08 Principles Indications and Limits

of 8
-
Upload
maytorenacger -
Category
Documents
-
view
212 -
download
0
Transcript of 08 Principles Indications and Limits
-
7/29/2019 08 Principles Indications and Limits
1/8
7Principles for Breast Reconstruction:Indications and LimitsJennifer L. Marti and Virgilio Sacchini
7.1 Introduction
Breast cancer occurs in one of eight American women.
Although many patients are candidates for breast-conser-
vation therapy, the rates of mastectomy and of contralateral
risk-reducing mastectomy have risen in recent years in theUSA [1]. The vast majority of patients undergoing mas-
tectomy are candidates for breast reconstruction. Accord-
ingly, the number of breast reconstruction operations has
also increased [2].
Extensive literature clearly supports the advantages and
oncologic safety of reconstruction after mastectomy.
Reconstruction after mastectomy has been shown to be
effective in restoring body image, improving quality of life,
and reducing the psychological distress of mastectomy [3,
4]. At the same time, immediate reconstruction has been
found to be oncologically safe after mastectomy, even in
cases of advanced breast cancer [57]. This has been con-
clusively demonstrated in multiple studies, including a
meta-analysis by Gieni et al. [8], which confirmed no
increased risk of local recurrence with immediate breast
reconstruction after mastectomy. However, despite its
advantages and oncologic safety, fewer than 25 % of
American patients undergo immediate or delayed recon-
struction after mastectomy [9].
Options for reconstruction include reconstruction with
autologous tissue, or with a tissue expander and implant. For
unilateral reconstruction, symmetry is more easily obtained
with a tissue flap than with an implant [2]. Autologous flap
options include latissimus dorsi myocutaneous flaps,
transverse rectus abdominus myocutaneous (TRAM) flaps,
deep inferior epigastric perforator flaps, and gluteal artery
perforator flaps [3]. Implants contain either saline or silicone.
An immediate one-stage reconstruction with an implant may
be feasible; however, most patients undergo a staged proce-
dure with a tissue expander to allow for interval expansion,followed by an exchange to a permanent implant.
Autologous reconstruction may be difficult or compli-
cated in patients who have undergone prior surgery at
potential donor sites, or who have medical comorbidities
such as hypertension, diabetes, and chronic obstructive
pulmonary disease, who are smokers, or who are at the
extremes of body mass index [3].
7.2 Immediate Versus DelayedReconstruction
Most patients undergoing mastectomy are candidates for
immediate reconstruction. Immediate reconstruction offers
multiple advantages, including one-stage surgery, better
cosmetic outcome, and improved psychological state. In the
only randomized controlled trial to date comparing imme-
diate and delayed breast reconstruction, Dean et al. [10]
reported increased psychological well-being with immedi-
ate reconstruction [3]. Immediate reconstruction often
achieves a better aesthetic result than delayed reconstruc-
tion, owing to preservation of the skin envelope and infra-
mammary fold [11]. For patients who undergo delayed
reconstruction, use of an autologous flap is preferable to useof an implant, as the process of tissue expansion required
for an implant is difficult owing to skin stiffness, resulting in
a suboptimal cosmetic result [2]. A combination of a tissue
expander and an implant with a latissimus dorsi flap is
another option for breast reconstruction.
J. L. Marti
Department of Surgery, Beth Israel Medical Center,
New York, USA
e-mail: [email protected]
V. Sacchini (&)
Breast Service, Department of Surgery, Memorial Sloan-
Kettering Cancer Center, New York, USA
e-mail: [email protected]
C. Urban and M. Rietjens (eds.), Oncoplastic and Reconstructive Breast Surgery,DOI: 10.1007/978-88-470-2652-0_7, Springer-Verlag Italia 2013
77
-
7/29/2019 08 Principles Indications and Limits
2/8
7.2.1 Breast Reconstruction Considerationswith Anticipated PostmastectomyRadiotherapy
Immediate reconstruction in patients who will undergoanticipated postmastectomy radiotherapy (PMRT) is con-
troversial. The two main issues that raise concern are
compromised delivery of radiotherapy in the face of a
reconstructed breast, and the impact of radiotherapy on the
long-term cosmetic result of the reconstruction [12].
