
1 29-Year-Old Female with Ulcerative...
12
WWW.METAMETRIX.COM 1 29-Year-Old Female with Ulcerative Colitis
Transcript of 1 29-Year-Old Female with Ulcerative...
| 1
w w w. m e ta m e t r i x . c o m
1 29-Year-OldFemalewithUlcerativeColitis
2 | metametrix —CaseStudiesinIntegrativeandFunctionalMedicine
1 ( 8 0 0 ) 2 2 1 - 4 6 4 0
ULCERATIVE COLITISUlcerative colitis (UC) and Crohn disease are the principal constituents of the gastrointestinal inflammatory condition group known as Inflammatory Bowel Disease (IBD). IBD is one of the five most common gastrointestinal diseases in the United States. Because there is no recognized cure, patients require a lifetime of care. Annually, the health care cost of IBD exceeds $1.7 billion and more than 115,000 patients are placed on disability.1 IBD is associated with an increased risk for intestinal cancers.2 Up to 75% of Crohn disease patients and 33% of UC patients will require surgery (colectomy).1 The case below describes a patient with pancolitis, a severe form of UC that involves the whole colon. Pancolitis that is non-responsive to medications, as was the case with this individual, frequently requires surgical intervention.3
29-Year-Old Female with Ulcerative Colitis/PancolitisAdditional Symptoms and Conditions Chronic diarrhea, erythema nodosum, weight
loss, fatigue; medications ineffective
Lifestyle Factors Standard American diet, high stress due to illness
Medications Mesalamine (Asocol®), azathioprine (Imuran®), prednisone
Tests Used Food- specific IgG4 antibodies, microbial stool analysis using DNA identification; celiac genes and serology
Imbalances Identified Elevated food-specific IgG4 antibodies, intestinal dysbiosis and parasitosis
Treatments Diet modification, albendazole, digestive enzymes, antimicrobial and nutritive botanicals, probiotics
Outcome Weight normalization (gain), 80% resolution of symptoms, improved energy, daily use of medications no longer required
Discussion/Significance
The testing and treatment used in this case resulted in dramatic clinical improvement and enhanced quality of life. It is probable that the treatment prevented the need for surgical intervention. Given the grim epidemiological statistics of IBD, research investigating the efficacy of this cost-saving, multifactorial, integrative approach is highly recommended.
29-Year-OldFeMalewIthUlCeratIveCOlItIS | 3
w w w. m e ta m e t r i x . c o m
CASE HISTORYEMwasa29-year-oldfemalepresentingwithextremelyactiveulcerativecolitis(UC).Colonoscopyhaddetectedpancolitis.Shewasatherlowestbodyweightsinceadulthood.Shewastakingprednisone,mesalamine(acyclooxygenaseandprostaglandinblocker),andazathioprine(animmunosuppressivedrugwithunknownmechanism),butthesemedica-tionswerenotbringingherrelief.Shehadchronicdiarrheaandseverefatigue.Shealsohaderythemanodosum(nodularerythematouseruptionsonthelowerlegs)whichpresentedaslarge,multipleoozinglesionswhichwereprecededbybruises.Fortheerythemanodosum,shewasprescribedatwo-monthcourseoftheantibioticcephalexin.Becauseofthedebilityofherillness,EMstatedthatshecouldn’tbeamothertohertwochildren.
Formostofherlife,EMhadeatenastandardAmericandiet(SAD)characterizedbyhighintakeofredmeat,sugarydessertsanddrinks,high-fatfoods,dairyproducts,eggs,andrefinedgrains.Tenmonthspriortoherinitialvisit,anIgG4foodantibodytestreportedsignificantreactionstoyeast,gluten,anddairy,andsheeliminatedfoodscontainingthesecomponentsfromherdiet.Celiacserologyandgeneswerealsotestedforandfoundtobenegative.Evenwiththeadoptionofthisoligoantigenicdietbasedonherspecificreactions,shenotednosignificantchangetoherconditionatthetimeofherinitialvisit.
EM’sfamilyhistorydidnotincludeinflammatoryboweldiseaseorotherautoimmunecon-ditions.Herhusbandhadirritablebowelsyndrome.AlthoughEMwasunderagreatdealofstressbecauseofherconditionandhadeatentheSADformostofherlife,therewerenootherapparentcontributinglifestylefactors.
Initial Laboratory ResultsLaboratory tests ordered and rationale:
1. Previous testing:Celiacserologyandceliacgenesweretestedandfoundtobenegative.IgG4food-specificantibodytestingidentifiedsignificantantibodyelevationstoyeast,glutenanddairy.Adversefoodreactions,includinganassociationwithceliacdisease,havebeenidentifiedinIBD.4-5Removalofoffendingfoodshasbeennotedtoimprovesymptoms.NotelaboratoryfindingsdemonstrateapositiveglutenIgG4reaction,butfrankceliacdisease(glutenintolerance)wasruledout,suggestinganalternativeinflammatoryresponsetogluten.
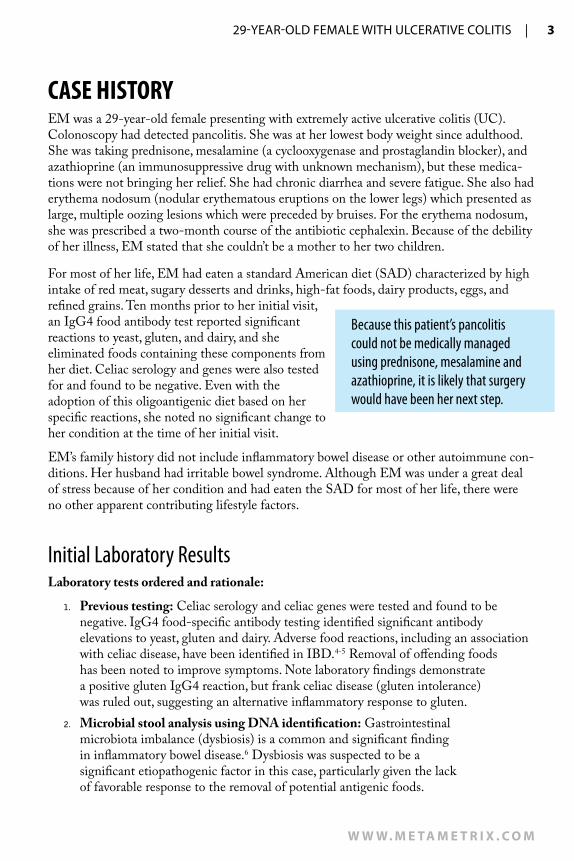
2. Microbial stool analysis using DNA identification:Gastrointestinalmicrobiotaimbalance(dysbiosis)isacommonandsignificantfindingininflammatoryboweldisease.6Dysbiosiswassuspectedtobeasignificantetiopathogenicfactorinthiscase,particularlygiventhelackoffavorableresponsetotheremovalofpotentialantigenicfoods.
