
1 Emergence of Carbapenem-Resistant Klebsiella pneumoniae in an Acute Care Facility and the...
23
1 Emergence of Carbapenem- Resistant Klebsiella pneumoniae in an Acute Care Facility and the Potential Risk of Inter-Healthcare Facility Transmission Dawn Terashita MD, MPH Acute Communicable Disease Control Los Angeles County Department of Public Health
-
Upload
curtis-baker -
Category
Documents
-
view
221 -
download
0
Transcript of 1 Emergence of Carbapenem-Resistant Klebsiella pneumoniae in an Acute Care Facility and the...
1
Emergence of Carbapenem-Resistant Klebsiella pneumoniae in an Acute Care Facility and the Potential Risk of Inter-
Healthcare Facility Transmission
Dawn Terashita MD, MPH
Acute Communicable Disease Control
Los Angeles County Department of Public Health

Background
• Carbapenems treat severe infections of ESBL gram-negative pathogens
• Resistance to carbapenems evolved in Enterobacteriaceae
• CRKP has become the most common species of carbapenem-resistant Enterobacteriaceae
• CRKP has rapidly emerged as a new threat in public health
2Kochar Infect Control Hosp Epidemiol 2009Jacoby N Engl J Med 2005Falagas J Antimicrob Chemother 2007
3
Background
• CRKP 1st identified in NC hospital (1999)• Infrequently isolated until 2001
– Several extended outbreaks in NY, NJ
• In 2007, 8% of all Klebsiella isolates were CRKP, compared with fewer than 1% in 2000
• Reported in many states and countries
Background
•In October 2007, LAC began receiving occasional CRKP reports from hospitals
•Sporadic reports continued, mainly to facilitate confirmatory testing for carbapenem resistance
•In October 2009, LAC was notified of a cluster of cases by facility A
4

Objectives
• To describe the acute emergence of CRKP in an acute care facility
• To illustrate the potential risks of inter-healthcare facility transmission
5

Setting
• Non-profit, acute care healthcare institution providing a full range of medical services with approximately 400 licensed beds
• Mean daily census is approximately 300 patients (78% occupancy)
• Average of length of hospital stay is 8 days
6

7
Methods
• Clinical and Laboratory Standards Institute (CLSI) interpretive criteria for carbapenem resistance in Klebsiella isolates
• CDC National Healthcare Safety Network (NHSN) MDRO LabID module definitions used to identify new/recurrent cases
• Case definition: patient in Facility A with CRKP positive culture that meets above criteria
Methods
• New case: CRKP culture with no prior positive in previous 28 days
• Recurrent case: subsequent CRKP culture occurring 14–28 days after initial positive
• Duplicate cases: subsequent CRKP culture occurring 0–14 days after initial positive (excluded from study)
8

Methods
• Healthcare onset (HO): specimen collected ≥ 4 days after admission
• Community onset (CO): specimen collected ≤ 3 days after admission
9
Methods
• Conducted retrospective case finding by reviewing laboratory records from facility A
• Reviewed medical records for all cases identified for data including:– Demographics– Lab reports (including susceptibilities)– Disposition
• Available isolates sent to LAC PHL for PFGE
10