7.2.2 Oncologic Safety of Reconstruction Priorto PMRT
Historically, delayed reconstruction has been recommended
when PMRT is planned. Some still advocate this approach,
owing to concerns of compromised delivery of radiotherapy
in the presence of a reconstructed breast, whether a tissue
flap or an implant [1216]. Concerns include compromised
delivery to the internal mammary lymph nodes, nonuniform
radiotherapy delivery, underdosing of the chest wall, and
increased radiotherapy dose to normal tissues with a breast
reconstruction in place [12]. The evidence is conflicting. On
the one hand, Motwani et al. [15] reported compromised
delivery of radiotherapy in 52 % of patients who had
undergone immediate reconstruction, compared with 7 % of
controls. However, Koutcher et al. [17] found no compro-
mised delivery of radiotherapy to the chest wall in most
patients, with an excellent 30-month actuarial locoregional
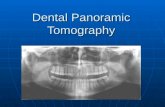
control rate of 97 %.Owing to concerns of compromised radiotherapy deliv-
ery attributable to the reconstructed breast, a delayed
immediate reconstruction algorithm is advocated at the
MD Anderson Cancer Center for patients who will receive
PMRT [2]. With this approach, a tissue expander is placed
at the time of mastectomy, and is deflated during adjuvant
radiotherapy (protocol outlined in Fig. 7.1). Tissue expan-
sion is performed after the completion of radiotherapy, and
reconstruction with an autologous flap is performed
46 months thereafter [18]. In this series, the approach
resulted in low complication rates, with tissue expander loss
in 14 % of patients. The recurrence rate at 32 months of
follow-up was low, at 3 % [18]. The complication rate with
a delayedimmediate approach with subsequent flap
reconstruction may be lower than that for a standard
delayed flap reconstruction (26 % vs. 38 %, p = 0.40) [18].
Despite the concerns about radiation delivery that
prompted development of the delayedimmediate
approach, many authors have reported acceptable recur-
rence rates and cosmetic outcomes with immediate recon-
struction followed by PMRT [17]. In one retrospective
Fig. 7.1 MD Anderson CancerCenter delayedimmediate breast
reconstruction protocol. LD
latissimus dorsi flap, PMRT
postmastectomy radiation
therapy, SGAP superior gluteal
artery perforator flap, TRAM
transverse rectus abdominus
myocutaneous flap. (Reprinted
with permission from Kronowitz
et al. [62])
78 J. L. Marti and V. Sacchini
-
7/29/2019 08 Principles Indications and Limits
3/8
review of 191 patients requiring PMRT who underwent
TRAM flap reconstruction in either an immediate or a
delayed fashion, the risk of locoregional recurrence was not
significantly increased in the group undergoing immediate
reconstruction (3.7 % vs. 1.8 %, p = 0.65) at 40 months of
follow-up [19]. Similarly, Wright et al. [20] retrospectively
reviewed 104 patients who underwent exchange for a per-
manent implant prior to PMRT. Local control rates wereexcellent, 0 % at 5 years, and immediate reconstruction was
not associated with an elevated risk of distant metastases or
death.
In contrast to these data, others have reported higher
rates of locoregional recurrence among patients undergoing
immediate reconstruction. Nahabedian et al. [21] retro-
spectively analyzed 146 patients who underwent immediate
or delayed reconstruction after PMRT. Locoregional
recurrence rates were higher in patients who underwent
immediate versus delayed reconstruction (27 % vs. 15 %,
p = 0.04). These data should be interpreted with caution
because of the higher than expected rates of recurrence [21,
22]. As a result of these conflicting data, the safety of
immediate reconstruction prior to PMRT remains
controversial.
7.2.3 Effects of Radiotherapy on the CosmeticOutcome of the Reconstructed Breast
In addition to conflicting data about oncologic safety, there
is also debate about the impact of reconstruction prior to
PMRT on cosmetic outcomes. The main complications
caused by radiation on the reconstructed breast include fat
necrosis, impaired wound healing, contracture, fibrosis,
volume loss, and architectural distortion [23]. There are
data to support superior cosmetic results with delayed
reconstruction compared with immediate reconstruction.
Javaid et al. [23] in a systematic review of ten published
reports of patients undergoing immediate and delayed
reconstruction and PMRT found a higher incidence of
breast fibrosis and contracture with immediate reconstruc-
tion. Similarly, Kronowitz et al. [16], in a systematic review
of 49 articles, reported high rates of contracture and implant
loss among patients undergoing immediate reconstruction
prior to PMRT.
Other groups have also reported lower rates of compli-
cations after delayed reconstruction. Adesiyun et al. [24], in
a review of 113 patients who underwent immediate or
delayed breast reconstruction with PMRT, reported a lower
rate of complications in the delayed-reconstruction group
(32 % vs. 44 %, p = 0.18), although this difference was not
statistically significant. The patients general satisfaction
with their cosmetic outcome was similar in the two groups
(68 %) [24]. Another group found no significant difference
in complication rates with immediate or delayed recon-
struction with TRAM flaps in patients who received PMRT,
but the authors ultimately recommended delayed recon-
struction because of possible low power of the study [25].
Compared with the aforementioned studies, other groups
have reported acceptable cosmetic results and complication
rates with immediate reconstruction. A meta-analysis of 11
studies by Barry et al. [26] concluded that postoperativeoutcomes did not differ depending on whether reconstruc-
tion was performed before or after PMRT. Autologous flaps
appeared to have superior outcomes. Postoperative com-
plications such as fibrosis, contracture, infection, fat
necrosis, and reoperation were lower with autologous flap
reconstruction than with implant reconstruction [26]. Thus,
if immediate reconstruction is pursued, many authors
advocate reconstruction with an autologous flap over a tis-
sue expander/implant to enhance cosmetic results [6].
