1 Acute Bronchiolitis By: Dr. Manzoor Ahmed. 2 A CASE PRESENTATION BY DEPT: OF PAEDIATRICS; Acute...
43
1 Acute Bronchiolitis By: Dr. Manzoor Ahmed 1 Acute Bronchiolitis By:D r.M anzoor Ahm ed
-
Upload
kristin-thomas -
Category
Documents
-
view
220 -
download
0
Transcript of 1 Acute Bronchiolitis By: Dr. Manzoor Ahmed. 2 A CASE PRESENTATION BY DEPT: OF PAEDIATRICS; Acute...

1
Acute Bronchiolitis
By: Dr. Manzoor Ahmed
1
Acute Bronchiolitis
By: Dr. Manzoor Ahmed
2
A CASE PRESENTATION BY DEPT: OF
PAEDIATRICS;
Acute Bronchiolitis:
By: Dr. Manzoor Ahmed Registrar , paediatrics ,AKMICH
3
BRONCHIOLITIS:
A common resp. illness chracterized by inflammation of bronchioles.
Consists: acute inflammation edema and necrosis of epithelial cells lining
small airways increased mucus production bronchospasm
4
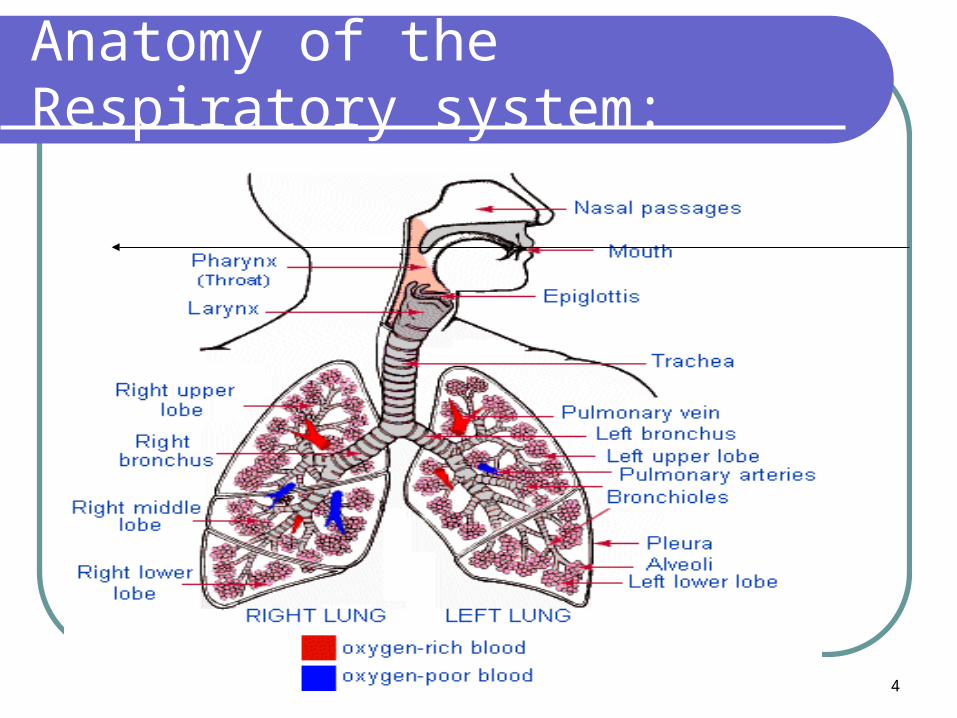
Anatomy of the Respiratory system:
5
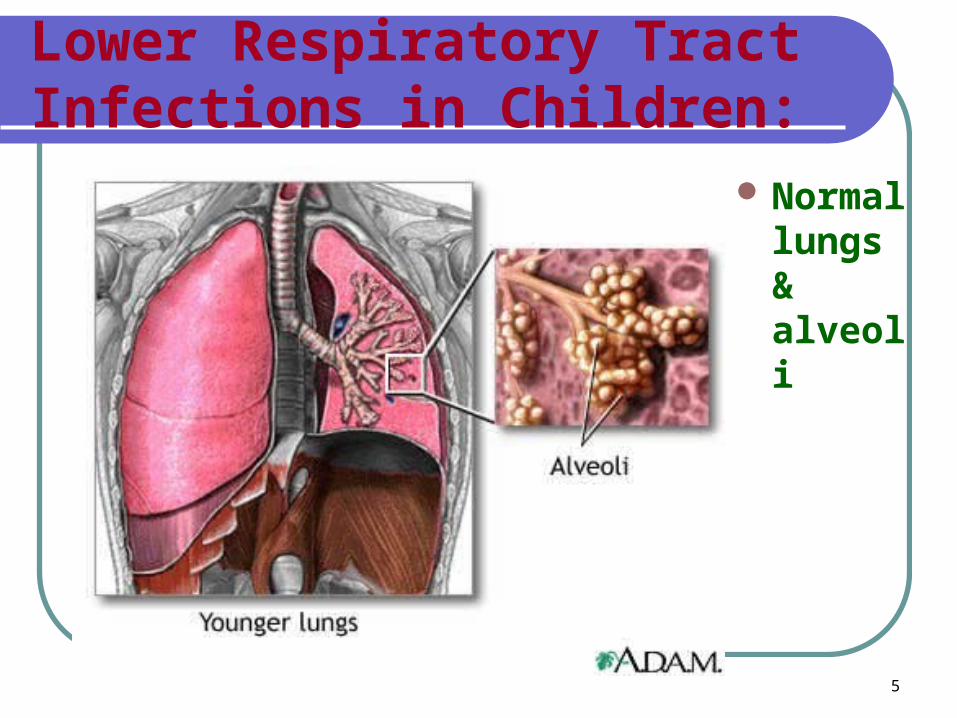
Lower Respiratory Tract Infections in Children:
Normal lungs & alveoli
6
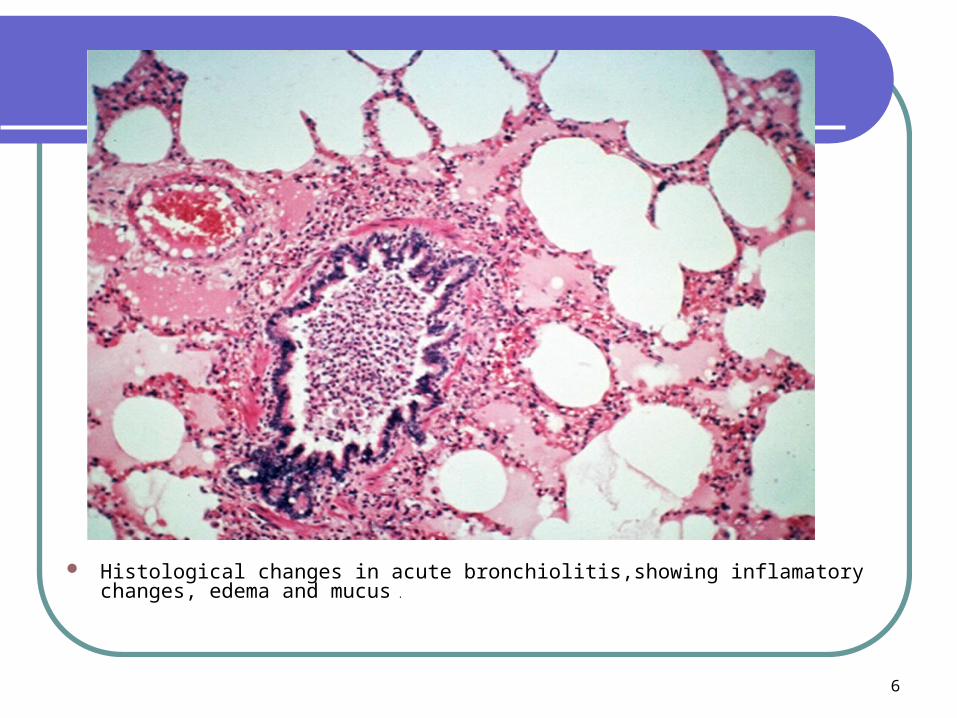
Histological changes in acute bronchiolitis,showing inflamatory changes, edema and mucus .
7
Epidemiology
Statistics:
typically occurs in 1st 2 years of lifePeak occurrence = 3 to 6 months
90% of children 0-2 yrs, are infected with RSV(respiratory synctial virus)
20% have lower respiratory infection3% hospitalized 0.002% mortality.
