
04 Volume Regulation
24
63 S. Faubel and J. Topf 4 Volume Regulation 4 4 Volume Regulation
Transcript of 04 Volume Regulation
63
S. Faubel and J. Topf 4 Volume Regulation
44 Volume Regulation

64
The Fluid, Electrolyte and Acid-Base Companion
The purpose of this chapter is to explain volume regulation. An under-standing of volume regulation is necessary to understand most of the disor-ders covered in this book, including hyponatremia, hypernatremia, meta-bolic alkalosis, congestive heart failure and edema formation.
Volume regulation is the simultaneous adjustment of plasma volumeand blood pressure in order to maintain the adequate perfusion of tissues.Although the term volume regulation implies only the regulation of plasmavolume, adequate tissue perfusion requires that plasma moves. The move-ment, or circulation, of plasma throughout the body requires the mainte-nance of blood pressure.
Effective circulating volume is a term which implies that for adequatetissue perfusion, plasma volume, as well as blood pressure, must be main-tained. Therefore, volume regulation should be thought of as effective circu-lating volume regulation.
3L
2L
1L
plasma volume
Volume regulation is the concomitant adjustment of plasma_________ and blood _________.
aaavolume; pressure
and
Introduction�The regulation of volume involves the regulationof plasma volume and blood pressure.
volume(effective circulating volume)
blood pressure
In this book, the terms “effective volume depletion”, “volume depletion” and “low effectivevolume” all refer to the same concept: low effective circulating volume from a decrease inplasma volume and/or blood pressure. The term “hypovolemia” is only used to refer toeffective volume depletion from fluid loss, such as with vomiting or diarrhea.

65
S. Faubel and J. Topf 4 Volume Regulation
Plasma volume is the extracellular component of the blood volume. Plasmavolume is approximately 3 liters in a 70 kg man.
Plasma volume is regulated by signals which act at various sites of thenephron to affect the resorption of sodium and water.
Sodium resorption by the kidney is the primary mechanism by whichplasma volume is increased. In the nephron, the important sites for volumeregulation are the proximal tubule and the collecting tubule. In the proxi-mal tubule, the resorption of sodium causes the resorption of water; in thecollecting tubule, the resorption of sodium occurs without water. Renal re-sorption of sodium is the first and best defense against volume depletion.
Water resorption is an additional mechanism by which the kidney canincrease plasma volume. Resorption of water alone (without sodium or an-other solute) occurs in the collecting tubules of the distal nephron. The re-sorption of water is not as effective at increasing plasma volume as theresorption of sodium. This second-line defense is employed only when vol-ume is very low.
3L
2L
1L
plasma volume
The primary mechanism of increasing plasma volume is the resorp-tion of _________ by the kidney.
aaasodium
Effective circulating volume�Plasma volume�Plasma volumeis increased through the resorption of sodium and water.
Water resorptionwithor
without
As reviewed in Chapter 1, Moles and Water, the plasma compartment is about 8% of totalbody water (TBW). In an adult man, TBW is 60% of weight. Therefore, in a 70 kg man, TBWis 42 liters (60% of 70 liters); the plasma compartment is 3 liters (8% of 42).
H2O
H2O
H2O
Sodium resorption
Na+
Na+
Na+
Na+
Na+

66
The Fluid, Electrolyte and Acid-Base Companion
Effective circulating volume�Plasma volume�Water resorptionand sodium resorption have different effects on plasma volume.
intracellular
sodium
interstitial
Water resorbed from the collecting tubules distributes between the_____________ and extracellular compartments.
The resorption of __________ is like the administration of 0.9% NaClwhich remains in the extracellular compartment. The extracellularcompartment consists of the _________ and the plasma compartments.
The effects of water resorption versus sodium resorption on plasma volumeare analogous to the effects of the administration of D5W and 0.9% NaCl.