Although many authors have reported superior outcomes
with flap reconstruction compared with implant recon-
struction prior to PMRT, this does not necessarily imply
that successful outcomes cannot be achieved with implant
reconstruction. For example, Cordeiro et al. [27, 28]
reported satisfactory aesthetic results with immediate tissue
expander placement, followed by exchange for a permanent
implant prior to radiotherapy. Aesthetic results were cate-
gorized as good to excellent in 80 % of patients, with an
implant loss rate of 11 % [27].
7.2.4 Inflammatory Breast Cancer
In patients with inflammatory breast carcinoma, delayed
reconstruction is recommended because of extensive skin
involvement and a high risk of local recurrence [29]. The
required resection of skin precludes a skin-sparing mas-
tectomy. Furthermore, timely administration of radiother-
apy is imperative, making the delay for healing after
reconstruction undesirable. Therefore, reconstruction
should be delayed in patients undergoing mastectomy for
inflammatory breast cancer. This recommendation is
reflected in the 2012 National Cancer Comprehensive
Network guidelines [30].
There are two small series that have reported success
with immediate reconstruction. Chin et al. [31] performed a
retrospective analysis of 23 patients with inflammatory
breast cancer who underwent immediate or delayed recon-
struction. They reported similar rates of locoregional
recurrence (29 % vs. 33 %, p not significant), suggesting no
compromised oncologic outcome with immediate recon-
struction. Another small series found no overall survival
difference in patients who underwent immediate recon-
struction, although six of ten patients did develop local
recurrence [32]. Importantly, these small studies do not
7 Principles for Breast Reconstruction: Indications and Limits 79
-
7/29/2019 08 Principles Indications and Limits
4/8
offer sufficient statistical power to conclusively demonstrate
the safety of immediate breast reconstruction for patients
with inflammatory breast cancer.
In conclusion, for patients who will likely require
PMRT, immediate reconstruction remains controversial,
owing to concerns of compromised radiotherapy delivery
and impaired cosmetic outcome of the reconstructed breast.
However, many authors have reported acceptable cosmeticoutcomes and comparable rates of locoregional recurrence
with immediate reconstruction. Immediate reconstruction is
not recommended in patients with inflammatory breast
cancer.
7.2.4.1 Nipple-Sparing Mastectomy
After a traditional skin-sparing mastectomy, patients may
subsequently undergo nipple reconstruction. This requires
an additional surgical procedure and tattooing, and ulti-
mately, many patients may never pursue this. Furthermore,
results may be disappointing. Jabor et al. [33] reported a
14 % rate of patient dissatisfaction after nippleareola
complex (NAC) reconstruction owing to loss of nipple
projection and the overall appearance and texture of the
reconstructed NAC. Therefore, preservation of the NAC
with a nipple-sparing mastectomy (NSM) may be desirable
in some patients.
Subcutaneous mastectomy with NAC preservation and
breast reconstruction was first described by Freeman [34] in
1962. Preservation of the NAC may enhance cosmetic
outcome and offer psychological benefit, as the NAC plays
an important role in the identification of a womans body
image [35]. Indeed, Boneti et al. [36] reported higher
patient cosmetic satisfaction in patients who had undergone
NSM as compared with skin-sparing mastectomy. There is
theoretical concern about the oncologic safety of this pro-
cedure owing to an inability to resect all of the retroareolar
ductal tissue.
7.2.5 Candidates for NSM
When selecting a candidate for NSM, one must consider the
risk of cancer involvement of the NAC, and the size and
degree of ptosis of the breast [37]. Candidates for NSM
include patients undergoing risk-reducing mastectomy.
Patients may pursue risk-reducing mastectomy because of
high-risk factors such as a strong family history, the pres-
ence or history of a contralateral breast tumor, lobular
carcinoma in situ, or previous radiation for Hodgkin lym-
phoma [38]. Selected patients with ductal carcinoma in situ
(DCIS) or invasive breast cancer may also be candidates for
NSM [38]. In appropriately selected patients, only 12 %
will have tumor involvement at the NAC, precluding
preservation [39, 40].
The factors associated with nipple involvement include
tumors larger than 24 cm, a tumornipple distance of less
than 2 cm, breast tumors overlapping more than one
quadrant, grade 3 or undifferentiated cancers, stage III
disease, human epidermal growth factor receptor 2 (HER2)/
neu positivity, and an extensive intraductal component of
greater than 25 % [4143].
For patients with invasive cancer, small tumors located
in the periphery of the breast have the lowest risk of NAC
involvement. The lowest risk of NAC involvement occurs
in tumors smaller than 2 cm, located at least 2.5 cm from
the NAC [44]. Tumors located within 2 cm of the NAC, or
larger than 4 cm, were found in one report to have occult
tumor present at the nipple in 50 % of cases [44]. A path-
ologic analysis of 140 mastectomy specimens reported a
16 % rate of NAC involvement with cancer. In all cases, the
primary tumor was located within 2.5 cm of the NAC [45].