Because this patient’s pancolitis could not be medically managed using prednisone, mesalamine and azathioprine, it is likely that surgery would have been her next step.
4 | metametrix —CaseStudiesinIntegrativeandFunctionalMedicine
1 ( 8 0 0 ) 2 2 1 - 4 6 4 0
Accession Number:A1002190015
Patient: Sample Case
Comment:Reprinted: Fax:Telephone:
Date Collected:
Sex:Age: 29 Female
2/18/10
Report Date:Date Received: 2/19/10
(770) 446-4583(770) 441-22372/23/10
Reference Number:
Date of Birth: 09/10/1980
2/19/10
Metametrix
3425 Corporate WayDuluth, GA 30096
3425 Corporate WayDuluth, GA 30096
770.446.5483 Fax:770.441.2237
2105 Microbial Ecology Profile Methodology: DNA Analysis, GC/MS, Microscopic,Colorimetric, Automated Chemistry, ELISA
80%60%40%20%
5th4th3rd2nd1stResultsCFU/gram
95%Reference
Range
Consistency = Formed/NormalPercentile Ranking by Quintile
Predominant Bacteria E+007E+007
Units and Reference RangesOrganisms are detected by DNA analysis.
One colony forming unit (CFU) is equivalent to one bacterium. Each genome detected represents one cell, or one CFU. Results are expressed in scientific notation, so an organism reported as 2.5 E7 CFU/gram is read as 25 million colony forming units per gram of feces. The cutoff for significance of Opportunistic Bacteria has been set at 1.0E+ 005 (100,000). These are levels above which clinically significant growth may be present. Rather than reporting semi-quantitative +1 to +4 levels, the new methodology provides full quantitative analysis.
Predominant Bacteria play major roles in health. They provide colonization resistance against potentially pathogenic organisms, aid in digestion and absorption, produce vitamins and SCFA's, and stimulate the GI immune system. DNA probes allow detection of multiple species (sp.) within a genus, so the genera that are reported cover many species.
Obligate anaerobes
Bacteroides sp. >= 1.37.76.71.6
Clostridia sp. >= 1.010.96.21.5
Prevotella sp. >= 1.11.86.21.6
Fusobacteria sp. >= 1.125.57.41.6
Streptomyces sp. >= 1.02.35.81.6
Mycoplasma sp. >= 1.21.86.21.7
Facultative anaerobes
Lactobacillus sp. >= 1.23.67.81.8
Bifidobacter sp. >= 1.822.97.62.3
Obligate aerobes
Escherichia coli >= 1.16.97.71.7
Opportunistic BacteriaOpportunistic Bacteria may cause symptoms and be associated with disease. They can affectdigestion and absorption, nutrient production, pH and immune state. Antibiotic sensitivity testswill be performed on all opportunistic bacteria found, although clinical history is usually considered to determine treatment since the organisms are not generally considered to be
Enterobacter sp. 5.3E+008 H <=1.0E+005
Georgia Lab Lic. Code #067-007CLIA ID# 11D0255349
New York Clinical Lab PFI #4578Florida Clinical Lab Lic. #800008124
Laboratory DirectorsJ. Alexander Bralley, PhD
Robert M. David, PhDPage 1
Figure 1. Microbial stool analysis using DNA identification. Opportunistic bacteria present. Imbalance in the pattern of predominant bacteria suggested dysbiosis.
Accession Number:A1002190015
Patient: Sample Case
Comment:Reprinted: Fax:Telephone:
Date Collected:
Sex:Age: 29 Female
2/18/10
Report Date:Date Received: 2/19/10
(770) 446-4583(770) 441-22372/23/10
Reference Number:
Date of Birth: 09/10/1980
2/19/10
Metametrix
3425 Corporate WayDuluth, GA 30096
3425 Corporate WayDuluth, GA 30096
770.446.5483 Fax:770.441.2237
2105 Microbial Ecology Profile Methodology: DNA Analysis, GC/MS, Microscopic,Colorimetric, Automated Chemistry, ELISA
Pathogenic Bacteria95% Reference
Range
<=1.0E+005<0.01Helicobacter pylori<=1.0E+005H5.5E+008Campylobacter sp.<=1.0E+005<0.01Clostridium difficile<=1.0E+005H5.9E+008E.H.E. coli
Yeast/FungiNo clinically significant amounts. Yeast/Fungi
Yeast overgrowth has been linked to manychronic conditions, in part because of antigenic responses in some patients to even low rates ofyeast growth. Potential symptoms include diarrhea, headache, bloating, atopic dermatitis and fatigue. Positives are reported as +1, +2, +3 or +4 indicating >100, >1000, >10000 or >100000 pg DNA/g.
ParasitesPositive NegNecator americanus (hookworm)
ParasitesParasite infections are a major cause of
non-viral diarrhea. Symptoms may include constipation, gas, bloating, increased allergy response, colitis, nausea and distention.
Adiposity Index<= 8078Firmicutes>= 2022Bacteroidetes
The Adiposity Index is derived by using DNprobes that detect multiple genera of the phyla Firmicutes and Bacteroidetes. Abnormalities of these phyla may be associated with increased caloric extraction from food.
Drug Resistance GenesaacA, aphD Neg gyrB, ParE Neg
mecA Neg PBP1a, 2B NegvanA, B, and C Neg
These test results are not for the diagnosis of disease. They are intended to provide nutritional guidelines to qualified healthcare professionals with full knowledge of patient history and concerns to assist in their design of an appropriate healthcare program.
