0750647132 - Binocular Vision Orthoptics
148
-
Upload
maria-jose-toro-rojas -
Category
Documents
-
view
425 -
download
27
Transcript of 0750647132 - Binocular Vision Orthoptics
-
Butterworth-HeinemannLinacre House, Jordan Hill, Oxford OX2 8DP225 Wildwood Avenue, Woburn, MA 01801-2041A division of Reed Educational and Professional Publishing Ltd
& A member of the Reed Elsevier pic groupFirst published 2001
Original articles Optician 1998-1999Revisions and new material Reed Educational and Professional Publishing Ltd 2001
All rights reserved. No part of this publication may be reproduced in any material form(including photocopying or storing in any medium by electronic means and whether or nottransiently or incidentally to some other use of this publication) without the writtenpermission of the copyright holder except in accordance with the provisions of theCopyright, Designs and Patents Act 1988 or under the terms of a licence issued by theCopyright Licensing Agency Ltd. 90 Tottenham Court Road, London, England W1P aLP.Applications for the copyright holder's written permission to reproduce any part of thispublication should be addressed to the publishers
British Library Cataloguing in Publication DataA catalogue record for this book is available from the British Library
Library of Congress Cataloguing in Publication DataA catalogue record for this book is available from the Library of Congress
ISBN0750647132
Typeset by David Gregson Associates, Beccles, SuffolkPrinted and bound in Spain
HlIt EHRYTn'U: TIIATWEPUBLISH, nUTIERWORTHHEINEMANNWILL PAY FOR8TCVTOPLANT ANU CAREI'OR ATREE.
-
Contributors
Paul AdlerBSe FCOptom DipCL
Alec AnsonsFRCS FRCOphth
Angela BishopBSe FCOptom DBO
Dick BruenechBSe PhD
Sandip DoshiPhD BSe MCOptom
Frank EperjesiBSe PhD FCOptom FAAO
Bruce EvansBSe PhD FCOptom DCLP FAAO
Sarah HoskingPhD MCOptom FAAO DBO
Adrian JenningsPhD FCOptom
John SiderovPhD MSeOptom MCOptom FAAO
Alison SpencerDBO
-
Preface
This book started life as a compilation of aseries of 16 articles that were published inthe journal Optician between 1998 and2000. Nine leading experts in the field ofbinocular vision and orthoptics were in-vited to write these articles. The series wasacclaimed a success. and led to the idea forthis venture. Each author was invited to up-date their article to form the chapters ofthis book. It is due to the willingness and en-thusiasm of these individuals that thisbook has been possible. and we thank themfor this.
The original articles were designed tomeet the needs of eye-care professionalswho encounter binocular vision anomalies;hence the reader will find that this book isbiased towards the commonest clinical bin-ocular vision problems. Several chaptersconcentrate on the very common con-ditions of heterophoria and vergence
anomalies. particularly convergence insuf-ficiency. Different authors have been in-vited to cover these important topics fromslightly different approaches. and it is ourbelief that this diversity of expert opinionstrengthens the book. Indeed, whilst thisbook is cohesive in its content, it is hopedthat the presentation of different authors'approaches will help readers to gain abalanced perspective.
More than 90 per cent of NHS contactsare said to occur in primary care. With itsfocus aimed at practitioners working inthis sector, Binocular Vision and Orthopticshas been designed to stress investigationsand treatments that are appropriate in thisarea of patient care. Although a greatmany orthoptic problems can be treated inthis environment, some can only be treatedmedically or surgically, and these topicsare also covered in this book.
Some of the topics in Binocular Vision andOrthoptics are dealt with in more detail inanother Butterworth-Heinemann book.Pickwell's Binocular Vision Anomalies, writ-ten by Dr Bruce Evans. For the keen readerthis book provides an interesting, addi-tional source of information.
Some practitioners confess to perceivingbinocular vision and orthoptics as intimi-dating subjects. We believe that, once at-tacked with an inquisitive and logicalapproach, these topics are far from daunt-ing. Indeed, we feel that they are amongstthe most fascinating and rewarding chal-lenges that eye-care practitioners can en-counter. We hope that this book will helppractitioners to share this enthusiasm,which can only be of benefit to theirpatients.
BruceEvansSandipDoshi
-
1Optometric evaluation of
binocular vision anomaliesPaul Adler
Prevalence of binocular problemsHistory
SymptomsObservations of the patient
VisionRefraction
Cover-uncover testHeterophoria measurements
ConvergenceJump convergence
AccommodationMotility
HeterophoriaBinocular sensory adaptationsMonocular sensory adaptations
The routine eye examination should bestructured to detect all abnormalities of theeye and refraction. To that end, some formof evaluation of the binocular systemshould be undertaken on every patientwith two eyes. A working knowledge ofbin-ocular vision anomalies is thus essential toenable practitioners to rule out. treat orrefer appropriate binocular vision cases.
Prevalence of binocularproblems
Research shows that up to 8 per cent ofchil-dren have significant refractive errors,although the definition of 'significant'varies (lngran et al., 1986). According tomany authorities (Vaughan and Asbury,
1977; Simpson et al., 1984; Kasmann-Kellner et al., 1998; Abrahamsson et al.,1999). 2-4 per cent have strabismus andup to 5 per cent have amblyopia. dependingon how amblyopia is defined (Preslan andNovak. 1998). In optometric practice. thechild patient is likely to be self-selecting orreferred if the practice has a special interestin binocular vision or in children. Theresult of this is that most optometric prac-tices will have a very large incidence ofpatients who have significant refractiveerrors and binocular problems. Childrenwill become adults. and these adults will bevery aware of the problems they had whenyoung and seek help or reassurance.Added to this is the large number ofpatientswho have common low-grade binocularproblems such as convergence insuffi-
ciency and accommodative dysfunctions.There is little in the literature to establishreliably the prevalence of general binocularproblems. One study of second-year optom-etry students (Porcar and Martinez-Palomera, 1997) found that 32 per centsuffered from such problems, and Hokoda(Hokoda, 1983) found a prevalence of 21per cent with general binocular dysfunc-tions.
History
Taking a good history is the cornerstone ofa good binocular routine. This will help toestablish a differential diagnosis and aidinvestigation, which should begin with de-termining the most likely cause.
-
Z Billocular Visioll alld Orthoptics
This applies to patients requiring investi-gation for binocular vision anomalies andto patients who have come for routine eyeexamination.
Since amblyopia and strabismus fre-quently present at typical ages, it is impor-tant to elicit details of onset and, wherepossible, the course of the condition. This isuseful in determining the likely prognosisand if referral is appropriate. Vital informa-tion required to make a proper evaluationincludes:
Age of onset of symptoms (ifany) Frequency of symptoms Time of occurrence of symptoms Speed of onset of symptoms Constancy of symptoms General health of the patient at the time
the symptoms were first noticed Any previous ocular investigations or
treatment.
Age of onset of symptomsUnderstanding the age of onset of the bin-ocular problems is vital in order to enable aprognosis to be made. Most authorities sug-gest that unless there is early interventionfor amblyopia and strabismus, the prog-nosis is poor. Griffin and Grisham (1995)feel that any strabismus manifest beforethe age 4 months can be classified ascongenital. After this period there has beensignificant development of the accommoda-tive system, and the description 'early ac-quired' could be used. They use the term'late acquired' for problems occurring upto the age of 2 years but after 4 months.
Determining the exact month of onsetwill help to determine how long there hasbeen normal cortical stimulation prior tostrabismus setting in. This will help thepractitioner to decide on the urgency of thecase, especially if surgery is a considera-tion.
Frequency of symptomsEstablishing the frequency ofthe symptomswill help to establish the severity of the con-dition and the prognosis. Severe, annoyingsymptoms usually suggest recent onset.and in these cases binocular evaluationneeds to rule out incomitancy due to sys-temic conditions such as diabetes orGraves' disease. Other causes include a de-compensating heterophoria. Previous his-tory is obviously a factor here, and it issometimes useful to contact the patient's
previous practitioner if the patient has notbeen seen previously.
Factors in decompensating heterophoriawill depend upon the binocular status ofthe patient, but could be caused by generalillness, fatigue, stress or an increase inwork load, as is frequently the case instudents coming towards the completion ofa course that culminates in examinations.
In these cases there is usually a decom-pensating heterophoria, commonly exo-phoria, but on occasions there is atendency towards accommodative excessas a direct consequence of attempting toutilize accommodative convergence for amild convergence insufficiency.
Time of occurrence of symptomsCareful evaluation of when the symptomsoccur helps to complete the picture. For ex-ample, in a young child symptoms oftenoccur after close work, suggesting particu-lar attention be paid to the near visual per-formance during the consultation. Indivergence excess, for example, intermit-tent asthenopia and photophobia asso-ciated with television viewing or driving isa useful clue. In these cases it is prudent toevaluate distance ocular motor balanceoutside the confines of modern examina-tion rooms. Viewing distances at the full6 m or more will often enable the problemto be found, using a cover test, that willotherwise be missed.
Speed of onset of symptomsUnderstanding when the symptoms firststarted allows the practitioner to pinpointthe aetiology. Diplopia with sudden recentonset deserves very careful evaluation andassessment. Symptoms should always beevaluated in association with other signs.Vascular accidents, neurological problemsor space-occupying lesions could causesudden onset diplopia. Raised intracranialpressure is another cause of sudden onsetstrabismus often associated with reducedvision. These patients often have recent his-tory of headache and nausea, and spendingan appropriate time on interviewing thepatient is invaluable. Practitioners shouldnot be slow to reach for an ophthalmoscopeor in arranging urgent visual field assess-ment in this category of patient.
