
1 Drug Resistant Streptococcus pneumoniae. 2 “… the microbes are educated to resist penicillin...
35
1 Drug Resistant Streptococcus pneumoniae
-
Upload
sharon-haynes -
Category
Documents
-
view
216 -
download
0
Transcript of 1 Drug Resistant Streptococcus pneumoniae. 2 “… the microbes are educated to resist penicillin...
1
Drug Resistant Streptococcus pneumoniae

2
“… the microbes are educated to resist penicillin and a host of penicillin-fast organisms is bred out which can be passed on to other individuals and perhaps from there to others until they reach someone who gets a
septicemia or a pneumonia which penicillin cannot save. In such cases the thoughtless person playing with penicillin treatment is morally responsible for the death of the man who finally succumbs to infection with the penicillin-resistant organism. I hope this evil can be averted.” Sir Alexander Fleming,
New York Times, June 26, 1945
3
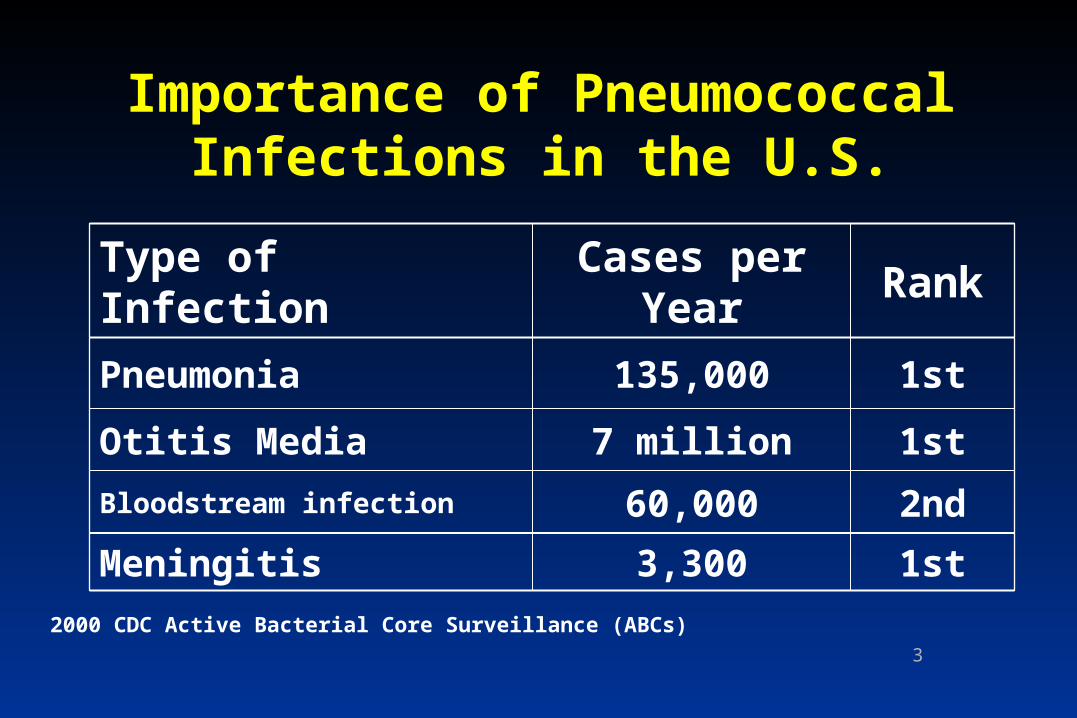
Importance of Pneumococcal Infections in the U.S.
1st3,300Meningitis
2nd60,000Bloodstream infection
1st7 millionOtitis Media
1st135,000Pneumonia
RankCases per
YearType of Infection
2000 CDC Active Bacterial Core Surveillance (ABCs)

4
Drug ResistantStreptococcus pneumoniae
• Emerged in Spain and South Africa
• Emerged in the U.S. in the last decade
• Use of antibiotics for viral infections
• Threatening use of antibiotics for common infections
5
Resistance and AntibioticPrescribing
• Risk factors for resistant S. pneumoniae are:– young age (< 1 year)– higher socioeconomic status– day-care attendance– recent receipt of antibiotics (2-5 times greater
risk)
Pediatrics 1993;92:761-7.