Many series of carefully selected patients have reported
low rates of NAC involvement, ranging from 6 to 10 % [37,
38, 4649]. In one series of patients with peripheral tumors
and clinically node-negative disease, a low rate (less than
2 %) of NAC involvement was reported [48]. Therefore, the
risk of NAC involvement is lower in patients with low-
grade, unicentric, small, peripheral tumors, with clinically
uninvolved axillary lymph nodes, who have not undergone
neoadjuvant chemotherapy [39, 48, 50, 51]. Patients who
will likely undergo radiotherapy are not ideal candidates, as
they have advanced disease that portends a higher proba-
bility of NAC involvement. Furthermore, radiotherapy may
result in distortion and asymmetric displacement of the
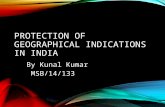
NAC. A proposed algorithm for patient selection is illus-
trated in Fig. 7.2.
Fig. 7.2 Patient selectioncriteria for nipple-sparing
mastectomy. CA cancer, NAC
nippleareola complex.
(Reproduced with permission
from Spear et al. [50])
80 J. L. Marti and V. Sacchini
-
7/29/2019 08 Principles Indications and Limits
5/8
7.2.6 Intraoperative Assessment of NAC TumorInvolvement
Identification of NAC tumor involvement precludes NAC
preservation. Intraoperative pathologic assessment with
frozen section of the retroareolar ducts can be useful to
identify the presence of NAC tumor involvement at the
initial surgery [39, 42, 52]. Dissection of the retroaerolarducts should be done sharply, as cautery can cause thermal
damage to the NAC [52]. Coring of the nipple ducts may be
facilitated by everting the nipple [52].
Frozen-section analysis is 91 % sensitive and 99 %
specific for assessing tumor involvement of the NAC [53].
Reported rates of positive frozen section range from 2.5 to
12 % in well-selected patients [36, 39, 54, 55]. With careful
patient selection and the use of preoperative MRI, Wi-
jayanayagam et al. [56] reported a low rate of NAC
involvement of 3 %. NAC tumor involvement may not be
identified until final surgical pathologic analysis, necessi-
tating NAC resection at a second surgery. When the NAC is
involved with tumor, the histologic finding is usually DCIS,
although atypical ductal hyperplasia and invasive breast
carcinoma may also be identified [39, 43, 54, 57].
7.2.7 Rates of Recurrence After NSM
Multiple series with less than 3 years of follow-up have
reported recurrence rates of 5 % or less after NSM, com-
parable to rates of recurrence after skin-sparing mastectomy
[36, 40, 55, 58]. Voltura et al. [55] reported a 5 % recur-
rence rate at 24 months in patients with aggressive triple-
negative tumors. Sacchini et al. [58] reported recurrences in
only two of 123 patients undergoing NSM, with a median
follow-up of 25 months. Recurrences did not occur at the
NAC [58]. Breast cancer occurred in two patients who
underwent risk-reducing mastectomies, located in periphe-
ral locations [58]. In another series of 96 patients who
underwent NSM with a median follow-up of 34 months,
only one patient developed a locoregional recurrence, and
two patients developed distant metastases [40].
The reported recurrence rates of longer-term studies,
with follow-up of at least 3 years, range from 5 to 28 % [39,
42, 59, 60]. In a review of 112 patients who underwent
NSM and had tumors located at least 2 cm from the nipple,
5 % of patients has recurrence at a mean follow-up of
59 months [42]. Recurrences occurred in the chest wall,
upper breast, and inframammary fold, with only one
recurrence in the NAC [42]. The location of these recur-
rences highlights the importance of considering the poten-
tial for elevated risk at the periphery of the breast after
NSM, as access to the peripheral breast may be more dif-
ficult if a small periareolar incision is used.
Studies with long-term follow-up of patients who
undergo NSM are limited, and have not definitively dem-
onstrated the long-term oncologic safety of NSM. In a series
with a follow-up of 5.5 years, Caruso et al. [59] reported a
recurrence rate of 12 % in 50 patients. Recurrences occur-
red at the NAC in one patient, and distant metastases
developed in four patients. In a prospective trial with a
median follow-up of 13 years, Benediktsson and Perbeck[53] reported a high overall locoregional recurrence rate of
28 %. This may suggest that NSM is not oncologically safe
in the long term, but this high rate may have been due to
patient selection. Patients at high risk of recurrence were
included, with tumors larger than 3 cm or multicentric
disease [53]. Patients in this study who received PMRT had
a local recurrence rate of 8.5 %, similar to reported rates
after skin-sparing mastectomy [53].
Petit et al. [60] recently published an update of their
experience with 934 patients who underwent NSM with a
median follow-up of 50 months. These investigators rou-
tinely treat the NAC intraoperatively with electron intra-
operative treatment if the frozen section is negative, and
preserve the NAC even if final pathologic investigation
reveals tumor involvement [60]. For patients with invasive
ductal cancer, 3.6 % had recurrence in the breast at 5 years,
and 0.8 % had recurrence at the NAC [60]. Of the patients
who had recurrence at the NAC, most had an extensive
intraductal component and had HER2/neu positivity [60].