Constancy of symptomsConstant strabismus rarely gives rise tosymptoms if it has been present for sometime. Almost by definition, it will be oflong
duration and less problematical for thepatient. Intermittent binocular problemscan be more difficult to assess because theymay not be present at the initial consulta-tion. Where binocular evaluation is unableto elicit any problems commensurate withthe symptoms, it is always advisable to askthe patient to return at a time when thereare most likely to be obvious difficulties. ITthis is not possible, repetitive testing mayfatigue patients enough to break downtheir ability to maintain compensated bin-ocular vision.
General health of the patientIt is useful to establish the state of health ofthe patient at the time that symptoms firstpresented. For example, there is the often-quoted onset of hypermetropia and conver-gent strabismus associated with measles. Itseems unlikely that the measles wouldcause either of these conditions, but it ismuch more likely that the patient willbecome decompensated and unable to copewith the effort to maintain stable binocularvision during a febrile illness such as this.
Family ocularhistoryIt is well known that there is a strong asso-ciation between those patients who have afamily history of strabismus and those thatarc hypermetropic. The incidence of stra-bismus, for example, is between 2 and 4per cent in the general population. In pri-mary care, nearly 10 per cent of patientshave some sort of binocular problem.
In large studies of children (Blum et a!"1959; Waters, 1984) levels of visual diffi-culties have been found to be between 1 'iper cent and 22 per cent, with some studiesfinding as many as 38 per cent of patientswith abnormalities (Kasmann-Kellner etal., 1998). Most of these are non-strabismicand relatively easy to treat.
For patients with a parent who has stra-bismus, there is a four-fold increase in theincidence. Where there is strabismus in aparent and over 2 D of hypermetropia, therisk factor for strabismus is increased byfour to six times (Ingram and Walker,1979; Abrahamsson et al., 1999). Forthose patients with a strong family historyand high hyperopia there is a 50 per centchance of developing strabismus (Abra-hamsson et al., 1999).
The group of patients most likely to visitan optometrist is self-selecting (those whoare particularly aware of potential visualproblems will be those who have family
-
Optometric evaluation oj binocular vision anomalies YIiI 3
members with significant visual histories).Optometrists should therefore expect to seea higher than average number of patientspresenting with binocular problems.
The patient's family history, includingthat of parents, uncles, cousins, siblings,grandparents and children, should besought. Details of ocular deviations, am-blyopia and refractive difficulties should berecorded.
General personalhistoryGeneral personal history should includepregnancy and birth delivery, including de-tails ofpre-term, forceps or Caesarean deliv-eries. which could cause birth trauma. andthe health of the baby after birth.
Developmental history and informationabout illness. regular medication. systemicdisease. accidental or non-accidental headtrauma and emotional crises must berecorded.
Previous ocular history and treatmentThis may be confused. since the patient hasoften been told that there are epicanthalfolds or has sought advice from inappropri-ate sources. Where there has been inter-vention from an eye-care professional, it isalways best to ensure that the details aresought from that practitioner rather thanrelying on the history from the patient.
Symptoms
Patients suffering from decompensated het-erophoria often complain of a variety ofsymptoms that could disappear if strabis-mus develops along with sensory adapta-tions (suppression or abnormal retinalcorrespondence). These symptoms may bedifflcult to elicit from small children since,even if they are able to express themselves.children often assume that everyone suffersfrom the same problems and consider themto be normal.
Symptoms could include intermittentblur for distance or reading; letters orwords doubling or moving; closing one eyewhen reading; confusing, omitting or re-peating words; and lack of concentrationon close work (Table 1.1). In addition, thepatient might report loss of place duringreading. burning. itching. tearing and sen-sitivity to light in the absence of anteriorsegment pathology. Some patients reportthat they have difficulty with activities re-quiring good eye-hand co-ordination,
TableLl SyaptDma .Iodatedwithclecompe..18tID1heterophoria
Intermittentblura~ distanceor near Closing oneoyewhenreading Confu.slng, omitting or repeating words
duringreadingWks Lack ofconcentratlon onclose work Loss of place,butnlng, Itchingor tearing
duringreadlnl Sensittvt~y to I1gh~
such as ball games. and sometimes thatthey bump into things.
Headaches are common in children andin adults. It is always vital to establishwhen they occur. where. how frequently,how severe the pain is. and what type ofpain is experienced. It is also useful toenquire if there is any association betweenthe headaches and possible sinusitis.Migraine headaches are an important dif-ferential diagnosis. Field examinationshould be performed on all patients present-ing with headache of unknown aetiology.
Observations of the patient
General observations of the patient are im-portant. Head turns and tilts often indicatesome problem with extraocular muscles,and the head posture tends towards thefield of action of an under-acting muscle tohelp the patient avoid potential binocularembarrassment. Postural changes and ex-cessive effort during visual tasks could indi-cate that all is not well. Patients will oftenexperience more difficulty during the test.as they become tired. This is especially thecase if they are only just coping and arethen forced to operate beyond their comfortzone. Cursory examinations will almostcertainly result in missing vital clues andsigns that will manifest themselves as fati-gue sets in. Care should be taken to associ-ate symptoms with the binocular testresults. Conversely. results that do not fitwith the patient's symptoms requirefurther clarification.
Vision
Vision should be measured monocularlyand binocularly, both with and without
E
H ZCE)P
T N CCO) V
&\.) PCF) E(B) LS 0 PCE) Z(B) D
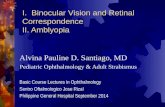
Figure 1.1Examples of letter chart and possibleconfusions (in script brackets) typicalofamblyopicpatients
the habitual spectacles. in order to assessthe effect of the prescription on both thevision and the binocular state. For non-am-blyopic eyes Snellen charts are sufficient.but for patients who are unable to achievewhat can be considered normal levels ofvision. alternative charts (e.g. LogMar) arepreferable. The standard clinical criterionfor Snellen testing to assess the visionthreshold is to continue the test until onlySOper cent ofthe letters ofthe line are accu-rately identified. This is usually easy innon-amblyopic eyes; however, in amblyo-pic eyes the first and last letters are oftencorrectly read in a number of different lineswhile mistakes are made in the inter-mediate letters (Figure 1.1).
The reason for this is often cited as the'crowding phenomenon'. It is sometimesknown as contour interaction, in whichthere is interference of the letter contoursfrom surrounding letters. This is dependenton letter thickness. separation of lettersand chart design.
For this reason line acuity is more impor-tant a measure of acuity than single letteracuity, and where amblyopia is suspectedboth should be measured (Table 1.2).
Table1.Z Amblyopia Ihould beIUlpected when
Letters are missed on several lineson Snel-len~esttna
Letters are more frequently missed In themiddle than at the endof the line
Letters are transposed InposlUon Isolated letteracultyIsbetter byoneor two
linescompared with singleletter acuityorfullchart acuity
-
4 Binocular Vision and Orthoptics
Figure 1.3Cambrid,qe crowdingcardsshould beused when testing children's binocularvision
Figure 1.2Lo,qMAR charts:letter sizesareequalas theyarebased on a logarithmicscaleof theminimum angleof resolution
Another possible cause of difficulty inamblyopia is that localization and fixationskills tend to be poor. Griffin and Grisham(1995) suggest that in a complex environ-ment, amblyopic spatial uncertainty andunsteady fixation can lead to an increasednumber of fixation errors. A restricted fieldwith fewer errors is less distracting andtherefore each letter can be fixated moreeasily.
Bailey-Lovie charts are a distinct im-provement over Snellen charts and stepsbetween the letter sizes are equal. beingbased on a logarithmic scale of theminimum angle of resolution. These areknown as LogMar charts. and are excellentfor binocular vision assessment (Figure1.2).
When testing children there are severalalternative tests available, including theKay picture test. Lea symbols, Ffooks cube,Ilhterute-E and Sheridan-Gardiner. Othersare available to deal with crowding, suchas the Cambridge crowding cards (Figure1.3), Keeler LogMar crowding charts, Leacrowding cards and the Kay crowdingpicture cards. Preferential looking (PL)tests such as the Cardiff acuity cards are ex-ceptionally helpful and easy to use for verysmall children unable to letter match orname letters/pictures.
As an additional diagnostic aid, a 2 logunit neutral density filter placed in front ofthe amblyopic eye will distinguish betweenrefractive, strabismic and organic amblyo-pia. An eye with strabismic amblyopia willperform at least as well (or even better)through the filter once dark adapted, whilethe eye with organic amblyopia will showa reduction in acuity that can be quitemarked.
Refraction
Any binocular assessment would be incom-plete without a thorough refractive evalua-tion. This is not surprising given therelationships between accommodation andconvergence as well as the influence on ac-curacy of these factors in relation toacuity. Furthermore the patient may de-velop strategies to deal with minor bin-ocular problems, which can easily beremedied by prescribing accurate and ap-propriate refractive compensations.
Many practitioners are surprised by theeffect of even quite low-powered prescrip-tions on relatively minor vergence or ac-commodative difficulties. Dwyer and Wick(1994) reported improvement in binocularfunction after 1 or more months of wearinginitial spectacle corrections in 143 non-strabismic patients who had a refractiveerror and a vergence anomaly, an accom-modative anomaly, or a combined
vergence and accommodative anomaly.Recovery of the normal vergence or accom-modative function depended on the type ofrefractive error. They reported that 79 percent of hyperopic astigmats recovered and20 per cent of myopes recovered. Of the as-tigmats, 67 per cent of those with against-the-rule improved, as did 45 per cent ofthose with against-the-rule astigmatism.Patients were more likely to benefit fromthis approach under the age of 12 years(63 per cent), and only 41 per cent of olderpatients benefited. Those with vergence dis-orders were more likely to be successful(67 per cent), but only 38 per cent ofpatients with basic exophoria were success-fully treated in this manner. Whilst thisstudy shows the benefit of dealing with therefractive element, caution and carefulfollow-up is advised.
