

1 dr mario sideri
72
HPV NATURAL HISTORY AND HPV TESTING Mario Sideri Unità Ginecologia Preventiva Istituto Europeo di Oncologia, Milano Italian HPV Study Group (IHSG)
-
Upload
tariq-mohammed -
Category
Science
-
view
257 -
download
1
description
ALL
Transcript of 1 dr mario sideri

HPV NATURAL HISTORY AND HPV
TESTING
Mario SideriUnità Ginecologia Preventiva
Istituto Europeo di Oncologia, Milano
Italian HPV Study Group (IHSG)
What’s new?
In the last 30 years the causal association
between HPV infection and cervical cancer
has been demonstrated
papillomavirus

The Nobel Prize in Physiology or Medicine 2008
Harald Zur Hausen for his discovery of human
Papilloma viruses causing cervical cancer

Vaccination Population at
risk (screening)
Detection & Intervention
(pre-cancer elimination)
OLD STRATEGYNEW STRATEGY
Papillomavirus is known from decades.
However only in the recent years we have
recognized the wide diffusion and the benign
meaning of HPV infection
What is HPV?

Human Papillomavirus

Papillomavirus are species specific viruses
HPV are very common viruses and are present in almost all the species of mammalians and birds
More than 100 HPV types have beendescribed in humans
Human PV infect the skin and mucousmembranes where they can cause typicalbenign proliferations as warts and papillomas
Papillomavirus
De Villiers et al., Virology (2004)
HPV infection causes in some instances microproliferations not visiblewith the naked eye
HPV tends to prersist for long periodsof time, often as latent infection
Some HPV associated lesions can evolve into malignant neoplasia
Papillomavirus
De Villiers et al., Virology (2004)

HPV Infection
Langerhans
cells
Dendritic
cellsDermis
Micro-wound
Epidermis
Draining lymphatics
Basementmembrane
CD 16

90% of young women acquires the virus with the beginning of sexual intercourses
Most of them become negative after 6-18 months of transient infection
Only about 10% of young women become persistently infected with HPV for a longer period of time
HPV natural history
less than 30% of persitently infected women develops a CIN lesion
the vast majority of CIN clears spontaneously
some CIN persist, but even most of persistent CIN3 will never become cancer
HPV natural history
In this way, the almost ubiquitary HPV
infection, very rarely ends up into cervical
cancer.
Conversely, the association of HPV
infection with cervical cancer offers unique
opportunities of cancer prevention
HPV and Cervical Cancer

553 college students (mean age 19)
HPV test and pap smear every 4 months for 5 years
mean follow up 41.2 months
HPV natural history:Seattle Study
Winer et al., Am J Epidemiol (2003)

19.7% was HPV DNA positive at enrollment
During two years follow up 39% of women negative at enrollment became HPV DNA positive
High risk HPV were found more frequently, types 16,18,51,56,33,35,39
Winer et al., Am J Epidemiol (2003)
HPV natural history:Seattle Study