For patients with DCIS, the rate of locoregional recurrence
at 5 years was high: 8 % [60]. The rate of recurrence was
4.9 % in the breast and 2.9 % at the NAC [60]. These high
recurrence rates may cause one to pause before offering this
procedure to patients with DCIS. Predictors of breast
recurrence among patients with DCIS included age under
40 years, positive retroareolar margins, estrogen receptor
negativity, progesterone receptor negativity, high-grade
histologic findings, HER2/neu positivity, and Ki-67 index
greater than 20 % [60].
In conclusion, several studies support the short-term
oncologic safety of NSM, with locoregional recurrence
rates similar to those of skin-sparing mastectomy, and rare
recurrences occurring at the NAC. However, the long-term
oncologic safety of this procedure has not been determined,
and the recent data of Petit et al. [60] may be a reason for
caution in patients with DCIS. More studies with longer-
term follow-up are needed, as the literature to date is not yet
definitive on the oncologic safety of NSM in the long term.
7.2.8 NSM in BRCA Mutation Carriers
The oncologic safety of NSM in BRCA mutation carriers is
controversial, as breast tissue connects with the nipple and
cannot be completely resected with NAC preservation [61].
7 Principles for Breast Reconstruction: Indications and Limits 81
-
7/29/2019 08 Principles Indications and Limits
6/8
One pathologic analysis of mastectomy specimens of
BRCA patients revealed that terminal ductal lobular units
were present in 24 % of the NACs and 8 % of nipples [61].
The long-term potential of this retained tissue developing a
cancer is unknown [61]. In this study, occult NAC tumor
involvement was 0 % in risk-reducing specimens, and 10 %
in therapeutic specimens. These rates are similar to those
for non-BRCA mutation carriers [61]. Long-term studiesare needed before we can say with absolute certainty that
NSM is an oncologically sound procedure in BRCA
patients.
7.2.8.1 Postoperative Outcomes of the NAC
Patients should be counseled that the NAC preservation in
NSM is mainly of cosmetic, not functional benefit. Most
patients will not experience sustained preservation of nipple
sensation or erectile ability [39]. There is a risk of
approximately 12 % of occult tumor involvement at the
NAC, requiring resection [39, 40]. Furthermore, there is a
risk of partial or complete necrosis of the NAC in approx-
imately 411 % of patients [38, 39, 42, 54, 58]. Preserva-
tion of the blood supply to the NAC may be maximized by
use of a lateral incision, without a circumareolar extension.
Also, the NAC may ultimately settle in a displaced or
asymmetric position, with lateral displacement occurring in
67 % of cases in one series [54].
Numerous studies have demonstrated the short-term
oncologic safety of NSM in risk reduction, and in patients
with early-stage breast cancer. Larger studies with longer
follow-up are needed to definitely demonstrate that NSM
has locoregional recurrence rates comparable to those of
skin-sparing mastectomy. Ideal candidates for NSM should
have small tumors (less than 3 cm), located at least 2 cm
from the nipple, with clinically uninvolved axillary lymph
nodes, and without skin involvement [50]. Patients with
extensive DCIS are not good candidates for NSM because
of reported high rates of locoregional recurrence [60]. Use
of intraoperative frozen section can identify most patients
with occult NAC involvement. Preservation of the NAC
may enhance cosmetic outcome and overall patient
satisfaction.
7.3 Conclusions
Most patients are candidates for immediate breast recon-
struction after mastectomy. For patients who will require
PMRT, immediate reconstruction is controversial, but many
authors have reported acceptable cosmetic results and
locoregional recurrence rates with immediate reconstruc-
tion. NSM may be an attractive option for women for risk
reduction, or in selected patients with early-stage breast
cancer.
References
1. Tuttle TM, Habermann EB, Grund EH, Morris TJ, Virnig BA
(2007) Increasing use of contralateral prophylactic mastectomy for
breast cancer patients: a trend toward more aggressive surgical
treatment. J Clin Oncol 25:52035209
2. Serletti JM, Fosnot J, Nelson JA, Disa JJ, Bucky LP (2011) Breast
reconstruction after breast cancer. Plast Reconstr Surg 127:124e
135e3. DSouza N, Darmanin G, Fedorowicz Z (2011) Immediate versus
delayed reconstruction following surgery for breast cancer.