6
Pneumococcal Carriage in Day Care Center Outbreak, East
Tennessee, 1996
05
101520253035404550
MDRSP Serotype 14 Other Serotypes
Per
cent
car
rier
s
DCC-ADCC-BDCC-CPediatrics practice
Craig, Clin Infect Dis 1999;29:1257-1264
7
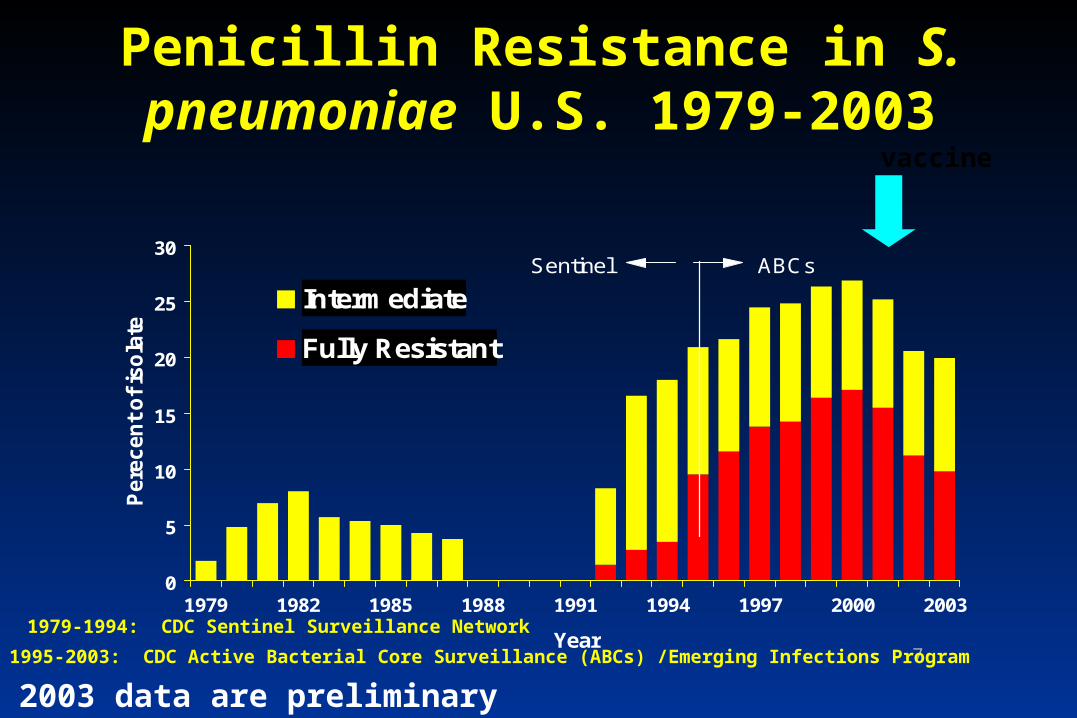
Penicillin Resistance in S. pneumoniae U.S. 1979-2003
0
5
10
15
20
25
30
1979 1982 1985 1988 1991 1994 1997 2000 2003
Year
Pere
cen
t o
f is
ola
tes Intermediate
Fully Resistant
1979-1994: CDC Sentinel Surveillance Network
1995-2003: CDC Active Bacterial Core Surveillance (ABCs) /Emerging Infections Program
Sentinel ABCs
vaccine
2003 data are preliminary

8
0102030
Pen Ery Oflox /Levo
Tet
Antibiotic
Per
cen
t
no
nsu
scep
tib
le
1995 1996 1997 1998 1999 2000
CDC Active Bacterial Core Surveillance (ABCs)
Trends in Pneumococcal Susceptibility, U.S, 1995-2000