Water resorption in the distal nephron is similar to the administration ofD5W. Remember from Chapter 2, Water, Where Are You?, that the adminis-tration of one liter of D5W only increases the plasma volume by about 80mL. Likewise, as water is resorbed from the collecting tubules and added tothe plasma, osmotic forces cause the water to redistribute among all threebody water compartments, leaving little in the plasma compartment.
Sodium resorption, on the other hand, is similar to the administration ofisotonic saline (0.9% NaCl). As sodium is resorbed in the proximal tubule,water follows. Thus, the resorption of sodium and water in the proximaltubule is isotonic. Additional sodium is resorbed in the collecting tubules.As sodium and water are added to the plasma, plasma volume is substan-tially increased because the sodium and water remain in the extracellularcompartment.
Sodium resorption
Na+
Na+
Sodium and water remain in the ex-tracellular compartment.
0.9%NaCl
670 250 80
750 250
Water resorption
Water distributes among all threebody compartments.
H2O D5W
67
S. Faubel and J. Topf 4 Volume Regulation
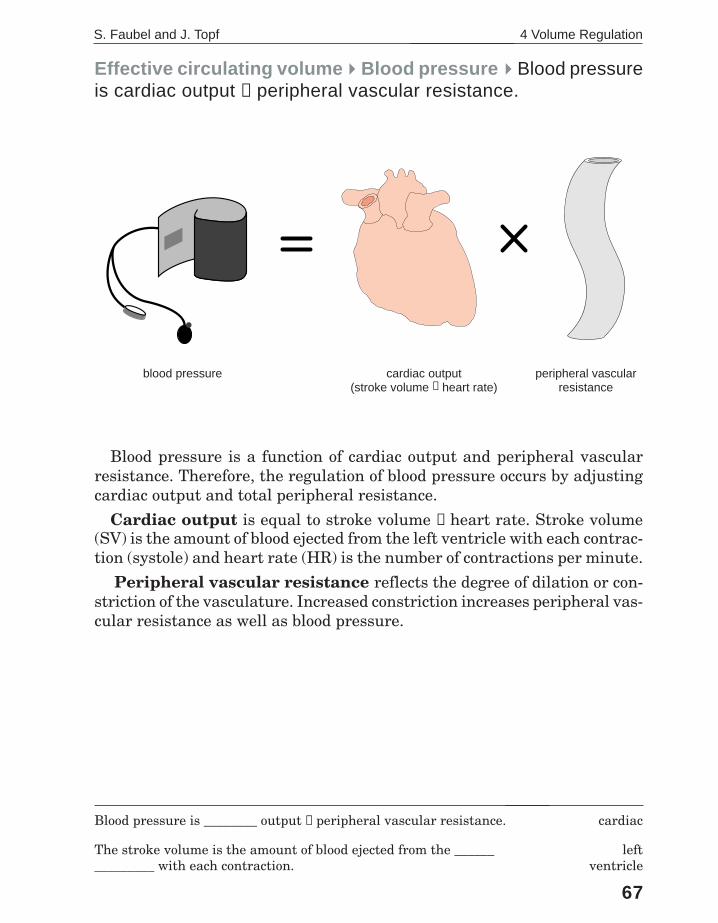
Blood pressure is a function of cardiac output and peripheral vascularresistance. Therefore, the regulation of blood pressure occurs by adjustingcardiac output and total peripheral resistance.
Cardiac output is equal to stroke volume × heart rate. Stroke volume(SV) is the amount of blood ejected from the left ventricle with each contrac-tion (systole) and heart rate (HR) is the number of contractions per minute.
Peripheral vascular resistance reflects the degree of dilation or con-striction of the vasculature. Increased constriction increases peripheral vas-cular resistance as well as blood pressure.
Effective circulating volume�Blood pressure�Blood pressureis cardiac output × peripheral vascular resistance.
Blood pressure is ________ output × peripheral vascular resistance.
The stroke volume is the amount of blood ejected from the _______________ with each contraction.
cardiac
leftventricle
blood pressure cardiac output(stroke volume × heart rate)
peripheral vascularresistance

68
The Fluid, Electrolyte and Acid-Base Companion
Volume regulation�Volume regulation occurs in three steps:monitoring, signaling and action at targets.