Winer et al., Am J Epidemiol (2003)
60 adolescents (14-17) were followed for a mean time of 26 months
Every three months were evaluated for HPV infection
In addition a weekly self sampling for HPV was performed for a time lenght up to 15 weeks
Brown et al., J Infect Dis (2005)
HPV natural history:Adolescent study
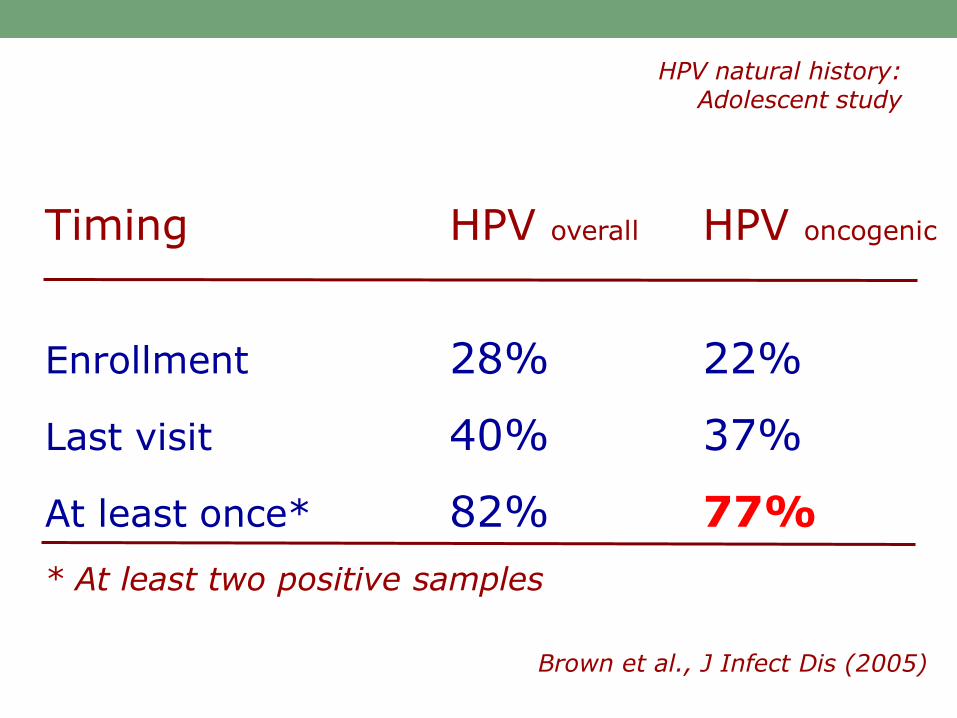
Timing HPV overall HPV oncogenic
Enrollment 28% 22%
Last visit 40% 37%
At least once* 82% 77%
Brown et al., J Infect Dis (2005)
* At least two positive samples
HPV natural history:Adolescent study

Only 3 girls were always negative to vaginal HPV testing
All referred to be virgins
Brown et al., J Infect Dis (2005)
HPV natural history:Adolescent study
HPV detectability rarely persist for more than 24 months
in more than 90% of the cases HPV becomes undetectable within 24 months
HPVNatural history

Detectable HPV
Author Age 6 12 24
__________________________________
Woodman 20 24 4 <1
Mosicki 20 50 30 10
Ho 20 30 9
% persistent HPV infection in months

persistent HPV infection may cause the development of invasive cervical cancer in 10 to 15 years
many known and unknown co-factors are responsible for cancer develpoment
HPVNatural history

20.817 women with neagtive cytology at baseline
HPV test at enrollement
Follow up for 10 years; endpoint CIN2-3 development
Natural history of HPV oncogenesisPortland study
Kahn et al., JNCI (2005)

