
1 A Quick Glance at Meaningful Use “Proposed” Modifications for 2015 and MIPS September 16, 2015...
23
1 A Quick Glance at Meaningful Use “Proposed” Modifications for 2015 and MIPS September 16, 2015 Antonio Vega Sandy Swallow
-
Upload
valentine-tucker -
Category
Documents
-
view
215 -
download
0
Transcript of 1 A Quick Glance at Meaningful Use “Proposed” Modifications for 2015 and MIPS September 16, 2015...

1
A Quick Glance at Meaningful Use “Proposed” Modifications for 2015 and MIPS
September 16, 2015Antonio Vega Sandy Swallow
2
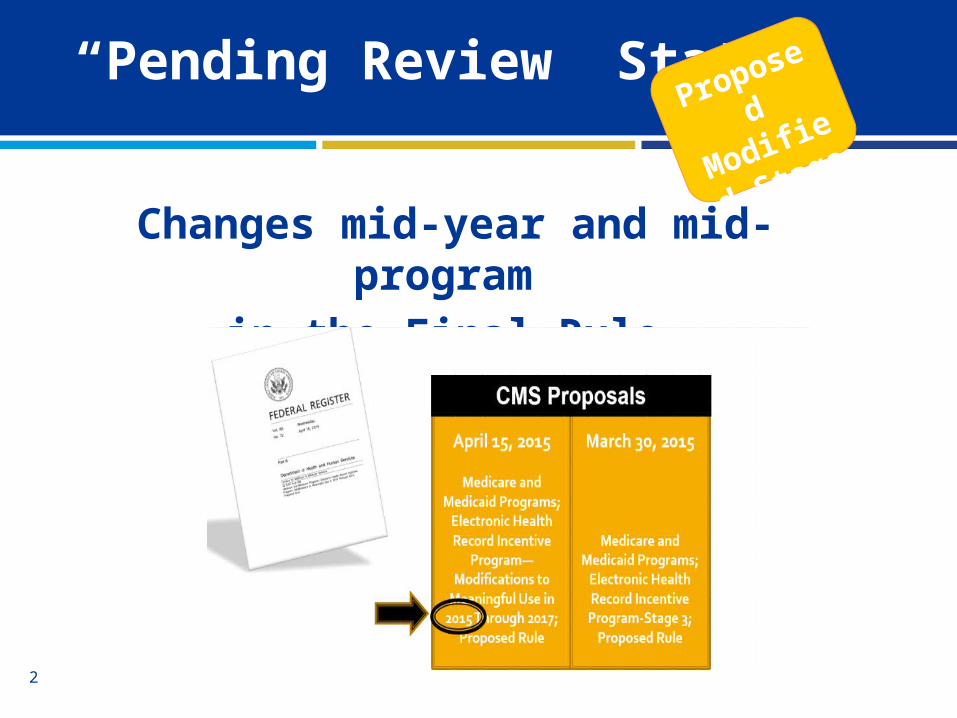
“Pending Review” Status
Changes mid-year and mid-program in the Final Rule
Proposed
Modified
Stage 2
3
A Quick Glance:• Program goals and long term program alignment• Updated participation timeline • Significant program changes for 2015• Medicare Incentives beyond 2017• MIPS
Today’s ObjectivesProposed
Modified
Stage 2
4
Modified Stage 2 Goals• Align with Stage 3 proposed rule• Align reporting period with full calendar year for ALL• Change reporting period to 90-day period in 2015
– EH 10/1/2014 to 12/31/15– EP 1/1/15 to 12/31/15