8
MICROBIOLOGY:
Typically caused by viruses: RSV-most common(80-90%) Parainfluenza Human Metapneumovirus Influenza Rhinovirus Coronavirus Human bocavirus
Occasionally associated with Mycoplasma pneumonia infection
9
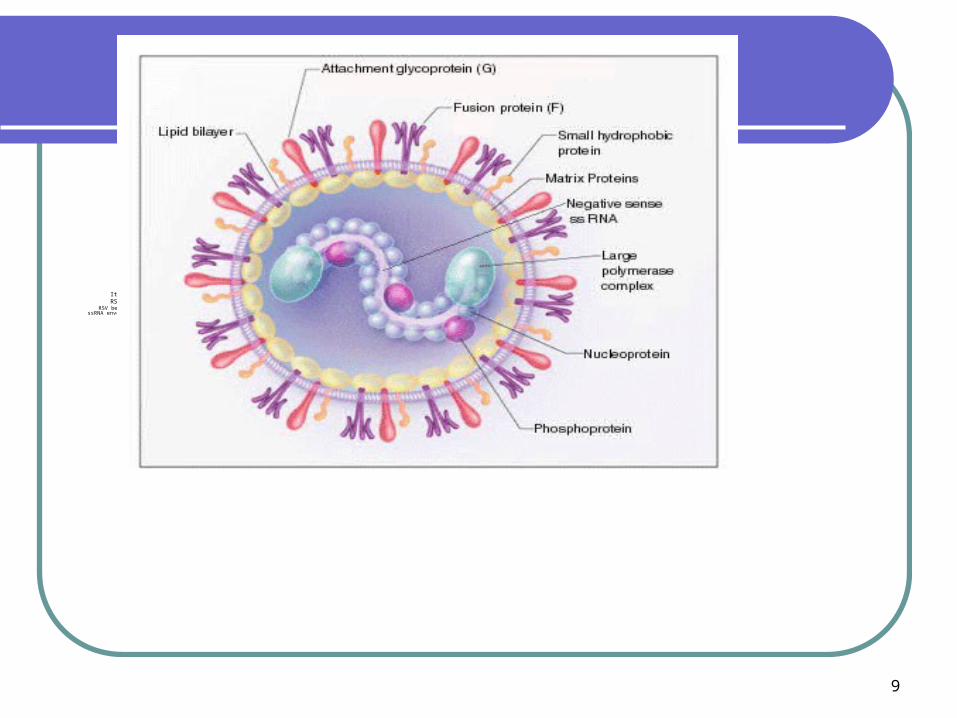
It is a RNA virus. RSV is distributed globally and an epidemic personality.
RSV belongs to the family of paramyxoviruses and is classified in the genus pneumoviruses. ssRNA enveloped virus, 120 - 300 nm in size
10
Pathophysiology:
Inflamation swelling fill with
mucus make it difficult to breath.
11
RISK FACTORS:
Prematurity Chronic heart/lung disease Weakened immune system due to illness and
medications More common in males Children who have not been breast fed Who live in crowded conditions Day care attendence Exposure to ciggerate smoke
12
RISK FACTORS FOR SEVERE DISEASE:
Prematurity Low birth weight Age less than 6-12 weeks Chronic pulmonary disease Hemodynamically significant cardiac disease Immunodeficiency Neurologic disease Anatomical defects of the airways
13
History:
Flu , cough,low grade fever,Breathing difficulty,poor feeding,cyanosis,Elder family member with flu and cough.Underlying cardiac and lung disease.
14
PHYSICAL EXAMINATION
15
Clinical features
SIGN & SYMPTOMS: Symptoms of common cold Stuffiness Runny nose Mild cough After 1 day or two; worsening of the cough & apperence of
wheezes Rapid shallow breathing Rapid heart beat Drawing in of chest & neck flaring of the nostrils Irratibility, difficult sleep & fatigue Fever poor appetite May vomit after cough In severe cases cyanosis&signs of dehydration
16
contagiousness
Air borne droplets thru infected person nose & mouth while coughing sneezing & laughing.
and also from things the person has touched, such as used tissues or toys, door handle, .
