
1 FMLA Training Part II presented by The Office of the State Employer Employee Health Management...
81
1 FMLA Training Part II presented by The Office of the State Employer Employee Health Management Toni McFarland & Contract Negotiations/Administration Cheryl Schmittdiel
-
Upload
rosamund-hopkins -
Category
Documents
-
view
213 -
download
0
Transcript of 1 FMLA Training Part II presented by The Office of the State Employer Employee Health Management...
1
FMLA Training Part II
presented by
The Office of the State Employer
Employee Health ManagementToni McFarland
&Contract Negotiations/Administration
Cheryl Schmittdiel

2
Review

3
The State of Michigan must observe employee (EE) rights under the FMLA;
The State of Michigan must observe EE rights under Collective Bargaining Agreements (CBA) and Civil Service Rules & Regulations (CSR&R) ; and
The State of Michigan cannot interpret CBA or CSR & R to diminish rights guaranteed by FMLA.
4
Employee Eligibility
Work for covered employer (ER) -- Public Agencies are covered ERs; and
Work 12 months, which need not be consecutive; and
Work at least 1,250 hours within the 12 months prior to the leave; and
Military leave counts as time worked.
5
Qualifying Events The State of Michigan (SOM) as a covered ER
must grant an eligible EE up to a total of 12 workweeks of paid/unpaid FMLA leave in a 12 month period for any of the following reasons:– for the birth of a son or daughter and to care for the
newborn;– for the placement of a child for adoption or foster care,
and to care for the newly placed child;– to care for a spouse, son, daughter, or parent with a
Serious Health Condition (SHC); and– for the EE's own SHC that makes the EE unable to
perform the essential functions of their position.

6
Employee Notification to Employer
Notice to ER may be given– In writing– Verbally– In person– By telephone– By fax machine– After the employee returns, but within two
(2) business days– By EE’s spokesperson

7
Foreseeable Leave
When need for leave is foreseeable EE notifies ER 30 days or more before leave begins
Or, as soon as practicable, but within two (2) business days of learning leave is necessary
Verbal or written notification is acceptable

8
Unforeseeable Leave
When need for leave is unforeseeable EE notifies ER as soon as practicable
Within two (2) business days of going on leave; or
Within two (2) business days of returning from leave
9
Employer Rules Any ER or department rules or
requirements regarding call in or notification when an EE cannot work are still in effect and are not relieved under the FMLA.
However, a transgression cannot serve as a basis for denial if timely notice is given.
“No call, no show” and subsequent FMLA request…

10
Employer Knows the Reason for FMLA Leave
The ER’s designation decision must be based only on information received from the EE or the EE's spokesperson (e.g., if the EE is incapacitated, the employee's spouse, adult child, parent, doctor, etc., may provide notice to the ER of the need to take FMLA leave).

11
Employer Hears It Through the “Grapevine”
If the EE tells their supervisor they are taking annual leave and that annual leave will be for an FMLA qualifying reason, then the EE has told the ER.
If the EE has told a co-worker and the co-worker tells the supervisor then the ER has not been told. However, the ER may request that the CS-1789 be filled out and returned. If the EE does not confirm the absence or fill out the paperwork the ER may not designate the leave as FMLA, and the EE has no FMLA protection.

12
FMLA, LTD and Workers’ Compensation
If an EE qualifies for an FMLA leave and the absence also qualifies for LTD or Workers’ Compensation, then all of the pertinent forms, documents, letters and notification need to be sent to the EE simultaneously.

13
Family Medical Leave ActEmployee Request
& Employer Response
Form CS-1790
14
Family Medical Leave ActEmployee Request & Employer Response
Form CS-1790

15
Employee Request
16
Employee Request

17
Employee Request
The EE is not required to use the CS-1790 to notify the ER.
If notification is made in any other manner, the ER/Supervisor/Human Resources office will complete Section I of the CS-1790 as well as Section II.

18
Employee Request
The EE need not specifically mention FMLA.
The EE must make clear the reason for the leave.
If the ER asks, the EE must provide details about the reason for leave, either for their condition or that of the EE’s family member, or the leave may not be approved.
19
Employee Request
The EE does not need to provide the diagnosis for a SHC.
ER may ask if this is a SHC. Staying home for personal problems, if
too sick to work or because a child is ill, do not trigger FMLA protection.

