
1 Atypical Language Gaia Scerif Room 426, Ext. 67926 [email protected] Office Hours:...
27
1 Atypical Language Atypical Language Gaia Scerif Room 426, Ext. 67926 [email protected] Office Hours: Mon 2-4
-
Upload
willa-hawkins -
Category
Documents
-
view
222 -
download
0
Transcript of 1 Atypical Language Gaia Scerif Room 426, Ext. 67926 [email protected] Office Hours:...

11
Atypical LanguageAtypical Language
Gaia ScerifRoom 426, Ext. 67926
[email protected] Hours: Mon 2-4

22
Learning objectivesLearning objectives
* Different theoretical approaches to language development
* How can genetic disorders impacting language development be used as tools to evaluate these theories?
* Consider specific examples of genetic disorders:1. Williams syndrome2. KE family
* Evaluate theoretical implications for neo-nativist and constructivist theories of language and cognitive development
33
The role of genes in The role of genes in developmentdevelopment
* Two contrasting approaches to the role of genes in cognitive development:
1. Constructivist - in which cognitive abilities emerge as a product of complex dynamic interactions between genes and environment
2. Nativist - in which a genetic blue-print determines cognitive abilities.
(Johnson, 2000)

44
Models of atypical cognitionModels of atypical cognition
* Theoretical assumptions:
Nativist ConstructivistCause genetic defect genetic defect;
general/specific deficits
Brain specific deficit deviates from normal development
Cognitive impaired acquisition of modules emerge with development; specific modules low-level computational devices
Environment static (acts as a trigger) dynamic (∆ with infant’s
selection & processing input
Behavioural domain-specific outcome specific & general outcomes; specific
outcome with late gene expression
(adapted from Karmiloff-Smith, 1998, 2002)

55
Genes and DevelopmentGenes and Development
* Many developmental disorders appear to have a genetic basis
* Two basic classes of genetic disorders:1. Inherited - transmission of genetic mutations from
parents (e.g., KE family), either dominant or recessive
- single genes or multiple genes
2. Sporadic - chance defective chromosomal configuration (e.g. trisomy 21, Down’s syndrome),
- chance mutation of a portion of DNA (e.g., deletion, WS)
- unknown or possible environmental influence
* Both types affect brain and cognitive development from the outset

66
• Can individual genes be selectively involved in language?
Genes and LanguageGenes and Language
77
* Williams syndrome (Williams-Beuren syndrome):
- affects both males and females - microdeletion on chromosome 7, involving
>20 genes - autosomal dominant (one copy of chromosome
7 carrying the mutation is sufficient for expressing the WS phenotype)
- incidence of Ω 1 in 20,000 live births
Williams syndrome (WS)Williams syndrome (WS)