0%
5%
10%
15%
20%
25%
0,0 4,5 15,0 27,0 39,0 51,0 63,0 75,0 87,0 99,0 111,0 119,5
Follow-Up Time (months)
Cu
mu
lati
ve I
ncid
en
ce R
ate
of
≥C
IN3 HPV16
+
HPV18
+
HPV
+
HPV+/
HPV16-
/18-HPV
-
Kahn et al., JNCI (2005)
CIN3 develpoment during follow up in relation to HPV status
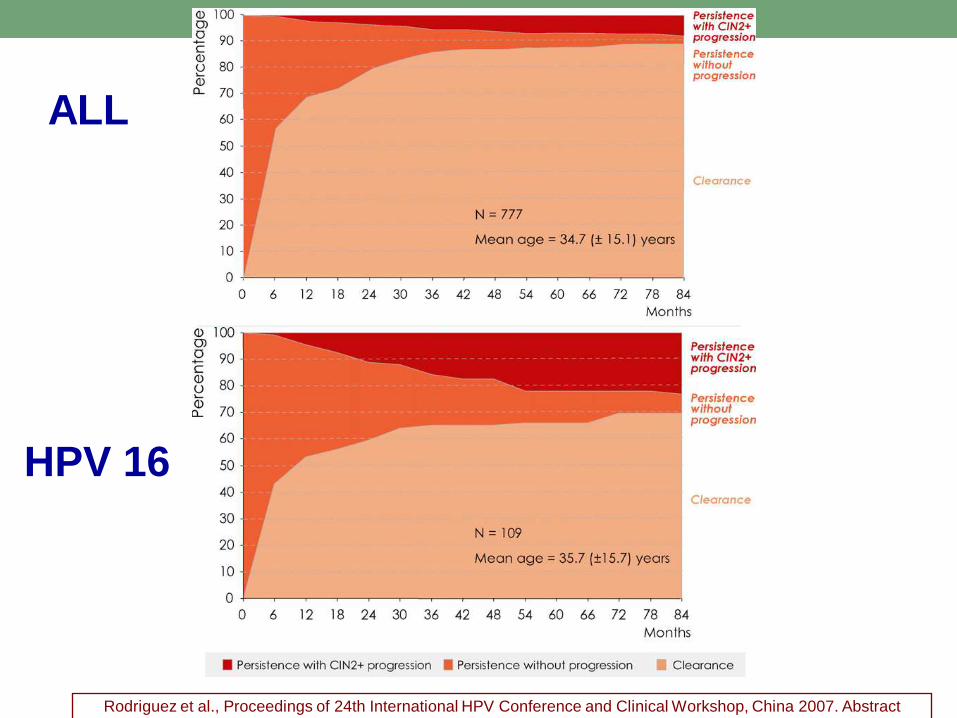
ALL
HPV 16
Rodriguez et al., Proceedings of 24th International HPV Conference and Clinical Workshop, China 2007. Abstract
section

HPV persistent infection can cause the development of invasive cervical cancer in 10 to 15 years
many co-factors are involved in the process of cancer development
Natural history of HPV infection

Few studies addressed
in longitudinal studies
HPV status in sex
couples
HPV: what we know in sex couples?
….In our current study, less than half of the couples exhibited perfect HPV-type specific concordance. More than one third of couples had complete discordance…..
Multivariate regression analysis.
Reporting a new sex partner or the same sex partner or no sex partner was not significantly associated with the risk of infection reappearance.

HPV Clearance
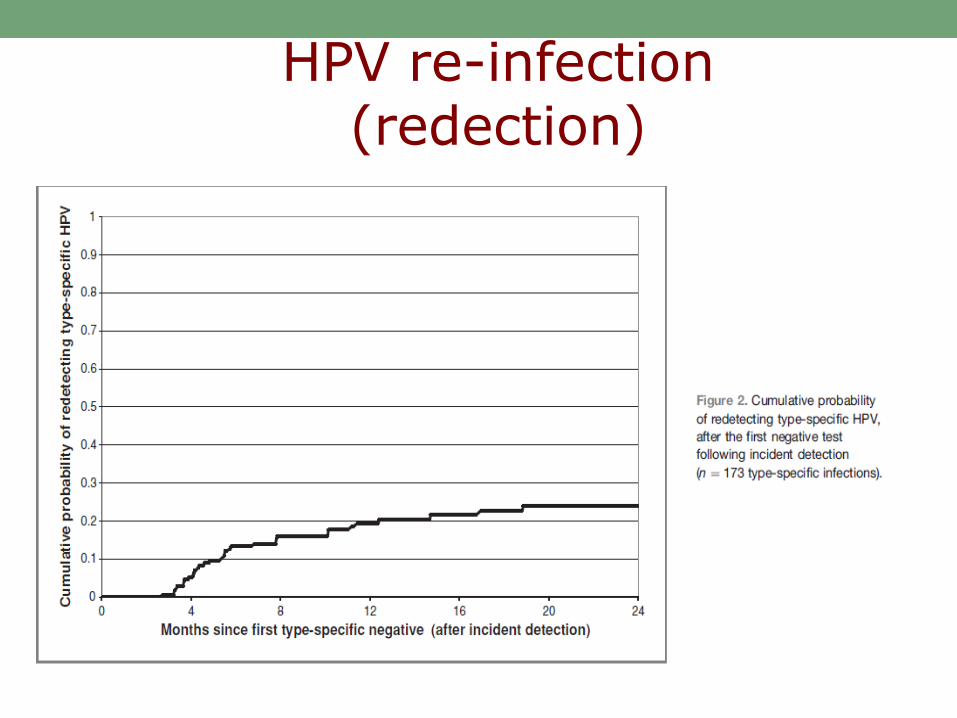
HPV re-infection(redection)