17
Incubation period days to one week.Typically last about 7 daysIn severe cases can cough for weeksPeak about the 2nd and 3rd day
DURATION & COURSE:
18
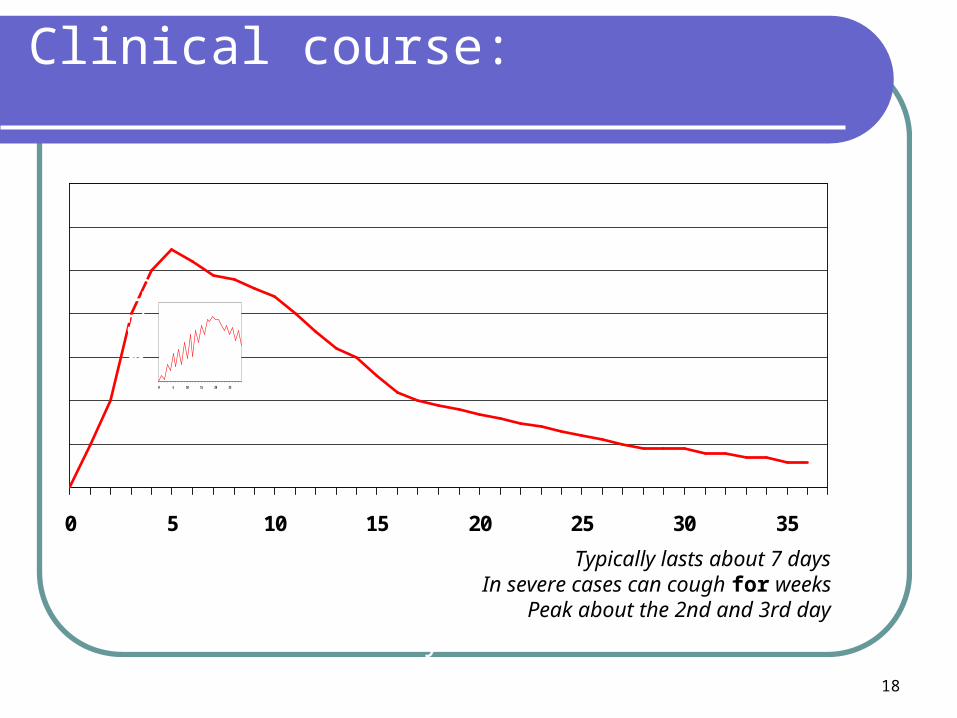
Clinical course:
0 5 10 15 20 25 30 35
Se
veri
ty
Days
0 5 10 15 20 25
Typically lasts about 7 daysIn severe cases can cough for weeks
Peak about the 2nd and 3rd day
19
DIFFERENTIAL DIAGNOSIS:
Viral-triggered asthma Bronchitis pneumonia Foreign body aspiration Gastroesophageal reflux or dysphagia leading
to aspiration Congenital heart disease or heart failure Vascular rings, bronchomalacia, complete
tracheal rings or other anatomical abnormalities

20
Complications:
After having bronchiolitis, some babies may be more likely to have a wheezy chest or cough, particularly while they have a cold. Neonates can develop APNEA,Asthma and other breathing problems later in life have also been linked with bronchiolitis
Babies with bronchiolitis can develop pneumonia,otiti media and sinusitis, . Also, babies with a lung or heart diseae, may find bronchiolitis makes their condition much worse,can lead to resp: failure and DEATH.
21
Otitis media
Otitis media a common complicationCohort study of 42 infants with bronchiolitis
62% acute OM (tympanocentesis confirmed)24% otitis media with effusion14% normal throughout course
22
Bronchiolitis Obliterans:
Inflammation of the BRONCHIOLES leading to an obstructive lung disease. Bronchioles are characterized by fibrous granulation tissue with bronchial exudates in the lumens. Clinical features include a non productive cough and DYSPNEA.
Mainly associated with adeno virus and mycoplasma.