• Synchronize objectives and measures to reduce burden– Remove redundant, duplicative, and topped out– Modify patient action measures related to patient engagement
Program GoalsProposed
Modified
Stage 2
5
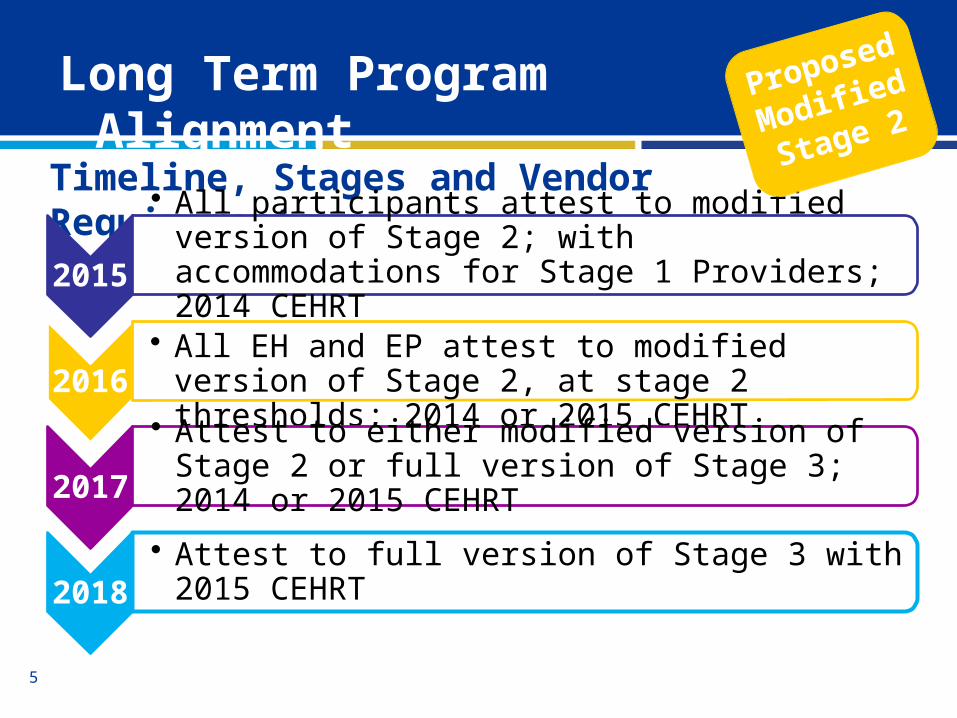
Timeline, Stages and Vendor Requirements
2015
• All participants attest to modified version of Stage 2; with accommodations for Stage 1 Providers; 2014 CEHRT
2016
• All EH and EP attest to modified version of Stage 2, at stage 2 thresholds; 2014 or 2015 CEHRT
2017
• Attest to either modified version of Stage 2 or full version of Stage 3; 2014 or 2015 CEHRT
2018
• Attest to full version of Stage 3 with 2015 CEHRT
Long Term Program Alignment Proposed
Modified
Stage 2
6
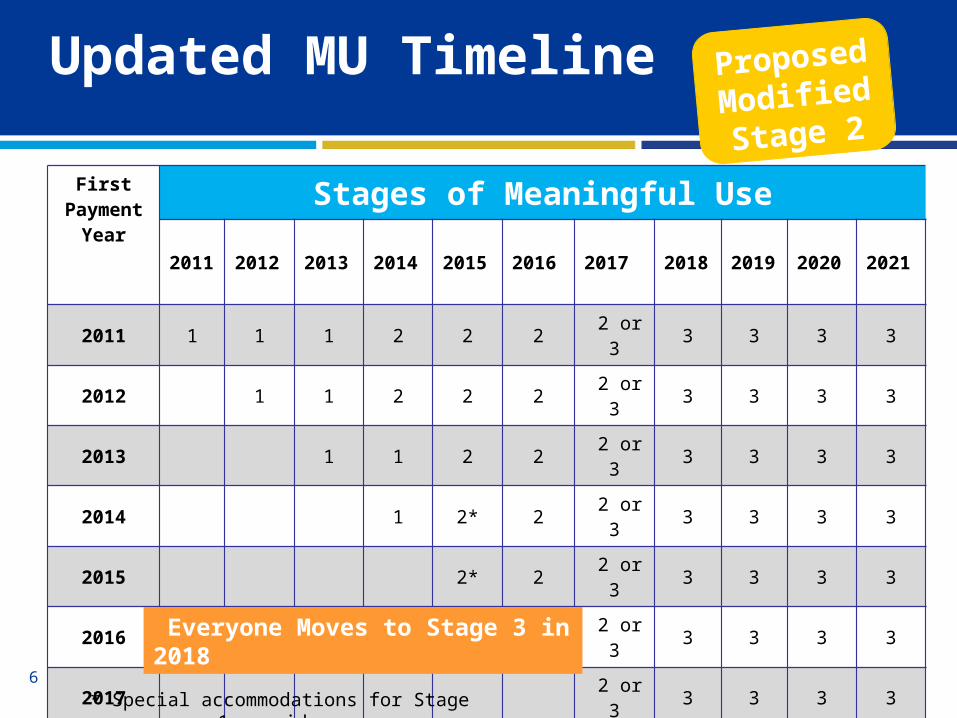
Updated MU Timeline Proposed
Modified Stage 2
First Payment
YearStages of Meaningful Use
2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021
2011 1 1 1 2 2 2 2 or 3 3 3 3 3
2012 1 1 2 2 2 2 or 3 3 3 3 3
2013 1 1 2 2 2 or 3 3 3 3 3
2014 1 2* 2 2 or 3 3 3 3 3
2015 2* 2 2 or 3 3 3 3 3
2016 2 2 or 3 3 3 3 3
2017 2 or 3 3 3 3 3
* Special accommodations for Stage 1 providers
Everyone Moves to Stage 3 in 2018