HPV infection is very common and is
not a disease
pre-cancer is a rare event
cancer is an exceptional event
HPV: what we now know
HPV infection is very rarelyassociated to cancer
development
However HPV is necessary for cancer develpoment
HPV and Cervical Cancer
Cervical cancer screening
• Pap smear as primary screening test
• Identification of CIN3
• Elimination of CIN3 through excisional
conservative surgery
The historical strategy

Screening aim
To identify and eliminate this lesion


Vaccination Population at
risk (screening)
Detection & Intervention
(pre-cancer elimination)
USUAL STRATEGYNEW STRATEGY
Cervical cancer screening
• Testing the population for the
causative agent of cervical cancer
• Testing aimed to identifcation of CIN3
• Testing not aimed to detect infection
HPV TESTING

Cervical cancer screening
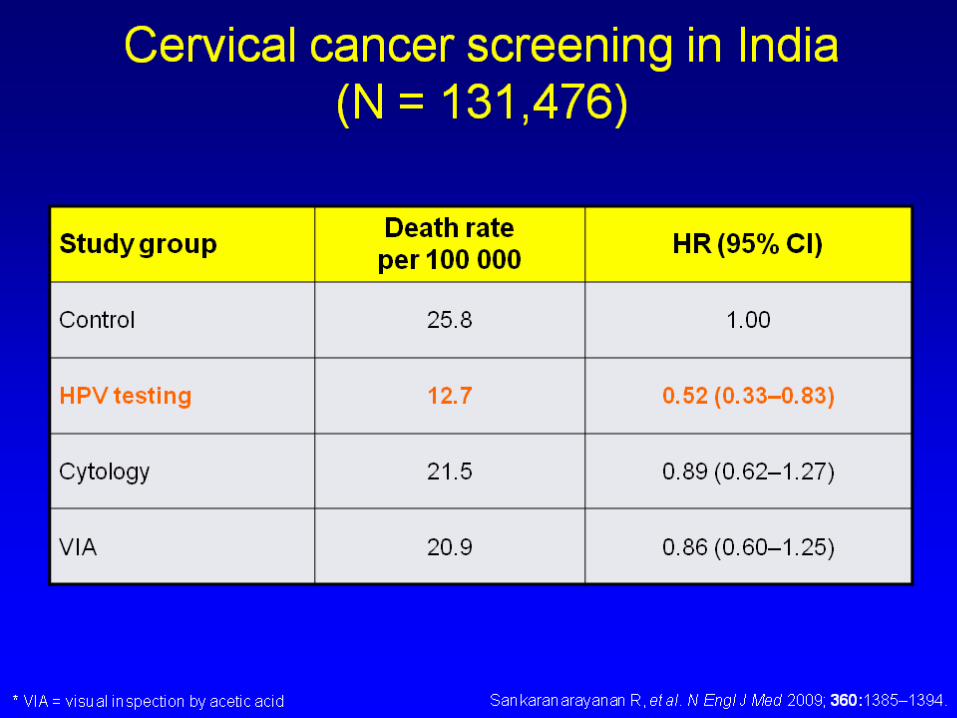
PROOF of PRINCIPLE
HPV TESTING

CERVICAL CANCER SCREENING IN INDIAN = 131.476
Four arms randomized study:
•Control
•VIA
•Pap smear
•HPV test
HPV test
Pap smear
VIA
Control