88
CA
Aetiology: Limited number of genes in the WS critical region
Cognitive profile:
VISUOSPATIAL
VOCABULARYVISUO-
PERCEPTION
FACE RECOGNITION
NUMBER PROCESSING
EXECUTIVE
CONTROL
WS?!?
WS?!?
WS: Theoretical IssuesWS: Theoretical Issues
99
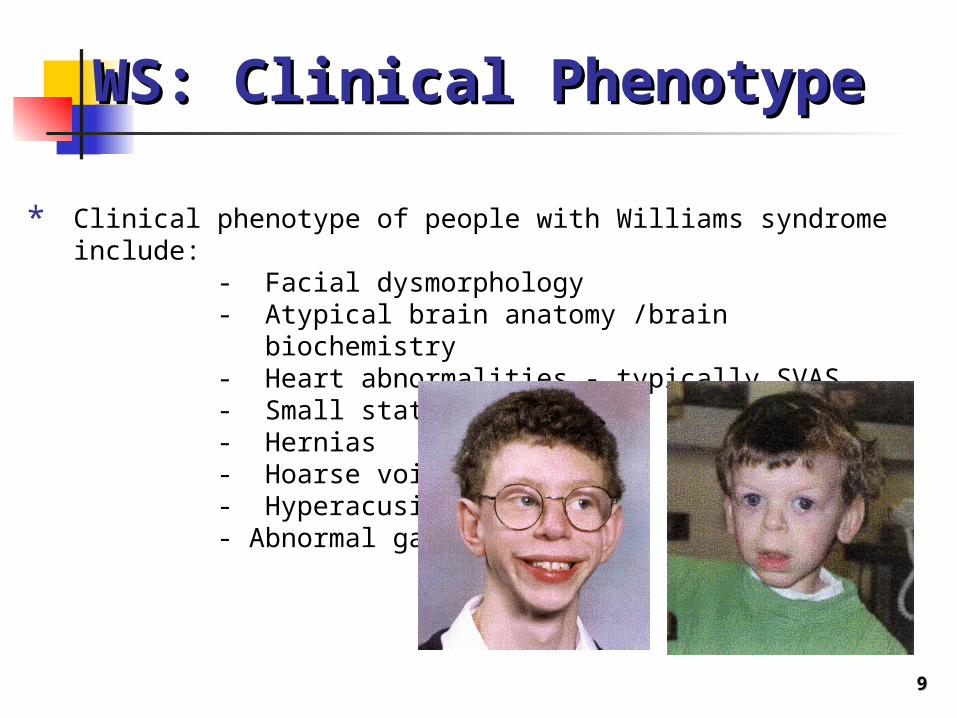
* Clinical phenotype of people with Williams syndrome include:
- Facial dysmorphology- Atypical brain anatomy /brain biochemistry- Heart abnormalities - typically SVAS- Small stature- Hernias- Hoarse voice- Hyperacusis- Abnormal gait
WS: Clinical PhenotypeWS: Clinical Phenotype

1010
FK
BP
6F
ZD
3W
ST
FB
CL
7B
TB
L2
CP
ET
R1
ST
X1A
CP
ET
R2
EL
N1
EL
N2
LIM
K1
WB
SC
R1
WB
S1
5R
FC
2C
YC
LN
2G
TF
3G
TF
2I
20+ gene deletion on chromosome 7
WS: Genotype and WS: Genotype and implicationsimplications
Are these genes selectively involved in WS difficulties? For example, debated role of ELN and LIMK1:
Frangiskakis et al. (1996) suggest a selective role for LIMK1 in visuo-spatial deficit
Tassabehji et al. (1999) argue that this is not the case, because patients with single deletions of LIMK1 do not necessarily have spatial deficits
DNA

