07 March, 2006
31
Immune response to cancer Normal cell mutation Loss of growth control Tumor cells Localized (benign) Invasive (malignant) (transformation)
Transcript of 07 March, 2006

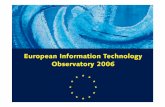
Immune response to cancer
Normal cellmutation
Loss of growth control Tumor cells
Localized (benign)
Invasive (malignant)(transformation)

Tumor rejection in mouse
Mouse
carcinogen
Tumor
Mouse (inbred, same MHC)
Tumor
Irradiated tumor cellsinduce immune responsetoward the tumor.
The protection can betransferred by T cells, not by serum.

Tumor antigens
Mutations alters the normal cellular protein to create new antigenic peptide.
Tumor specific transplantation antigens (TSTAs)
*
*
MHC
*
*
*
MHC
*

Idiotypic sequence of antigen receptor is TSTA for B and T cell tumors.
Difference between differentantigen binding sites
Antigen receptors may remain expressed by the B and Tcell tumors. The antigenbinding site is a unique feature (antigen) for the tumor.
Difference of the same IgC region betweendifferent alleles in a population.

Tumor associated transplantation antigens (TATAs)Tumor cells can express proteins of male germ cells.
Male germ cells do not express MHC and do not normally present these antigens.
Reactivation of genes normally expressed during embryonic development.
Overexpression of normal self antigen.
Oncofetal tumor antigens (alpha-fetoprotein, AFP; carcinoembryonic antigen, CEA)


Immune surveillance?
Tumors may not present tumor antigen/MHC.
Tumors tend to be genetically unstable and may lose the Expression of MHC or the tumor antigen.Such variants would have selective advantage.
Brown staining: HLA
Many cells in the prostate cancer sectionhave lost MHC expression.

MHC-loss variants could become a target for NK cells.
Nude mice are deficientIn T cells. They have higherlevels of NK cells.

Antibody binding to tumor antigens could induce endocytosis and degradation of the antigen.
Antigen presentation in the absence of co-stimulationmay cause T cell anergy.
Tumors do not induce inflammation.Inflammatory cytokines are needed to activate APCsto express co-stimulatory molecules.
Antibodies can modulate tumor antigens.

Tumors may suppress immune response.
Many tumors produce immunosuppressive cytokines such as TGF-, IL10, which inhibits TH1 and cell-mediated immune responses.
Tumors may be inaccessible to immune system.
Tumors may grow in nodules surrounded by collagens and fibrin.

Type I Hypersensitivity (immediate-type hypersensitivity, allergy)
IgE-mediated immune response to harmless environmental antigens (allergens).
Aeroallergens: pollens
Food allergens: nuts, seafood
Latex allergens
Pharmaceuticals: penicillin
Insect venom allergens: wasp venom

Der p 1 (dust mite)
Substilisin (bacteria)
Papain (Papaya)
Proteins (T cell response)
Low molecular weight
Soluble
Stable
Other features
Enzymatic activity may facilitate the entry of allergens.

Allergens are presented by DCs to CD4 T cells.
Antigen (microbial)
DCs
inflammation
CD4 T cells
IL12
TH1
IFN-, IL-2
Cell-mediatd immunity
allergen
No inflammation
DCs
CD4 T cells
TH2
Default?
IL4, IL5, IL13
IgE, allergic response
Low dose

IgE activates mast cells and basophils.
High affinity FcRI
(Basophil)
Degranulation Inflammatory mediatorscytokines
Mucosal tissues

Histamine(immediate)
Contraction of smooth muscles
Vascular permeability
Mucus secretion
LeukotrienesProstaglandins
(potent, lasting)
Cytokines
IL4, IL13 TH2
IL5, IL3, GM-CSF eosinophil
TNF- inflammation
Mast cell mediators

Recruitment of eosinophils.HSC
IL5, IL3, GM-CSF
Eosinophil
Bone marrow
Eosinophil (eosinophilia)blood
Eosinophil
Eotaxin 1 (CCL11) Eotaxin 2 (CCL24) Eotaxin 3 (CCL26)
CCR3 (eosinophil)
Mucous tissue
Cell adhesion molecules
chemokines
Activated eosinophil-FcR for IgE, IgA, IgG
Activated eosinopil-FcR-IgE Allegen
Inflammatory mediators
IL5, IL3, GM-CSF (survival, activation)

Eosinophil degranulation
Tissue damage
Allergic response

Basophils are recruited to allergic site.
Basophil Histamine, IL4, IL13
IL13 induces mucous secretion, bronchoconstriction, fibrotic process.

Primary exposure to allergen sensitize mast cells
Allergen
DC
CD4 T cell
TH2B cell
IgE
Mast cell-IgE
Sensitized mast cell

Re-exposure elicits allergic response.
Allergen
Mast cell-IgE (basophil-IgE)
Histamine, leukotrienes, Prostaglandins, IL13
Smooth muscle constrictionVasodilation, Vascular permeability
Acute phase (within minutes) Late phase (4-48 hr)
Eosinophilsneutrophils
Degranulate
TH2 cells
TH2 cytokines
Allergic responseTissue damage and remodeling
Chronic response (e.g. allergic asthma)

Peak expirationflow rate
Asthmatic response
8 hours
Mucous plugin airway
EosinophilsNeutrophilsLymphocytesin bronchial wall

The route and dose of allergen entry determineoutcome of allergic reaction.
allergen
Blood circulation
gut
Widespread activationof mast cells
Widespread vasodilationAirway constriction
Systemic anaphylaxis(anaphylactic shock)
epinephrine
Food (peanut) Drug (penicillin)

Penicillin can conjugates to proteins.

protein carrier
Hapten (antigen)
immunogen
immunizationimmunization
No response
Penicillin-protein conjugates are immunogens.

Signal 1
TH
Signal 2CD40-CD40L
cytokine
Activation
B cell

Allergen
skin
Insect bite
Wheal-and-flare
WidespreadEdematous response
Allergen (food, pepsin resistant protein)
gut
skin
circulation
DisseminatedWheal-and-flare(hives, urticaria)
Contraction of intestineOutflow of fluid into gut
Vomitingdiarrhea
Prolonged inflammation
Eczema, atopic dermatitis(persistent skin rash)
Allergen (pollen, etc)
Upper airway
Allergic rhinitis
eye
Allergicconjunctivitis
Lower airway
Allergic asthma

Genetic factors of allergy
Atopy
Chromosome 11: FcRI chain
Chromosome 5: Cluster of TH2 cytokines (IL4, IL5, IL13), IL-3, GM-CSF
IL-12 p40
Adrenergic receptor (smooth muscle responsiveness)
Chromosome 6: Class II MHC. Presentation of allergen peptides
ADAM33: Metalloproteinase expressed by bronchial smooth muscle cells and lung fibroblasts. Airway remodeling in asthma.
Chromosome 12:STAT6. IL4R signaling.

Environmental factor
Hygiene hypothesis
Exposure to infectious disease in early childhood protects against atopy.
TH0
DC
TH1 TH2
DC
IL12
TH0
TH1 TH2
inflammation
clean unclean
Inverse correlation between helminth infection and allergy?
Exposure to allergen in early childhood.

Treatment
Desensitization:Injection with increasing doses of allergen.
High density antigen presentation
TH0
TH1 TH2
Low density antigenpresentation
IgG IgE
Compete for allergen
(Unmethylated CpG?)
Anti-IgE antibodies (omalizumab)
Antihistamines block histamine H1 receptor.

Corticosteroids suppress inflammation.

Relevant part in book
Type I hypersensitivity: page 361-378.