Cervical cancer screening
known limitations of
cytology screening
PAP SMEAR

30
40
50
60
70
80
90
100
1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001
8
9
10
11
12
13
14
15
16
17
18
Inc
ide
nc
e/1
00
00
0S
cre
en
ing
Co
ve
rag
e (
%)
Cervical cancer screening
Start of organised screening

Never pap smear 162 62%
Pos. pap & adequate
follow-up29 11%
False negative pap 37 14%
Previous abnormal
smear*34 13%
TOTAL 262 100%
Screening “failures”
italian data
Amadori A. Int J Gynecol Cancer 1998262 invasive cancer cases, TR Romagna and Toscana (1986-93).
* Repeat smear not done, colposcopy not done, colposcopy done late, negative colposcopies, negative biopsies, CIN3 diagnosed with no further action.
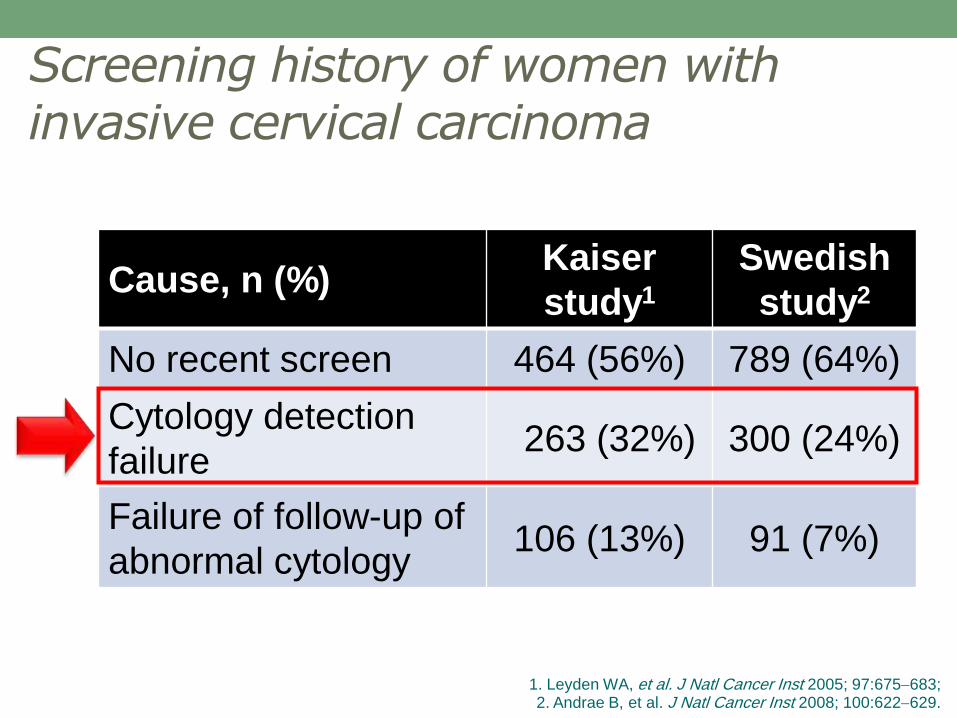
Cause, n (%)Kaiser
study1
Swedish
study2
No recent screen 464 (56%) 789 (64%)
Cytology detection
failure263 (32%) 300 (24%)
Failure of follow-up of
abnormal cytology106 (13%) 91 (7%)
Screening history of women with invasive cervical carcinoma
1. Leyden WA, et al. J Natl Cancer Inst 2005; 97:675683; 2. Andrae B, et al. J Natl Cancer Inst 2008; 100:622629.