Volume regulation occurs in three steps:
Monitoring. Baroreceptors, located at several points throughout the body,respond to changes in blood pressure. Baroreceptors are the primary moni-tors involved in volume regulation.
Signaling. There are three types of signals which respond to stimulationby the baroreceptors:
• renin-angiotensin II-aldosterone system• sympathetic activation• antidiuretic hormone (ADH)
Action at targets. The signals act at three main targets to increaseplasma volume and blood pressure: the kidney, heart and vasculature. Ac-tion at the kidney affects plasma volume while action at the heart and vas-culature affects blood pressure.
Each of these steps are discussed in detail on the following pages.
Volume regulation is a ________-part process.
Monitoring of volume is by ________________.
Signaling is by the ______-angiotensin II-aldosterone system, ___________ activity and ADH.
The targets activated by signals are the _______, heart and vasculature.
aaathree
baroreceptors
reninsympathetic
kidney
aldosterone
angiotensin II
renin
ADH
Signaling
sym
path
etic
Monitoring Action at targets
plasma volume
Na+
Na+
Na+
H2O
H2O
H2O
blood pressureac
tivat
ion
69
S. Faubel and J. Topf 4 Volume Regulation
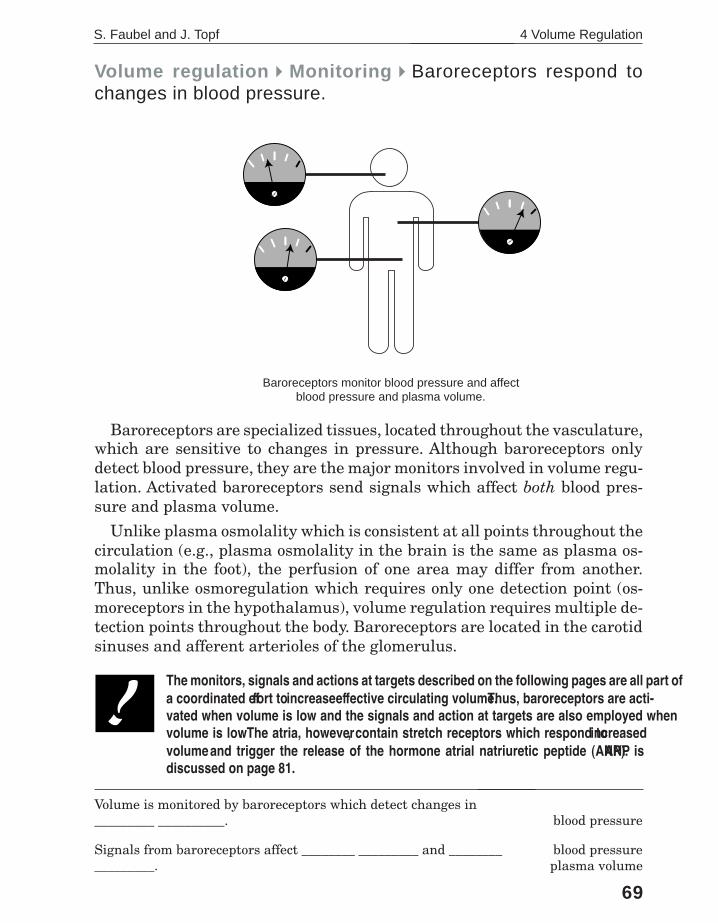
Volume regulation�Monitoring�Baroreceptors respond tochanges in blood pressure.
Baroreceptors are specialized tissues, located throughout the vasculature,which are sensitive to changes in pressure. Although baroreceptors onlydetect blood pressure, they are the major monitors involved in volume regu-lation. Activated baroreceptors send signals which affect both blood pres-sure and plasma volume.