1111
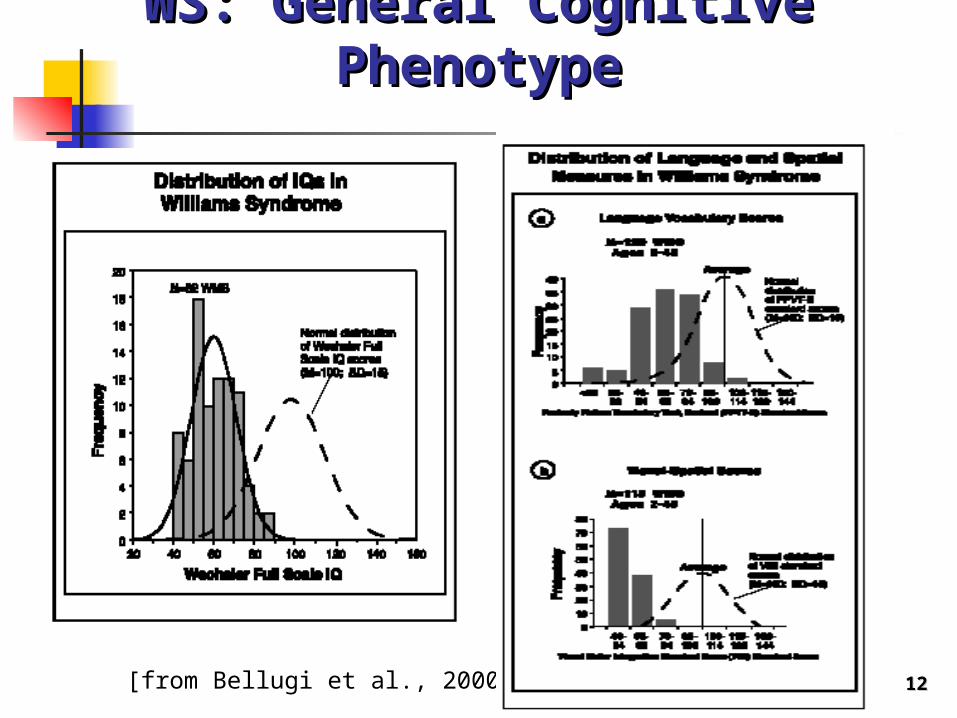
* Cognitive phenotype of adults with Williams syndrome includes:
- Low IQ (between 50-65)
BUT:- Relative strengths in language
development- Relative strengths in face recognition
and face processing- Relative weaknesses in visuo-spatial
cognition
- Dissociation between general intellect and linguistic skills ?
WS: General Cognitive WS: General Cognitive PhenotypePhenotype
1212
WS: General Cognitive WS: General Cognitive PhenotypePhenotype
[from Bellugi et al., 2000]

1313
WS adults: SemanticsWS adults: Semantics
Semantics: Large expressive and receptive vocabulary are large, but highly atypical
Examples of responses on word fluency test:
WS: e.g., brontosaurus, tyranodon, ibex, hippopotamus, bull, yak
DS: e.g., goat, bunny, rabbit
1414
“Look! Look at the car.”
WS: Language Development WS: Language Development II

1515
WS: Language Development WS: Language Development II
Understanding of First Words: Paterson et al. (1999) found WS delayed receptive vocabulary (also Singer-Harris et al., 1997)

1616
Joint attentionJoint attentionDyadic interaction
Triadic interaction
First words and joint attention: Laing et al. (2002) found that infants with WS did not follow their caregiver’s focus of attention to a third object, but remained focused on his/her face (dyadic interaction). Furthermore, their social interactions did not correlate with early vocabulary development (unlike DS and controls)
WS: Language Development IIWS: Language Development II
1717
* The study of Williams syndrome raises crucial issues (illustrated here with regard to language v. general IQ; and with regard to various linguistic processes) :
1. Even a domain of strength (language) shows atypical characteristics => Cognitive modularity and dissociations
2. WS Language does not start as an area of strength => Are deficits innately specified or the product of a developmental trajectory
Williams syndrome: SummaryWilliams syndrome: Summary
1818
* Autosomal dominant condition, associated with the silencing of a single gene (FOXP2)
* Clinical phenotype of affected members of the KE family:- Relatively low IQ- To naïve listeners, unintelligible speech,
especially early in life, and also later after intensive speech therapy
• Affected members first reported by Hurst et al. (1990) as a severe disorder of fine praxis (fine motor control)
• Later focus on their specific grammatical impairment (Gopnik & Crago, 1991)
THEORETICAL ISSUE:• Can the single gene mutated in the affected members of the
family be selectively involved in the grammatical impairments reported for the affected members?
KE family: Clinical KE family: Clinical PhenotypePhenotype