Results of the NTCC study
(Nuove Tecnologie per lo Screening
del Cancro Cervicale)

Setting: population based screening programme
Prospective randomized study on new screening test
Accrual phase: March 2002 to December 2004
94,370 women aged 25–60 years were randomized
Arm A 47,001 = conventional cytology
Arm B 47,369 = HPV testing (HC2)
Two screening rounds were completed (6 years)
METHODS

Women were divided into two different age
groups:
• 25 to 34
• 35 to 60
METHODS

The primary endpoint was the detection of
grade 2 and 3 CIN, and of invasive cervical
cancers during the first and second screening
rounds.
Analysis was done by intention to screen.
METHODS
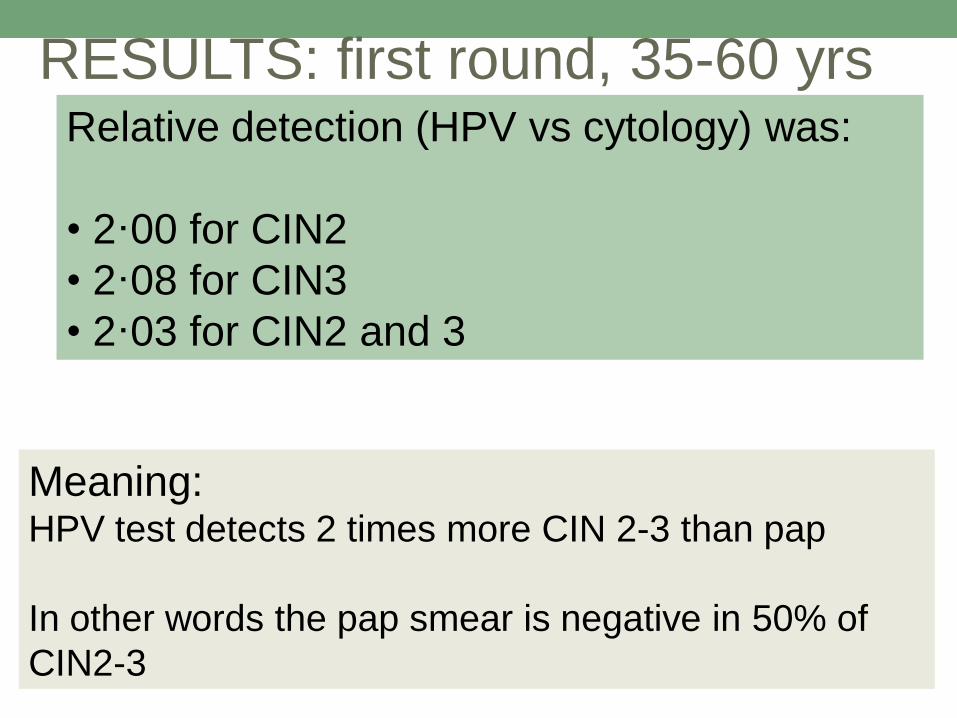
Relative detection (HPV vs cytology) was:
• 2·00 for CIN2
• 2·08 for CIN3
• 2·03 for CIN2 and 3
RESULTS: first round, 35-60 yrs
Meaning:HPV test detects 2 times more CIN 2-3 than pap
In other words the pap smear is negative in 50% of
CIN2-3