23
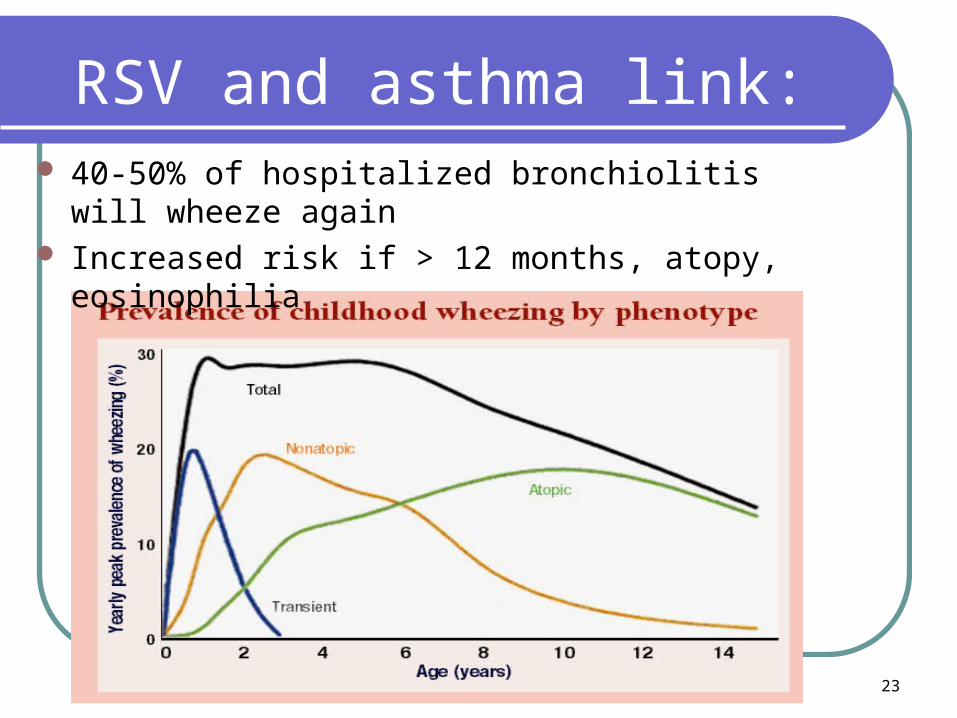
RSV and asthma link: 40-50% of hospitalized bronchiolitis will wheeze again Increased risk if > 12 months, atopy, eosinophilia
24
HOSPITALIZATION:
Children with severe disease Toxic with poor feeding, lethargy, dehydration Moderate to severe respiratory distress (RR > 70,
dyspnea, cyanosis) Apnea Hypoxemia(O2 sat: <90%) Parents unable to care for child at home.
25
INVESTIGATIONS:
Diagnosis should be made clinically, without routine use of laboratory or radiologic tests
But useful in children with complicating signs and symptoms.
CBC--to help determine bacterial illness Blood gas--evaluate respiratory failure Nasopharyngeal secretions 4 immunoflourescence + VE for RSV or other viruses (adeno , influenza
and para -influenza viruses) Chest X-ray: not routinely recommended;
should b done if atypical presentation or Suspecting complications .
26
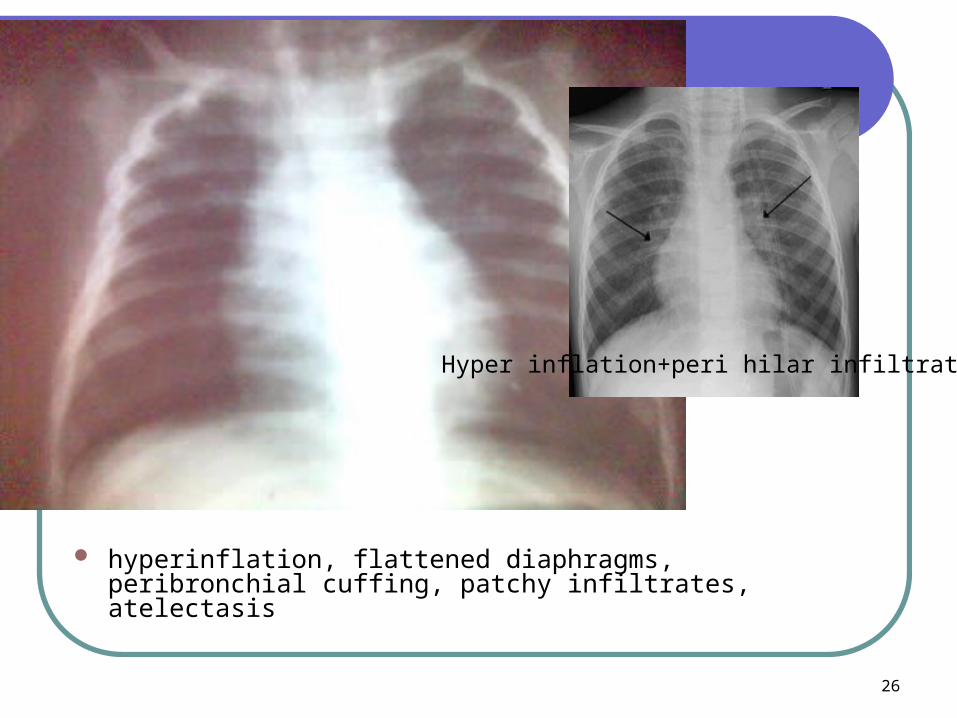
hyperinflation, flattened diaphragms, peribronchial cuffing, patchy infiltrates, atelectasis
Hyper inflation+peri hilar infiltrates
27
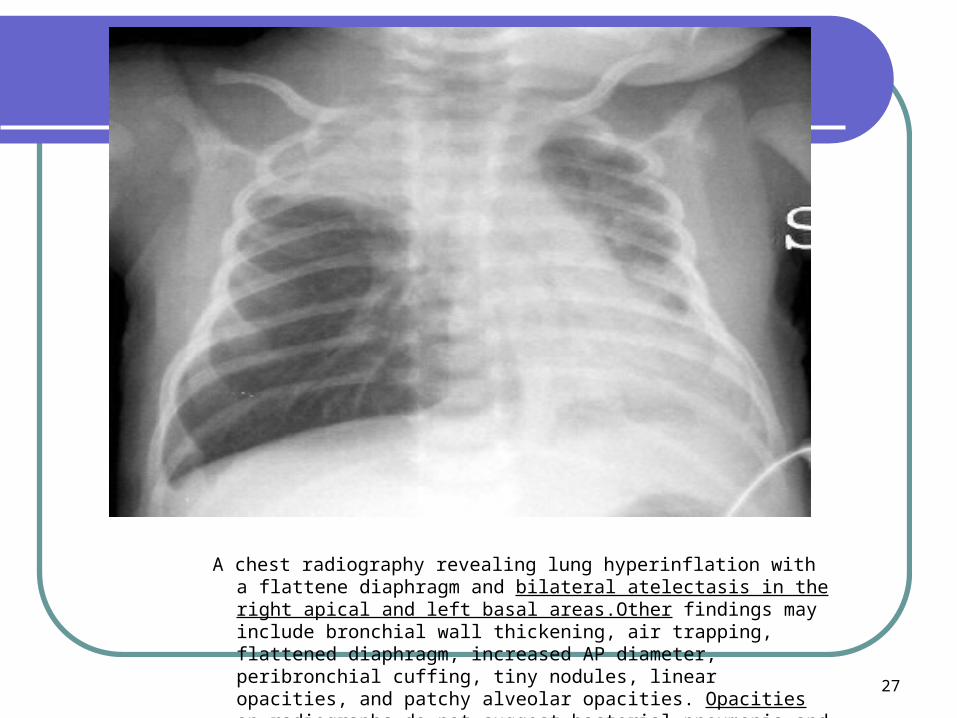
A chest radiography revealing lung hyperinflation with a flattene diaphragm and bilateral atelectasis in the right apical and left basal areas.Other findings may include bronchial wall thickening, air trapping, flattened diaphragm, increased AP diameter, peribronchial cuffing, tiny nodules, linear opacities, and patchy alveolar opacities. Opacities on radiographs do not suggest bacterial pneumonia and incorrectly lead to
inappropriate treatment with antibiotics.
28
Treatment:
HOME TREATENT: Plenty of fluids; in small
amounts,frequently. Cool-mist vapuorizer duirng winter Avoid hot water & steam humidifiers Tilt the child matress up Keep baby nose clear using bulb syringe
and saline Acetaminophen for fever
29
TREATMENT:
HOSPITAL TREATMENT: SUPPORTIVE: Most cases are mild and reqiure no specific
treatment Monitor heart & resp. rate & o2 saturation Look 4 apnea & bradycardia Give O2 if tachypaenic, or O2 sat: < 90% N.G or I.V fluids
30
TREATMENT DRUGS: Bronchodilators are NOT recommended ; but have some
benefits on clinical grounds. Nebulized & inhaled Epinephrine ( racemic and levo(1)-
epinephrine) has been shown to decrease hospitalization rates.