9
0%
10%
20%
30%
40%
50%
60%1999
2000
2001
2002
2003
1999
2000
2001
2002
2003
1999
2000
2001
2002
2003
1999
2000
2001
2002
2003
Davidson Hamilton Knox Shelby
Invasive Pneumococcal Disease, Proportion of Non-susceptible Isolates,
Tennessee, 1999-2003
10
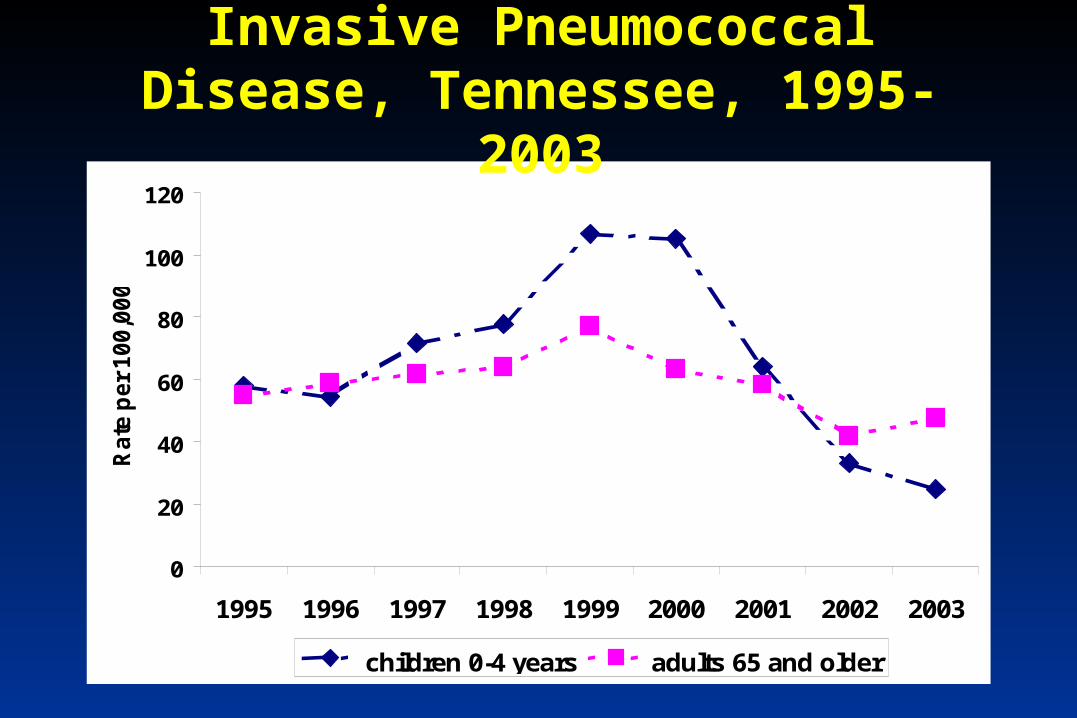
0
20
40
60
80
100
120
1995 1996 1997 1998 1999 2000 2001 2002 2003
Rate
per
100,0
00)
children 0-4 years adults 65 and older
Invasive Pneumococcal Disease, Tennessee, 1995-2003
11
• NAMCS data (1992):– Antibiotics 2nd leading class of Rx in the US
• most for RTI(JAMA 1995;273:214-19)
• Antibiotic use in children: – URI: 44%– Colds: 46%
– Bronchitis: 75% (JAMA 1998;279:875-77)
Evidence of Excessive Antibiotic Use in the US

12
• NAMCS data (2000): Children < 15– Population-based antibiotic prescriptions
• decreased 40%
– Visit-based antibiotic prescriptions • decreased 29%
– Declines coincide with increased media attention
– Antibiotic resistance has continued to increase through the 1990’s
(JAMA 2002;287:3096-3102)
UPDATE!
13
Antibiotic use in Tennessee
• In 2002, TN had the highest prescription rates in the country.
Novartis Pharmacy Benefit Report: 2002 Facts and Figures.
• In 2001, Tennessee’s utilization rates for -Penicillins,
-Cephalosporins
-Trimethoprims
were over 20% higher than the national average.Novartis Pharmacy Benefit Report: 2001 Facts and Figures.