Cover-uncover test
This is an essential test in all binocularvision routines, and one with which allpractitioners will be familiar. In fact. whileit is the cornerstone of binocular assess-ment (after all, it is the only test that willdistinguish between heterophoria and stra-bismus), many practitioners are so familiarwith it that they pay it scant regard. Inrecent years students have been en-couraged to estimate the degree of themovement, and hence the amount of
-
Optometric evaluation of binocular vision anomalies til 5
heterophoria present. Checking the ap-proximate amount of movement is easy. At6 m. the 6/12 Snellen line is approximately12 em long. and looking from one end tothe other will give the approximate move-mentof 2~.
While estimations are useful, practi-tioners should beware. since it has beenshown that cover tests give underestima-tions of results - especially at near - by asmuch as I I A of exophoria and 13~ of eso-phoria (Calvin et al., 1996) using the USstandard method of measuring heterophor-las.
Cover testing is used to determine if thereis a heterophoria or strabismus present, toelicit the presence of A or V patterns. andto allow estimates of the size. direction andrate of recovery of the deviation. It is alsoused to establish the preferred eye and toallow a rough evaluation of the patient'sability to maintain fixation. Whilst thisbook will not attempt to explain the basicmethod of cover test procedures, a fewuseful points are discussed. The author's10 tips on the cover-uncover test are givenbelow.
Clinical pearls for the cover-uncover test:
Make sure that the patient looks at aletter size slightly larger than theletter representing the thresholdacuity to ensure that fixation Is easilymaintained.
Distance testing Is recommended ath m, but Iflntermlttent divergent stra-bismus for distance Is suspected It Isbetter to test at 20 m, Near testing Isperformed at either 30 em or 40 em.depending on who gives the advice.Ideally, practitioners should test atthe habitual near working distance ofIhe patient.
Make sure the illumination level inthe room Is high and that the patientis well lit (but It Is not so bright as tocause glare or discomfort).
Remove the cover vertically; this willavoid the observer doing a beautifulcover test on hlrn- or herself.
Holdthe cover In place long enough toget a good result - some authoritiessuggest 1 s, some 2 s (Evans, 1997).Recent research suggests that 4-5 smay be the period of choice (Barnard.1447). Barnard has suggested that
the speed of recovery movements aregood predictors of symptoms. but thatthe number of movements are not.
If amblyopia is suspected take a littlelonger before removing the cover, asthe amblyople eye takes longer totake up fixation.
Do not assume there Is no strabismusIfyou see no movement. There couldbe a mlerotropla (see Chapter 11)with abnormal retinal correspond-ence. so consider a 4~ suppressiontest and the Bagolinl lens test (seeChapter 9).
Use the alternating cover test If youare unsure of the direction of move-ment and to see how easily the bino-cularity breaks down. There shouldbe no difference In the amplitude ofthe heterophorlas In each eye fornormal subjects (Barnard, 1997).
When the patient wlll not pay atten-tion. consider using multiple targetsa few centimetres apart and watch fora versional movement to re-Ilxate,
Do not use additive prisms with theirbases In the same direction to measurethe heterophoria or strabismus angle;they do not add arithmetically. For in-stance, adding a 40A and a 5A prismgives 58A (Stldwell, 1990).
A useful tool for assessing what goes onunder the cover is an opaque occluder,which is available from several sources. IThis allows the observer to see the eyebeing occluded but prevents the owner ofthe eye from seeing more than 6/60 equiva-lent and thus suspending normal binocularvision, almost as if the occluder wasopaque.
Decision making in assessment of thecover test inevitably involves the consid-eration of history, symptoms, and thespeed and quality of recovery as well as theangle of deviation or degree of hetero-phoria.
It Is useful, especially if referring forfurther treatment. to measure the hetero-phoria/tropia using a prism cover test. Thisis accomplished by estimating the amountof heterophoria and direction, and thenneutralizing the movement by introducinga prism bar in front of one eye. In a strabis-mic patient it should be placed in front ofthe deviating eye to measure the primaryangle.
The cover test is then repeated to assess ifthe estimate is correct. and the prism barmoved to adjust the level of prism intro-duced if the estimate is inaccurate. The pro-cedure is repeated until there is nomovement on repeating the cover test.
A caveat is justified at this point. Repeat-ing a cover test will inevitably interferewith fusion and increase the risk of bin-ocular breakdown. which will exaggeratethe amplitude ofheterophoria or heterotro-pia measured. It should thus be appreciatedthat the least number of attempts atmeasuring will yield the most accurateresults.
Clinical pearlIt Is essential to be aware that measure-ment of the deviation will result In 11change of what Isbeing measured.
Heterophoria measurements
Confirmation of the cover test results andassessment of the level of decompensationmay be very useful, and can be made by uti-lizing any ofthe recognized methods of het-erophoria measurements (e.g, Maddoxwing test). The aligning prism, often calledthe 'associated heterophoria' or 'fixationdisparity'. can be measured using the Mal-lett unit. It has been suggested that if bothtests are to be used in a patient with bin-ocular instability, the aligning prismshould be measured first (Braustet and [en-nings.1999).
AC/A ratioUnderstanding the patient's AC/A ratio willhelp to predict the expected change in het-erophoria measurements when sphericallenses are added. There will be a corre-sponding amount of vergence induced forevery dioptre of accommodation exerted.This can be calculated. However, mostpractitioners use a clinically derived valuecalled the gradient AC/A ratio.
It can be measured either at distance or atnear. For distance measurements, a pair ofminus lenses is added to the basic distancerefraction result and the distance hetero-phoria re-measured, The measured changethen becomes the value of the AC/A ratio.The ratio can be measured at near. when
-
6 Binocular Vision and Orthoptics
either plus or minus lenses may be added.The results are not, however, always thesame for both the plus and minus gradients.The reason for this difference is often to befound in the results of the accommodativefacility tests. It cannot necessarily beassumed that the patient will accommodateaccurately through the plus or minuslenses, and thus all the results should betreated with a certain amount of caution.Nevertheless, the AC/A ratio can beusefully employed to assess the effect of therefractive correction on the ocular motorbalance whilst considering managementoptions in binocular vision management.
Convergence
Testing for convergence can be done im-mediately after the cover test. If a repeatedcover test has been necessary to ensurethat accurate information is recorded, careshould be taken to ensure that there is suffi-cient time to allow binocular vision to bere-establishcd. This may involve asking thepatient to read a few lines of text. It is aswell to start off by assessing how well fixa-tion is maintained and then to bring thetarget in closer to the patient. The targetused is either a vertical line, which canmore easily be noticed by the patient if it be-comes double, or a letter of 6/9 equivalent,which has become the clinical standard(Griffin and Grisham, 1995). A picturemay be better for small children. These tar-gets will allow a normal amount of accom-modation to be used. For this reason it isnot really a test of pure convergence, and itmay be better to use a dim pen-torch lightif it is desirable to measure convergencefree from accommodation.
There is often debate in optometric circlesregarding the best target to be used, withsome suggesting that a fine pencil point orpen is sufficient and others insisting thatan 'accommodative' target is required.This is generally believed to be a smallletter. This author believes that an accom-modative target can be either of these,since the main criterion in this respect isthe ability of the patient to pay andmaintain attention to the target, whichthen results in accurate accommodation.
Many patients are unable accurately toreport diplopia, sometimes confusing itwith blur, while others are so slow that theresults would be totally inaccurate if
recorded. Objective assessment is thereforeessential.
Failure values of over 8 em have beensuggested (Griffin and Grisham, 1995),although Jones (1997) emphasized that itis better to be able to maintain convergencecontrol accurately in the 15-20 cm range.There is a lack of research that has at-tempted to control all the variables intesting of convergence. Hayes et al. (1998)suggested that a cut-off value of 6 emwould identify the worst 15 per cent ofcases in children, and that 73 per cent ofthese were likely to be symptomatic.
Three attempts should be made at the testbefore any conclusion is reached. As withmost things practice makes perfect. and animprovement is expected on each succes-sive attempt. If the results become repeat-edly worse, there is a suggestion of ill-sustained convergence. This can be theresult of poor convergence, reducedfusional reserves, poor accommodation, orsimply difficulty in maintaining attention.
The patient should be asked when dis-comfort is noticed, as this may be morerelevant than when diplopia occurs. Anote of this distance should be made, aswell as the more usual blur, break andrecovery points. When blur or diplopia isnoted, cover each eye in turn and ask thepatient if the print becomes clear or is stillblurred. This will allow differentiationbetween an accommodative and a conver-gence problem.
Assuming that the motility test revealsno abnormalities of the medial rectimuscles, then there should theoretically beno problem in converging almost all theway to the nose for most individuals(Griffin and Grisham, 1995).
Jump convergence
This is a measure of the ability to make ver-gence movements from one distance to an-other and to maintain fixation withoutbeing distracted. The targets used are oftenpencil tips or small letters on tongue depres-sor-type boards, held at 20 em and approxi-mately 35 ern, or sometimes 50 em, Thepatient is asked to fixate from one ofthe tar-gets to the other and back again on com-mand. The quality of movements isrecorded. It can often be observed thatwhile convergence is normal. the patienthas a problem with maintaining fixation.The optometrist needs to decide if there is a
primary problem with attention, fixation,convergence or visual figure ground.
Occasionally convergence can be sofragile and physiological diplopia such asurprise that patients are unable tomaintain concentration on the targetbecause they are distracted by the physio-logical diplopia or the background againstwhich the target is held. This can causeconfusion, and it is as well to ask patientsto explain what they can see. Sometimesthe convergence can be better controlled ifthe background is more homogeneous. Oc-casionally the brightly coloured shirt andtie or clothing that the examiner iswearing can be the cause of an apparentconvergence problem. Where this is thecase, it could be assumed that any increasein background 'noise' from a visual pointof view could cause a breakdown in bin-ocular function.