Inhaled hypertonic saline: Inhaled hypertonic saline (3%) appears to be effective in
improving clinical outcomes and shortening the duration of hospital stay.
steroids are ineffective. Ribavirin is an antiviral drug which does not appear to be
effective Antibiotics; are not indicated unless evidence of bacterial
pneumonia Ventilation therapy; on clinical grounds.
31
Discharge criteria:
Tolerating feeds.
Parents can handle well to baby at home and can identify ,if baby,s condition deteriorates .
family education complete
Respiratory Status:
respirations less than 70 per minute and/or no
clinical evidence of increased work of breathing or distress
parent can clear the infant’s airway using bulb
suctioning
patient’s oxygen saturation remains >92 % on
room air
32
Follow Up :
follow-up appointments to check for,
Any complications like, otitis media, effusion or asthma.
33
Hand washing is strongly recommended :
PREVENTION:
preferably with alcohol-based rubs , antimicrobial soaps
before and after contact with patient or with objects in patient’s vicinity
after removing gloves void contact with viral
infections. Educate personnel and
family members on hand hygiene
34
Attempts to provide immunity to RSV: Passive immunity via hyper immune globulin. Monoclonal antibody to F protein (palivizumab)
55% hospitalizations for preterm/chronic lung disease 45% hospitalizations for congenital heart disease
Palvizumab injection, is given on monthly basis during rsv season.
RSV immunoprophylaxis(passive immunization) RSV IVIG /monoclonal
antibody : Palivizumab (Synagis®)
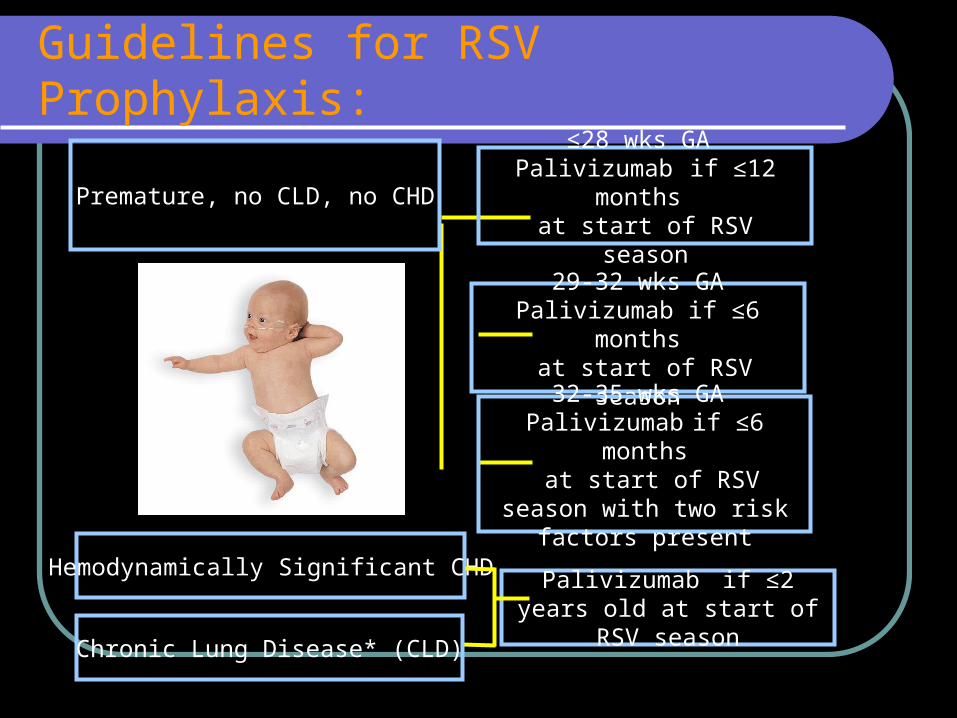
35*Receiving medical therapy for CLD within 6 months
Guidelines for RSV Prophylaxis:
Premature, no CLD, no CHD
29-32 wks GAPalivizumab if ≤6 months at start of RSV season
≤28 wks GA Palivizumab if ≤12 months
at start of RSV season
32-35 wks GA Palivizumab if ≤6 months
at start of RSV season with two risk factors present
Chronic Lung Disease* (CLD)
Hemodynamically Significant CHDPalivizumab if ≤2 years old
at start of RSV season
36
American Academy of Pediatrics (AAP) Guidelines for palvizumab:
Infants born at 32 weeks of gestation or earlier may benefit from RSV prophylaxis, even if they do not have CLD. For these infants, major risk factors to consider include their gestational age and chronologic age at the start of the RSV season. Infants born at 28 weeks of gestation or earlier may benefit from prophylaxis during their first RSV season, whenever that occurs during the first 12 months of life. Infants born at 29 to 32 weeks of gestation
may benefit most from prophylaxis up to 6 months of age. Prophylaxis should be considered for infants between 32 and 35 weeks of
gestation who are younger than 6 months of age at the start of the RSV season if 2 or more of these risk factors are present.