14
Oral Antibiotic Prescriptions, Knox County, 1996-1999
0
20
40
60
80
100
120
140
160
180
200
Knox Davidson Hamilton Shelby
Rate
per
100 P
ati
en
t-years
Year 1 Year 2 Year 3
Perz, JAMA 2002;287:3103-3109

15
Changes in Prescribing From Year 1 to Year 3, per Child-year

16
Ratio of Prescriptions : URI Visits, Knox County, 1996-1999
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
1.3
Knox Davidson Hamilton Shelby
Rati
o
Year 1 Year 2 Year 3
17
Patient Concerns• want clear explanation• green nasal discharge• need to return to
work/child care
Physician Concerns• patient expects
antibiotic• diagnostic uncertainty• time pressure
Barden, Clin Pediatric 1998;37:665-672
Antibiotic Prescription
Reasons for Antibiotic Use: Conclusions from 8 Focus Groups

18
Hamm, J Fam Pract 1996;43:56Mangione-Smith, Pediatrics 1999;103:711-8
Satisfaction predicted by:
– time spent by MD explaining illness
– patient understanding of treatment choice
Satisfaction not predicted by receipt of antibiotics
Patient Satisfaction and Antibiotics

19
• Public health campaign in Iceland following dramatic increase in the rates of penicillin-resistant pneumococci from 2.3% to 20% in 4 years
• Rates fell from peak of 20% in 1993 to 16.9% in 1994
• Carriage rates of resistant strains among day care attendees dropped from 20% to 15% in same period
JAMA 1996;275;175
Can Resistance Trends Be Reversed?

20
• Episodes of otitis media should be classified as acute otitis media (AOM) or otitis media with effusion (OME)
• Antibiotics are not indicated for initial treatment of OME
Principles of Judicious Antimicrobial Use:
Otitis Media - Key Messages

21
Principles of Judicious Antimicrobial Use:
Rhinitis and Sinusitis- Key Messages
• Rhinitis:– antibiotics should not be given for viral
rhinosinusitis • Sinusitis:
– prolonged URI symptoms– more severe URI symptoms (i.e. facial swelling,
high fever)– antibiotic treatment with the most narrow-
spectrum agent
22
Principles of Judicious Antimicrobial Use:
Pharyngitis- Key Messages
• Diagnose as group A strep
• Penicillin is the drug of choice in treating group A strep– use erthromycin if penicillin allergic

23
Principles of Judicious Antimicrobial Use:
Cough and Bronchitis- Key Messages
• Cough/bronchitis rarely needs antibiotics
• Antibiotic treatment for prolonged cough (>10 days) may be needed– Mycoplasma pneumonia- use macrolide agent
for children >5
24
• 23-valent polysaccharide vaccine (PPV)– ~60% effective in preventing bacteremic
pneumococcal infection in immunocompetent adults
• 7-valent conjugate vaccine (PCV-7) for children age 3 -59 months– >95% effective in preventing invasive
disease in young children
Bartlett, Clin Infect Dis 2000;31:347-382CDC, MMWR 2000;49(RR-9):1-34
Prevention - Pneumococcal Vaccination

