1. BLS Primary Survey - Save A Heart CPR. BLS Primary Survey • Be proficient with BLS: 2. AED:...
15
1. BLS Primary Survey • Be proficient with BLS: 2. AED: • Turn ON, Attach Pads, Analyzing (do not touch patient), Shock Advised, Clear and Shock • TAKE NOTE: Resume chest compressions when AED is charging ACLS 2010 Study Guide 1 | Page Monitor “RDR” (Rate/ Depth/Recoil) during compressions BLS primary survey continues during ALS secondary survey (ABCD) If pulses are present with ineffective respirations, provide rescue breathing giving 1 breath every 5-6 seconds. Assess for bilateral chest rise and fall. Check carotid pulses for less than 10 seconds. At least 100 compressions per minute 2 breaths are given with 30 compressions for 2 minutes (5 cycles of 30:2)
-
Upload
nguyennhan -
Category
Documents
-
view
230 -
download
1
Transcript of 1. BLS Primary Survey - Save A Heart CPR. BLS Primary Survey • Be proficient with BLS: 2. AED:...
1. BLS Primary Survey
• Be proficient with BLS:
2. AED:
• Turn ON, Attach Pads, Analyzing (do not touch patient), Shock Advised, Clear and Shock
• TAKE NOTE: Resume chest compressions when AED is charging
ACLS 2010 Study Guide
1 | P a g e
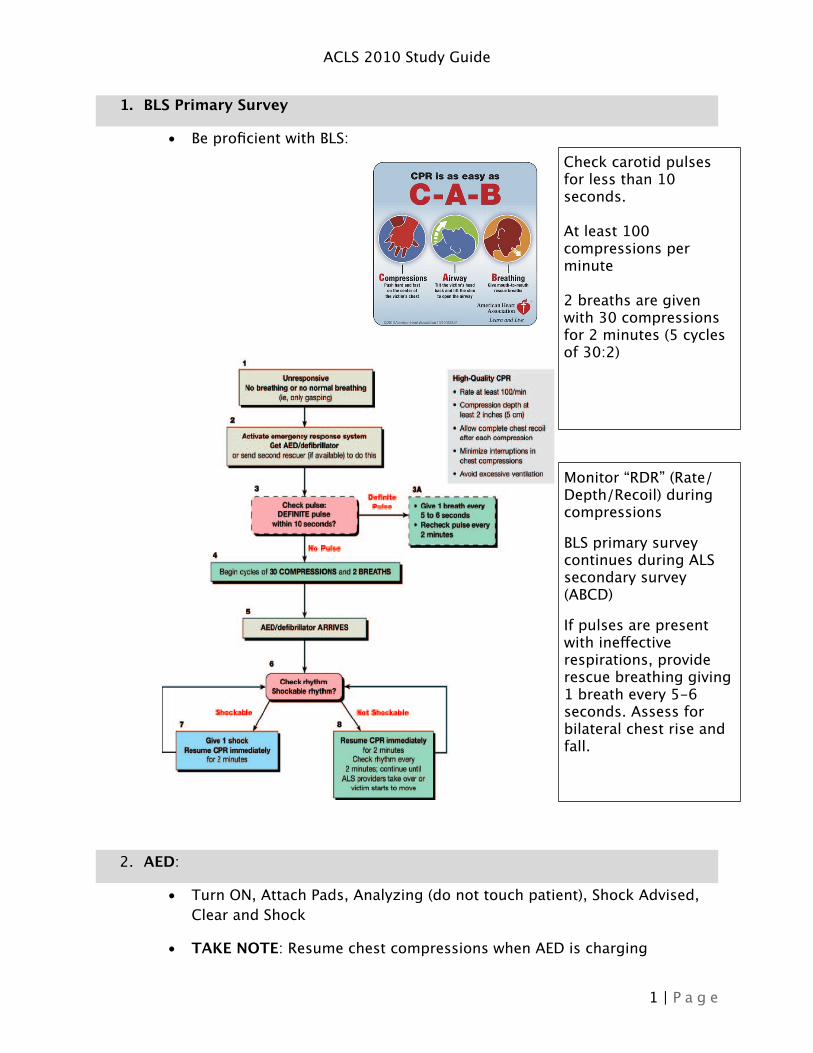
Monitor “RDR” (Rate/Depth/Recoil) during compressions
BLS primary survey continues during ALS secondary survey (ABCD)
If pulses are present with ineffective respirations, provide rescue breathing giving 1 breath every 5-6 seconds. Assess for bilateral chest rise and fall.
Check carotid pulses for less than 10 seconds.
At least 100 compressions per minute
2 breaths are given with 30 compressions for 2 minutes (5 cycles of 30:2)

