
Micro16.Nebal (1) crctd -...
18
. number 16 Done by Nebal Al-Gallab Corrected by Doctor
Transcript of Micro16.Nebal (1) crctd -...

.
number16
Done byNebal Al-Gallab
Corrected by
Doctor
AA
Typewritten Text
AA
Typewritten Text
25

The last page includes definitions for the asterisked words*
❖ Main Lecture’s Points
1)Spirochetes
o Trepanoma
o Borrelia
o Liptospiral
2)Chlamydia
o Trachomatis
o Psittaci
o Pneumonia
➢Spirochetes
Spirochetes are tiny gram negative organisms that look like corkscrews, they are devided into 3 genera :
1)Trepanoma
- (T.pallidum)
- (T.pertenue)
- (T.endemicum)
- (T.carateum)

- other non pathogenic spp
• T.Pallidum (Syphillis)
✓ Treponema pallidum is the infectious agent responsible for the sexually transmitted disease syphilis*.
✓ Belongs to spirochetes which are thin walled, flexible spiral rods.
✓ Motile by flagella:
- At both sides
- wrap around the bacterial cell body - In contrast to other motile bacteria, these flagella do not
protrude into the surrounding medium but are enclosed within the bacterial outer membrane.
✓Has not been grown on bacteriologic media.
Electron micrograph of T.Pallidum, the flagella (arrowheads) are inserted at the tip and follow the
helical contour of the bacterial cell enclosed within the outer membrane.
✓ Transmission:
- Sexually (mainly) - Contact with skin lesions
- Congenital (mother to baby)

- Blood donation during primary and secondary stages
✓ Incubation period:
2-10 weeks (usually 3 weeks).
✓ Pathogenesis: - Human pathogen (only human)
- No toxins
- Multiplication at primary site of infection leading to a painless ulcer called Chancre*
- Infectious dose* less than 10 organisms
- Widespread via blood to many tissues
If untreated, patients with syphilis will progress through 3 clinical stages, with a latent period between stages 2 and 3.
Stages of Syphilis:- Early (primary and secondary), latent, and tertiary
stages- Overall and the early diseases:- 1/3 will heal without treatment - 1/3 will go to latent - 1/3 into tertiary
❖Primary Syphilis- The primary lesion of syphilis is a painless chancre on
genitalia, cervix or anogenital area - Usually single
- Disappear spontaneously in 3-6 weeks
(it’s actually erupt at the site of inoculation 3-6 weeks after the initial contact)
- Infectious
- Inguinal LNE (caused swelling to lymph nodes)
- Exudates used for diagnosis.
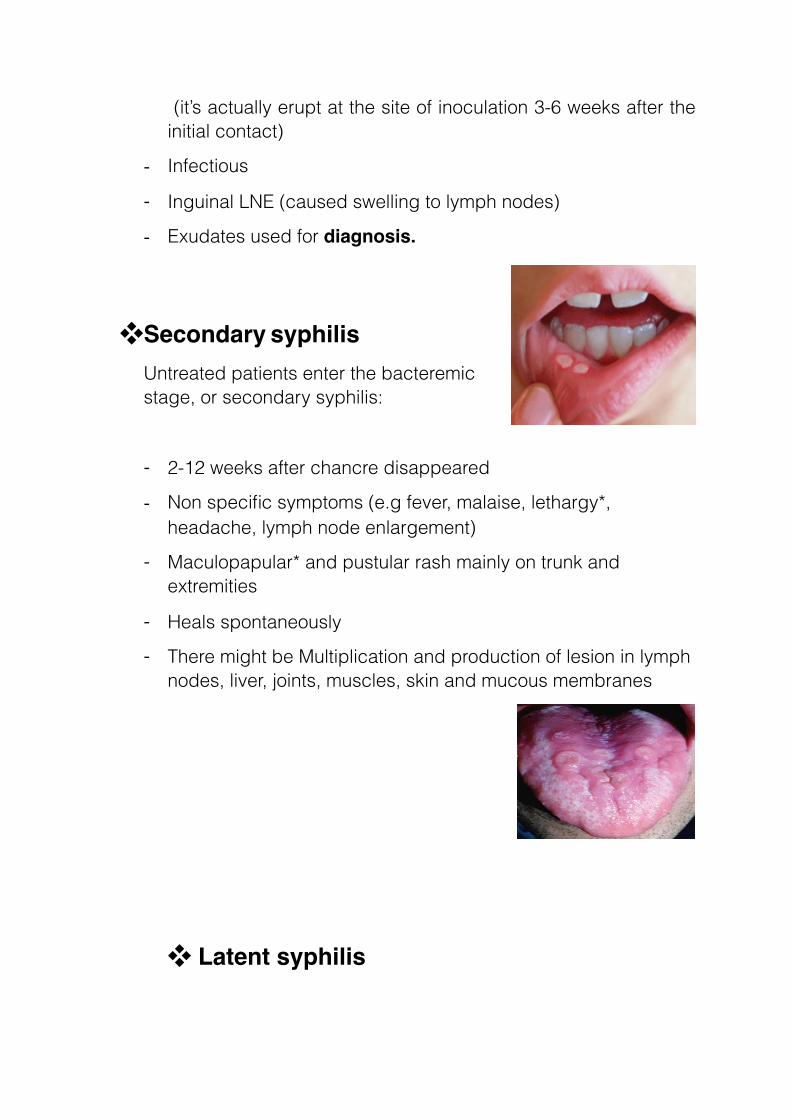
❖Secondary syphilisUntreated patients enter the bacteremic stage, or secondary syphilis:
- 2-12 weeks after chancre disappeared
- Non specific symptoms (e.g fever, malaise, lethargy*, headache, lymph node enlargement)
- Maculopapular* and pustular rash mainly on trunk and extremities
- Heals spontaneously - There might be Multiplication and production of lesion in lymph
nodes, liver, joints, muscles, skin and mucous membranes
❖ Latent syphilis