The 20b. dioptre fusion testThis is often used with children as a screen-ing test to evaluate the ability of patients tomake a vergence movement to fuse a de-tailed near vision target. It is an excellenttest for young children where other testsprove difficult. It is quick, easy and requiresno special equipment.
A 20b. prism is placed with the basealong the horizontal line and orientatedbase outwards. This will displace the imagetowards the nasal position and if single bin-ocular vision is to be maintained, willresult in the immediate initiation of afusional vergence movement inwards tore-establish fixation. Observation of thefusional movement is made. In addition,the number of movements, smoothnessand speed of re-taking fixation is assessedto gain an idea of the quality of fusion. Thetest should be performed once with theprism before the right eye and again, aftera pause for fusion to stabilize, with theprism before the left eye.
The 4b. base-out suppression testThis test is used to attempt to ascertain if asuppression area is present. If this is thecase during a cover test, it implies there is amicro-strabismus.
The patient fixes an accommodativetarget and the clinician introduces a 4b.base-out prism in front of the right eye andthen in front of the left eye. If there is nosuppression zone, there will be nomovement of the eye after the prism isadded. This is because the apparent
-
Optometric evaluation of binocular vision anomalies lIli 7
movement of the object induced by theprism will be unobserved by the patientbecause it will fall on the suppressed area.This test is discussed in detail in ChapterII, where it is noted that an isolateddetailed target is most appropriate.
Bruckner testThis is a simple and very sensitive test fordetecting strabismus. although it is notalways reliable. The clinician shines adirect ophthalmoscope light at the bridgeof the patient's nose from a distance ofaround 75 em, and observes the red fundusreflex within the pupils. This should beequal in appearance ifthere is no significantrefractive error or strabismus. Where thereis a strabismus, the red reflex will appearbrighter. There are some exceptions to thisrule, which must be taken into considera-tion in view of other clinical findings. Pupilsizedifferences, pigmentary differences andrefractive anisometropia all will lead to thefixing eye appearing to have the brighterreflex (Griffin and Cotter, 1986; Griffin etal., 1989).
The Hirschberg testThis test was first used in the latter part ofthe nineteenth century. with a candle as alight source. Nowadays a pen-torch light isshone at the eyes of the patient from a dis-tance of 50-100 ern, The examiner ob-serves the corneal reflexes with his or herdominant eye directly behind the lightwhilst the patient fixes the light.
Some authorities suggest that 1 mm ofdisplacement of the reflex is equivalent to
12~. Others (Griffin and Grisham, 1995)have suggested that the value should bemore like 1 mm to 22~. as proposed byJones and Eskridge (1970) and the photo-graphic study by Griffin and Boyer (1974).It is vital to take angle K into considerationwhen looking at the results of this test. Azero angle is rare, and it is usual for thereto be an angle represented by displacementof the pupil reflex of around +0.5-+1.0 mm. The realistic sensitivity is there-fore limited to about 5~. since it is almostimpossible to observe a displacement ofany less than 0.25 mm.
The Krimsky testThis is a similar test to the Hirschberg test.which adds accuracy by using a prism barto centralize the corneal reflex. As in theHirschberg test, it is important to assessthe position ofthe pupil reflexes in each eye
in turn when measuring the angle. Thiscould be affected by prism adaptation. andtherefore the prism should be introducedfor a short period of time only - in theregion of 2-3 s would be appropriate. Inpractice, if the patient is able to sit still longenough and maintain fixation accurately.cover testing can usually be accomplished.As a consequence. this test is rarely used inpractice.
The fusional range testThis tests the ability of a patient to react toincreasing demands on vergence byhaving to adjust the fusional vergence (seeChapter 3). This is usually accomplishedeither by use of a prism bar, in which case astepped vergence response is being tested.or by use of Risley rotary prisms. which in-duces smooth increasing demands. Thetest can also be performed using a synopto-phore. vectograms and tranaglyphs. Griffinand Grisham (1995) suggested a speed of
4~ dioptres per second be used.No assessment of binocular vision is
complete without evaluating this impor-tant function. which is performed atdistance and at the patient's usual readingdistance. Prisms are introduced. andslowly increased. with the patient fixing atarget that is appropriate to ensure good ac-commodative interest.
It is customary in orthoptic practice tomeasure the point when the patientreports diplopia or the clinician notices mis-alignment of the eyes. This is called thebreak point. The value of prism when bin-ocular function is restored is also recorded.This is known as the recovery point. Thenormative values expected are different de-pending on whether step or smooth
Table 1.3 Adequate values forfusional ranses at near(after Griffin andGrisham, 1995)
Base Out Blur point 15 to 17 Breakpoint 22 to 28 Recovery point 8 to 11
Base In Blur point 12 to 13 Breakpoint 20 to 21 Recovery point 11to 13
vergence testing is performed (see Table1.3 for expected results).
Additional valuable information may begleaned by asking the patient to reportwhen the object of regard becomes blurred.This will be the point at which the patientcan no longer maintain accommodationon the target and begins to lose comfortablebinocular function. This value may bemore significant from a functional point ofview than the break point. since it isunlikely that any patient will continue tobe able to function efficiently after this'blur point' has been reached.
When a patient reports that the targetseems to be moving. there is suppressionpresent. Good observers will also noticethat for base-out demand, the target willappear to be reducing in size.
Understanding the information gleanedin measuring fusional ranges will aid thepractitioner in deciding the significance ofthe binocular problems. and will help in re-evaluation during progress checks whiletreatment progresses.
Accommodation
Because of the physiological link betweenaccommodation and convergence. an as-sessment of the binocular status must in-clude evaluation of the accommodativesystem.
The ability to stimulate and release ac-commodation both monocularly and bin-ocularly, and to change focus from onedistance to another, should be checked toensure that skill levels in both eyes aresimilar where appropriate. The relation-ship between accommodation and conver-gence is also an important factor. and thisshould be considered when making deci-sions in dealing with the patient.
Near point ofaccommodationThis test is usually performed both mon-ocularly and binocularly (Scheiman andWick. 1994; Griffin and Grisham, 1995;Adler. 1998). In the UKmost texts refer tothe RAF rule. which is considered to be thepreferred method of use. This is convenientbecause of the easy scales on the rule,which relate centimetres. dioptres andnorms for age. However, the disadvantageof a rest pressing firmly on the patients'cheeks may increase awareness of wherethey should be looking. There is sufficientevidence in recent literature to suggest
-
8 Binocular Vision and Orthoptics
ability to stimulate accommodation. It isoften assumed that all patients are able torelease accommodation that has beenstimulated. Moving the target closer to thepatient than the blur point and then bring-ing it out again can check this. The patientshould be asked to report when the text be-comes clear again.
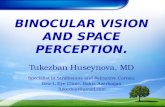
Figure 1.4Semi-opaque occluder beingusedduring nearpoint of accommodation testing. Thepatient canbarelyread 6/60 but the eye undercovercaneasily beseenby the observer. Note that the right eyeis appropriately converging underthe coverduringaccommodation
that the proximal effect is significant (Northet al., 1993). This problem can easily be re-duced by using a simple near card and a re-tractable tape measure.
The near point of accommodation shouldbe measured in each eye. and significantdifferences should be noted and evaluatedin the light ofthe other findings. Treatmentcan be instituted if necessary. In the sameway that convergence should be testedseveral times, accommodation should alsobe tested at least three times. In normalpatients there will be a small learningeffect. This will result in each measurementbeing at least the same as the previous one,if not slightly better. In patients with ac-commodative insufficiency, there is likelyto be a receding near point of accommoda-tion.
The results obtained monocularly shouldbe compared to those obtained binocularly.This will help to decide if there is an im-provement when convergence is involved,which is the expected result. If there is a re-duction in accommodative near point bin-ocularly, poor convergence or reducedbase-out fusional reserves should be sus-pected (base-out fusional reserves are alsoknown as positive or convergent fusionalreserves).
Testing for the near point of accommoda-tion skills should be done slowly. This willallow time for the patient to register ifthere has been a subjective blur and thento tell the practitioner. An excellent tool foraiding diagnosis is the semi-opaque
occluder (Figure 1.4). Accommodationwill produce a convergence effect in botheyes, and if the eye under the cover ceasesto converge it can safely be assumed thatthe patient has stopped accommodating.Likewise, observation of pupil reflexes is aneasy way to assess the performance of thepatient. Pupils will continue to constrictwhilst there is an increasing accommoda-tive response, and when the patient stopsaccommodating the pupils will be seen todilate.
If accommodative insufficiency is sus-pected, latent hypermetropia should beexcluded by cycloplegic examination. Analternative to this is the Mohindra methodof near point retinoscopy.
It is vital in cases of suspected insuffi-ciency that the target is brought all theway towards the nose. It is very easy to mis-diagnose accommodative excess if this isnot diligently performed. since the assump-tion is that the patient has reached his orher near point. In many instances thepatient is unable to control accommodationaccurately and institutes an 'all-or-nothing' strategy, resulting in accommoda-tive excess or spasm. In these cases thetarget becomes clearer as it is broughtcloser still. and near point retinoscopy willreveal accommodation is leadingcompared to convergence.
Releasing accommodationTesting accommodation as described abovewill enable an assessment of the patient's
Interactive accommodation(binocular accommodative facility)Having tested the patient's ability to stimu-late. sustain and release accommodation.it is useful to check if the patient canchange accommodation at will. This test iscommonly used by optometrists, and canprovide valuable information about the dy-namics of the accommodative system. Thisis accomplished by the accommodative flip-per method, and is often referred to as ac-commodative facility (flippers availablefrom Paul Adler. 50 High Street. Stotfold,Hertfordshire SG5 4LL). This is first donemonocularly. and then binocularly.