Page 2
Laboratory DirectorsJ. Alexander Bralley, PhD
Robert M. David, PhD
New York Clinical Lab PFI #4578Florida Clinical Lab Lic. #800008124
Georgia Lab Lic. Code #067-007CLIA ID# 11D0255349
Accession Number:A1002190015
Patient: Sample Case
Comment:Reprinted: Fax:Telephone:
Date Collected:
Sex:Age: 29 Female
2/18/10
Report Date:Date Received: 2/19/10
(770) 446-4583(770) 441-22372/23/10
Reference Number:
Date of Birth: 09/10/1980
2/19/10
Metametrix
3425 Corporate WayDuluth, GA 30096
3425 Corporate WayDuluth, GA 30096
770.446.5483 Fax:770.441.2237
2105 Microbial Ecology Profile Methodology: DNA Analysis, GC/MS, Microscopic,Colorimetric, Automated Chemistry, ELISA
Pathogenic Bacteria95% Reference
Range
<=1.0E+005<0.01Helicobacter pylori<=1.0E+005H5.5E+008Campylobacter sp.<=1.0E+005<0.01Clostridium difficile<=1.0E+005H5.9E+008E.H.E. coli
Yeast/FungiNo clinically significant amounts. Yeast/Fungi
Yeast overgrowth has been linked to manychronic conditions, in part because of antigenic responses in some patients to even low rates ofyeast growth. Potential symptoms include diarrhea, headache, bloating, atopic dermatitis and fatigue. Positives are reported as +1, +2, +3 or +4 indicating >100, >1000, >10000 or >100000 pg DNA/g.
ParasitesPositive NegNecator americanus (hookworm)
ParasitesParasite infections are a major cause of
non-viral diarrhea. Symptoms may include constipation, gas, bloating, increased allergy response, colitis, nausea and distention.
Adiposity Index<= 8078Firmicutes>= 2022Bacteroidetes
The Adiposity Index is derived by using DNprobes that detect multiple genera of the phyla Firmicutes and Bacteroidetes. Abnormalities of these phyla may be associated with increased caloric extraction from food.
Drug Resistance GenesaacA, aphD Neg gyrB, ParE Neg
mecA Neg PBP1a, 2B NegvanA, B, and C Neg
These test results are not for the diagnosis of disease. They are intended to provide nutritional guidelines to qualified healthcare professionals with full knowledge of patient history and concerns to assist in their design of an appropriate healthcare program.
Page 2
Laboratory DirectorsJ. Alexander Bralley, PhD
Robert M. David, PhD
New York Clinical Lab PFI #4578Florida Clinical Lab Lic. #800008124
Georgia Lab Lic. Code #067-007CLIA ID# 11D0255349
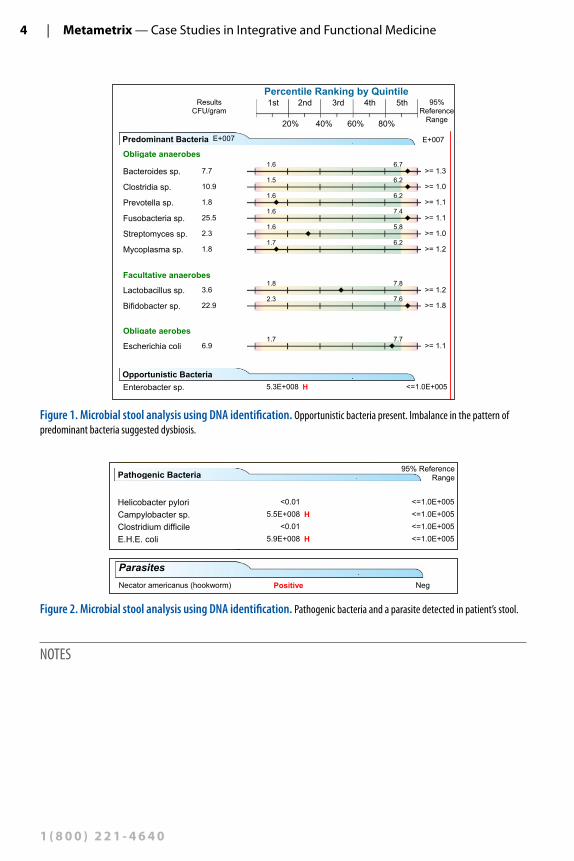
Figure 2. Microbial stool analysis using DNA identification. Pathogenic bacteria and a parasite detected in patient’s stool.
NOTES
29-Year-OldFeMalewIthUlCeratIveCOlItIS | 5
w w w. m e ta m e t r i x . c o m
Accession Number:A1002190015
Patient: Sample Case
Comment:Reprinted: Fax:Telephone:
Date Collected:
Sex:Age: 29 Female
2/18/10
Report Date:Date Received: 2/19/10
(770) 446-4583(770) 441-22372/23/10
Reference Number:
Date of Birth: 09/10/1980
2/19/10Metametrix
3425 Corporate WayDuluth, GA 30096
3425 Corporate WayDuluth, GA 30096
770.446.5483 Fax:770.441.2237
2150 Sensitivity - Bacteria Methodology: DNA Analysis, ELISA
PharmaceuticalsBacterial growth suppression is measured in a
liquid growth medium where fungal growth is suppressed and specific antibacterial agents are introduced before incubation. In contrast to the oldeisolation and culture techniques, such universal culturing more closely approximates the actions of antibacterials in the complex milieu of the colon.
Agents marked as "Sensitive" cause effectivebacterial growth suppression. Those antibacterial agents are candidates for suppressing the growth obacteria in the patient's colon. The results apply to all organisms reported under "Opportunistic Bacteria". Agents indicated as "Resistant" have low effectiveness. If all tested agents are resistant, synergistic mixtures of antibacterial agents may be effective.
Amoxicillin RAmpicillin RCefuroxime RCiprofloxacin SClindamycin SErythromycin RLevofloxacin SPenicillin RPotassium Clavula RSulfamethoxazole STetracyclin STrimethoprim-Sulfa S
Botanicals
For Botanical sensitivity testing the active ingredients are tested and an example of the available source is shown.
Sensitivities are not performed on "Pathogens" or "Parasites" because they do not grow in culture under normal laboratory conditions. Standard protocols are generally used for treatmentof pathogens and parasites.