Epidemiologic data suggest that RSV infection is more likely to lead to hospitalization for these infants when the
following risk factors are present: child care attendance, school-aged siblings, exposure to environmental air pollutants, congenital abnormalities of the airways, or severe neuromuscular disease.
37
Palivizumab or RSV-IGIV prophylaxis should be considered for infants and children younger than 2 years of age with CLD who have required medical therapy (supplemental oxygen, bronchodilator, diuretic or corticosteroid therapy) for CLD within 6 months before the anticipated start of the RSV season.
Children who are 24 months of age or younger with hemodynamically significant cyanotic and acyanotic congenital heart disease will benefit from 5 monthly intramuscular injections of palivizumab (15 mg/kg).
Once a child qualifies for initiation of prophylaxis at the start of the RSV season, administration should continue throughout the season and not stop at the point an infant reaches either 6 months or 12 months of age.
Synagis® (palivizumab) is preferred for most high-risk children because of its ease of administration, safety, and efficacy. It also does not interfere with live vaccines such as MMR and varicella.
Children with more severe CLD may benefit from two consecutive years of RSV prophylaxis. This should be individualized for each patient, as should the duration of prophylaxis.
RSV prophylaxis should be initiated just before the onset of the RSV season and terminated at the end of the RSV season, based on local hospitalization and virology data.
Strict observance of infection control practices, including screening and isolation of RSV-infected children, especially in NICU and PICU settings is critical.
38
development of rapid, cost-effective tests for viruses other than RSV that may also play a role in bronchiolitis
studies to determine if there are selected patients who may benefit from bronchodilators or corticosteroids
clinical studies of the target SpO2 for the most efficient use of oxygen and oxygen monitoring
development of new therapies including new antiviral medications
continued research into the development of an RSV vaccine
continued development of immunoprophylaxis that would require fewer doses and decreased cost
Future Investigations
39
Message to take home.
1. Diagnosis should be made clinically, without routine use of laboratory or radiologic tests, and should include assessment of risk factors for severe disease (e.g., prematurity, underlying lung or heart disease, and immunodeficiency)
2. Bronchodilators should not be used routinely for management. An optional trial of an - or ß-agonist should be continued only if objective evaluation indicates a clinical response.
3. Routine use of corticosteroids is not recommended4. Routine use of ribavirin is not recommended5. Antibiotics should be used only when bacterial infection is clearly
present6. Assessment of hydration status and oral intake is strongly
recommended. IV fluids should be given as necessary7. Routine chest physiotherapy is not recommended
Message to take home
Encourage breast feeding.Avoid contact with smoking.Pay more attention to high risk group.
40
41
Message to take home
8. Supplemental O2 and continuous monitoring are not routinely recommended unless Spo2 persistently falls below 90%. The infant’s clinical work of breathing may also be used to determined need for supplemental oxygen
9. Prophylactic palivizumab is recommended in selected high-risk children with prematurity or heart or lung disease
10. Hand washing is strongly recommended, preferably with alcohol-based rubs or antimicrobial soaps

42
43










![[OPTIMUS BONUS - Bronchiolitis]...High Flow therapy in paediatrics and a committee member on the Research Committee of the World Federation of Pediatric Intensive and Critical Care](https://static.fdocuments.us/doc/165x107/5f101a5d7e708231d44775b3/optimus-bonus-bronchiolitis-high-flow-therapy-in-paediatrics-and-a-committee.jpg)