Cochrane Database Syst Rev CD008674
4. Miller MJ (1998) Immediate breast reconstruction. Clin Plast Surg
25:145156
5. Langstein HN, Cheng MH, Singletary SE, Robb GL, Hoy E, Smith
TL, Kroll SS (2003) Breast cancer recurrence after immediate
reconstruction: patterns and significance. Plast Reconstr Surg
111:712720(discussion 721712)
6. Newman LA, Kuerer HM, Hunt KK, Ames FC, Ross MI, Theriault
R, Fry N, Kroll SS, Robb GL, Singletary SE (1999) Feasibility of
immediate breast reconstruction for locally advanced breast
cancer. Ann Surg Oncol 6:671675
7. OBrien W, Hasselgren PO, Hummel RP, Coith R, Hyams D,
Kurtzman L, Neale HW (1993) Comparison of postoperative
wound complications and early cancer recurrence between patients
undergoing mastectomy with or without immediate breast
reconstruction. Am J Surg 166:15
8. Gieni M, Avram R, Dickson L, Farrokhyar F, Lovrics P, Faidi S,
Sne N (2012) Local breast cancer recurrence after mastectomy and
immediate breast reconstruction for invasive cancer: A meta-
analysis. Breast 21(3):230236
9. Agarwal S, Pappas L, Neumayer L, Agarwal J (2011) An analysis
of immediate postmastectomy breast reconstruction frequency
using the surveillance, epidemiology, and end results database.
Breast J 17:352358
10. Dean C, Chetty U, Forrest AP (1983) Effects of immediate breast
reconstruction on psychosocial morbidity after mastectomy.
Lancet 1:459462
11. Drucker-Zertuche M, Robles-Vidal C (2007) A 7 year experience
with immediate breast reconstruction after skin sparing
mastectomy for cancer. Eur J Surg Oncol 33:140146
12. Buchholz TA, Strom EA, Perkins GH, McNeese MD (2002)
Controversies regarding the use of radiation after mastectomy in
breast cancer. Oncologist 7:539546
13. Schechter NR, Strom EA, Perkins GH, Arzu I, McNeese MD,
Langstein HN, Kronowitz SJ, Meric-Bernstam F, Babiera G, Hunt
KK, Hortobagyi GN, Buchholz TA (2005) Immediate breast
reconstruction can impact postmastectomy irradiation. Am J Clin
Oncol 28:485494
14. Kronowitz SJ, Robb GL (2004) Breast reconstruction and adjuvant
therapies. Semin Plast Surg 18:105115
15. Motwani SB, Strom EA, Schechter NR, Butler CE, Lee GK,
Langstein HN, Kronowitz SJ, Meric-Bernstam F, Ibrahim NK,Buchholz TA (2006) The impact of immediate breast
reconstruction on the technical delivery of postmastectomy
radiotherapy. Int J Radiat Oncol Biol Phys 66:7682
16. Kronowitz S, Hunt K, Kuerer H, Strom E, Buchholz T, Ensor J,
Koutz C, Robb G (2009) Immediate versus delayed repair of
partial mastectomy defects in breast conservation. Breast Cancer
Res 11(Suppl 1):S8
17. Koutcher L, Ballangrud A, Cordeiro PG, McCormick B, Hunt M,
Van Zee KJ, Hudis C, Beal K (2010) Postmastectomy intensity
modulated radiation therapy following immediate expander-
implant reconstruction. Radiother Oncol 94:319323
82 J. L. Marti and V. Sacchini
-
7/29/2019 08 Principles Indications and Limits
7/8
18. Kronowitz SJ (2010) Delayed-immediate breast reconstruction:
technical and timing considerations. Plast Reconstr Surg
125:463474
19. Huang CJ, Hou MF, Lin SD, Chuang HY, Huang MY, Fu OY,
Lian SL (2006) Comparison of local recurrence and distant
metastases between breast cancer patients after postmastectomy
radiotherapy with and without immediate TRAM flap
reconstruction. Plast Reconstr Surg 118:10791086 (discussion
10871078)
20. Wright JL, Cordeiro PG, Ben-Porat L, Van Zee KJ, Hudis C, Beal
K, McCormick B (2008) Mastectomy with immediate expander-
implant reconstruction, adjuvant chemotherapy, and radiation for
stage II-III breast cancer: treatment intervals and clinical
outcomes. Int J Radiat Oncol Biol Phys 70:4350
21. Nahabedian MY, Momen B (2008) The impact of breast
reconstruction on the oncologic efficacy of radiation therapy: a
retrospective analysis. Ann Plast Surg 60:244250
22. Anavekar NS, Rozen WM, Le Roux CM, Ashton MW (2011)
Achieving autologous breast reconstruction for breast cancer
patients in the setting of post-mastectomy radiotherapy. J Cancer
Surviv 5:17
23. Javaid M, Song F, Leinster S, Dickson MG, James NK (2006)
Radiation effects on the cosmetic outcomes of immediate and
delayed autologous breast reconstruction: an argument about
timing. J Plast Reconstr Aesthet Surg 59:1626
24. Adesiyun TA, Lee BT, Yueh JH, Chen C, Colakoglu S, Anderson
KE, Nguyen MD, Recht A (2011) Impact of sequencing of
postmastectomy radiotherapy and breast reconstruction on timing
and rate of complications and patient satisfaction. Int J Radiat
Oncol Biol Phys 80:392397
25. Spear SL, Ducic I, Low M, Cuoco F (2005) The effect of radiation
on pedicled TRAM flap breast reconstruction: outcomes and
implications. Plast Reconstr Surg 115:8495
26. Barry M, Kell MR (2011) Radiotherapy and breast reconstruction:
a meta-analysis. Breast Cancer Res Treat 127:1522
27. Cordeiro PG, Pusic AL, Disa JJ, McCormick B, VanZee K (2004)
Irradiation after immediate tissue expander/implant breast
reconstruction: outcomes, complications, aesthetic results, and
satisfaction among 156 patients. Plast Reconstr Surg 113:87788128. McCarthy CM, Pusic AL, Disa JJ, McCormick BL, Montgomery
LL, Cordeiro PG (2005) Unilateral postoperative chest wall
radiotherapy in bilateral tissue expander/implant reconstruction
patients: a prospective outcomes analysis. Plast Reconstr Surg
116:16421647
29. Singletary SE (2008) Surgical management of inflammatory breast
cancer. Semin Oncol 35:7277
30. National comprehensive cancer network (2012). NCCN clinical
practice guidelines in oncology. Breast Cancer (Version 3.