5-Hydroxy-1,4-naphthoquinone SBlack Walnut
Alliin RGarlic
Arbutin RUva Ursi
Artemisinin RWormwood
Berberine SGoldenseal
Caprylic acid SOctanoic acid
Carvacrol SOregano
Oleuropein ROlive Leaf
Quinic Acid SCats Claw
Thymol SOil of Thyme
Undecylenic acid SUndecylenic acid
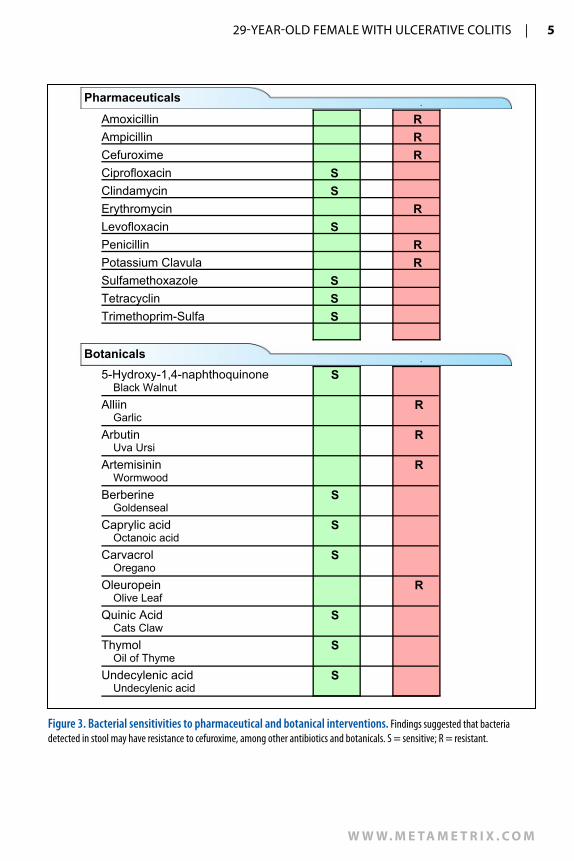
Figure 3. Bacterial sensitivities to pharmaceutical and botanical interventions. Findings suggested that bacteria detected in stool may have resistance to cefuroxime, among other antibiotics and botanicals. S = sensitive; R = resistant.

6 | metametrix —CaseStudiesinIntegrativeandFunctionalMedicine
1 ( 8 0 0 ) 2 2 1 - 4 6 4 0
Assessment♦ Pancolitiswithassociatedweightloss,fatigueanddiarrhea♦ Erythemanodosum♦ Dysbiosis♦ Antibioticresistance
Treatment Plan♦ Albendazole250mg:1tabPOBIDfor3days;
then1tabonday8,day30,andday90♦ Berberine(botanicalantimicrobialformula):1tabPOBID♦ Multi-botanicalantimicrobialformula:2capsPOBID(contains:bilberryextract
(25%anthocyanosides),noni,milkthistle,echinacea(purpurea&angustifolia),goldenseal,shiitake,whitewillow(bark),garlic,grapeseedextract,blackwalnut(hullandleaf ),raspberry,fumitory,gentian,teatreeoil,galbanumoil,lavenderoil(plantandflower),oreganooil(plantandflower)
♦ Deglycyrrhizinatedlicorice(DGL):2tabsPOTIDAC♦ Aloeveracapsules:2capsPOBID♦ Vegetablegreenspowder:1scoopPOQD♦ Probiotic1:Lactobacillus rhamnosusstrainGG♦ Probiotic2:Saccharomyces boulardii♦ Probioticcombination:Lactobacillus sp.,Bifidobacter sp.,andStreptococcus thermophilus♦ Digestiveenzymes:2tabsPOTIDAC♦ Continue:
x Diet:Eliminategluten,dairy,andyeastx Mesalamine(COX/PGblocker)400mg:1tabPOTID
NOTES
29-Year-OldFeMalewIthUlCeratIveCOlItIS | 7
w w w. m e ta m e t r i x . c o m
Treatment plan rationale:Itwasdecidedthatthepotentiallypathogenicparasitewouldbetreatedwithalbendazole,andthepathogenicandopportunisticbacteriawouldbead-dressedusingacombinationofantimicrobialbotanicalsthatwereidentifiedassensitiveonlaboratorytesting(Figure3).Botanicalswerechosenbecausethepatienthadanextensiveexposurehistorytoantibiotics.Botanicalsmaybelessdisruptivetothepredominantfloraforanumberofreasons.Forexample,someantimicrobialbotanicalscontainprebioticsubstancessuchaspolysaccharides.7Theyarealsosuggestedtobelesslikelytocontributetoantibioticresistance.8Themucilaginousbotanicalsaloeveraandlicorice(DGL)wereusedtoreduceGIinflammationandsupporthealingofthemucosa.9-10Avegetable-greenspowderwasemployedwiththeexpectationthatitwouldprovidebioavailablenutritionalsupport.Comprehensiveprobiotics,includingSaccharomyes boulardii,wereusedtonormal-izemicroflora,reduceinflammationandsupportintestinalhealth.11Digestiveenzymesweregiventooptimizemacronutrientbreakdowntofacilitateimprovedbioavailabilityandabsorptionofmicronutrients.Thedietaryrestrictionsandmesalaminewerecontinued.Notethatthisrelativelylow-riskprotocolwasdirectedataddressingthesuspectedcausalfactorsofEM’sIBDasidentifiedonlaboratoryanalysis,ratherthansuppressingthesymp-tomsandpathogenicmechanisms,asthehigher-riskmedicationsweredesignedtodo.
Ten-Month Follow-UpEMwasfeelingapproximately80%betterfromherinitialpresentation.Shehadgainedweightandtheerythemanodosumresolved.Herenergylevelwasmuchbetter.Shehadstoppedtheazathioprineandtitratedoffthesteroidsbythecompletionoftheantimicrobialregimen.Herdoseofmesalaminewasreducedthendiscontinued,althoughsheoccasionallyuseditforflare-ups.Theflare-upsweremostlycausedbyinadvertentexposuretofoodsshewasreactiveto.Theseexposurestofoodswouldthrowherofftrackforafewdays,butsherecoveredmorequicklythaninthepast.Shethoughtthatifshewassuccessfulinavoidanceofthesefoods,herrecoverywouldbe100%.ToEM,themostimportantbenefitofherhealingwasthatshecouldonceagainbeamothertohertwochildren.Asshedescribedit,shewasdoing“incrediblywell.”Formaintenancetreatment,itwasrecommendedthatEMcontinuewithdietaryrestrictions,probioticsanddigestiveenzymes;periodicclinicalandlaboratoryassessmentswoulddetermineneedforadditionalinterventions.
To EM, the greatest benefit of her healing was that she could once again be a mother to her two children.
8 | metametrix —CaseStudiesinIntegrativeandFunctionalMedicine
1 ( 8 0 0 ) 2 2 1 - 4 6 4 0
Ten-Month Follow-up Laboratory Results
Accession Number:A1002190016
Patient: Sample Case
Comment:Reprinted: Fax:Telephone:
Date Collected:
Sex:Age: 29 Female
2/18/10
Report Date:Date Received: 2/19/10
(770) 446-4583(770) 441-22372/23/10
Reference Number:
Date of Birth: 09/10/1980
2/19/10
Metametrix
3425 Corporate WayDuluth, GA 30096
3425 Corporate WayDuluth, GA 30096
770.446.5483 Fax:770.441.2237
2105 Microbial Ecology Profile Methodology: DNA Analysis, GC/MS, Microscopic,Colorimetric, Automated Chemistry, ELISA
80%60%40%20%
5th4th3rd2nd1stResultsCFU/gram
95%Reference
Range
Consistency = Formed/NormalPercentile Ranking by Quintile
Predominant Bacteria E+007E+007
Units and Reference RangesOrganisms are detected by DNA analysis.