7
Program Changes
• 9 Core Criteria
• 1 Public Health Criterion
Proposed
Modified
Stage 2
Applies to all eligible professionals, hospitals and critical access hospitals

8
Objective EP Measure EH MeasureProtect Elec Health Info Conduct SRA/correct deficiencies Same
Clinical Decision Support 5 rules related to 4+ CQM; drug/drug and drug/allergy interaction check
Same
CPOE >60% med, >30% lab, > 30% radiology Same
eRx >50%; drug formulary query >10%; drug form. query
Summary of Care Use CEHRT to create summary; >10% electronically transmit
Same
Patient Specific Education >10% unique patients Same
Medication Reconciliation >50% transitions of care Same
Patient Elec Access (VDT) >50% timely access; 1 patient VDT Same
Secure Messaging Fully enabled n/a
Public Health 5 measure options 6 measure options
MU Objectives 2015 -2017

9
Removed Measures
• Record Demographics• Record Vital Signs• Record Smoking Status• Structured Lab Results• Patient List• Electronic Notes• Imaging Results• Family Health History
• Summary of Care– Measure 1 and 3
• Clinical Summaries (EP)• Patient Reminders (EP)• eMAR (EH)• Advanced Directive (EH)• Structure Labs to
Ambulatory Providers (EH)
Proposed
Modified
Stage 2
10
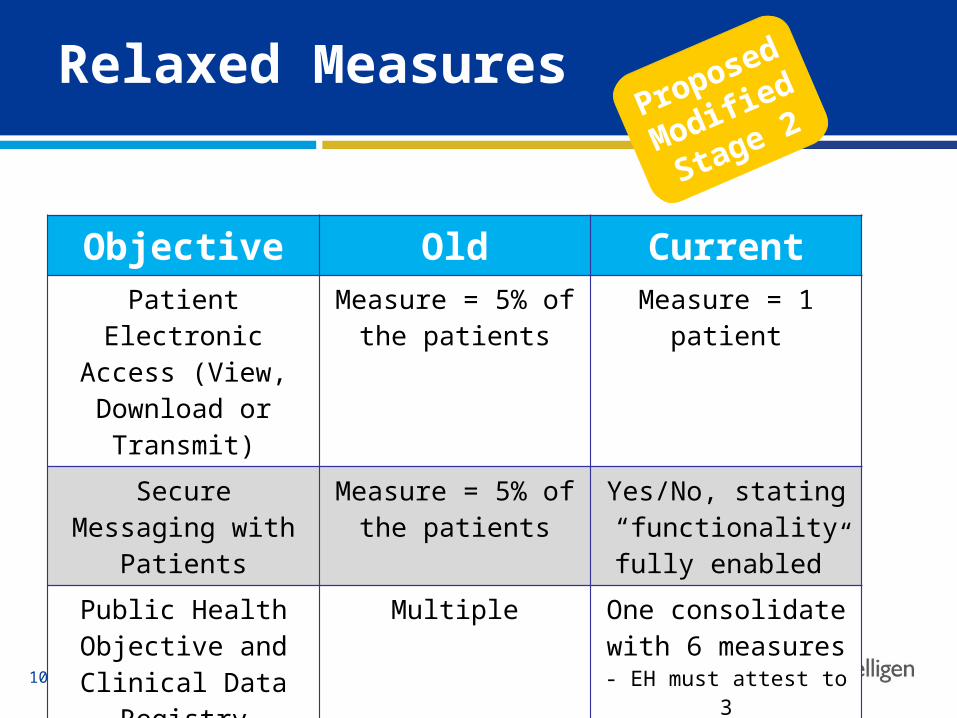
Relaxed MeasuresProposed
Modified
Stage 2
Objective Old CurrentPatient Electronic
Access (View, Download or Transmit)
Measure = 5% of the patients
Measure = 1 patient
Secure Messaging with Patients
Measure = 5% of the patients
Yes/No, stating “functionality fully
enabled”Public Health Objective
and Clinical Data Registry
Multiple One consolidate with 6 measures
- EH must attest to 3- EP must attest to 2