• If no shock advised, resume compressions
• Know the contraindications with AED (i.e. hairy chest, wet victims, dermal patches, pacers, bra with wires, etc.)
3. Airway Management
• Always intervene with the least to the most invasive interventions
POSITION
PATENCY• Suction (<10 sec)• OPA, NPA
OXYGENATE• Nasal Cannula• Simple Masks
VENTILATE• Bag-Mask: Give 1 breath every 5-6 seconds
(10-12/min)• Advanced Airways: Give 1 breath every 6-8
· Waveform Capnography: PETCO₂ (Partial End-Tidal CO₂)
- Normal range: 35-45 mmHg
- Used for quantitative measurement of perfusion
- Reliable verification of ETT placement
- Monitor’s quality of compressions. Must have at least 10 mm Hg or greater to achieve perfusion.
- Identifies ROSC (return of spontaneous circulation) during compressions with abrupt increase of PETCO₂.
ACLS 2010 Study Guide
2 | P a g e

- Post-Arrest Care: PETCO₂ goal is to achieve 35-40 mmHg or greater
· Advanced Airways
- Not needed if airway is patent during compressions
- ETT (endotracheal tube) – Verify by auscultating 5 placements, visualizing bilateral chest rise/fall, using PETCO₂ as continuous monitoring
- LMA and King Tube can be inserted without stopping chest compressions
- Give 1 breath every 6-8 seconds (8-10 breaths/minute) with or without compressions.
4. Ischemic Stroke
ACLS 2010 Study Guide
3 | P a g e
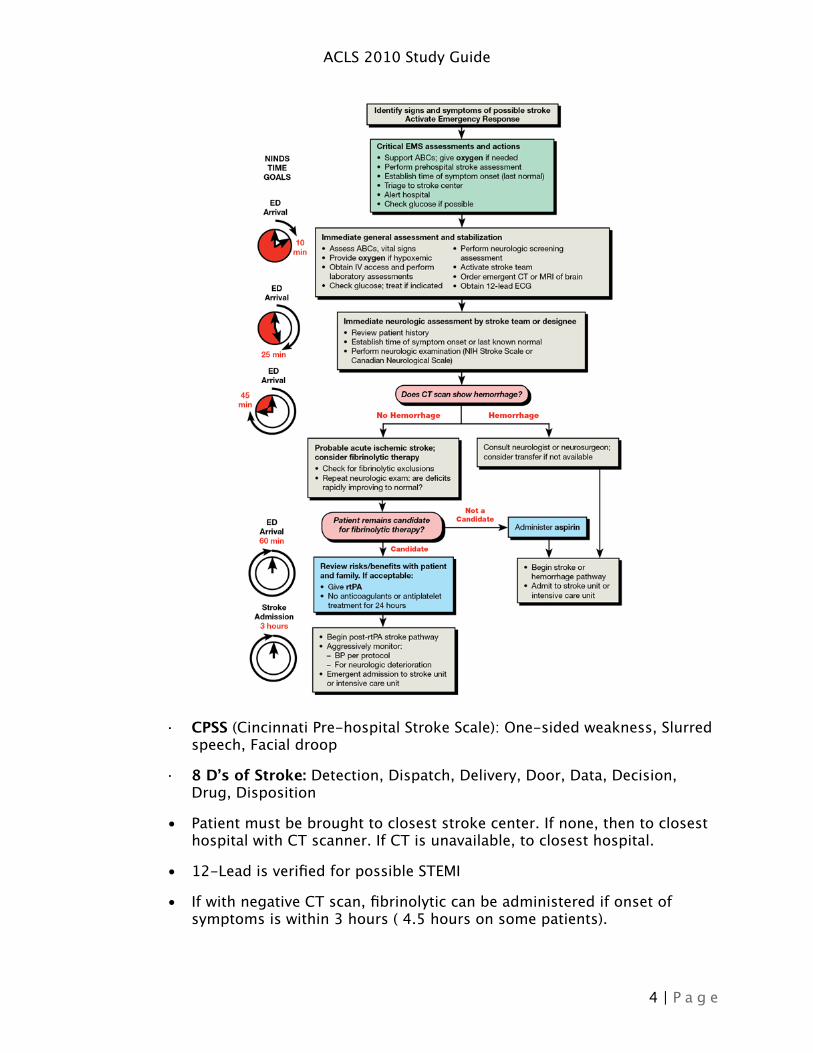
· CPSS (Cincinnati Pre-hospital Stroke Scale): One-sided weakness, Slurred speech, Facial droop
· 8 D’s of Stroke: Detection, Dispatch, Delivery, Door, Data, Decision, Drug, Disposition
• Patient must be brought to closest stroke center. If none, then to closest hospital with CT scanner. If CT is unavailable, to closest hospital.
• 12-Lead is verified for possible STEMI
• If with negative CT scan, fibrinolytic can be administered if onset of symptoms is within 3 hours ( 4.5 hours on some patients).
ACLS 2010 Study Guide
4 | P a g e
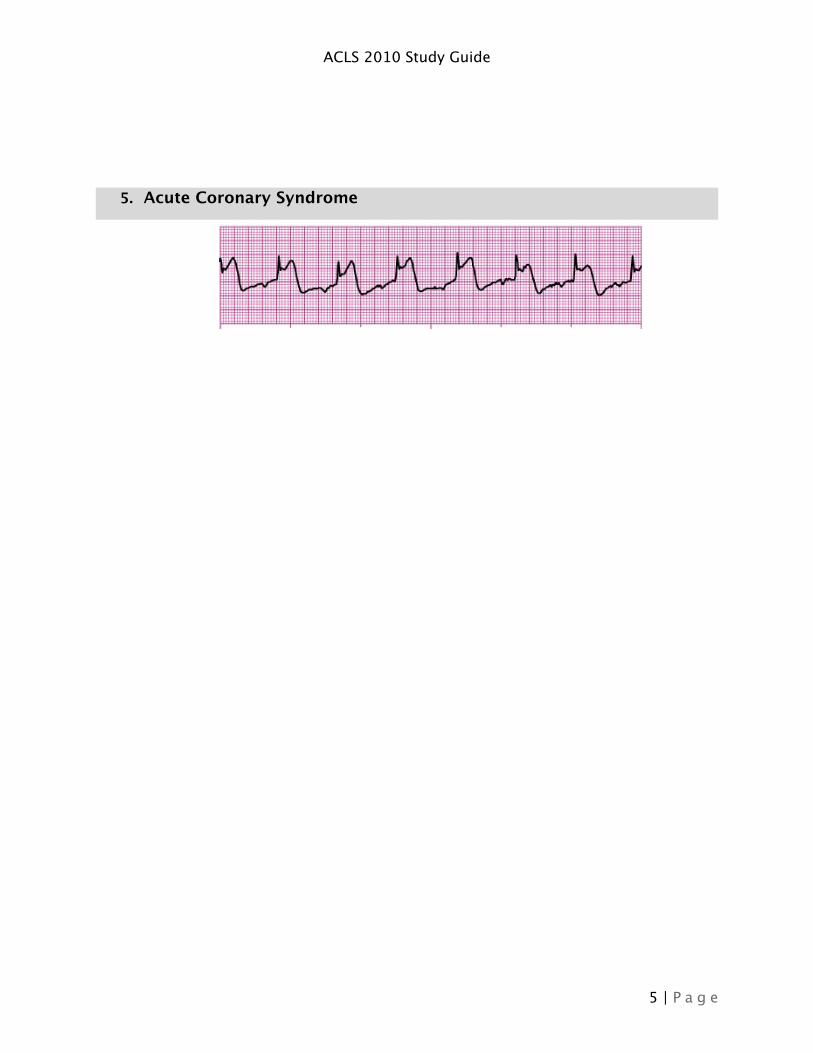
5. Acute Coronary Syndrome
ACLS 2010 Study Guide
5 | P a g e