1919
Single-gene deletion on chromosome 7
(FOXP2 gene)
KE family: GenotypeKE family: Genotype
[from Vargha-Khadem, et al., 1995; Lai et al., 2001]
2020
KE adults: SyntaxKE adults: Syntax
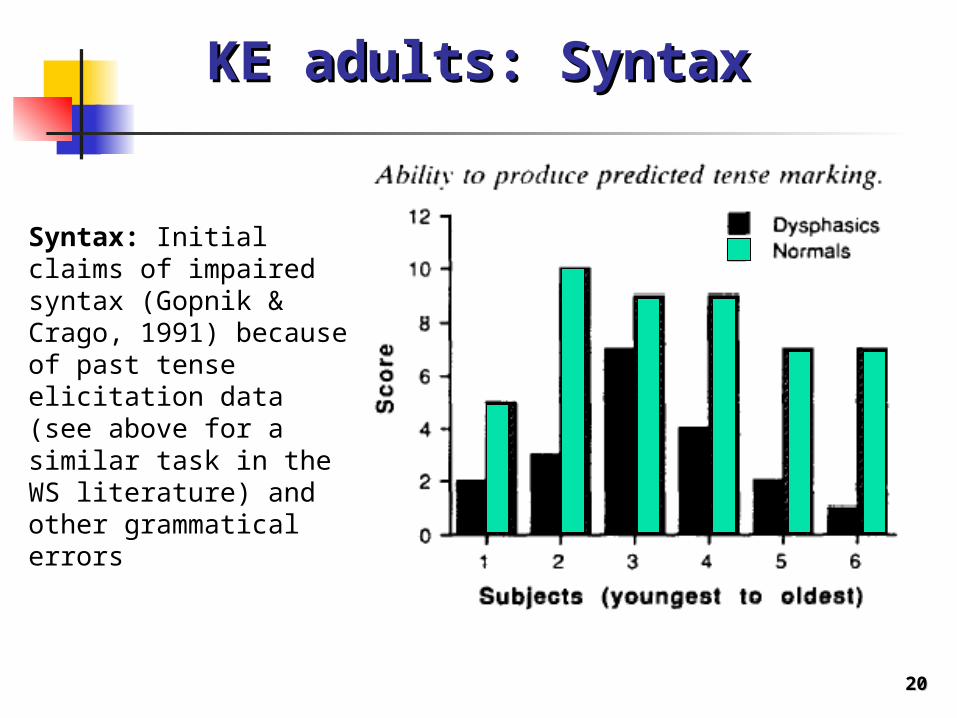
Syntax: Initial claims of impaired syntax (Gopnik & Crago, 1991) because of past tense elicitation data (see above for a similar task in the WS literature) and other grammatical errors
2121
KE adults: SyntaxKE adults: Syntax
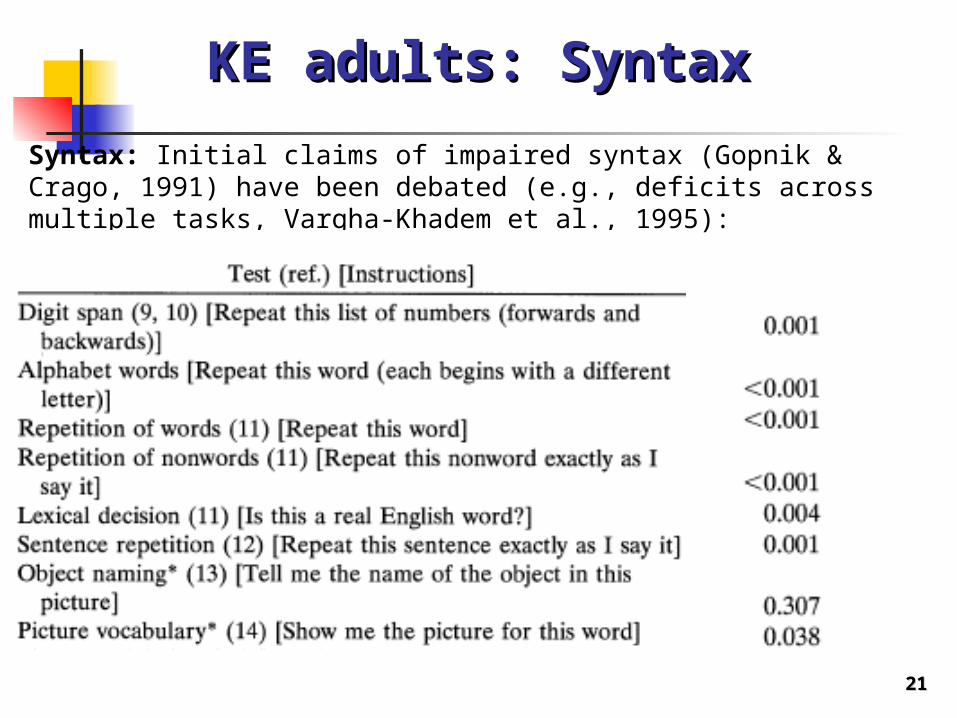