11
Modified Stage 2 Objectives
Public Health and Clinical Data Registry (CDR) Reporting
Attest to any 2 (EP) or 3 (EH)…1. Immunization registry reporting (bi-directional)2. Syndromic surveillance reporting3. Case reporting4. Public health registry reporting*5. Clinical data registry reporting*6. Electronic Reportable Laboratory Reporting
https://www.idph.state.ia.us/meaningful_use.aspm
*May choose to report to more than one registry to meet the number of measures required

12
Modified Stage 2 - Clinical Quality Measures
Clinical Quality Measures
• 9 measures out of 64, covering at least three domains
• None are “required” but some are recommended
• Zero in the denominator is a positive response
• Can report through the PQRS portal
• CQM reporting period can be different than the rest of MU

13
Accommodations for Stage 1 Providers
You are attesting to Stage 1 in 2015…
• Stage 1 based on the same 10 objectives
• Attest to Stage 1 thresholds• Will take an exclusion for the
Stage 2 measures if there is no equivalent Stage 1 measure
• Menu objectives move to core objectives

14
Objective Alternate Measure, Exclusion/SpecificationsProtect Elec Health Info None
CDS Implement one CDS rule EP; no exclusion EH
CPOE >30% med, exclusion for lab and radiology
eRx >40 % EP; exclusion EH Stage 1 and Stage 2 did not intend to demonstrate as a Menu in Stage 2
Summary of Care Exclusion
Pt-Specific Education Exclusion, if did not intend to demonstrate as a Menu objective in Stage 1
Med. Reconciliation Exclusion, if did not intend to demonstrate as a Menu objective in Stage 1
Pt. Electronic Access Exclusion
Secure Electronic Messaging Exclusion
Public Health None
Accommodations for Stage 1 Providers
15
Hospital-Based EPsProposed
Modified
Stage 2
Qualifications for Hospital-Based EPs• Include place of service 22 (outpatient) for those EPs
considered hospital-based*• EP is ineligible for incentive payment and payment
adjustments if >90% covered professional services in sites of service identified as:– POS 21 (inpatient)– POS 22 (outpatient)*– POS 23 (emergency room)

16
• Attestation will not begin until after January 1, 2016
• In 2015 only - First time EH and EP participants will have until February 29, 2016 to attest; but may be subject to a payment adjustment on claims submitted prior to attestation to MU for an EHR reporting period in 2015
Attestation UpdatesProposed
Modified
Stage 2
17
• Hardship Exceptions were due July 1, 2015– Lack of Infrastructure– Unforeseen and/or Uncontrollable Circumstances– Lack of Control over the Availability of Certified EHR Technology– Lack of Face-to-Face Interaction
• Began in January 2015; 1% and increases every year until 2018 when government makes a decision
• Annual attestation required to avoid adjustment
Payment Adjustments Facts
18
Merit-Based Incentive Payment System (MIPS)
• Federal Quality Program combines PQRS, MU and VBM• Replaces the SGR reimbursement formula• Goal is to lower cost while improving quality of care by
rewarding high-performers and penalizing low-performers based on a composite threshold score
• 2017 will be the first performance year
Medicare Incentives Beyond 2017
19
• 2019 & 2020 (First two years)– Physicians, PAs, Certified Registered Nurse Anesthetists, NPs, Clinical
Nurse Specialists, Dentists, Podiatrist and Groups that include such professionals
• 2021 onward– Dietitians, Midwives, Psychologist and most other healthcare
professionals
• Excluded EPs– Qualifying APM participants– First year Medicare participation– Low volume threshold exclusions
• MIPS DOES NOT apply to RHC or FQHC payments
Eligibility for MIPS

20
Potential Annual Score 0-100 Points
Quality 30 pts.
Resource Use 30 pts.
Meaningful Use 25 pts.
Clinical Practice Improvement
15 pts.
MIPS Assessment Categories

21
Payment Alignment

22
• Telligen: Quality Innovation Network-Quality Improvement Organization (QIN-QIO) for Colorado, Illinois and Iowa
Telligen QIN QIO

23
Thank you!
QIN-QIO Contact:Sandy Swallow515.223.2105
IHIN Contact:Antonio Vega515.362.8311
This material was prepared by Telligen, the Medicare Quality Innovation Network Quality Improvement Organization, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 11SOW-QIN-B4-9/2015-11239


