- No lesion but serological evidence exists (serologic test remain positive)
- Early and late latent ( Early latent phase may reactivate and manifest as a secondary lesion i.e infectious)
❖ Tertiary
- Develops over 3-30 years
- Slow inflammatory damage to organ tissue, small blood vessels, and nerve cells
- It can be grouped into 3 general categories: o Skin and bone granulomatous lesions (Gummas) o Cardiovascular: aneurysm* of ascending aorta, aortitis o Neurosyphilis: e.g Meningoencephalitis and paralysis
✓Congenital syphilis - Occurs in the fetus of an infected pregnant woman (Blood –
placenta - fetus)
- Fetuses that acquire the infection have a high mortality rate, intrauterine death, abortion, low birth weight
- Facial abnormalities e.g saddle shape nose
✓Diagnosis

1. Detection of the organism in the exudates and lesions using dark field E.M or phase contrast, Immunofluorescent antibodies – Low sensitivity.
2. Serology
I. Non-specific antibodies (1-2 weeks after the primary chancre appears)
▪ Extra note -to understand the technique-, you can ignore it
“Infection with syphilis results in cellular damage and the release into the serum of a number of lipids, including cardiolipin, the body produces antibodies against these antigens, we therefore quantitatively measure the titer of the antibodies that bind to these lipids. If a patient's serum has these antibodies, we suspect that he/she has syphilis. “
The two most common tests employing this technique and detecting anticardiolipin antibodies are:
a) Rapid Plasma Reagin (RPR) test
b) Venereal Disease Research Laboratory (VDRL)
II. Specific antibodies
These tests should be used to confirm that a positive result with a non-specific test is truly due to syphilis.
a) Fluorescent Treponema antibodies absorption (FTA-Abs):
patient's serum is first absorbed with non-pathogenic treponemes to remove cross-reacting antibodies before reaction with T. pallidum antigens.
b) Treponema Pallidum Haemagglutinin Antibodies (TPHA)

▪ Sensitivity of serological test in syphilis
✓Treatment - Penicillin G
- If allergic, Doxycycline or erythromycin is a good alternative - In neurosyphilis use penicillin and Doxycycline together.
✓Prevention - No vaccine
- Early diagnosis and treatment of case and contact is important
- Sexually transmitted: Test for syphilis if any sexually transmitted disease (STD) exists.
2)Borrelia
• Burgdorferi
✓ Borrelia are larger than the Treponema, and therefore can be viewed under a light microscope
✓ Cause Lyme disease, which is the most commonly reported tick-borne illness in the USA