2012):1167
31. Chin PL, Andersen JS, Somlo G, Chu DZ, Schwarz RE, Ellenhorn
JD (2000) Esthetic reconstruction after mastectomy for
inflammatory breast cancer: is it worthwhile? J Am Coll Surg
190:304309
32. Slavin SA, Love SM, Goldwyn RM (1994) Recurrent breastcancer following immediate reconstruction with myocutaneous
flaps. Plast Reconstr Surg 93:11911204 (discussion 12051197)
33. Jabor MA, Shayani P, Collins DR, Jr., Karas T, Cohen BE (2002)
Nipple-areola reconstruction: satisfaction and clinical determinants.
Plast Reconstr Surg 110:457463 (discussion 464455)
34. Freeman BS (1962) Subcutaneous mastectomy for benign breast
lesions with immediate or delayed prosthetic replacement. Plast
Reconstr Surg Transplant Bull 30:676682
35. Wellisch DK, Schain WS, Noone RB, Little JW 3rd (1987) The
psychological contribution of nipple addition in breast
reconstruction. Plast Reconstr Surg 80:699704
36. Boneti C, Yuen J, Santiago C, Diaz Z, Robertson Y, Korourian S,
Westbrook KC, Henry-Tillman RS, Klimberg VS (2011)
Oncologic safety of nipple skin-sparing or total skin-sparing
mastectomies with immediate reconstruction. J Am Coll Surg
212:686693 (discussion 693685)
37. de Alcantara Filho P, Capko D, Barry JM, Morrow M, Pusic A,
Sacchini VS (2011) Nipple-sparing mastectomy for breast cancer
and risk-reducing surgery: the Memorial Sloan-Kettering Cancer
Center experience. Ann Surg Oncol 18:31173122
38. Chen CM, Disa JJ, Sacchini V, Pusic AL, Mehrara BJ, Garcia-
Etienne CA, Cordeiro PG (2009) Nipple-sparing mastectomy and
immediate tissue expander/implant breast reconstruction. Plast
Reconstr Surg 124:17721780
39. Crowe JP, Patrick RJ, Yetman RJ, Djohan R (2008) Nipple-sparing
mastectomy update: one hundred forty-nine procedures and clinical
outcomes. Arch Surg 143:11061110 (discussion 1110)
40. Paepke S, Schmid R, Fleckner S, Paepke D, Niemeyer M,
Schmalfeldt B, Jacobs VR, Kiechle M (2009) Subcutaneous
mastectomy with conservation of the nipple-areola skin:
broadening the indications. Ann Surg 250:288292
41. Lambert PA, Kolm P, Perry RR (2000) Parameters that predict
nipple involvement in breast cancer. J Am Coll Surg 191:354359
42. Gerber B, Krause A, Reimer T, Muller H, Kuchenmeister I,
Makovitzky J, Kundt G, Friese K (2003) Skin-sparing mastectomy
with conservation of the nipple-areola complex and autologous
reconstruction is an oncologically safe procedure. Ann Surg
238:120127
43. Brachtel EF, Rusby JE, Michaelson JS, Chen LL, Muzikansky A,
Smith BL, Koerner FC (2009) Occult nipple involvement in breast
cancer: clinicopathologic findings in 316 consecutive mastectomy
specimens. J Clin Oncol 27:49484954
44. Cense HA, Rutgers EJ, Lopes Cardozo M, Van Lanschot JJ (2001)
Nipple-sparing mastectomy in breast cancer: a viable option? Eur J
Surg Oncol 27:521526
45. Vyas JJ, Chinoy RF, Vaidya JS (1998) Prediction of nipple and
areola involvement in breast cancer. Eur J Surg Oncol 24:1516
46. Spear SL, Willey SC, Feldman ED, Cocilovo C, Sidawy M, Al-
Attar A, Hannan C, Seiboth L, Nahabedian MY (2011) Nipple-
sparing mastectomy for prophylactic and therapeutic indications.Plast Reconstr Surg 128:10051014
47. Petit JY, Veronesi U, Orecchia R, Rey P, Martella S, Didier F,
Viale G, Veronesi P, Luini A, Galimberti V, Bedolis R, Rietjens
M, Garusi C, De Lorenzi F, Bosco R, Manconi A, Ivaldi GB,
Youssef O (2009) Nipple sparing mastectomy with nipple areola
intraoperative radiotherapy: one thousand and one cases of a five
years experience at the European institute of oncology of Milan