20
Employee Information

21
Reason for Leave Request
22
Reason for Leave Request EE must have SHC and be unable to do the
“essential functions” of the job. The ability to perform other jobs or light-duty
work is not relevant. Consecutive days refers to calendar days, not
work days, and weekends are included even if the EE is not scheduled to work.
A full or partial day absence to receive medical treatment counts as a day of incapacity.
If an EE is absent for substance abuse and is not receiving inpatient treatment or continuing treatment by a health care provider, they do not qualify for FMLA leave.

23
Reason for Leave Request Some CBA’s permit EE to certify the need to use
up to two weeks of sick leave, upon the birth of their child, prior to the beginning of any parental leave.
The time counts against the 12 weeks of FMLA. An eligible EE is entitled to a total of 12 weeks of
FMLA leave in a 12-month period. The two weeks of sick leave are deemed to be due to the serious health condition of the EE’s spouse or newborn child and are attributable to family care leave under the FMLA.
24
Notice Requirements

25
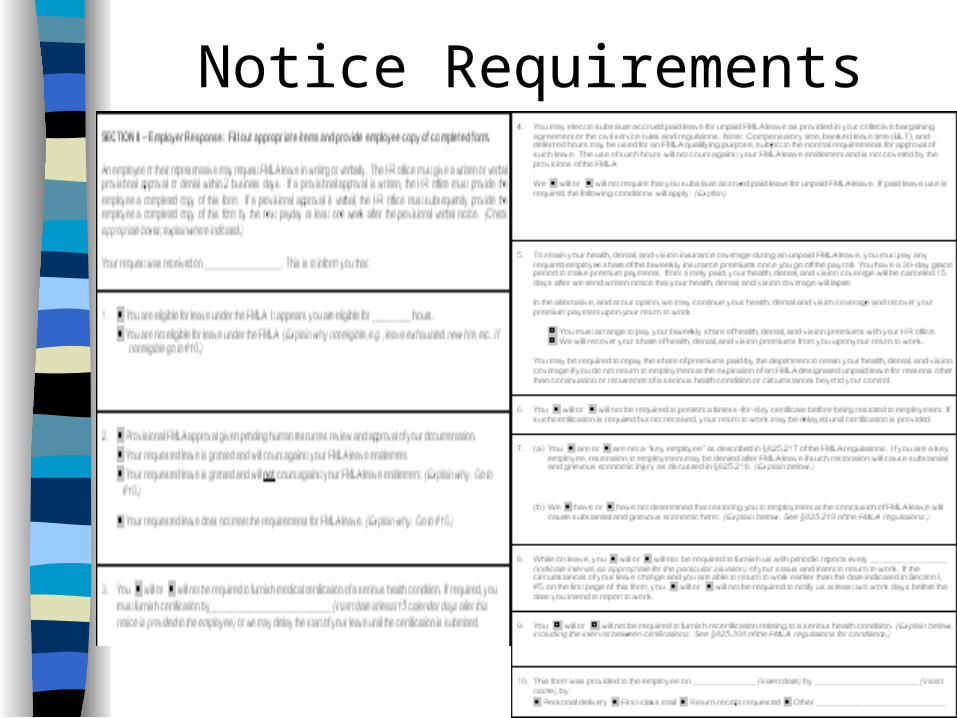
Notice Requirements “Section 301 Notice”
The CS-1790 meets the FMLA “Section 301 notice” requirements.
This form replaces the US DOL WH 381 and the need to provide the EE with Fact Sheet #28.