25
8.415.5
59.1
93.7
0102030405060708090
100
1 2 3+ 3+ HiB
Number of doses
Vac
cin
e co
vera
ge,
%
National Immunization Survey, Q3/2002-Q2/2003
83.7
Receipt of PCV7 Among Children 19-35 Months, U.S, 2002-2003
26
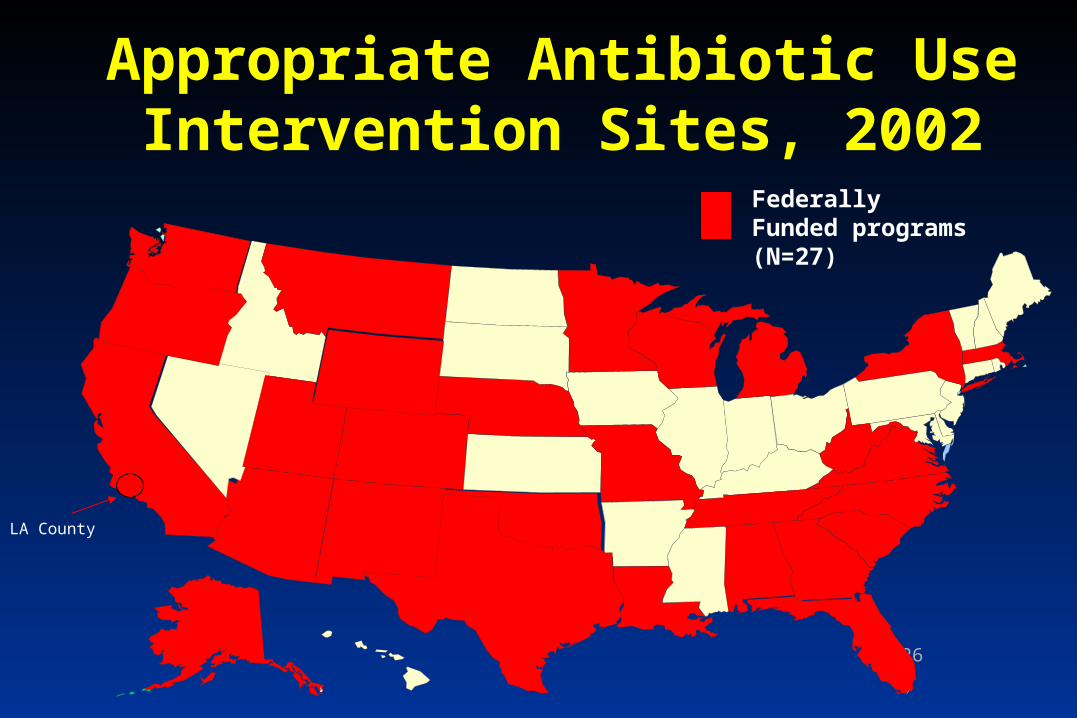
Appropriate Antibiotic Use Intervention Sites, 2002
LA County
Federally Funded programs (N=27)
27
• Mission– To reduce inappropriate antibiotic use and the
spread of antibiotic-resistant bacteria that cause many upper respiratory illnesses through state and local partnerships
Tennessee’sAppropriate Antibiotic Use
Campaign
28
TAAUC History• Created in the Spring of 2002 in response to TN’s
high levels of antibiotic resistance
• 2002-2003: Began developing partnerships and focused on educating health care providers and parents and relaying the program’s key messages
• 2003-2004: Continued Year 1 activities, developed a coalition and partnerships, developed and produced program materials, and began media campaign development
• 2004-2005: Continuing Year 1 and Year 2 activities, program expansion, development, etc.

29
Campaign Goals
Reduce inappropriate antibiotic use and the prevalence of antibiotic resistance in Tennessee by:
• Increasing parental knowledge of appropriate antibiotic use
• Changing practitioner’s antibiotic prescribing behavior
• Increasing community awareness of appropriate
antibiotic use and resistance
30
TAAUC Partners
Knox County Health
Dept.
Metropolitan Health
Dept. of Nashville and
Davidson County
East TN Regional Office
St. Thomas Hospital
East Tennessee
Children’s Hospital
Bristol-Myers Squibb
University of TN
Medical Center
Vanderbilt University
Knox County Schools
Vanderbilt Health Plan
• Blue Cross Blue
Shield of TN
• Nashville Academy of
Medicine
• Shaller Anderson of
TN
• John Deer Health
• TN Pharmacists
Association
• UT Medical Center
• GlaxoSmithKline
• Abbott Laboratories
• TN Academy of Family
Physicians
• Pfizer
• Xantus
• Daiichi
• Bayer
• Roche
• TennCare
• Head Start
• Lamar Outdoor Advertising
• American Academy of
Pediatrics (TN Unit)
• TN Radio Network

31
Program Components
• Provider Education
• Parent/Childcare Center Education
• Public Education

32
TAAUC Billboard

33
• Increasing antibiotic resistance threatens success of antibiotic treatment for common infections
• Many consumers use antibiotics inappropriately
• Decreased antibiotic use has been shown to reverse antibiotic resistant trends
• Physician and public education: principles of appropriate use, educational materials, presentations & mass media
Conclusions

34

35
CDC Treatment Guidelines
www.cdc.gov/drugresistance/community/technical.htm
TAAUC Website
www.tennessee.gov/health


