• Focus on STEMI (ST Elevation MI) pathway, verified on 2 contiguous leads on 12-Lead
• Memorize “MONA” doses and contraindications specially for Nitro and Morphine
• Know atypical signs of MI• Know contraindications of Right Ventricular Infarction (RVI) or Inferior
Infarct
ACLS 2010 Study Guide
6 | P a g e

6. Invtravenous/Intraosseous
• Preferred route of medication administration is via peripheral IV
• After multiple attempts of IV insertion without success, IO is inserted.
• Know IO insertion sites and be familiar with various IOs
• All medications given through IV can be administered via IO.
• Goals of IO: Insertion, Administration and Discontinuation (<24 hours)
ACLS 2010 Study Guide
7 | P a g e

7. Bradycardia
ACLS 2010 Study Guide
8 | P a g e
Sinus Bradycardia
3rd Degree AV Block

8. Tachycardia
ACLS 2010 Study Guide
9 | P a g e
NOTE:
Know appropriate dosing of Dopamine and Epinephrine
TCP is preferred for 3rd Degree AVB unless unavailable then Atropine is
Regular: Narrow Complex TachycardiaSupraventricular Tachycardia
Rate: 150 >
ACLS 2010 Study Guide
10 | P a g e
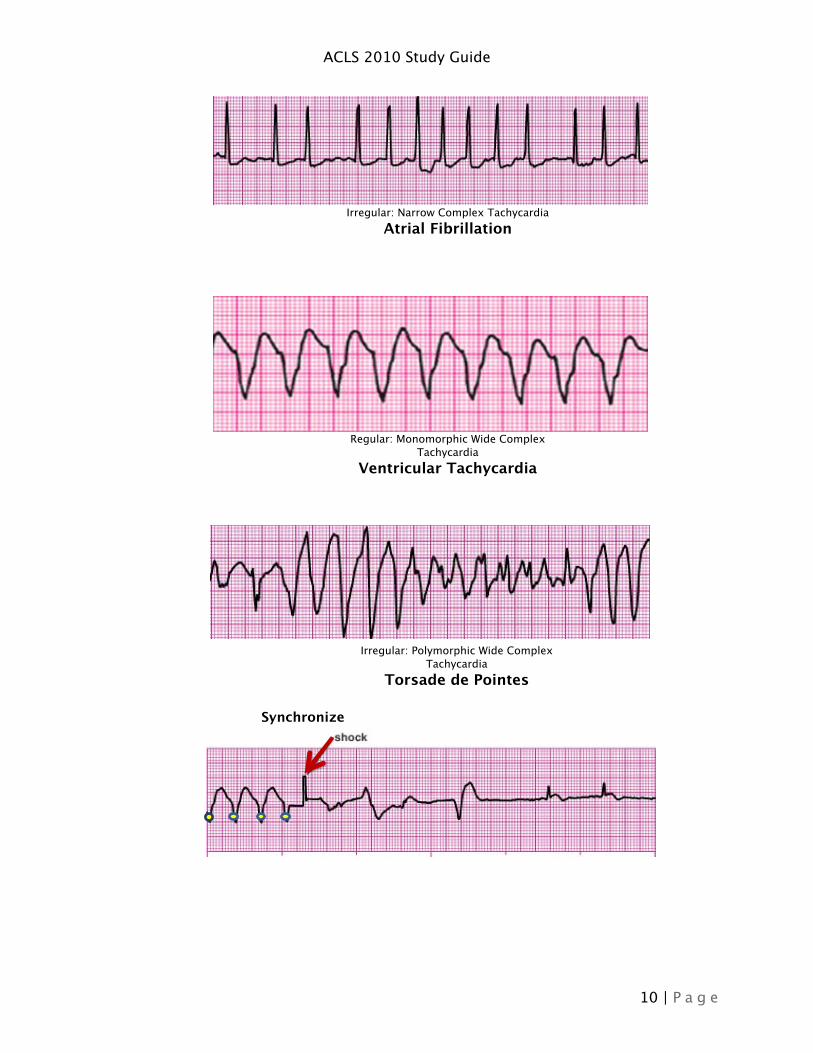
Irregular: Narrow Complex TachycardiaAtrial Fibrillation
Regular: Monomorphic Wide Complex Tachycardia
Ventricular Tachycardia
Irregular: Polymorphic Wide Complex Tachycardia
Torsade de Pointes
Synchronize

ACLS 2010 Study Guide
11 | P a g e

9. Pulseless Arrest
ACLS 2010 Study Guide
12 | P a g e
Ventricular Fibrillation
Pulseless Ventricular Tachycardia
Asystole
Pulseless Electrical Activity
No Pulse
No Pulse

ACLS 2010 Study Guide
13 | P a g e
NOTE: VF, Pulseless VT, Asystole and Agonal are not

10.Post-Resuscitation Care: ROSC
• ROSC (Return of Spontaneous Circulation)• Maintain O₂ Sat 94%>, titrate 10-12 breaths/min• Consider advanced airway and maintain PETCO₂ 35-40 mm Hg>• 1-2 L NS/LR bolus (at 4˚C to induce hypothermia if ALOC)• Titrate vasopressors to keep BP 90 mm Hg>• Identify and treat reversible causes • 12-Lead ECG for possible PCI if STEMI or high suspicion of AMI
ACLS 2010 Study Guide
14 | P a g e

• Consider hypothermia for 12-24 hours in ALOC for cerebral oxygenation and ventilation
• Keep glucose slightly above normal to avoid hypoglycemia during hypothermia
11.Termination of Resuscitation Effort
• DNAR (Do Not Attempt Resuscitation)
• Decapitation
• Presence of Rigor Mortis
• Continued decompensation during resuscitative efforts
• Inherent danger to team during resuscitation
• Unwitnessed arrest
• No defibrillation during BLS or ALS
• MD ordered termination
ACLS 2010 Study Guide
15 | P a g e