Reduced interactive facility has been as-sociated with asthenopic near pointsymptoms in young children (McKenzie etal..1987).
The patient is asked to fix a suitable neartarget at 40 ern whilst looking through a-2.00 D lens. The introduction of a-2.00D lens will initially make the printblur. The patient must recognize this, andwork out if the blur needs to be resolved byadding extra accommodation or by releas-ing accommodation. The patient is askedto report that the print is as clear as it wasbefore the lens was introduced. The lensholder is flipped to the other side. whichhouses a +2.00D lens. In order to 'clear'this. the initial accommodation resultingfrom the -2.00 D lens will need to bereleased. as well as another 2.00 D. Theability to make both tasks clear is called acycle. Most normative values in the litera-ture are measured in cycles per minute(Zellers et al., 1984; Table 1.4).
Once the ease of stimulating and releas-ing accommodation has been establishedin each eye in turn. testing can beginbinocularly. Siderov suggested this shouldbe called interactive facility. because itreally measures the ability to operate theaccommodative system whilst makingflexible and appropriate changes invergence in order to maintain binocularsingle vision (Siderov, 1990). Treatment isusually based on orthoptic principles, and
-
Table1.4 Accommodative racilltynorm. (Zellen et al.1984)
+/ --2.00 11cycles per minute monocular !l cycles per minute binocular for young
adults 17cycles per minute monocular I] cycles per minute binocular f> cycles per minute with suppression
control
Optometric evaluation of binocular vision anomalies II 9
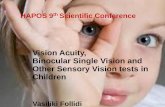
Figure 1.5Diagram showing thecardinal diagnostic directions ofgaze andtheextraocular muscles pulling inthose directions
is effective after only a few hours training(Siderov and Johnson, 1990).
Adding a pair of minus lenses will resultin the stimulation of accommodation toensure the print clarity is maintained. Itwill inevitably result in an increase in con-vergence. In these circumstances, this willbring convergence closer than the plane ofthe paper and hence produce what is effec-tively an esophoric posture. In order toensure that there is no diplopia or perceivedblur, a vergence movement outward isrequired. This can be accomplished eitherby utilizing base-in fusional reserves (oftenreferred to as negative or divergentfusional reserves), or by inhibiting accom-modative convergence.
The converse will be true of asking thepatient to clear a pair of plus lenses. In thiscase, it will be necessary to release accom-modation. This will result in a release of ac-commodative convergence, which willlead to an exophoric posture. To cope withthis. the patient will need to be able toutilize fusional convergence. If the fusionalreserves are low this will be difficult atspeed. and thus there will be a low score onthis test.
Observations over a 1 minute period willhelp to determine precisely what is happen-ing. Sometimes the patient begins well andbecomes fatigued despite good monocularskills; other times the patient may beunable to accomplish the task at all. Someauthorities feel that measurements can beaccurately taken over a 30 second periodso long as the clinician is aware of the waythe patient performs the test. so that alonger period can be given if difficulties aresuspected (Siderov, 1990).
Ideally. in the binocular situation thepatient should be asked to use some form ofsuppression control to avoid a situationwhere only one eye is really being used.
This can be in the form of a thumb-barreader or, more conveniently, a red-greenor polarized bar reader with the appropriatered-green or polarized glasses. The OXOtest on the Mallett unit can be used, butpatients need to be advised to ignore anymovement of the strips.
Despite the usefulness of this method ofmeasurement of binocular accommodativefacility (interactive facility) there are somepotential hazards in its use, and theaccuracy of clinical measurements of ac-commodative facility has been criticized(Kedzia et aI., 1999). Measurements areprone to errors due to strong practiceeffects(McKenzieet aI., 1987). Single meas-urements should be interpreted withcaution, Test parameters are critical, andvariations in target size, testing distance,lens power used, speed of 'flipping',lighting and task demand, and whether thepatient or clinician is holding the textshould be noted. Decreasing distance willresult in an improved ability to do this test,which has been attributed to a strongproximal effect(Siderov, 1990).
Motility
Testing for ocular movements is another es-sential test. There should be smooth move-ments throughout the motor field of action
of the extraocular muscles within the bin-ocular field (the field where both eyes areoperating together) and also in the mon-ocular field, where the eyebrows or nosemay be restricting the view.
The test is designed to elicit over- orunder-action of the extraocular musclesand to identify any incomitancy. A non-focused pen torch at 33 cm is used forfixation, and the patient is asked to lookdirectly at it. The pupil reflexes areobserved for symmetry, but it is importantto check where the reflexes appear to bemonocularly since the pupil centre andposition of the line of sight through theoptical components of the eye may notcoincide, resulting in non-central pupilreflexes. Once the position of the reflexes isknown, they can be observed for any depar-ture from normal as the test proceeds.
The light is moved along each ofthe diag-nostic directions of gaze (Figure 1.5). Thepatient can be asked to report any diplopia;however, careful observation needs to bemaintained since long-standing strabismusoften leads to inhibition of the image be-longing to the non-fixing eye.
The pen torch should be moved in an arcin front of the patient, as in a perimeter.until the point is reached where the pa-tient's eyes stop moving. Repeating the testwith a near fixation card (in the shape of atongue depressor) as the target will allowthe patient to observe any tilting more
-
10 Biflocular Visiofl afld Orthoptics
easily. This helps to identify any torsionalelement of the deviation.
It should be noted that the verticalmeridian is not a diagnostic direction ofgaze. However. it is still useful to test inthis direction, since it will help to identifysome A and V patterns.
The horizontal meridians will onlyinvolve the lateral and medial recti, and itis often convenient to start with these. Nar-rowing of the palpebral fissure and also lidlag, which can be signs of Duane'ssyndrome or hyperthyroidism (Dwyer andWick, 1994), should be noted. Thediagonal meridians should then be tested.
The practitioner should look for an over-or under-action of the muscles. If unsure, itis worthwhile performing a cover test inthe nine cardinal points of gaze. In incomi-tant deviations, patients may reportdiplopia. The image seen furthest awaybelongs to the eye with the under-actingmuscle that pulls in that direction.
It is not uncommon to find that morethan one muscle is affected. Over longperiods of time contracture may take place,leading to complications in making a firmdiagnosis regarding which muscle is theprimary problem. The use of a red andgreen filter to help the patient identify thediplopia is a useful and valid way to makethe diagnosis easier.
A useful tip when deciding if there is anover- or under-action is to remember thatthe image belonging to the under-actingeye is further away.
Hess chartsUntil recently it was rare for optometrypractices to possess a Hess or Lees screen.These tend to take up lots of space, and thetime required led to only those practicesthat specialized in this area using them.More recently a computerized Hess screenhas become available which is accurate,quick and affordable (available from DrDavid Thomson, telephone/fax 01707851051).
Heterophoria
Heterophoria is measured under disso-ciated conditions. These dissociation testsmeasure the departure from the situationwhere the lines of sight would intersect theobject of regard without fusional vergence.
By deflnttion. the dissociated hetero-phoria is measured in the absence of bin-
ocular fusion (Super, 1992). The eyes areusually dissociated by a device such as aMaddox rod or by vertical prism. Hetero-phoria measurements are useful to elicitthe degree of stability, size and direction ofthe heterophoria. Some authorities favourassessing heterophoria solely by the covertest and measuring the aligning prismusing, for instance, a Mallett unit.
The aligning prism is independent of theamount of the heterophoria itself, and is ameasure of the ability of the patient to com-pensate for the heterophoria. Mallettclaimed that the degree of retinal slip(fixation disparity) is related to asthenopiaand gives an indication of how to prescribe.The dissociated heterophoria and aligningprism have the apex ofthe correcting prismin the same direction as the deviation.
Binocular sensory adaptations
SuppressionSuppression (see Chapter 8) is usually thefirst line of defence for an individual experi-encing diplopia following the onset of stra-bismus, and is one form of sensoryadaptation. Small suppression zones canoccur in microtropia. Superficial foveal sup-pression can also occur in some cases ofhet-erophoria, and this could be a reason whysome apparent convergence insufficiencypatients fail to respond to simple exercises.In normal binocular vision, physiologicalsuppression naturally occurs outside thehoropter and there is active cortical inhibi-tion (Griffinand Grisham, 1995).
Suppression can vary in its intensity on acontinuous scale from shallow (superficial)to deep, as well as in its size and position(either central or peripheral). Central sup-pression can extend 5 from the fovea.
There are many tests for suppression, allof which vary in sensitivity. Shallow sup-pression can be elicited using a pen torchat a distance at which the strabismus ismanifest, and asking the patient if diplopiacan be seen. Seeing two lights under theseconditions indicates that either there is nosuppression at all, or there is very shallowsuppression. If one light is reported, an ad-ditional neutral density filter or a red lensshould be inserted in front of the fixing eyeand the patient asked if he or she sees onered light (in which case the other eye is sup-pressing), a pink light (in which case therewill be fusion), or both a red and a white
light (indicating a diplopic response).Patients with strabismus and ARC mayreport some variation to a pink light. indi-cating fusion, whilst those with suppres-sion and alternating strabismus will reportthat the light changes from red to pink.The advantages of this technique are thatit is quick and easy, and that most trialcases and phoropters have a red lens.Other methods include the Worth four-dottest, stereoscope tests, bar-reading tech-niques, the Bagolini lens or even thenonius bars on a Mallett unit. The Mallettunit also has a specific test using words,some of the letters of which are seen byboth eyes and some just by the left or righteyes. These are of increasing size and allowa measure of the degree of suppression.
In heterophoria, any foveal suppressionneeds to be eliminated if full binocularfunction is to be restored.