(EIO). Breast Cancer Res Treat 117:333338
48. Laronga C, Kemp B, Johnston D, Robb GL, Singletary SE (1999)
The incidence of occult nipple-areola complex involvement in
breast cancer patients receiving a skin-sparing mastectomy. Ann
Surg Oncol 6:609613
49. Petit JY, Veronesi U, Rey P, Rotmensz N, Botteri E, Rietjens M,
Garusi C, De Lorenzi F, Martella S, Bosco R, Manconi A, Luini A,
Galimberti V, Veronesi P, Ivaldi GB, Orecchia R (2009) Nipple-sparing mastectomy: risk of nipple-areolar recurrences in a series
of 579 cases. Breast Cancer Res Treat 114:97101
50. Spear SL, Hannan CM, Willey SC, Cocilovo C (2009) Nipple-
sparing mastectomy. Plast Reconstr Surg 123:16651673
51. Lagios MD, Gates EA, Westdahl PR, Richards V, Alpert BS
(1979) A guide to the frequency of nipple involvement in breast
cancer. A study of 149 consecutive mastectomies using a serial
subgross and correlated radiographic technique. Am J Surg
138:135142
52. Chung AP, Sacchini V (2008) Nipple-sparing mastectomy: where
are we now? Surg Oncol 17:261266
7 Principles for Breast Reconstruction: Indications and Limits 83
-
7/29/2019 08 Principles Indications and Limits
8/8
53. Benediktsson KP, Perbeck L (2008) Survival in breast cancer after
nipple-sparing subcutaneous mastectomy and immediate
reconstruction with implants: a prospective trial with 13 years
median follow-up in 216 patients. Eur J Surg Oncol 34:143148
54. Wagner JL, Fearmonti R, Hunt KK, Hwang RF, Meric-Bernstam
F, Kuerer HM, Bedrosian I, Crosby MA, Baumann DP, Ross MI,
Feig BW, Krishnamurthy S, Hernandez M, Babiera GV (2012)
Prospective evaluation of the nipple-areola complex sparing
mastectomy for risk reduction and for early-stage breast cancer.
Ann Surg Oncol 19:11371144
55. Voltura AM, Tsangaris TN, Rosson GD, Jacobs LK, Flores JI,
Singh NK, Argani P, Balch CM (2008) Nipple-sparing
mastectomy: critical assessment of 51 procedures and
implications for selection criteria. Ann Surg Oncol 15:33963401
56. Wijayanayagam A, Kumar AS, Foster RD, Esserman LJ (2008)
Optimizing the total skin-sparing mastectomy. Arch Surg
143:3845 (discussion 45)
57. Cheung KL, Blamey RW, Robertson JF, Elston CW, Ellis IO
(1997) Subcutaneous mastectomy for primary breast cancer and
ductal carcinoma in situ. Eur J Surg Oncol 23:343347
58. Sacchini V, Pinotti JA, Barros AC, Luini A, Pluchinotta A, Pinotti
M, Boratto MG, Ricci MD, Ruiz CA, Nisida AC, Veronesi P, Petit
J, Arnone P, Bassi F, Disa JJ, Garcia-Etienne CA, Borgen PI
(2006) Nipple-sparing mastectomy for breast cancer and risk
reduction: oncologic or technical problem? J Am Coll Surg
203:704714
59. Caruso F, Ferrara M, Castiglione G, Trombetta G, De Meo L,
Catanuto G, Carillio G (2006) Nipple sparing subcutaneous
mastectomy: sixty-six months follow-up. Eur J Surg Oncol
32:937940
60. Petit JY, Veronesi U, Orecchia R, Curigliano G, Rey PC, Botteri
E, Rotmensz N, Lohsiriwat V, Cassilha Kneubil M, Rietjens M
(2012) Risk factors associated with recurrence after nipple-sparing
mastectomy for invasive and intraepithelial neoplasia. Ann Oncol
23(8):20532058
61. Reynolds C, Davidson JA, Lindor NM, Glazebrook KN, Jakub
JW, Degnim AC, Sandhu NP, Walsh MF, Hartmann LC, Boughey
JC (2011) Prophylactic and therapeutic mastectomy in BRCA
mutation carriers: can the nipple be preserved? Ann Surg Oncol
18:31023109
62. Kronowitz SJ, Hunt KK, Kuerer HM, Babiera G, McNeese MD,
Buchholz TA, Strom EA, Robb GL (2004) Delayed-immediate
breast reconstruction. Plast Reconstr Surg 113:16171628
84 J. L. Marti and V. Sacchini