26
Designation Rights & Responsibilities
27
Designation Rights & Responsibilities
The ER must make a preliminary designation of whether or not the leave qualifies as FMLA leave.
The ER has a duty to “inquire further” if the ER needs additional information to determine whether a request for leave is for an FMLA qualifying reason.
ER may only inquire further of EE or EE’s spokesperson.
ER may not have direct contact with EE’s healthcare provider.
28
Eligibility/Ineligibility Notice

29
Eligibility/Ineligibility Notice
If the ER fails to notify the EE that they do not meet the eligibility requirement prior to the start of leave, when the leave is foreseeable, then the EE could be “deemed eligible” even if they do not meet the eligibility criteria.
See US DOL Opinion Letter, FMLA 2002-1.
30
Designation of FMLA Leave
31
Designation of FMLA Leave Provisional designation should be given
pending receipt of CS-1789 Medical Certification form.
If the ER fails to designate FMLA leave and the EE takes 12 weeks, then later the EE states they want to take more time, the EE must establish that they would have shortened their original leave if it had been designated FMLA.
The designation of FMLA leave must be made within two (2) business days after the EE returns to work and can be made by either the EE or the ER. If not designated within two (2) business days cannot be designated FMLA.
32
Medical Certification

33
Medical Certification
The ER must give specific notice of the need for medical certification and the consequences of failing to obtain medical certification.
The EE must be given the CS-1789 Medical Certification form within two (2) days of the EE notice of need for FMLA.
The ER may ask for only the information on the CS-1789, no greater amount of information is allowed.
34
Medical Certification cont’d
The information on the CS-1789 must relate only to SHC for which the current need for leave exists.
The EE has 15 calendar days to have the form completed and returned to the ER.
If the form is incomplete the ER may ask the EE for clarification.
Any charges associated with completing the form are the EE’s responsibility.
35
Paid or Unpaid Leave

36
Paid or Unpaid Leave An employee may elect to use accrued sick,
annual or personal leave, as appropriate, in place of an unpaid FMLA leave.
If the EE fails to designate sick, annual or personal leave for an unpaid leave, the ER may require the use of appropriate accrued leave before allowing an unpaid leave.
The EE must be informed within two (2) business days of giving FMLA notice that the paid leave will be imposed except where the ER does not have sufficient information to make an FMLA designation.

37
Group Health Benefits

38
Group Health Benefits Group Health Benefits (health, dental
and vision) must be maintained during FMLA leave.
EEs make arrangements with their Human Resources Office to pay their bi-weekly premium share.
If an EE is laid off or their limited term appointment expires during an FMLA leave, the ER can stop paying for the EE’s health insurance.
39
Fitness for Duty Certification
40
Fitness for Duty Certification This certification must be required uniformly for
all similarly-situated EEs. The certification can be as simple as a
statement that the EE is able to return to work. There is no fitness-for-duty certification for
intermittent leave. The ER cannot contest the fitness-for-duty
certification through second and third opinions. The EE may be terminated if the fitness-for-
duty certification is not provided and notice was given of the requirement.

41
Fitness for Duty Certification If a CBA permits ER to require an EE to have
a medical examination, notice of this requirement must be given to an EE when leave is requested or shortly after leave is requested.
The medical examination must be to determine whether:– The EE’s ability to perform the essential job
functions is impaired by a medical condition; or
– The EE poses a direct threat to other EEs due to a medical condition.

42
“Key Employee”

43
“Key Employee”
The “Key EE” exemption is very rare. It applies only to high-salaried (must be in the
highest 10% of all EEs for the ER) EEs whose reinstatement after a leave would cause the ER substantial and grievous economic injury.
A “Key EE” may not be denied the right to take FMLA leave if the EE is eligible and the FMLA leave is properly designated, but can be denied reinstatement if properly noticed of “Key EE” designation.

44
Periodic Report &Intent to Return

45
Periodic Report &Intent to Return
An ER may require an EE on FMLA leave to report periodically on the EE’s status and intent to return to work.
If there is a change in the EE’s circumstances that will allow them to return to work earlier, or will need to extend their leave, they are required to notify the ER within two (2) business days of the change in their circumstances.
If an EE gives unequivocal notice of intent not to return to work, the ER’s obligations under FMLA to maintain health benefits and to restore the EE cease unless the EE will not be returning due to a continuation of a SHC.

46
Periodic Report &Intent to Return
A returning EE is entitled to any unconditional pay increases that occurred during the leave, unless the pay increases are dependent on seniority, work performed or length of service.
If an EE is no longer qualified for their position because they have not renewed a license, attended a necessary course, flown a minimum number of hours due to the FMLA leave, the EE must be given a “reasonable opportunity” to fulfill those conditions upon their return to work.