Another test for suppression is the 4t:.base-out test at near (see Chapter 11).
Abnormal retinal correspondence(ARC)
Abnormal retinal correspondence (seeChapter 9) is another binocular adaptation.and occurs when correspondence exists be-tween areas of the retina on the fixing andstrabismic eye that receive the same image.The correspondence allows the brain to'pretend' there is no diplopia, and permitsthe development of a limited degree ofstereopsis. ARCis often described as harmo-nious or unharmonious; however, unhar-monious ARC must be accompanied bydiplopia, and if it is seen on clinical testingin the absence of diplopia then it is alwaysan artefact of the test.
ARC is examined with a Bagolini lensplaced before the non-fixing eye while thepatient is fixing a spot light target. If a stra-bismic patient reports the streak of theBagolini lens as being centred on the spot.then ARC is present. Practitioners withoutBagolini lenses can use a distance Mallettunit at 3 m. If the patient sees that thenonius lines are aligned when a manifeststrabismus is present, there is ARC.Modern near Mallett units have a special'large OXO' test for assessing ARC and sup-pression (available from 1.0.0. MarketingLtd, Institute of Optometry, London).
StereopsisStereo-acuity should be reduced if suppres-sion is present, although it should be rc-
-
Optometric evaluation of binocular vision anomalies III 11
Figure 1.6TheSuper timed stereo test. Super (1992) suggestedthat the speedat which the stereo test isperformed is infact a better measureas to the binocularefficiency than recording the best stereoacuity achieved
membered that 2 per cent of the binocularpopulation are stereo-blind (Super, 1992).The use of sensitive stereo tests will alsoconfirm the presence of good vision, sinceit is impossible to achieve good stereopsiswithout good acuity in both eyes.
Super suggested that the speed at whichthe stereo test is performed is in fact abetter measure as to the binocular effi-ciency than recording the best stereo-acuity achieved. He has described an in-strument, along with standardized norms,to test for this, called the Super TimedStereo Test (Super, 1992; Figure 1.6).
Monocular sensory adaptations
Eccentric fixationEccentric fixation (see Chapter 10) existswhen a non-foveal point is used for fixation.Since retinal sensitivity is reduced parafo-veally, there is always a reduced acuitymeasured in these eyes that depends uponthe degree of eccentricity of fixation.
Assessment can be made by asking thepatient to fix the eccentric fixation graticuleof the direct ophthalmoscope while occlud-ing the other eye. This is usually a red-free
target to ensure that the patient remainscomfortable during the test. The fixationshould be classified by its state (i.e, steadyor unsteady), position (superior, inferior,nasal or temporal) and size in degrees fromthe centre of the fixation target. Readersshould refer to the manual of their particu-lar instrument for the precise dimensionsof the targets. In the absence of a purpose-built target, the macular stop can be usedand projected on the optic disc, which is ap-proximately 5 by 7. An estimate of thenumber of degrees of eccentricity can thenbe made relative to the optic disc.
1 Bernell, a divisionofVision Training Products,40l6N HomeStreet, Mishawaka, Indiana 4654,USA or VTE, via F. Petrarca 10, 20040 Buragodi Mologora (MI), Italy.
References
Abrahamsson, M., Magnusson, G. and Sjos-trand, J. (1999). Inheritance of strabis-mus and the gain of using heredity todetermine populations at risk of develop-
ing strabismus. Acta Ophthalmol. Scand.,77(6),653-7.
Adler, P. M. (1998). Treatment of accom-modation. CEOptom., 2(3),76-80.
Barnard, N. A. S. (1997). The cover test. Isthere anything new to learn? Lecturepresented at the 75th Anniversary Con-ference of the Institute of Optometry,London.
Blum, Peters and Bettman (1959). VisionScreening for Elementary Schools: TheOrinda Study. University of CaliforniaPress.
Braustet. R. 1. and Jennings, J. A. M.(1999). The influence of heterophoriameasurements on subsequent aligningprism measurement in a refractive rou-tine. Ophthal. Physiol. Opt., 19(4),347-50.
Calvin, H., Rupnow, P. and Grosvenor. T.(1996). How good is estimated covertest at predicting the Von Graefe hetero-phoria measurement? Optom. Vis. Sci.,73(11),701-6.
Dwyer, P. and Wick, B. (1994). The influ-ence of refractive correction upon dis-orders of vergence and accommodation.Optom. Vis. Sci., 72(4), 224-32.
Evans, B. J. W. (1997). Pickwell's BinocularVision Anomalies: Investigation and Treat-ment. 3rd edn. Butterworth-Heinemann.
Griffin, J. R. and Boyer, F. (1974). Strabis-mus: measurement with the Hirschbergtest. Optom. Today, 75. 863-6.
Griffin, J. R. and Cotter, S. (1986). TheBruckner test: evaluation and clinicalusefulness. Am. J. Physiol. Opt., 63,957-61.
Griffin. J. R. and Grisham, J. D. (1995). Bin-ocular Anomalies: Diagnosis and VisionTherapy. Butterworth-Heinemann.
Griffin, J. R., McLin, 1. and Schor, C. M.(1989). Photographic method for Bruck-ner and Hirschberg testing. Optom. Vis.Sci., 66, 474-9.
Hayes, G. J., Cohen, B. E.. Rouse, M. W, andDeLand, P. N. (1998). Normative valuesfor the near point of convergence in ele-mentary school children. Optom. Vis.Sci.. 75(7), 506-12.
Hokoda, S. C. (1983). General binocularconditions in an urban optometry clinic.J. Am. Optom. Assoc., 56, 643-7.
Ingran, R. M. and Walker, C. (1979). Re-fraction as a means of predicting squintor amblyopia in preschool siblings ofchildren known to have these defects.Br. J. Ophthalmol., 63(4), 238-42.
-
12 Binocular Vision and Orthoptics
Ingran. R. M., Walker, C.. Wilson. J. M. etal. (1986). Prediction of squint bymeans of refraction at age 1 year. Br. ].Ophthalmol.. 70(1). 12-15.
Jones. M. A. (1997). Normal and abnormalhead and eye movements in reading andtheir role in the classification and man-agement of dyslexia. Br. Orthop. J.. 54.53-5.
Jones. R. and Eskridge. J. B. (1970). TheHirschberg test. A re-evaluation. Am. J.Optom. Arch. Am. Acad. Optom.. 47.105-14.
Kasmann-Kellner, B.. Heine. M.. Pfau, B. etal. (1998). Screening for amblyopia.strabismus and refractice abnormalitiesin 1030 kindergarten children. Klin.Monatsbl. Augenheilkd. 213(3).166-73.
Kedzta, B.. Pieczyrak, D., Tonde!, G. andMaples. W. C. (1999). Factors affectingthe clinical testing of accommodativefacility. Ophthal. Physiol. Opt.. 19.12-21.
McKenzie, K. M., Kerr, S. R., Rouse, M. W.and Del.and, P. N. (1987). Study of ac-
commodative facility testing reliability.Am. J. Physiol. Opt.. 66,186-94.
North, R. V., Henson. D. B. and Smith, T. J.(1993). Influence of proximal. accom-modative and disparity stimuli upon thevergence system. Ophthal. Physiol. Opt.,13,239-43.
Porcar, E. and Martinez-Palomera, A.(1997). Prevalence of general binoculardysfunctions in a population of univer-sity students. Optom. Vis. Sci., 74(2).11l-B.
Preslan, M. W. and Novak. A. (1998). Bal-timore Vision Screening Project. Phase2. Ophthalmology, 105(1), 150-53.
Scheiman, M. N. and Wick, B. (1994). Clin-ical Management of Binocular Vision. Het-erophoric. Accommodative, and EyeMovement Disorders. Lippincott.
Siderov, J. (1990). Improving interactivefacility with vision training. Clin. Exp.Optom., 73, 4.
Siderov, J. and Johnson, A. W. (1990). Theimportance of test parameters in the clin-
ical assessment of accommodative facil-ity. Optom. Vis. Sci., 67(7). 551-7.
Simpson, A. Kirkland. C. and Silva, P. A.(1984). Vision and Eye Problems inSeven-year-olds: A Reportfrom the VIHled/nMultidisciplinary Health and Develop-ment Research Unit. Jul. 11, 97(959).445-9.
Stidwell, D. (1990). Orthoptic Assessmentand Management. Blackwell Scientific.
Super. S. (1992). Testing stereopsis: first.last or not at all? S. Afr. Optom.. 51( 3),129-34.
Vaughan. D. and Asbury, T. (1977) GeneralOphthalmology. 8th edn. Lange LosAltos.
Waters, J. (1984). Portsea modified clinicaltechnique: results from an expanded op-tometric screening protocol for children.Aust. J. Optom.. 67(5),176-86.
Zellers. J. A.. Alpert, M. W. and Rouse, M.W. (1984). A review of the literatureand a normative study of accommoda-tive facility. J. Am. Optom. Assoc., 55.31-7,166-73.
-
2Classification of comitant eye
deviationsFrank Eperjesi
TerminologyTypes of classification
HeterophoriaHeterotropia
Patients with abnormal eye movements oreye positions often present to optometristsfor advice, and through history, symptomsand evaluation the optometrist can deter-mine whether the eye deviation iscomitant or incomitant. The latter oftenhas a serious cause and requires referralfor an ophthalmological opinion,
Comitant deviations, however, are oftenamenable to vision training and/or refrac-tive management. While it is acknowledgedthat rigid classification is never strictlypossible, many comitant deviations fallinto groups, and therefore it is of value todefine the classic conditions that occur.
This chapter concentrates on the classifi-cation and appearance of comitant eye de-viations; investigation and treatment aredealt within other chapters.