One colony forming unit (CFU) is equivalent to one bacterium. Each genome detected represents one cell, or one CFU. Results are expressed in scientific notation, so an organism reported as 2.5 E7 CFU/gram is read as 25 million colony forming units per gram of feces. The cutoff for significance of Opportunistic Bacteria has been set at 1.0E+ 005 (100,000). These are levels above which clinically significant growth may be present. Rather than reporting semi-quantitative +1 to +4 levels, the new methodology provides full quantitative analysis.
Predominant Bacteria play major roles in health. They provide colonization resistance against potentially pathogenic organisms, aid in digestion and absorption, produce vitamins and SCFA's, and stimulate the GI immune system. DNA probes allow detection of multiple species (sp.) within a genus, so the genera that are reported cover many species.
Obligate anaerobes
Bacteroides sp. >= 1.3L1.16.71.6
Clostridia sp. >= 1.03.26.21.5
Prevotella sp. >= 1.12.46.21.6
Fusobacteria sp. >= 1.12.17.41.6
Streptomyces sp. >= 1.03.35.81.6
Mycoplasma sp. >= 1.23.26.21.7
Facultative anaerobes
Lactobacillus sp. >= 1.24.37.81.8
Bifidobacter sp. >= 1.86.77.62.3
Obligate aerobes
Escherichia coli >= 1.13.87.71.7
Opportunistic BacteriaNo clinically significant amounts.
Opportunistic Bacteria may cause symptoms and be associated with disease. They can affectdigestion and absorption, nutrient production, pH and immune state. Antibiotic sensitivity testswill be performed on all opportunistic bacteria found, although clinical history is usually considered to determine treatment since the organisms are not generally considered to be
Georgia Lab Lic. Code #067-007CLIA ID# 11D0255349
New York Clinical Lab PFI #4578Florida Clinical Lab Lic. #800008124
Laboratory DirectorsJ. Alexander Bralley, PhD
Robert M. David, PhDPage 1
Accession Number:A1002190016
Patient: Sample Case
Comment:Reprinted: Fax:Telephone:
Date Collected:
Sex:Age: 29 Female
2/18/10
Report Date:Date Received: 2/19/10
(770) 446-4583(770) 441-22372/23/10
Reference Number:
Date of Birth: 09/10/1980
2/19/10
Metametrix
3425 Corporate WayDuluth, GA 30096
3425 Corporate WayDuluth, GA 30096
770.446.5483 Fax:770.441.2237
2105 Microbial Ecology Profile Methodology: DNA Analysis, GC/MS, Microscopic,Colorimetric, Automated Chemistry, ELISA
Pathogenic Bacteria95% Reference
Range
<=1.0E+005<0.01Helicobacter pylori<=1.0E+005<0.01Campylobacter sp.<=1.0E+005<0.01Clostridium difficile<=1.0E+005<0.01E.H.E. coli
Yeast/FungiNegSaccharomyces sp. +1 => 100 pg DNA/g specimen
Yeast/FungiYeast overgrowth has been linked to many
chronic conditions, in part because of antigenic responses in some patients to even low rates ofyeast growth. Potential symptoms include diarrhea, headache, bloating, atopic dermatitis and fatigue. Positives are reported as +1, +2, +3 or +4 indicating >100, >1000, >10000 or >100000 pg DNA/g.
ParasitesPositive NegParasite present; taxonomy unavailable.
A taxonomy unavailable finding likely indicates an ingested protozoan and not a human parasite. It does not indicate treatment unless patient symptoms and other inflammatory markers are consistent with parasite infection.
ParasitesParasite infections are a major cause of
non-viral diarrhea. Symptoms may include constipation, gas, bloating, increased allergy response, colitis, nausea and distention.
Adiposity Index<= 8056Firmicutes>= 2044Bacteroidetes
The Adiposity Index is derived by using DNprobes that detect multiple genera of the phyla Firmicutes and Bacteroidetes. Abnormalities of these phyla may be associated with increased caloric extraction from food.
Drug Resistance GenesaacA, aphD Neg gyrB, ParE Neg
mecA Neg PBP1a, 2B NegvanA, B, and C Neg
These test results are not for the diagnosis of disease. They are intended to provide nutritional guidelines to qualified healthcare professionals with full knowledge of patient history and concerns to assist in their design of an appropriate healthcare program.
Page 2
Laboratory DirectorsJ. Alexander Bralley, PhD
Robert M. David, PhD
New York Clinical Lab PFI #4578Florida Clinical Lab Lic. #800008124
Georgia Lab Lic. Code #067-007CLIA ID# 11D0255349
Accession Number:A1002190016
Patient: Sample Case
Comment:Reprinted: Fax:Telephone:
Date Collected:
Sex:Age: 29 Female
2/18/10
Report Date:Date Received: 2/19/10
(770) 446-4583(770) 441-22372/23/10
Reference Number:
Date of Birth: 09/10/1980
2/19/10
Metametrix
3425 Corporate WayDuluth, GA 30096
3425 Corporate WayDuluth, GA 30096
770.446.5483 Fax:770.441.2237
2105 Microbial Ecology Profile Methodology: DNA Analysis, GC/MS, Microscopic,Colorimetric, Automated Chemistry, ELISA
Pathogenic Bacteria95% Reference
Range
<=1.0E+005<0.01Helicobacter pylori<=1.0E+005<0.01Campylobacter sp.<=1.0E+005<0.01Clostridium difficile<=1.0E+005<0.01E.H.E. coli
Yeast/FungiNegSaccharomyces sp. +1 => 100 pg DNA/g specimen
Yeast/FungiYeast overgrowth has been linked to many
chronic conditions, in part because of antigenic responses in some patients to even low rates ofyeast growth. Potential symptoms include diarrhea, headache, bloating, atopic dermatitis and fatigue. Positives are reported as +1, +2, +3 or +4 indicating >100, >1000, >10000 or >100000 pg DNA/g.
ParasitesPositive NegParasite present; taxonomy unavailable.
A taxonomy unavailable finding likely indicates an ingested protozoan and not a human parasite. It does not indicate treatment unless patient symptoms and other inflammatory markers are consistent with parasite infection.