47
Periodic Report &Intent to Return
An equivalent position must have the same pay, benefits, working conditions and must also have substantially similar duties and responsibilities, authority, skill and effort.
The returning EE is not entitled to any more preferential treatment,(e.g., if the EE’s position is eliminated due to a reduction in force or a limited term appointment has expired) than they would have had if they had been at work.
An EE may be terminated while on FMLA leave if the EE would have been terminated absent their leave.

48
Re-certification
49
Re-certification For pregnancy, chronic, or permanent/long
term conditions under continuing supervision of a health care provider the ER may request re-certification no more often than every 30 days and only in connection with an absence unless:– Circumstances described in the previous
certification have changed (change in severity of the condition or frequency of absences).
– The ER receives information that casts doubt on the reason for the EE’s absence.

50
Re-certification If the minimum period of continuous incapacity
on the previous certification is more than 30 days, the ER may not request re-certification (this also applies to intermittent leave and leave taken for treatment) during the designated period unless:– The EE requests an extension of leave.– Circumstances described in the previous
certification have changed (change in severity of the condition or frequency of absences).
– The ER receives information that casts doubt on the reason for the EE’s absence.
51
Re-certification The EE must provide the requested re-
certification to the ER within the timeframe requested by the ER but not less than 15 days from the date of the request.
Any expenses associated with the re-certification are the EE’s responsibility.
No second or third opinion on re-certification may be required.

52
Return to Employee

53
Return to Employee The ER must provide a verbal or written
approval or denial to the EE within two business days. If approval is given verbally the ER must subsequently provide the EE with a copy of this completed form by the next payday which is at least one (1) week after the verbal notice.
Documentation should be made on the form as to the date, sender and how this form was provided to the EE.
This form meets the US DOL “Section 301 notice” requirements.

54
Certification of Health Care ProviderForm CS-1789
55
Certification of Health Care ProviderForm CS-1789 cont’d.
56
Serious Health Condition

57
Serious Health Condition Considered a SHC are examinations to
determine if a SHC condition exists and evaluations of the condition.
Treatment does not include routine physical examinations, eye examinations, or dental examinations.
A regimen of continuing treatment that includes the taking of over-the-counter medications such as aspirin, antihistamines, or salves; or bed-rest, drinking fluids, exercise, and other similar activities that can be initiated without a visit to a health care provider, is not, by itself, sufficient to constitute a regimen of continuing treatment for purposes of FMLA leave.

58
Serious Health Condition cont’d Conditions for which cosmetic treatments
are administered (such as most treatments for acne or plastic surgery) are not ''SHCs'' unless inpatient hospital care is required or unless complications develop.
Ordinarily, even if the absence is three (3) days or more, unless complications arise, the common cold, the flu, ear aches, upset stomach, minor ulcers, headaches other than migraine, routine dental or orthodontia problems, periodontal disease, etc., are examples of conditions that do not meet the definition of a serious health condition and do not qualify for FMLA leave.
59
Medical Facts

60
Medical Facts “Medical facts” do not include a diagnosis. An EE who must be absent from work to
receive medical treatment for a SHC is considered to be unable to perform the “essential functions” of the position during the absence for treatment.
An ER has the option of providing a statement, or a copy of the EE’s PD, showing the “essential functions” of the EE’s position for the health care provider to review.
If the ER does not provide the “essential functions”, the health care provider will ask the EE.
61
Medical Facts cont’d An EE is ''needed to care for'' a family
member encompasses both physical and psychological care. It includes situations where a family member is unable to care for their own basic medical, hygienic, or nutritional needs or safety, or is unable to transport themself to the doctor. This also includes providing psychological comfort and reassurance which would be beneficial to a child, spouse or parent with a SHC who is receiving inpatient or home care.