✓ The animals reservoir for Borrelia burgdorferi includes Wild animals, Rodents, Birds ..Incubation is few weeks-months
✓ Systemic diseases include Arthritis, CNS, Cardic Abnormalities
✓ Painless skin lesion (Single/Multiple)
• Recurrent
✓ Recurrent fever, can be fatal
3)Liptospira
✓Liptospiral diseases
- Zoonosis - Mild-severe fatal systemic
✓Weils’s disease
- High fever - vasculitis
- Bleeding
- Jaundice*
✓Diagnosis
Serological Tests, Special culture
➢Chlamydia
✓ Small obligate intracellular parasites

✓ It’s classified as gram negative because it stains red with Gram stain technique and has an inner and outer membrane.
✓ Unlike other gram-negative bacteria, it does not have a peptidoglycan layer.
✓ Energy parasites, using a cell membrane transport system that steals an ATP from the host cell and spits out an ADP (can’t make ATP by itself)
✓ The Chlamydia life cycle is complex as the bacteria exist in 2 forms:
I. Elementary body (EB)o Infectious form -bind to columnar epithelial cells (macrophages) o Non-replicating, non-metabolically active form o Resistant to harsh conditions o The outer membrane has extensive disulfide bond cross-
linkages that confer stability for extracellular existence
II. Reticulate bodies (RB)o Non-infectious form o Replicating, metabolically active form o The outer membrane has fewer disulphide bond cross-
linkage (fragile membrane) so it’s an intracellular form
✓ Developmental cycle of chlamydia
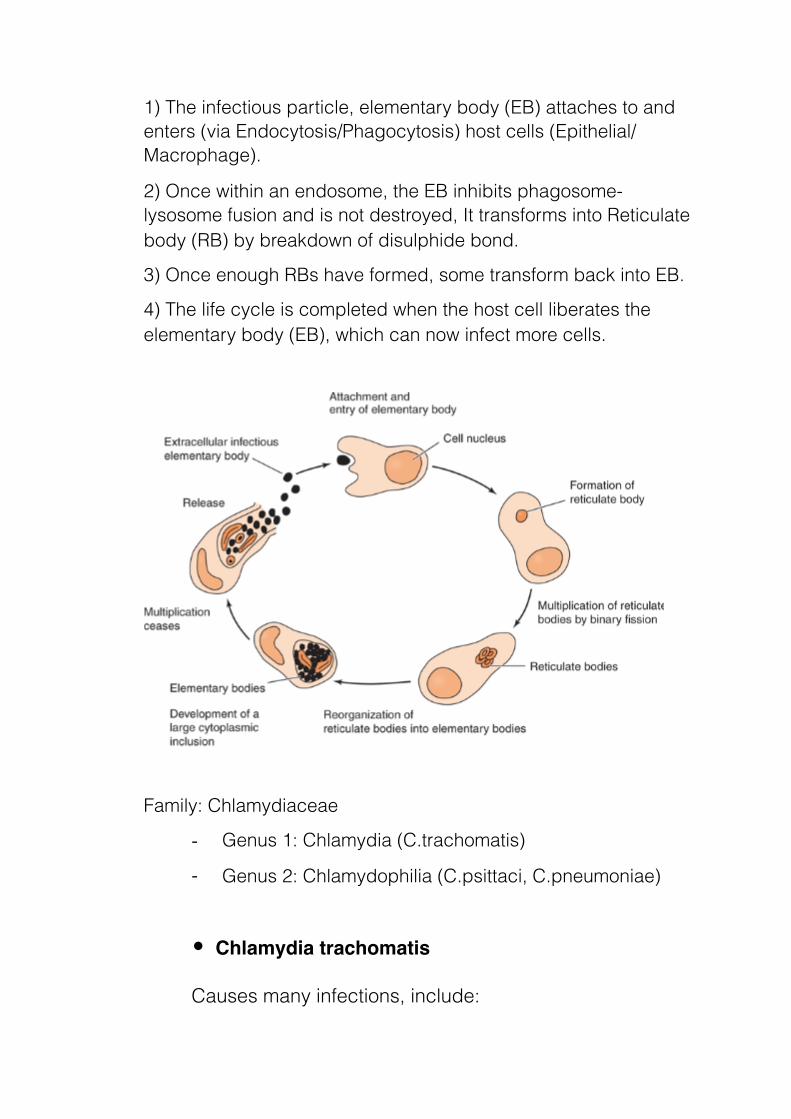
1) The infectious particle, elementary body (EB) attaches to and enters (via Endocytosis/Phagocytosis) host cells (Epithelial/Macrophage).
2) Once within an endosome, the EB inhibits phagosome-lysosome fusion and is not destroyed, It transforms into Reticulate body (RB) by breakdown of disulphide bond.
3) Once enough RBs have formed, some transform back into EB.
4) The life cycle is completed when the host cell liberates the elementary body (EB), which can now infect more cells.
Family: Chlamydiaceae
- Genus 1: Chlamydia (C.trachomatis)
- Genus 2: Chlamydophilia (C.psittaci, C.pneumoniae)
• Chlamydia trachomatis
Causes many infections, include:

- Inclusion conjunctivitis*
- Infant pneumonia (during baby's passage through an
infected birth canal).
- Ocular lymphogranuloma venerium
- Urogenital infections
- Lymphogranuloma venerium (STD)
- Trachomao a type of chronic conjunctivitis that is currently the
leading cause of preventable blindness in the world o It is a disease of poverty, prevalent in overcrowd parts of
the world (Endemic in Africa, Middle East, India, SE Asia – United States - American Indians)
o Infection of children o Transmission:
droplets, hands, contaminated clothing, flies, contaminated birth canal.
o sexually transmitted o Clinical syndrome- Trachoma
▪ Chronic or repeated infection (Follicle formation on conjunctiva – Scarring of the conjunctiva)
▪ Eyelids turn in and abrade cornea (Ulceration – Scarring – Blood vessel formation)
▪ Flow of tears impeded (Secondary infections)
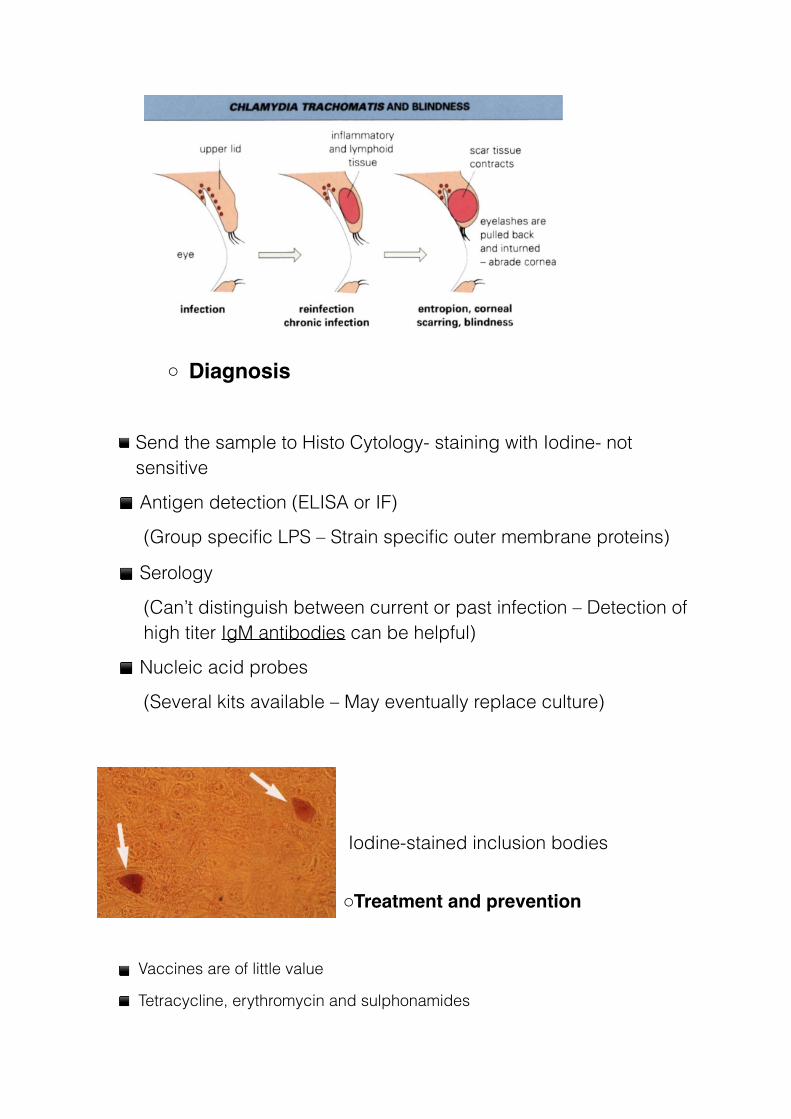
o Diagnosis
▪ Send the sample to Histo Cytology- staining with Iodine- not sensitive
▪ Antigen detection (ELISA or IF)
(Group specific LPS – Strain specific outer membrane proteins)
▪ Serology
(Can’t distinguish between current or past infection – Detection of high titer IgM antibodies can be helpful)
▪ Nucleic acid probes
(Several kits available – May eventually replace culture)
Iodine-stained inclusion bodies
oTreatment and prevention
▪ Vaccines are of little value
▪ Tetracycline, erythromycin and sulphonamides