Unlike plasma osmolality which is consistent at all points throughout thecirculation (e.g., plasma osmolality in the brain is the same as plasma os-molality in the foot), the perfusion of one area may differ from another.Thus, unlike osmoregulation which requires only one detection point (os-moreceptors in the hypothalamus), volume regulation requires multiple de-tection points throughout the body. Baroreceptors are located in the carotidsinuses and afferent arterioles of the glomerulus.
Volume is monitored by baroreceptors which detect changes in_________ __________.
Signals from baroreceptors affect ________ _________ and _________________.
aaablood pressure
blood pressureplasma volume
Baroreceptors monitor blood pressure and affectblood pressure and plasma volume.
The monitors, signals and actions at targets described on the following pages are all part ofa coordinated effort to increase effective circulating volume. Thus, baroreceptors are acti-vated when volume is low and the signals and action at targets are also employed whenvolume is low. The atria, however, contain stretch receptors which respond to increasedvolume and trigger the release of the hormone atrial natriuretic peptide (ANP). ANP isdiscussed on page 81.

70
The Fluid, Electrolyte and Acid-Base Companion
Blood pressure and plasma volume usually correlate because a drop in plasmavolume causes a drop in blood pressure. Loss of plasma volume causing a lowblood pressure occurs in dehydration and blood loss.
There are situations, however, where low blood pressure is not due to a lossof plasma volume and the associated plasma volume can actually be normal orelevated. In these disorders, it is the failure of the plasma to move, or circulate,through the vasculature which causes low blood pressure. Conditions associ-ated with both low blood pressure and increased plasma volume include heartfailure, liver failure, A-V malformations and sepsis.
Regardless of plasma volume, the response to decreased blood pressure isthe same: signals act at the heart, vasculature and kidney to increase bloodpressure and plasma volume. Increasing both blood pressure and plasma vol-ume is beneficial as it helps to restore adequate tissue perfusion. This responsecan, however, have negative clinical consequences. Increasing plasma volumein patients with normal or increased plasma volume can increase venous hy-drostatic pressure and cause pulmonary and/or peripheral edema. (Peripheraledema is discussed further at the end of this chapter.)
Volume regulation�Monitoring�Low blood pressure can beassociated with low, normal or high plasma volume.
low plasma volumelow blood pressure
normal plasma volumelow blood pressure
high plasma volumelow blood pressure
low
normal
high
low
normal
high
low
normal
high
When blood pressure is low, plasma volume can be low, normal or_____.
Low blood pressure with high plasma volume is seen in both_______ and _______ failure.
aaahigh
heart; liver
71
S. Faubel and J. Topf 4 Volume Regulation
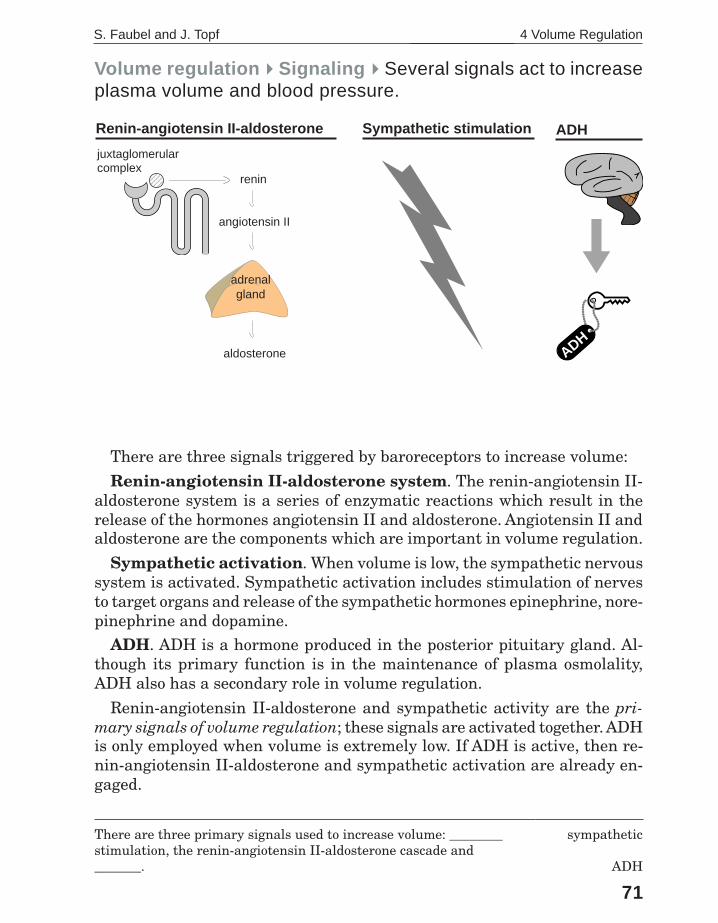
Volume regulation�Signaling�Several signals act to increaseplasma volume and blood pressure.