Syntax: Initial claims of impaired syntax (Gopnik & Crago, 1991) have been debated (e.g., deficits across multiple tasks, Vargha-Khadem et al., 1995):
2222
KE adults: Orofacial praxisKE adults: Orofacial praxis
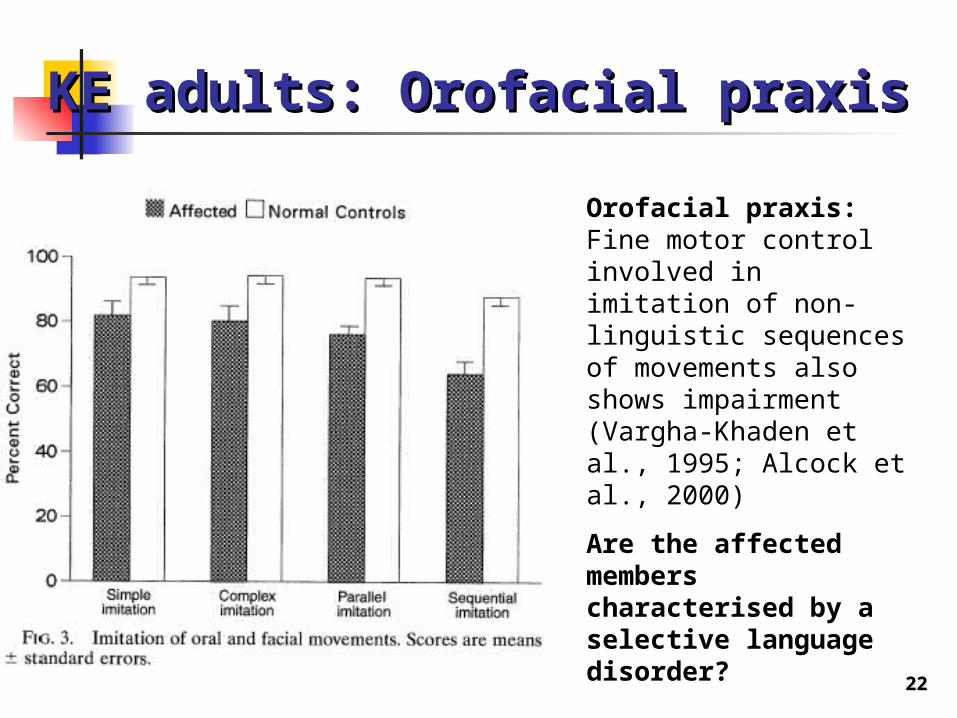
Orofacial praxis: Fine motor control involved in imitation of non-linguistic sequences of movements also shows impairment (Vargha-Khaden et al., 1995; Alcock et al., 2000)
Are the affected members characterised by a selective language disorder?