ParasitesParasite infections are a major cause of
non-viral diarrhea. Symptoms may include constipation, gas, bloating, increased allergy response, colitis, nausea and distention.
Adiposity Index<= 8056Firmicutes>= 2044Bacteroidetes
The Adiposity Index is derived by using DNprobes that detect multiple genera of the phyla Firmicutes and Bacteroidetes. Abnormalities of these phyla may be associated with increased caloric extraction from food.
Drug Resistance GenesaacA, aphD Neg gyrB, ParE Neg
mecA Neg PBP1a, 2B NegvanA, B, and C Neg
These test results are not for the diagnosis of disease. They are intended to provide nutritional guidelines to qualified healthcare professionals with full knowledge of patient history and concerns to assist in their design of an appropriate healthcare program.
Page 2
Laboratory DirectorsJ. Alexander Bralley, PhD
Robert M. David, PhD
New York Clinical Lab PFI #4578Florida Clinical Lab Lic. #800008124
Georgia Lab Lic. Code #067-007CLIA ID# 11D0255349
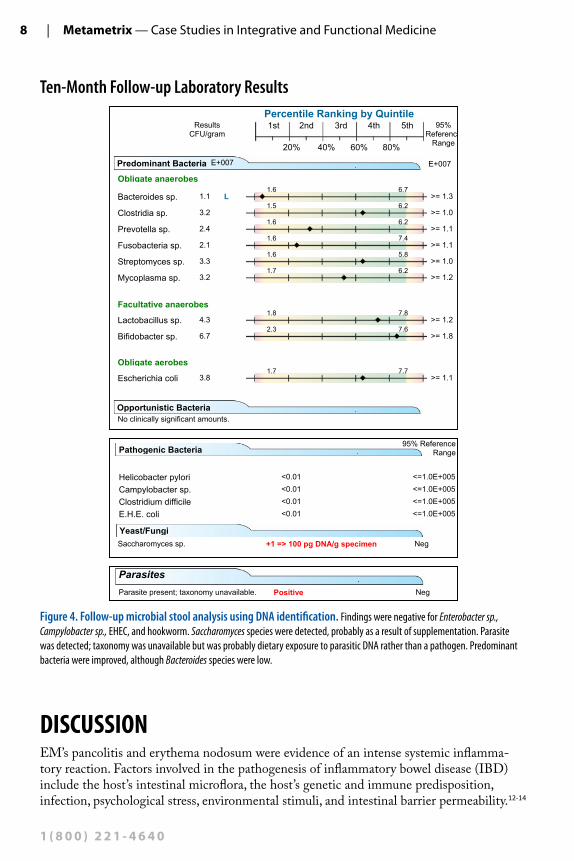
Figure 4. Follow-up microbial stool analysis using DNA identification. Findings were negative for Enterobacter sp., Campylobacter sp., EHEC, and hookworm. Saccharomyces species were detected, probably as a result of supplementation. Parasite was detected; taxonomy was unavailable but was probably dietary exposure to parasitic DNA rather than a pathogen. Predominant bacteria were improved, although Bacteroides species were low.
DISCUSSIONEM’spancolitisanderythemanodosumwereevidenceofanintensesystemicinflamma-toryreaction.Factorsinvolvedinthepathogenesisofinflammatoryboweldisease(IBD)includethehost’sintestinalmicroflora,thehost’sgeneticandimmunepredisposition,infection,psychologicalstress,environmentalstimuli,andintestinalbarrierpermeability.12-14

29-Year-OldFeMalewIthUlCeratIveCOlItIS | 9
w w w. m e ta m e t r i x . c o m
Immunologicalreactivitytofoods,includingglutenintolerance,havebeenreportedascausesofcolonicinflammationandIBD.4-5
Inthiscase,EMdidnothaveafamilyhistoryofIBD,butshewasunderagooddealofstresscausedbyherlimitedabilitytocareforherchildrenduetoherillness.Whilethisparticularstressorwasnotacausativefactor,itmayhaveexacerbatedherIBD.ComponentsoftheSADsheatemostofherlifewereveryantigenicforher,asidentifiedonIgG4testing.Theseverereactions,whilenotnumerousenoughtoindicateintestinalhyperpermeability,doreflectapronouncedinflam-matoryresponse.IgG4isanimmunoglobulinthatformsacomplexwiththeoffendingfoodprotein.Thisantigen-antibodycomplexmayinitiateanimmuneresponse,leadingtoawidevarietyofsymptoms,rangingfromgastroin-testinalsymptomsincludingdiarrhea,skinchanges,headachesorjointinflammationandmyopathy.Indeed,symptomsassociatedwithIgGreactionsarefoundassociatedwithmostorgansystems.15ItisinterestingtonotethatEMhadaseverereactiononIgG4testingtogluten,butwasnegativeforceliacdisease,suggestingthataninflammatoryresponsetofoodsinUCisnotlimitedtoasinglepathogenicmechanism.
Thispatient’slaboratoryresultspointedtoseveralfactorsthatmayhavecontributedtothepathogenesisofUC.AsshowninFigure1,veryhighlevelsofpredominantbacteriaspp.(Bacteroides sp., Clostridia sp., Fusobacteria sp., and Bifidobacter sp.)andEnterobacter sp.(anopportunisticbacterium)demonstratedsignificantlyalteredmicroflora(dysbiosis).Imbal-ancesofpredominantanaerobicbacteria(bothhighandlow)havebeenreportedinIBD.Specifically,Bacteroides, Eubacterium (suchasE. coli,Enterobacter, Shigella, Salmonella, Yer-sinia,etc.),andLactobacillushavebeenidentified.16SimilartoEM’sfindings,studieshavealsoshownincreasedanaerobes(especiallygram-negativeanaerobessuchasBacteroides)inCrohndisease(CD),UC,andpouchitis.Inonestudy,50%ofCDpatientshadeitherE. coliorBacteroidesasthepredominantGIbacterialgroup.17
Enterobacter spp, theopportunisticbacteriashowninFigure1, areasymptomaticinhealthyindividualsbutarealeadingcauseofnosocomialbacterialinfections,includingurinarytractinfections,bacteremia,skinandsofttissueinfections,andsepticarthritis.18However,therearenotmanycasesintheliteratureofEnterobacter-inducedcolitisorgastroenteritis.