Relative detection (HPV vs cytology) was:
• 2·00 for CIN2
• 2·08 for CIN3
• 2·03 for CIN2 and 3
RESULTS: first round, 35-60 yrs
Question:
Are these “new” CIN2-3 clinically relevant?
Go to the second round…
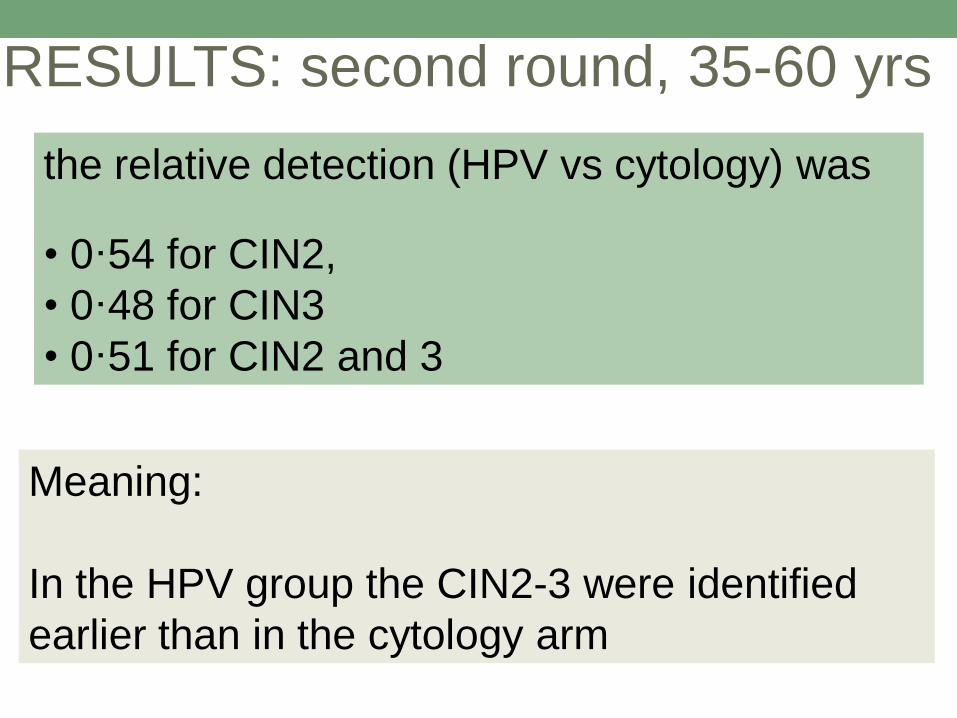
RESULTS: second round, 35-60 yrs
Meaning:
In the HPV group the CIN2-3 were identified
earlier than in the cytology arm
the relative detection (HPV vs cytology) was
• 0·54 for CIN2,
• 0·48 for CIN3
• 0·51 for CIN2 and 3

RESULTS: second round, 35-60 yrs
Question:
Which is the clincal value of the “anticipated”diagnosis?
the relative detection (HPV vs cytology) was
• 0·54 for CIN2,
• 0·48 for CIN3
• 0·51 for CIN2 and 3

RESULTS: 35-60 yrs
Question:
Which is the clincal value of the “anticipated”diagnosis?
It is safe to increase the intervals between two
screens.
But what about the invasive cancers?

First Round 6 8 0.61Second Round 0 7 0.016Total 6 15 0.052
HPV test pap smear P value
RESULTS: 35-60 yrs
Number of invasive cancers
Meaning:
Follow up of untreated CIN2-3 carries the risk
of cancer development