Results
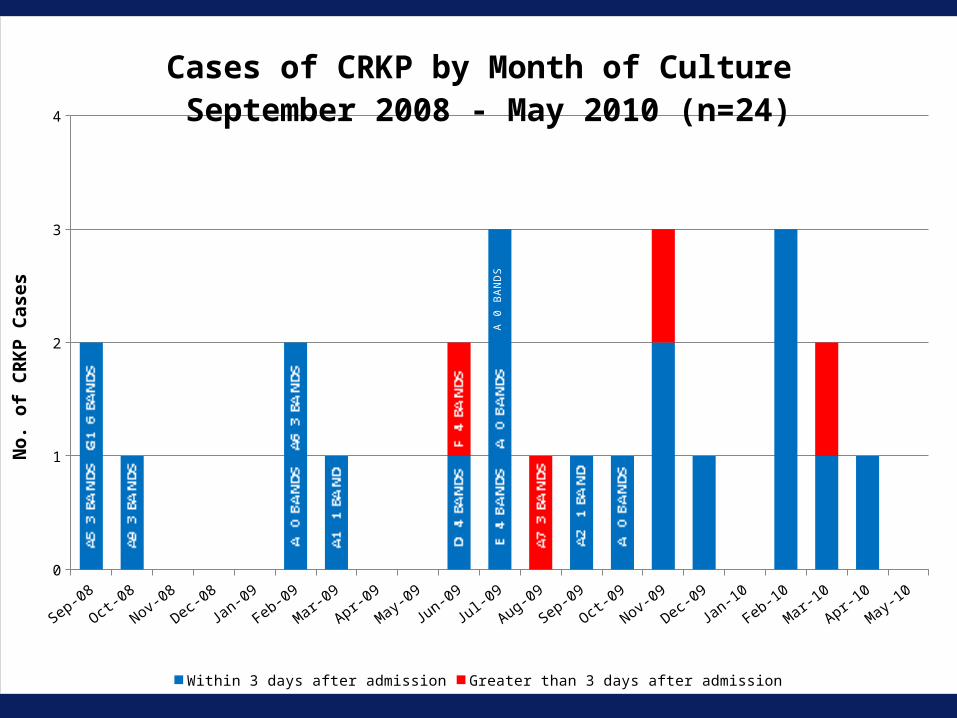
• From September 2008 through May 2010– 25 CRKP specimens from 24 patients
• Prior to September 2008 there were no CRKP isolates identified
11
12
Sep-08
Oct-08
Nov-08
Dec-08
Jan-09
Feb-09
Mar-09
Apr-09
May-09
Jun-09
Jul-0
9
Aug-09
Sep-09
Oct-09
Nov-09
Dec-09
Jan-10
Feb-10
Mar-10
Apr-10
May-100
1
2
3
4
Cases of CRKP by Month of Culture September 2008 - May 2010 (n=24)
Within 3 days after admission Greater than 3 days after admission
No.
of
CR
KP
Cas
es
A 0
BA
ND
S

13
Age (years) NumberRange 45-91Median 61.5Mean 65
Sex
Female 13 (54%)Male 11 (46%)
Outcome
Recovered 23 (96%)Died 1 (4%)
Acquisition (n=20)
Community onset 16 (80%)Hospital onset 4 (20%)
Results: Demographic and Clinical (n=24)