Twopathogens,Campylobacter sp.andEnterohemorrhagic Escherichia coli (EHEC),werealsodetected(Figure2),illustratingtheseverityofdysbiosis.BacterialenteritiscaninduceorexacerbateIBD.13Campylobacter sp.andEHEChavebeenreportedascausesofbacterialcolitis.14,19-20
CampylobacterspecificallyhasbeendetectedinIBD,21andhasbeencitedasararecauseofpancolitis.19
ErythemanodosumisthemostcommondermatologicmanifestationofIBD,andUCspecificallyisknowntotriggerthiscondition,especiallywithflare-ups.22Further,itcanbecausedbybacterialorfungalinfection,andCampylobacter sp.hasbeenspecificallyimplicat-ed.22Erythemanodosumhasalsobeenassociatedwithceliacdisease.23Inthiscase,itmay
This patient’s laboratory results point to several factors that may have contributed to the etiopathogenesis of ulcerative colitis.
Campylobacter specifically has been detected in IBD, and has been cited as a rare cause of pancolitis.

10 | metametrix —CaseStudiesinIntegrativeandFunctionalMedicine
1 ( 8 0 0 ) 2 2 1 - 4 6 4 0
bethatthecombinationofimmunosuppressivesteroids,IBD,GICampylobacter, andglutensensitivityledtotheexpressionofthiscondition.
Hookworm,Necator americanus,wasdetected(Figure2).UChasbeenexacerbatedorevencausedbyhelminthinfections,specificallyStrongyloidesspecies.24-25However,“wormtherapy”usingthehelminthTrichuris suishasbeenreportedtosignificantlyimproveIBDsymptoms.26
GiventhedearthofevidenceconnectingEnterobacter sp.andNecator americanustopancoli-tis,itisnotclearthecontributiontheseplayedinEM’scondition,althoughtheymayhaveaddedtoheroverallinflammatoryburden.
Itisnoteworthythatthebacterialcultureandsensitivity(Figure3)showedresistancetocefuroxime,asecondgenerationcephalosporinantibiotic.Atthetimeofherfirstvisit,EMhadbeenontwomonthsofcephalexinwhichisafirst-generationcephalosporinantibiotic.Resistancetothisclassofantibioticscouldexplainwhyshehadhighpredominantbacteria,opportunisticbacteria,andpathogenicbacteriaevenaftertwomonthsofcephalexin.Be-causeofherhistoryofantibioticuse,thispatientwasacandidateforantimicrobialbotani-cals,towhichmicrobesmayhavemoredifficultydevelopingresistance.27
Basedonresearchfindings,Campylobacter sp.andEHECweremostlikelyinvolvedinthepathogenesisofEM’spancolitis.AsEM’sremarkableclinicalresponseandnormalized
follow-uplaboratoryresultsinFigure4demon-strated,sherespondedfavorablytotreatmentwithalbendazole,antimicrobialherbalformulas,digestiveenzymes,DGL,aloevera,vegetablegreenspowder,andavarietyofprobiotics.Thisrelativelylow-riskprotocoladdressedthesuspectedcausalfactorsofIBD,ratherthaninhibitingsymptomsandpatho-genicmechanismsasherhigh-riskmedicationwas
designedtodo.Consistentwithpublishedresearch,theaggressiveprotocolofprobioticsappearstohavebeenquitetherapeuticinEM’scase.16-17,28CertainspeciesofLactobacillusand Bifidobacteria havebeenshowntoattenuatecolitisinanimalmodels.28TreatmentswithLactobacillus sp.,Bifidobacteria sp.,andSaccharomyces boulardiihavebeenshowntobringaboutremissioninUC.16
ThepresenceoftaxonomicallyunidentifiedparasiticDNA(Figure4)wasconsideredtobeclinicallyirrelevant,asevidencedbyhersignificantimprovement.ItissuggestedthatifthemajorpathogenicparasitesinhumanshavebeentestedforusingPCRtechnologyandruledout,thefindingofparasiticDNAislikelyfromatransient,food-basedexposureandnotindicativeofparasiticinfection.TheSaccharomycesspeciesdetectedonfollow-upwasmostlikelyfromsupplementationofSaccharmycesboulardii.WhilethepredominantBacte-roides sp.werelowaftertreatment,itmayhaveactuallybeenadesirablefinding.IthasbeenshownthatBacteroides vulgatuscausesinflammationandthatincreasedBacteroides fragilismaybeinvolvedwithCD.16ThefactthatBacteroides sp.werehighwhenshewassymptom-aticandwereloweraftertreatmentthatresultedinclinicalimprovementsuggeststhattheBacteroidesinherstoolincludedB. vulgatusorB. fragilis.
In this case, it may be that the combination of immunosuppressive steroids, IBD, GI Campylobacter, and gluten sensitivity led to the expression of erythema nodosum.
29-Year-OldFeMalewIthUlCeratIveCOlItIS | 11
w w w. m e ta m e t r i x . c o m
AcomprehensiveprotocoldesignedtoremoveGImicrobialimbalancesandantigenicfoods,replacedigestiveenzymesandnutrients,repairtheintestinallining,andreinoculatewithbeneficialmicrofloraresultedinan80%improvementfromtheinitialpresenta-tion.Thepatientexperiencedasignificantimprovementorresolutionofallofhermajorsymptoms,includingdiarrhea,erythemanodosum,fatigueandweightloss,andwasabletostopregularuseofallmedications.Sheobservedthatitwaslikelythathiddenexposurestoantigenicfoodsresultedintheperiodicflare-upsthatkeptherfromafull,100%recovery.
ItisinterestingtonotethattheremovalofantigenicfoodsfromEM’sdietappearstohaveclearlycontributedtoherimprovement,asevidencedbythefactthataccidentalingestionofthosesubstancestriggeredsymptomaticflare-ups.However,itwasonlyafternormalizationofbowelmicrobialstatusthattheeffectofantigenicfoodswasexperienced.ThissuggeststhattheGImicrobialimbalancesinEMwerethesignificantunderlyingetiologicalfactors.
CONCLUSIONPancolitisthatisnon-responsivetomedicationsfrequentlyrequiressurgicalintervention(colectomy),resultinginsignificantquality-of-lifeissues.3Becausethispatient’sconditioncouldnotbemedicallymanagedusingthehigh-risk,immunosuppressivecombinationofprednisone,mesalamineandazathioprine,colectomywouldmostprobablyhavebeenhernextstep.
LaboratorytestingidentifiedIgG4foodreactionsandseveregastrointestinalmicrobialimbalances,includingdisruptionofthepredominantflora,thepresenceofopportunisticandpathogenicbacteriaandaparasite.Thelow-riskandnon-invasiveprotocolemployedwasdesignedtoaddressunderlyingcausesofthepatient’sIBD,andindoingso,dramaticallyreducedGIinflamma-tionandmayhavepreventedtheneedforsurgicalintervention.