2323
KE: Developmental changesKE: Developmental changes
[from Watkins et al., 2002]
Longitudinal changes in non-verbal abilities: Longitudinal assessments of few cases show declines in non-verbal abilities over time, perhaps supporting the suggestion that their deficits are not specific to language and progressive.

2424
* The study of the KE family raises crucial issues about the relationship between a single gene and cognitive effects on language development:
1. Cognitive modularity and dissociations?
2. It especially addresses the issue of whether effects this a single-gene mutation are specific to language, or also affect other aspects of fine motor control
KE family: SummaryKE family: Summary
2525
ReferencesReferences Bellugi, U., P. Wang, T. L. Jernigan, in Atypical Cognitive Deficits in
Developmental Disorders: Implications for Brain Function, S. Broman and J. Graffman, Eds. (Erlbaum, Hillsdale, NJ, 1994), pp. 23-56.
Bellugi, U., Lichtenberger, L., Jones, W., & Lai, Z. (2000). The neurocognitive profile of Williams syndrome: A complex pattern of strengths and weaknesses. Journal of Cognitive Neuroscience, 12, Supplement, pp. 7-29.
Frangiskakis JM, Ewart AK, Morris CA, Mervis CB, Bertrand J, Robinson BF, Klein BP, Ensing GJ, Everett LA, Green ED, Proschel C, Gutowski NJ, Noble M, Atkinson DL, Odelberg SJ, Keating MT (1996). LIM-kinase1 hemizygosity implicated in impaired visuospatial constructive cognition. Cell, 86, 59-69
Gopnik, M., & Crago, M.B. (1991). Familial aggregation of a developmental language disorder. Cognition, 39, 1-30.
Grant J, Valian V, Karmiloff-Smith A. A study of relative clauses in Williams syndrome. J Child Lang. 2002 May;29(2):403-16.
Hook, E.B. (1981). Prevalence of chromosome abnormalities during human gestation and implications for studies of environmental mutagens. Lancet, 2, 169.

2626
ReferencesReferences Johnson, M.H. (1997). Developmental Cognitive Neuroscience. Oxford:
Blackwell Publishers Karmiloff-Smith, A. (2002). Development itself is the key to
understanding developmental disorders. In M.H. Johnson, Y. Munakata, & R.O. Gilmore (Eds). Brain Development and
Cognition: A Reader. Oxford: Blackwell Publishing. Karmiloff-Smith A, Tyler LK, Voice K, Sims K, Udwin O, Howlin P, Davies
M. Linguistic dissociations in Williams syndrome: evaluating receptive syntax in on-line and off-line tasks. Neuropsychologia. 1998 Apr;36(4):343-51.
Lai, C. et al. (2001). A forkhead-domain gene is mutated in a severe speech and language disorder. Nature, 413, 519-522.
Laing, E. et al. (2002) Atypical development of language and social communication in toddlers with Williams syndrome. Dev Science, 5, 233-246.
Levy Y, Smith J, Tager-Flusberg H. Word reading and reading-related skills in adolescents with Williams syndrome. J Child Psychol Psychiatry. 2003 May;44(4):576-87.
2727
ReferencesReferences Menghini D, Verucci L, Vicari S. Reading and phonological awareness
in Williams syndrome. Neuropsychology. 2004 Jan;18(1):29-37. Paterson SJ, Brown JH, Gsodl MK, Johnson MH, Karmiloff-Smith A.
Cognitive modularity and genetic disorders. Science. 1999 Dec 17;286(5448):2355-8.
Tassabehji M, Metcalfe K, Karmiloff-Smith A, Carette MJ, Grant J, Dennis N, Reardon W, Splitt M, Read AP, Donnai D. (1999). Williams syndrome: use of chromosomal microdeletions as a tool to dissect cognitive and physical phenotypes. Am J Hum Genet., 64(1):118-25.
Thomas et al., (2001). Past tense formation in Williams syndrome. Language and cognitive processes, 16, 143-176.
Vargha-Khadem, F., Watkins, K., Alcock, A., Fletcher, P. & Passingham. R. (1995). Praxic and nonverbal cognitive deficits in a large family with a genetically transmitted speech and language disorder. Proceedings of the National Academy of Sciences, USA, 92, 930-933.
Watkins, K. et al. (2002). Behavioural analysis of an inherited speech and language disorder: comparison with acquired aphasia. Brain, 125, 452 - 464.


