First Round 6 8 0.61Second Round 0 7 0.016Total 6 15 0.052
HPV test pap smear P value
RESULTS: 35-60 yrs
Number of invasive cancers
Clinical consequences of the study:
Stop pap smear screening and switch to HPV
testing
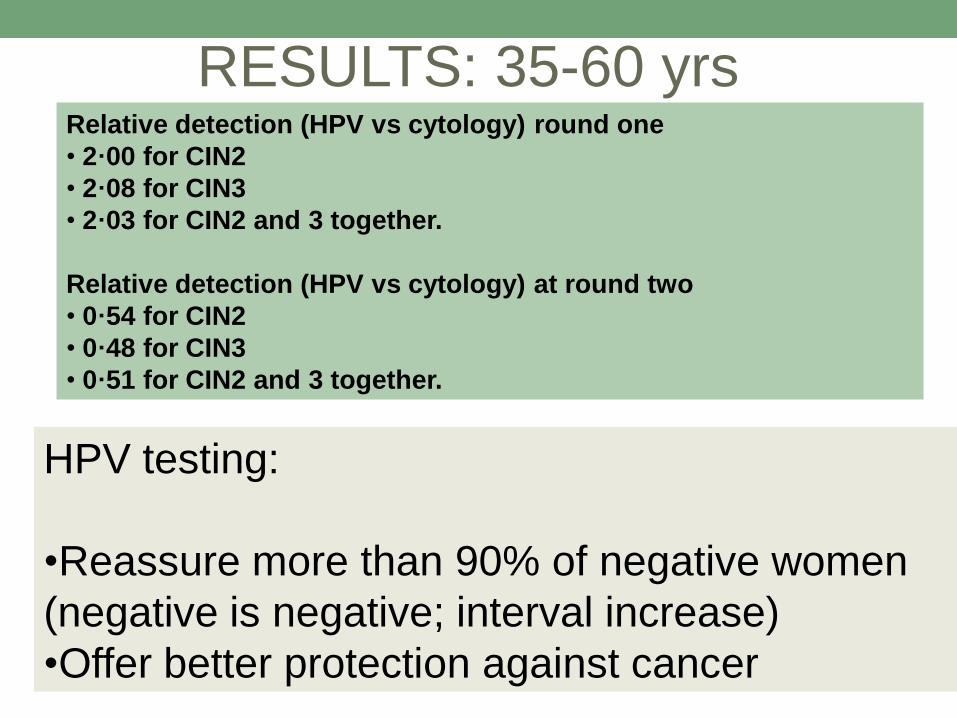
Relative detection (HPV vs cytology) round one
• 2·00 for CIN2
• 2·08 for CIN3
• 2·03 for CIN2 and 3 together.
Relative detection (HPV vs cytology) at round two
• 0·54 for CIN2
• 0·48 for CIN3
• 0·51 for CIN2 and 3 together.
RESULTS: 35-60 yrs
HPV testing:
•Reassure more than 90% of negative women
(negative is negative; interval increase)
•Offer better protection against cancer

RESULTS: 25-34 yrs
What about the young women,
aged 25 to 34?
Same results or different situation?

RESULTS: 25-34 yrs The relative detection (HPV vs cytology) was:
Round 1
• 3·91 for CIN3 and AIS
Round two
• 0·20 for CIN3 and AIS.
Meaning:
Four times more CIN3 and AIS detected by
HPV testing
Five times less CIN3 and AIS in the subsequent
round (more evident effect in young women
than in older)

First Round 1 1 1.00Second Round 0 2 0.50Total 1 3 0.37
HPV test pap smear P value
RESULTS: 25-34 yrs
Number of invasive cancers
Clinical consequences of the study:
Some considerations….

RESULTS: 25-34 yrs The relative detection (HPV vs cytology) was:
Round 1
• 3·91 for CIN3 and AIS
Round two
• 0·20 for CIN3 and AIS.
Considerations:
Double number of lesions in the whole period
(overdiagnosis-overtreatment)

First Round 1 1 1.00Second Round 0 2 0.50Total 1 3 0.37
HPV test pap smear P value
RESULTS: 25-34 yrs
Number of invasive cancers
Clinical consequences of the data 25-34 yrs:
The increment in cancer detection is counter balanced by an
increase in diagnosis and treatment of clinically non relevant
(regressing?) CIN2-3

First Round 7 9 0.62Second Round 0 9 0.004Total 7 18 0.028
HPV test pap smear P value
RESULTS: 25-60 yrs
Number of invasive cancers
The total figures of cancer reduction is still
impressive; this figure prompted GISCi to start
the long and difficult process to abandon pap
smear as primary screening test because it is
unethical to continue with pap smear screening

HPV TEST:
Which optimal use?
• HPV test has an high NPV
• HPV test is ideally suited to reassure the
negative HPV individuals and to increase
intervals between two subsequent screens
• at any age HPV negative test is reassuring

There are no scientific doubt that HPV test should be used as
primary screening test.
Implementation is still a problem where pap smear
screening system is in place
CONCLUSIONS
It is a Copernican revolution…Copernicus was placed under investigation…..



THANK YOU FOR YOUR
ATTENTION!
Mario SideriUnità Ginecologia Preventiva
Istituto Europeo di Oncologia, Milano
Italian HPV Study Group (IHSG)


















