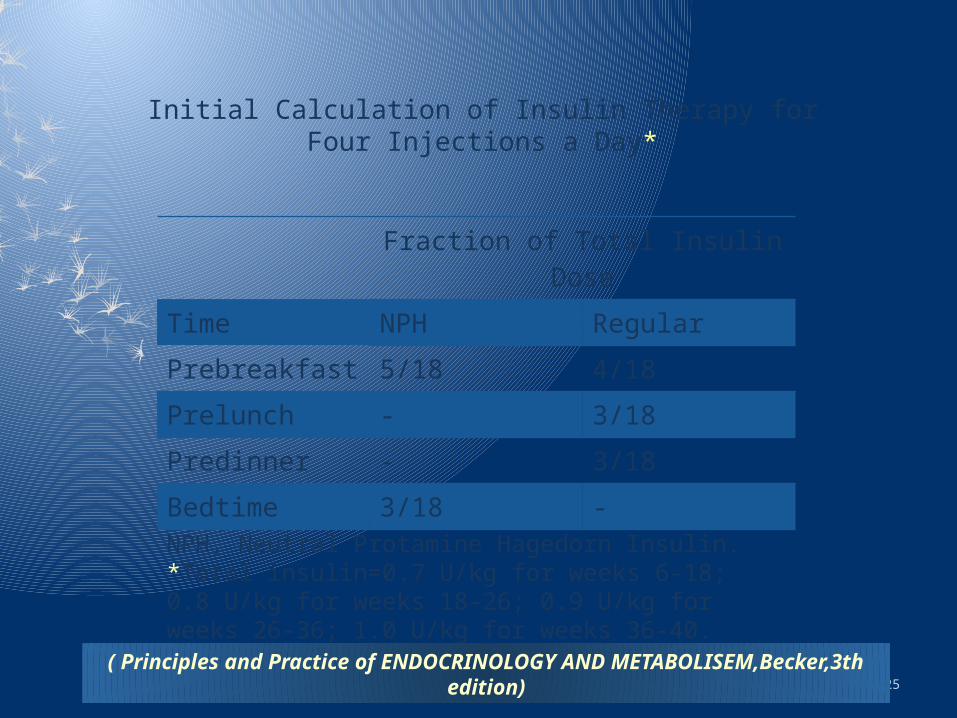
Fraction of Total Insulin Dose
Time NPH Regular
Prebreakfast 5/18 4/18
Prelunch - 3/18
Predinner - 3/18
Bedtime 3/18 -
Initial Calculation of Insulin Therapy for Four Injections a Day*
NPH, Neutral Protamine Hagedorn Insulin.*Total insulin=0.7 U/kg for weeks 6-18; 0.8 U/kg for weeks 18-26; 0.9 U/kg for weeks 26-36; 1.0 U/kg for weeks 36-40.
( Principles and Practice of ENDOCRINOLOGY AND METABOLISEM,Becker,3th edition)

26
Hypo or Hyperglycemia Acute hypoglycemia treated by administering 10 to 20 g of
carbohydrate immediately.
Use a correction factor of one unit of rapid-acting insulin lowers blood glucose by 25 mg/dL
For glucose <50 mg/dL, we subtract two units of rapid-acting insulin from the dose of insulin given before the meal
For glucose 50 to 75 mg/dL, subtract one unit from the dose of insulin given before the meal
For glucose 75 to 100 mg/dL, do not change insulin dose
For glucose 100 to 125 mg/dL, add one unit rapid-acting insulin to the dose of insulin given before the meal
For glucose 100 to 150 mg/dL, add two units rapid-acting insulin to the dose of insulin given before the meal.