14
Admitted from (n=20 cases)SNF 13 (65%)Home 5 (25%)LTAC 2 (10%)
Previous healthcare exposure – admitted from home4 discharged from hospitals within previous 30 days2 discharged from the same LTAC – hospitalizations did not overlap3 had interaction with Facility A in previous 2 months1 had no previous healthcare exposure
Results: Previous Healthcare Exposure
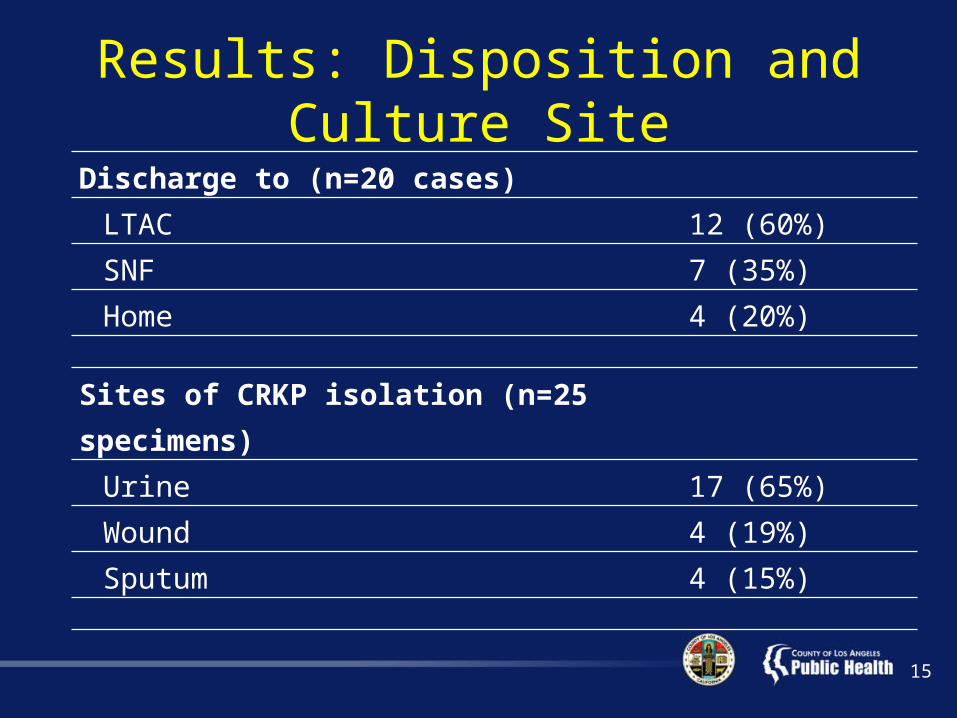
Results: Disposition and Culture Site
15
Discharge to (n=20 cases)LTAC 12 (60%)SNF 7 (35%)Home 4 (20%)
Sites of CRKP isolation (n=25 specimens) Urine 17 (65%)Wound 4 (19%)Sputum 4 (15%)
Lab Results: Pulsed Field Gel Electrophoresis (PFGE) (n=14)
• Eleven different strain genotypes– Four patients have > 3 band differences– Six patients have 1-3 band differences– Four patients share the same strain type (0 band
difference)
• No common risks were identified• Two HO cases tested had unique PFGE
patterns
16

Lab Results: Antimicrobial Susceptibility
Performed on 25 isolates from 24 patients, all resistant to:
1. Cefazolin
2. Ceftazidime
3. Ceftriaxone,
4. Cefepime
5. Ampicillin
6. Ampicillin/sulbactam
7. Piperacillin-tazobactam
8. Levofloxacin
9. Tobramycin
17
Lab Results: Antimicrobial Susceptibility
• Seventeen of 20 isolates (85%) susceptible to tigecycline
• Four of 25 isolates (16%) susceptible to gentamicin
• One of 21 (5%) isolates susceptible to amikacin
• One isolate was tested for colistin and was susceptible
18
Discussion
• Multiple CRKP strains appear in facility A– No common risks in those with same PFGE
• 80% of cases are defined as community onset• Patients (96%) were admitted from other
healthcare facilities around the community• Patients (83%) were discharged to another
healthcare facility• Potential risks of inter-healthcare facility
transmission 19

Discussion
• Potential risks of inter-healthcare facility transmission
• Perhaps represents a higher than expected prevalence in the county
20

Limitations
• Unable to trace back patient location beyond place of admit
• Inconsistent testing for susceptibility to carbapenems
• True prevalence in county unknown
21
Conclusion
• Cluster was not a hospital outbreak• Undetected patients with CRKP pose considerable
risk of transmission between healthcare facilities• Heightened awareness is needed• Emphasize transfer reporting between healthcare
facilities• CRKP surveillance by public health to monitor the
prevalence/trends in the community and identify outbreaks
22

Acknowledgements
• May Mei-Sheng Riley• L’Tanya English• Patricia Marquez• Sheena Chu• Ron Jackson• Laurene Mascola• Robert Kim-Farley• David Dassey
• Chart review team:– Kim Bryant– Merle Baron– Lorraine Sisneros– Sovirny Norng– Rosie Vasquez
23









![NICU Database Appendices - CPQCC NICU Appendices.pdf2020 NICU Appendices| 4 1101 [K. oxytoca, K. pneumoniae and others] including Carbapenem-resistant Klebsiella and Cephalosporin-resistant](https://static.fdocuments.us/doc/165x107/5f0e96fb7e708231d43ff847/nicu-database-appendices-cpqcc-nicu-2020-nicu-appendices-4-1101-k-oxytoca.jpg)