Terminology
The term 'strabismus' is used in many dif-ferent ways; it has been used as anumbrella term to describe any deviation,whether a heterophoria (latent strabismus)or heterotropia (manifest strabismus). Theuse of the term 'squint' is undesirable,since in discussions with patients it maybecome confused with the more commonuse of this word to explain half-shut eyes.
The literature uses both 'concomitant'and 'comltant' to describe an eye deviationthat is the same in all positions of gaze and/or when it is the same when one or theother eye fixates, although the deviationmay vary with fixation distance. However,'cornltant' is becoming accepted as thecorrect term to describe this kind of ocularanomaly, and as it is consistent with its an-tonymous form incomitant ('non-comitant' in North America), it will beused throughout this chapter. The terms'latent strabismus' will be used synony-mously with heterophoria and 'manifeststrabismus' with heterotropia.
A brief note of the most usual forms oftreatment for each type of deviation will beincluded (see also Chapter 6); the mostcommon types of management include re-fractive correction, orthoptic eye exercises(vision training), manipulation of the re-fractive correction using small spheres andprism, and referral for medical manage-ment (see also Chapter 14) or surgery (seealso Chapter 15).
Types of classification
Comitant strabismus classification iscomplex, and deviations can be categorizedin many different ways; primary; secondary
to another condition; or consecutive (thischapter discusses only primary types);latent or manifest; constant or intermittent(relates to manifest strabismus only); withregard to eye position and direction of eyemovement during the cover-uncover andalternate cover test; with respect tofixation distance or the effect of accommo-dation; compensated or decompensated(relates to heterophoria only); and withrespect to time (Figure 2.1).
Heterophoria
Heterophoria occurs where both visualaxes are directed towards the fixation pointbut deviate on dissociation. It can be classi-fied (Table 2.1) according to; eye positionunder the cover during the cover-uncoverand alternate cover test; fixation distance;and whether compensated or not.
Fixation distanceEso- and exophoria can also be classifiedaccording to whether the size of thedeviation varies with respect to fixationdistance.
Esophoria Convergence excess; deviation greater at
near than distance
-
14 BillocllJar Visioll illld ()rtlIOI'UCS
tHyper/hypophoria
I
IExophoria
INear
IHeterophoria
tDistance
Table 1.1 Eye pOliltlon durlnt the cover test
IEsophoria
IDistance
Comltant deviationI
IFixationdistance
INear
I INon-specific Convergence weakness
IExotropia
IjDivergence
exc('ss
IIntermittent
I
I( :onsecutiv('
IEsotropia
tWitJlOUI
accommodativeelement
Isecondary
IHeterotropia
IPrimary
Constant
Withaccurumodarive
element
I 1Esotropia Exotropia Vertical
Convergenceexcess
CyclicAccomrnodat iveelement
.-LFully
accommodative
Fixationdistance~
Near Distanre
EyepOlltlon
NasalTemporalSupraInfraRotatednasally
Deviation
EsophoriaExophoriaHyperphorlaHypophorlaIncycluphorla
Figure 2.1Summary ofcomitanteye deviation classification
Divergence weakness: deviation greaterat distance than near
Non-specific (basic): deviation same atdistance and near.
Exophoria Convergence weakness: deviation
greater at near than distance Divergence excess: deviation greater at
distance than near Non-specific (basic): deviation same at
distance and near.Note that convergence insufficiency is notsynonymous with convergence weaknessexophoria. The former is characterized byan unusually remote near point of conver-gence. and is often but not always asso-ciated with an exophoria greater at nearthan distance. Convergence weakness exo-phoria is often used to describe a decompen-sated exophoria at near. and the near pointof convergence may be within the normalrange (see Chapter 5).
DecompensationHeterophoria can be classified according towhether it is compensated or not: a decom-pensated heterophoria is defined as onethat causes symptoms.. Developmental abnormalities in the
anatomical. motor or sensory systems may
result in a predisposition to symptoms.People who do not have these developmen-tal abnormalities and who are healthy andhave no undue stress on the visual systemwill remain asymptomatic. However. ifthey become ill. run down. stressed. workunder poor lighting conditions. have longperiods of close work. change occupationto a more visually demanding position. orexperience a reduction in their fusionalreserves. they may become symptomatic(Evans. 1997).
A compensated heterophoria may de-compensate as the vergence system can nolonger comfortably overcome the hetero-phoria. which may intermittently breakdown to a heterotropia. Other causes of de-compensation include uncorrected refrac-tive error. incorrectly prescribed glasses.ill-fitting spectacles. aniseikonia. fatigue.head injury. drugs and alcohol. Symptomsof a decompensating heterophoria aretypically headaches. asthenopia. blurringof print. intermittent diplopia. and visualconfusion.
Causes of esophoriaAnatomical irregularities include en-ophthalmos. narrow interpupillary dis-tance and extraocular muscle anomalies.Refractive causes are hypermetropia and
anisometropia. High AC/A ratio and weakdivergent fusional reserves can also resultin this type ofdeviation.
Causes of exophoriaExophoria can be caused by structuralanomalies including exophthalmos. wideinterpupillary distance and extraocularmuscle anomalies. Refractive causes aremyopia. presbyopia and anisometropia.Weak convergent fusional reserves and in-creasing age may also result in an exo-phoria.
Causes of hyper/hypophoriaVertical heterophorias can result from dis-placed globes. abnormal extraocularmuscles or ptosis. Refractive causes arehigh myopia. also known as heavy-eyesyndrome. Weak vertical fusional reservescan also playa role.
Other deviationsOther deviations are alternating hyper-phoria, in which either eye rotatesupwards on dissociation. and alternatinghypophoria, in which either eye rotatesdownwards on dissociation. These are dis-sociated vertical deviations. and usuallyresult from an interruption to binocularityin early life - generally infantile esotropia
-
syndrome. Cyclophoria is often associatedwith oblique astigmatism.
Classification of comitant eye deviations 15--~---------------------- -------------
Table .1.2 The types of accomodative esotropias
Treatment of heterophoriaManagement of heterophoria involves cor-rection of the refractive error. improvementof the fusional reserves with orthoptic exer-cises. and bar reading (see Chapters 3-6.16). When exercises are not an option. ma-nipulation of any refractive error usingsmall negative and plus spherical lensesmay be considered. Prismatic correctionscan be useful in some cases. For moderateor large deviations it may be necessary toreduce the angle surgically. although thisintervention is only rarely needed for het-erophoria.
Type!iof acccmodattve esotropla Distance Near
EsotropiaPully accommodattve esotropia esotropia
Convergent excess orthotropia esotropia(high ACIA ratio)
Convergent excess orthotropia esotropia(normal ACIA ratio)
Accommodative plus esotropia esotropiahigh AC!A ratio
Partially accommodatlve esotropia esotropia
Treatment
optical
optical. mfotics, surgery
surgery
optical.surgery
accommodative treatment.surgery
Heterotropia
'---------------------------------------------
Figure 2.2(a) Fullyaccommodative left convergent strabismusthat is (b) fully corrected by thehypermetropic correction
This is a condition in which one or othervisual axis is not directed towards thefixation point. It can be classified asprimary. secondary or consecutive. Aprimary deviation constitutes the initialdefect. A secondary deviation is as a resultof ocular disease. visual impairment orsurgical intervention. The latter is oftencalled consecutive. in which the originaldeviation is replaced by one with a con-trasting direction.
EsotropiaConstant esotropia withanaccommodativeelementThis deviation (Table 2.2) is presentunder all conditions and increases whenaccommodation is exerted. Onset is usuallyat 3-4 years of age, and is associated withhypermetropia. astigmatism and aniso-metropia.
A fully accommodative strabismusresults from uncorrected hypermetropia.and the patient is orthotropic whenwearing the full refractive correction(Figure 2.2). A partially accommodativestrabismus is present without spectacles.and is reduced but not eliminated by thewearing of a hypermetropic prescription.Constant deviations are normally unilat-eral and result in the typical secondarydefects associated with such a condition.e.g. amblyopia (see Chapter 10) and anom-alous retinal correspondence (see Chapter9).
Management involves correction of therefractive error and treatment of amblyo-pia; surgery may be required for a cosmetic
(a)
or functional result in cases that are notfully accommodative (see Chapter IS).Some cases can be straightened at nearwith bifocals (see Chapter 6).
Constant esotropia withoutanaccommodativeelementOne form of non-accommodative comitantesotropia is infantile esotropia syndrome.which presents in the first 6 months oflife.
Although it may be associated withhypermetropia. refractive correction rarelyreduces the size of the deviation, which isusually large. present under all conditionsand stable in size. with a limited potentialfor single binocular vision (Figure 2.3).
It may be unilateral or alternating; ifalternating the deviation will not result inamblyopia. It can be associated withdissociated vertical deviation. obliquemuscle dysfunction and latent nystagmus
(b)
(see Chapter 13). The aetiology remainscontroversial, and it may be that differentmechanisms acting early in life lead to thesame end-point.
Management involves correction of therefractive error. treatment of amblyopiaand possibly surgery for a cosmetic or func-tional result (see Chapter IS).
Comitant strabismus can be caused bypathology affecting the eye or visual areasof the brain. Cases that do not have a clearcause (e.g. uncorrected refractive error, de-compensation of previous heterophoria)should be referred for neuro-ophthalmolo-gical assessment. Cases that do notrespond to treatment should also bereferred.