62
Duration of Incapacity

63
Duration of Incapacity
A period of incapacity of more than three (3) consecutive days (including any subsequent treatment or period of incapacity related to the same condition), that also involves:– Treatment two (2) or more times by a health
care provider or under the direction of a health care provider; or
– Treatment by a health care provider on at least one occasion which results in a regimen of continuing treatment that is under the supervision of the health care provider.

64
Treatment Frequency

65
Treatment Frequency Any period of absences to receive multiple
treatments (including any period of recovery therefrom) by a health care provider or services under the supervision of a health care provider (chemotherapy, radiation treatment, physical therapy, dialysis).
Any illness or injury that if left untreated would result in an incapacity of three (3) or more days (e.g., cancer, arthritis, and kidney disease, etc).
The EE or their family member must be under the supervision of a health care provider even if they are not in active treatment, e.g., Alzheimer’s, severe stroke or terminal stages of a disease.

66
Absence from Work

67
Absence from Work A chronic condition requires
– Periodic visits for treatment by a health care provider or treatment under the direction of a health care provider; and
– Continues over an extended period of time (including recurring episodes of a single underlying condition); and
– May cause episodic rather than a continuing period of incapacity (e.g., asthma, diabetes, epilepsy, etc.).

68
Care for Family Member

69
Care for Family Member The ER may request a medical certification
verifying that the family member has a SHC and needs care. If the ER has reason to doubt the medical certification it may schedule the family member for a second-opinion at the ER’s expense.
Care is needed if the family member is unable to provide his or her medical, hygienic, nutritional, safety, or transportation needs.
Care includes preparing meals, driving to medical appointments, changing dressings and supplying psychological comfort and reassurance.
70
Healthcare Provider
71
Healthcare Provider A SHC must be treated or supervised by a health
care provider qualified to practice in the area of the SHC.
Health care providers include: Physicians, Optometrists, Osteopaths, Chiropractors (when manipulating the spine to correct subluxation), Podiatrists, Dentists, Clinical Psychologist, Christian Science practitioners, Nurse practitioners, Nurse Midwives, and Clinical Social Workers ( if authorized under state law to diagnose and treat SHC without supervision), other providers recognized by the ER or the group health plan as qualified to substantiate a claim for health benefits (e.g., Acupuncturist).
72
Employee’s Statement
73
Employee’s Statement
The EE must state what care they will provide to a family member.
The EE must state the duration and frequency of the stated care they will be providing.
The care, frequency and duration must match the care, frequency and duration outlined by the health care provider.

74
Definitions
75
Clarification If the ER determines the medical certification is
incomplete, the ER must notify the EE and give the EE “a reasonable opportunity to cure any deficiency.”
The ER cannot request information not asked for on the CS-1789, the ER can only seek authentication or clarification of the medical certification.
The ER cannot have their health care professional make any contact with the EE’s health care provider unless the EE’s permission is obtained.
76
Second & Third Opinion The ER may require a second opinion
when there is reason to doubt the accuracy of the Medical Certification.
If the second provider’s report conflicts with the first report, then a third opinion must be obtained.The two providers must agree on a third provider and the third provider’s opinion is binding.
Second and third opinions are at the ER’s expense.

77
QUESTIONS &
ANSWERS
78
ENFORCEMENT
Complaints - Wage and Hour - ER Policy Review.
Litigation - DOL or private attorney. Remedies - wages/employment lost:
– monetary loss for providing care– reasonable legal and witness fees
Private right of action. 2 year statute of limitation.
79
CONTACT INFORMATION
Toni McFarland, DMB/OSE/EHM– (517) 33-54274, – [email protected]
Cheryl Schmittdiel, DMB/OSE/CNA– (517) 37-37400– [email protected]

80
RESOURCES The FMLA Handbook: A Union Guide to the Family
and Medical Leave Act, Second Edition, Robert M. Schwartz
A Medical/FMLA Leave Checklist: Emerging Issues and How to Comply with the FMLA and the ADA, David B. Calzone, Vercruysse Murray & Calzone
The Family Medical Leave Act of 1993: Federal Regulations, Part 825: Title 29, Part 825 of the Code of Federal Regulations
FMLA Resource Manual, Complete Text of FMLA and Applicable Federal Regulations, Council on Education in Management

81
Thank You!


