ThefactthatthisUCcaseshowedsuchdramaticimprovementsoncethemicrobiotawerenormalizedstronglysuggeststhatthisapproachmighthavegreatbenefitforanyinflammatorybowelcase,particularlyinlightofthenumerousreportsintheliteraturethatsignificantmicrobialimbalancesareassociatedwiththeetiopathogenesisofinflammatoryboweldiseases.GiventheepidemiologicalstatisticsofIBD,researchinvestigatingtheefficacyofthiscost-saving,safe,multifactorialandintegrativeapproachishighlyrecommended.
references1. Hanauer SB. Inflammatory bowel disease: epidemiology, pathogenesis, and therapeutic opportunities.
Inflammatory bowel diseases. Jan2006;12Suppl1:S3-9.2. O’Connor PM, Lapointe TK, Beck PL, Buret AG. Mechanisms by which inflammation may increase
intestinalcancerriskininflammatoryboweldisease.Inflamm Bowel Dis. Feb122010.3. Cuffari C, Present DH, BaylessTM, Lichtenstein GR. Optimizing therapy in patients with pancolitis.
Inflammatory bowel diseases. Oct2005;11(10):937-946.
The fact that this UC case showed such dramatic improvements once the microbiota were normalized, strongly suggests that this approach may have benefit for any IBD case.
12 | metametrix —CaseStudiesinIntegrativeandFunctionalMedicine
1 ( 8 0 0 ) 2 2 1 - 4 6 4 0
4. YangA,ChenY,ScherlE,NeugutAI,BhagatG,GreenPH.Inflammatoryboweldiseaseinpatientswithceliacdisease.Inflamm Bowel Dis. Jun2005;11(6):528-532.
5. MacDermottRP.Treatmentofirritablebowelsyndromeinoutpatientswithinflammatoryboweldiseaseusingafoodandbeverageintolerance,foodandbeverageavoidancediet.Inflamm Bowel Dis. Jan2007;13(1):91-96.
6. MarteauP.Bacterialfloraininflammatoryboweldisease.Dig Dis. 2009;27Suppl1:99-103.7. GuoFC,WilliamsBA,KwakkelRP,etal.Effectsofmushroomandherbpolysaccharides,asalternativesfor
anantibiotic,onthececalmicrobialecosysteminbroilerchickens.Poult Sci. Feb2004;83(2):175-182.8. Abascal K YE. Herbs and Drug Resistance: Part 1—Herbs and Microbial Resistance to Antibiotics.
Alternative and Complementary Therapies. August200220028(4):237-241.9. DavisRH,DonatoJJ,HartmanGM,HaasRC.Anti-inflammatoryandwoundhealingactivityofagrowth
substanceinAloevera.J Am Podiatr Med Assoc. Feb1994;84(2):77-81.10. StewartPM,PrescottSM.Canlicoricelickcoloncancer?J Clin Invest. Apr2009;119(4):760-763.11. MengheriE.Health,probiotics,andinflammation.J Clin Gastroenterol. Sep2008;42Suppl3Pt2:S177-178.12. GoodhandJR,WahedM,RamptonDS.Managementofstressininflammatoryboweldisease:atherapeutic
option?Expert review of gastroenterology & hepatology. Dec2009;3(6):661-679.13. KalischukLD,BuretAG.AroleforCampylobacterjejuni-inducedenteritisininflammatoryboweldisease?
American journal of physiology. Oct292009.14. Singh J. Colitis. emedicine from WebMD 2009; http://emedicine.medscape.com/article/927845-overview.
Accessed12/31/09,2009.15. LordRSBJ.LaboratoryEvaluationsforIntegrativeandFunctionalMedicine.Atlanta:MetametrixInstitute;
2008:435-437.16. OttSJ,MusfeldtM,WenderothDF,etal.Reductionindiversityofthecolonicmucosaassociatedbacterial
microflorainpatientswithactiveinflammatoryboweldisease.Gut. May2004;53(5):685-693.17. Tamboli CP, Neut C, Desreumaux P, Colombel JF. Dysbiosis in inflammatory bowel disease. Gut. Jan
2004;53(1):1-4.18. FraserSL,ArnettM.Enterobacterinfections.emedicine from WebMD2009;http://emedicine.medscape.com/
article/216845-overview.Accessed1/05/2010,2010.19. SiegalD,SyedF,HamidN,CunhaBA.Campylobacter jejunipancolitismimicking idiopathiculcerative
colitis.Heart Lung. Jul-Aug2005;34(4):288-290.20. SumrallA,McMullanL,AbrasleyC,EastH.Acaseofseverehemorrhagicdiarrhea.Journal of the Mississippi
State Medical Association. Dec2007;48(12):366-369.21. GradelKO,NielsenHL,SchonheyderHC,EjlertsenT,KristensenB,NielsenH.Increasedshort-andlong-
termriskofinflammatoryboweldiseaseaftersalmonellaorcampylobactergastroenteritis.Gastroenterology. Aug2009;137(2):495-501.
22. Hebel JL, HabifT. Erythema Nodosum. emedicine from WebMD 2009; http://emedicine.medscape.com/article/1081633-overview.Accessed12/31/09,2009.
23. BartyikK,VarkonyiA,KirschnerA,EndreffyE,TuriS,KargE.Erythemanodosuminassociationwithceliacdisease.Pediatric dermatology. May-Jun2004;21(3):227-230.
24. GhoshalUC,AlexenderG,GhoshalU,TripathiS,KrishnaniN.Strongyloidesstercoralis infestationinapatientwithsevereulcerativecolitis.Indian journal of medical sciences. Mar2006;60(3):106-110.
25. WeightSC,BarrieWW.ColonicStrongyloidesstercoralisinfectionmasqueradingasulcerativecolitis.Journal of the Royal College of Surgeons of Edinburgh. Jun1997;42(3):202-203.
26. Summers RW, Elliott DE, Urban JF, Jr.,Thompson RA,Weinstock JV.Trichuris suis therapy for activeulcerativecolitis:arandomizedcontrolledtrial.Gastroenterology. Apr2005;128(4):825-832.
27. SibandaT,OkohA.Thechallengesofovercomingantibioticresistance:plantextractsaspotentialsourcesofantimicrobialandresistancemodifyingagents.African J of Biotechnology. December2007;6(25):2886-2896.
28. SheilB,ShanahanF,O’MahonyL.Probioticeffectsoninflammatoryboweldisease.J Nutr. Mar2007;137(3Suppl2):819S-824S.


