Intermittentesotropia with anaccommodativeelementIntermittent convergent deviations oftenhave an accommodative element. The
-
Figure 2.3(a) A lIOn-accommodative left convergentstrabismus that is (b) not correctedby spectacles
16 Binocular Vision and Orthoptics
(a)
deviation is present only under certain con-ditions, and is therefore unlikely to causeamblyopia,
It usually occurs at 2-5 years of age, andis associated with a moderate degree ofhypermetropia and a normal AC/A ratio.The convergent deviation is affected by thestate of accommodation, and this is theprimary factor in the aetiology of the stra-bismus. Two-thirds of cases of comitantconvergent strabismus have an accommo-dative element, and the angle of deviationwill be reduced by a refractive correctionfor hyperopia, fully in some cases and par-tially in others.
For intermittent fully accommodativeesotropia, binocular single vision is presentfor all distances when the hypermetropia iscorrected. Without refractive correction,the patient is usually orthotropic fordistance and markedly esotropic for near.When fully corrected, the patient is usuallyorthotropic at distance and either esopho-ric or orthophoric for near.
Full cycloplegic refractive correction isimportant, even at the risk of reducing thedistance VA slightly, to prevent the occur-rence of a partially accommodative eso-tropia and associated amblyopia. Orthopticexercises can be used with older children tocontrol the manifest deviation (see Chapter6).
Intermittent convergence excessesotropiaIn this condition, the eyes are straight fordistant fixation but there is an intermittentncar esotropia. There may be some controlwhen Iixing on a near non-accommodativetarget such as a light. An esophoria may bepresent for distance fixation. Onset isusually at 2-5 years of age, and is more no-
(b)
ticeable when the patient is looking atclose objects. This condition is often asso-ciated with hypermetropia, but sometimesoccurs with myopia and always with anAC/A ratio of greater than 5 : 1.
These children can often be managedwell with bifocals, at least until they reachan age when they can undergo visiontherapy. Often. the strength of the nearaddition can be gradually reduced withtime until the patient is comfortablystraight at distance and near with singlevision spectacles. Treatment may alsoinvolve orthoptic eye exercises (seeChapter 6) and surgery (see Chapter 15).
Intermittent nearesotropiawithout anaccommodative elementBinocular single vision is present fordistance fixation and intermittent esotropiafor near fixation, even when any extra ac-commodative effort due to uncorrectedhypermetropia is relieved. Multifocals areinappropriate, as there is no accommoda-tive element. Any refractive error shouldbe corrected and amblyopia treated:surgery is usually indicated. Orthoptic ex-ercises can be difficult for this group ofpatients.
Intermittent distanceesotropiaThese cases exhibit an esotropia ondistance fixation and heterophoria on nearfixation. Amblyopia, if present, should betreated, and prisms can be used if the angleat distance is 100 or less: surgery may benecessary (see Chapter 15).
Intermittent cyclicesotropiaThis deviation relates to time, the anomalyoccurring at regular intervals, with the
most common pattern being an alternateday deviation. It is usually late onset, at4-5 years of age. Occasionally, after 6months, the alternate day pattern mayalter and the deviation become constant.On the strabismic day a marked deviationfor near and distance fixation is present; onthe straight day an esophoria may bepresent for ncar and distance fixation.
Surgery is usually indicated, especially ifthe deviation becomes constant.
Intermittent non-specific esotropiaThis is an intermittent esotropia not con-forming to any pattern; the deviation is in-termittently manifest at any fixationdistance and there is no significant changein the angle of deviation for ncar ordistance fixation or with accommodationexerted. Any refractive error should be cor-rected and amblyopia treated; surgery maybe considered.
By definition an intermittent strabismusis not constantly undermining binocularfunction, and therefore immediate treat-ment may not be necessary. However. ifperiodic observation reveals that the devia-tion is becoming manifest more frequently.treatment becomes urgent.
MicrotropiaThe definition of microtropia is disputed.and clinicians disagree on its characteris-tics (see Chapter 11). The terms 'microstra-bismus', 'monoflxatlon pattern' (orsyndrome) and 'subnormal binocularvision' all refer to the same or similar con-ditions. The term 'microtropia' is preferredin the following discussion.
Microtropia can be described as a devia-tion of 1-100 , with some variability in themagnitude of the angle. Besides themanifest deviation there is often a latentdeviation seen on alternate cover test.which gives the appearance of a hetero-phoria. There is usually ARC with someperipheral stereopsis.
The causal mechanism is unknown, hutit is often secondary to surgery or visiontraining for an infantile or primarycomitant esotropia. and onset is frombirth or the time of therapeutic interven-tion.
Children should have any anisometropiafully corrected and any amblyopia treated.There are usually no symptoms, but theprognosis is poor for bifoveal fusion.However. if there is inadequate fusionalvergence to control the heterophoric
-
component, older patients may becomesymptomatic and will require visiontraining.
Dissociated verticaldeviation(DVD)In this condition, when the vision of eithereye is embarrassed the affected eye deviatesprogressively upwards but reverts to itsoriginal position when the embarrassmentceases.
It may be much more apparent in one eyethan the other, and may be associated withbinocular single vision or with a manifestdeviation. There is usually a history of stra-bismus from an early age, and spontaneouselevation may be noticed by parents, par-ticularly when the patient is daydreamingor fatigued.
Symptoms are rare. DVD is often asso-ciated with infantile esotropia syndrome,and is associated with manifest or latentnystagmus. Progressive elevation of eithereye is seen under cover, and a slowdownward movement when the cover isremoved. The elevation may be apparentas the cover approaches, even before theeye is actually occluded. The upwardmovement of the eye is slow, and is moremarked on distance fixation and on pro-longed dissociation. When the occluder isremoved, the eye drifts down to the midlineand occasionally may move below themidline before moving up again to refixate.
Nystagmus blocking esotropiaThis is another type of early esotropia. Itoccurs in young children with nystagmusof early onset, typically prior to the age of 6months; an esotropia often develops as thepatient learns to adduct the fixing eye in anattempt to control the nystagmus (seeChapters 13 and] 6). It eventually leads toa large, constant, unilateral esotropia,with an abnormal head posture tomaintain the position of the adducted eye.Non-accommodative esotropia is usuallytreated with surgery, although full refrac-tive correction and treatment of any asso-ciated amblyopia is advisable.
Esotropia associated with myopiaWhen uncorrected, some adults with highmyopia may demonstrate an esotropia.The mechanism is uncertain, but normalretinal correspondence is demonstratedwhen the deviation is corrected. Visualacuity might be reduced due to degenera-tive myopic fundus changes. Management
involves constant wear of a full myopiccorrection.
ExotropiaThis is a condition in which one eyedeviates outwards, and can be classified as:primary, secondary or consecutive; inter-mittent or constant; occurring at distanceor near; and true or simulated. The follow-ing discussion relates to primary anomaliesonly.
Constant exotropiaA divergent deviation constitutes the initialdefect, which is constantly present underall conditions. Anatomical causes includewide interpupillary distance, exophthal-mos, orbital asymmetry, muscle anomaliesand craniofacial anomalies. It may behereditary, and can be associated withmyopia.
It often commences as an intermittentdeviation, which then becomes constantwith time. The deviation may increase insize when the patient is in bright sunlight,and presentation is with a history ofclosing one eye and photophobia. If thedeviation is alternating, visual acuity canbe equal.
Refractive error should be corrected andamblyopia treated. Surgery is an option(see Chapter 15) but there is a risk of post-operative intractable diplopia, and use ofBotulinum toxin A (see Chapter 14) maybe an alternative.
Intermittent exotropiaThe eyes may be diverged at times butaligned at others. Intermittent exotropia isoften related to fixation distance, but theremay be no accommodative element. Thereare three types:
1 Near-fixation type (insufficient conver-gence). An exotropia is present onnear fixation with binocular singlevision on distance fixation, althoughthere may be an exophoria in the dis-tance. Onset is usually late, and maybe associated with myopia or presbyo-pia. It is very common among youngpeople with decompensating exo-phoria, who present with diplopia andasthenopic symptoms. Investigationwill reveal a remote near point of con-vergence, a manifest deviation atnear, and binocular single vision atdistance.
2
3
Classification of comitant eye deviations 17
Management (see Chapters 5 and 6)includes correction of the refractiveerror, orthoptic exercises, base-inprisms and, rarely, surgery.Distance fixation type (excessive diver-gence). Associated with high ACjAratio and anatomical abnormalities,this is a condition in which the patientmaintains binocular single vision atnear (there may be an exophoria) andhas an exotropia at distance. The dis-tance exotropia characteristically in-creases with greater viewingdistances, so it may be useful to testthe patient when looking at an objectout of a window (greater than 6 m).
The angle of deviation for near fixa-tion may increase on prolonged disrup-tion of fusion or elimination ofaccommodation. Patients who demon-strate an increase in angle for nearfixation on occlusion or with pluslenses are described as simulated dis-tance types, and these are character-ized by an increase in angle of greaterthan 10i1 for near fixation with a+3.00 D lens. The deviation mayappear controlled initially for distance,but decompensates quickly on disso-ciation.
Onset is usually within the first yearof life but small-angle deviations maynot be present until later because ofthe intermittent nature of the devia-tion. The condition is often noticed byparents when the child is not concen-trating or is fatigued. The patient isusually asymptomatic, but may beaware of the divergence from the 'feelof the eye' or notice an increase in thevisual field.
Like the near-fixation type, the de-viation is often larger in conditions ofbright sunlight, and photophobia iscommon. Visual acuity is usuallyequal, while good binocular visualacuity indicates good control of the de-viation. Management is by full correc-tion of any myopic refractive error,under-correction of any hyperopia,orthoptic exercises for small deviations 15 i1), negative over-correctionwhen the ACjA ratio is high, base-inprisms, tinted lenses when light consti-tutes a dissociative factor, and possiblysurgery.Non-specific type. This is characterizedby a manifest divergent strabismusthat occurs at any distance and at any
-
18 Binocular Vision and Orthoptics
time. The size of the deviation does notchange with fixation distance, andcauses can be any of those describedfor t