▪ Treatment of patients and their sexual partners
▪ Safe sexual practices
▪ Treatment coupled with improved sanitation
• Chlamydia (Chlamydophilia) psittaci
- infects a lot of species of birds
- Cause Psittacosis*, Ornithosis (Parrot fever)
- Pathogenesis
▪ Inhalation of organisms in bird droppings (Person to
person transmission is rare)
▪ Hematogenous* spread to spleen and liver (Local necrosis
of tissue)
▪ Hematogenous spread to lungs and other organs
▪ Lymphocytic inflammatory response (Edema, infiltration of
macrophages, necrosis and occasionally haemorrhage- Mucus plugs* may develop in alveoli)
▪ Cyanosis and anoxia*
- Diagnosis
- serology
- Fourfold rise in titer
- Treatment
▪ Tetracycline or erythromycin
▪Quarantine* of imported birds
▪ Control of bird infection
▪ Antibiotic supplementation of food
• Chlamydia (Chlamydophilia) pneumonia
- Atypical pneumonia, because the pneumonia is very different
from a typical bacterial pneumonia caused by Streptococcus
pneumonia.
- Person to person spread – Respiratory droplets
- Diagnosis: Serology
- Treatment: Tetracycline or erythromycin
➢Definitions
• Aneurysm: an excessive localized enlargement of an
artery caused by a weakening of the artery wall.
• Anoxia: an absence of oxygen.
• Chancre: a painless ulcer, particularly one developing
on the genitals as a result of venereal disease.
• Hematogenous: originating in or carried by the blood.
• Inclusion conjunctivitis: an infectious disease
especially of newborn infants characterized by acute

conjunctivitis and the presence of large inclusion
bodies and caused by a chlamydia (C. trachomatis).
• Infectious dose (ID): is the amount of pathogen
required to cause an infection in the host.
• Jaundice: a medical condition with yellowing of the
skin or whites of the eyes, arising from excess of the
pigment bilirubin and typically caused by obstruction
of the bile duct, by liver disease, or by excessive
breakdown of red blood cells.
• Maculopapular rash: is a type of rash characterized by
a flat, red area on the skin that is covered with small
confluent bumps.
• Mucus plug: An accumulation of mucus and thick fluid
that blocks the opening of the cervix (the opening from
the uterus to the vagina) during pregnancy, it serves to
protect the uterus and the fetus by preventing bacteria
from entering the uterus.
• Psittacosis: a contagious disease of birds, caused by
chlamydiae and transmissible (especially from parrots)
to human beings as a form of pneumonia.
• Quarantine: a state, period, or place of isolation in
which people or animals that have arrived from
elsewhere or been exposed to infectious or contagious
disease are placed.
• Serology: the scientific study or diagnostic examination
of blood serum, especially with regard to the response
of the immune system to pathogens or introduced
substances.
Prayer is the best Medicine
God is the best Doctor

















![Efficient Data Supply for Hardware Accelerators with ...tchen/files/accelmem-micro16-slides.pdf · Si = val[j] * vec[cols[j]]; sum = sum + Si; } 2380 8010 541C 2384 8328 5420 2388](https://static.fdocuments.us/doc/165x107/602d350d8815fa0be61f33f4/efficient-data-supply-for-hardware-accelerators-with-tchenfilesaccelmem-micro16-slidespdf.jpg)