27
Insulin Sensitivity Factor (ISF)
Calculates how much blood glucose decreases for each unite of bolus insulin
ISF (For human insulin)= 1500 ÷ TDD
ISF (For analogue insulin)= 1800 ÷ TDD
Example: TDD= 50 (human insulin), ISF = 1500 ÷ 50 = 30
It means that each unit of bolus decreases blood glucose by 30 mg/dl
Gabric
28
Bolus Dose Calculation
Carbohydrate counting of the meal
Number of units of carbohydrate in the meal × ICR
Example: 10 spoon of rice + 1 apple = 3 units of carbohydrate, ICR = 2.
Bolus dose required for the meal = 3 × 2 = 6 units
Gabric

29
Pre-Prandial Blood Glucose
Correction dose = Pre-prandial glucose – desired blood glucose ÷ ISF
Example: Pre-prandial glucose 230, correction dose= 230 – 130 ÷ 50 = 2
It means that 2 units of bolus are required to correct pre-parandial hyperglycemia
Total number of bolus = 6 + 2 = 8 units
Gabric

30
Type of Insulin Use of insulin preparations of low antigenicity will minimize the transplacental transport of insulin antibodies.
Human insulin is the least immunogenic
lispro, aspart, glulisine are comparable in immunogenicity to human Regular insulin, but only lispro and aspart have been investigated in pregnancy and shown to have acceptable safety profiles, minimal transfer across the placenta, and no evidence of teratogenesis.
Neonatal outcomes are similar to those of women treated with regular insulin.
These two insulin analogs both improve postprandial excursions compared to human Regular insulin and are associated with lower risk of delayed postprandial hypoglycemia.
Long-acting insulin analogs (insulin glargine, insulin detemir) have not been studied extensively in pregnancy; therefore prefer use of human NPH insulin as part of a MSI in pregnant women.

31
Oral Anti-Hyperglycemic Agents
A systematic review by the Johns Hopkins University Evidence-based Practice Center presented showed that
(1) maternal glucose levels did not differ substantially between gravidae treated with insulin versus those treated with oral glucose-lowering agents,
(2) there was no consistent evidence of an increase in any adverse maternal or neonatal outcome with use of glyburide, acarbose, or metformin compared with use of insulin
Inconsistencies in clinical outcome measures across studies and lack of data made it difficult to draw firm conclusions.
ADA and and ACOG do not endorse the use of oral anti-hyperglycemic agents during pregnancy and such therapy has not been approved by the Unites States Food and Drug Administration for treatment of GDM

32
Metformin
May "prevent" GDM since it is an OHA and would be expected to maintain euglycemia in some women who would otherwise be diagnosed with GDM.
In one study, GDM occurred in 3 percent women with PCOS taking metformin (2550 mg) compared with 23 percent not taking metformin . According to these findings, metformin would have to be given to five women with PCOS to prevent GDM in one.
No trials have directly compared metformin and glyburide in treatment of GDM.
In independent trials comparing each drug to insulin, patients using metformin were more likely to need supplemental insulin than patients using glyburide (46 versus 4 percent)

33
Metformin Appears to be an effective treatment for GDM, particularly for overweight or obese
patients.
Patients with multiple risk factors for insulin resistance may not meet treatment goals with metformin alone and will likely still require some insulin therapy.
Doses of metformin varied from study to study, ranging from 1000 mg/day to 2500 mg/day. Safety concerns (reports of hyaline membrane disease and premature births seen in the infants of women treated with metformin.)
It is not known whether these complications are due to metformin itself or poorly
controlled GDM.
In light of these concerns, insulin should remain the drug of choice if dietary measures alone fail.
Metformin, although not a first-line agent, appears to be a reasonable alternative to insulin therapy in GDM.
Further studies are needed to fully determine the role of metformin in GDM.
(The Annals of Pharmacotherapy: 2009 ,Vol. 43, No. 5, pp. 939-943).
34
Glyburide
Transplacental passage of glyburide minimal. Maternal use of glyburide was not associated with an excess of
neonatal hypoglycemia or congenital anomalies and that it was an effective treatment of GDM, particularly in women with mild to moderate degrees of hyperglycemia.
As with insulin therapy, glyburide must be carefully balanced with meals and snacks to prevent maternal hypoglycemia.
Glyburide may be less successful in obese patients or those with marked hyperglycemia earlier in pregnancy.
More research is needed to determine: (a) if maternal and neonatal outcomes with glyburide are equivalent to those obtained with insulin therapy; (b) if glyburide affects the potential postpartum progression of the woman with GDM towards imapired glucose tolerance/diabetes, or on the possibility of GDM recurrence; (c) whether glyburide affects the long-term well-being of offspring.

35
Peripartum Management
Insulin can usually be D/C during labor and delivery; an infusion of normal saline is usually sufficient to maintain normoglycemia .
Maternal hyperglycemia should be avoided during labor to prevent fetal hyperinsulinemia, fetal acidosis and subsequent neonatal hypoglycemia.
The risk of adverse metabolic outcomes (hypoglycemia, hyperbilirubinemia, hypocalcemia, erythremia) appears to increase with the degree of maternal hyperglycemia. Therefore, maternal blood glucose concentration should be maintained between 70 and 90 mg/dL .
A fasting or random blood glucose should be measured on the day after delivery to ensure that the mother no longer has hyperglycemia, using criteria established for nonpregnant individuals
Maintaining a diet low in carbohydrate content will facilitate postpartum weight loss. It suggested for continuing measurement of blood glucose intermittently at home for a few weeks after discharge from the hospital (especially if she was diagnosed early in gestation or required insulin during the pregnancy).

36
Future Risks ≥ 90 percent with GDM are normoglycemic after delivery. However, they are at risk for recurrent GDM, IGT ,IFG and overt diabetes.
1/3 to 2/3 of women with GDM will have GDM in a subsequent pregnancy.
Women who have a recurrence tend to be older, more parous, and have a greater increase in weight between their pregnancies than women without a recurrence .
Higher infant birth weight in the index pregnancy and higher maternal prepregnancy weight have also been associated with recurrent GDM.

37
Future Risks 20 % of women with GDM have IGT during the early postpartum period.
A systematic review and meta-analysis found that women with GDM were at significantly higher risk of developing subsequent type 2 diabetes than women with normoglycemic pregnancies (RR 7.43, 95% CI 4.79-11.51)
The relative risk was 4.69 within the first five years after delivery and 9.34 more than five years after delivery (BMI and WC)
.
Other major risk factors are gestational requirement for insulin and early gestational age at the time of diagnosis (ie, less than 24 weeks of gestation) ,
Autoantibodies (GAD )high FPG during pregnancy and early postpartum, higher FPG at diagnosis of GDM ,high glucose levels OGTT ,neonatal hypoglycemia, and GDM in more than one pregnancy. Parity, large birth weight, and diabetes in a first-degree relative are less correlated with later diabetes.
GDM is also a risk factor for the development of type 1 diabetes. Specific HLA alleles (DR3 or DR4) may predispose to the development of type 1 diabetes postpartum, as does the presence of islet-cell autoantibodies

38
Follow-up and Prevention of Type 2 Diabetes ACOG and ADA long term follow-up of women with GDM:
All women with previous GDM should undergo an OGTT ,6 to 12 weeks after delivery, using a two-hour 75 gram oral glucose tolerance test.
Women with NGTT should be counseled regarding their risk of developing GDM in subsequent pregnancies and type 2 diabetes in the future. Weight loss and exercise are clearly beneficial for reducing the incidence of these disorders
Long-term follow-up is essential.
Reassessment of glycemic status should be undertaken at a minimum of every three years, but the best means of follow-up has not been defined.
The 75-g OGTT is the more sensitive test in most populations, but the FPG is more convenient, specific, and reproducible, and less expensive
















![Three patients presenting with severe macrosomia and ......predictive of fetal macrosomia [12, 13]. Sardesai et al. reported the case of a fetus with fatal HCM and macrosomia. The](https://static.fdocuments.us/doc/165x107/6141240183382e045471e526/three-patients-presenting-with-severe-macrosomia-and-predictive-of-fetal.jpg)