There are three signals triggered by baroreceptors to increase volume:
Renin-angiotensin II-aldosterone system. The renin-angiotensin II-aldosterone system is a series of enzymatic reactions which result in therelease of the hormones angiotensin II and aldosterone. Angiotensin II andaldosterone are the components which are important in volume regulation.
Sympathetic activation. When volume is low, the sympathetic nervoussystem is activated. Sympathetic activation includes stimulation of nervesto target organs and release of the sympathetic hormones epinephrine, nore-pinephrine and dopamine.
ADH. ADH is a hormone produced in the posterior pituitary gland. Al-though its primary function is in the maintenance of plasma osmolality,ADH also has a secondary role in volume regulation.
Renin-angiotensin II-aldosterone and sympathetic activity are the pri-mary signals of volume regulation; these signals are activated together. ADHis only employed when volume is extremely low. If ADH is active, then re-nin-angiotensin II-aldosterone and sympathetic activation are already en-gaged.
There are three primary signals used to increase volume: ________stimulation, the renin-angiotensin II-aldosterone cascade and_______.
sympathetic
ADH
juxtaglomerularcomplex 1234
123412341234
aldosterone
angiotensin II
renin
adrenalgland
Renin-angiotensin II-aldosterone Sympathetic stimulation
ADH
��
��ADH

72
The Fluid, Electrolyte and Acid-Base Companion
Volume regulation�Signaling�The renin-angiotensin II-aldos-terone system is a series of enzymatic reactions.
The renin-angiotensin II-aldosterone system is a series of enzymatic re-actions that leads to the production and release of two hormones involved involume regulation: angiotensin II and aldosterone.
The pathway is initiated by the enzyme renin which is produced and storedin the juxtaglomerular cells of the afferent arterioles to the glomerulus. Asexpected, renin release is stimulated by conditions associated with low vol-ume such as low pressure in the afferent arteriole, decreased delivery ofsodium to the distal tubule and increased sympathetic activity.
Renin converts angiotensinogen, a protein produced by the liver, into an-giotensin I. Angiotensin I is then converted to angiotensin II by angiotensinconverting enzyme (ACE). ACE is contained primarily in the lung.
Angiotensin II is an extremely potent vasoconstrictor. It has a number ofeffects including the stimulation of the adrenal gland to release the hor-mone aldosterone.
________ is an enzyme which converts angiotensinogen to angio-tensin I.
Angiotensin converting enzyme is contained in the _____.
Renin
lung
angiotensinogen
angiotensin I
Angiotensin II
Aldosterone
RENIN
juxtaglomerularcomplex 1234
123412341234
ACE
lungs
liver
S. Faubel and J. Topf 4 Volume Regulation
73
Angiotensin converting enzyme (ACE) is one of the enzymes in therenin-angiotensin II-aldosterone system. ACE catalyzes the conversion ofangiotensin I into angiotensin II.
ACE levels are elevated in a number of disorders: hyperthyroidism,diabetes mellitus, sarcoidosis and other granulomatous diseases. Themechanism and clinical significance of the elevated levels is unknown.Clinically, ACE levels are only used to monitor the progression of sarcoi-dosis.
ACE is inhibited by a number of oral medications such as: captopril(Capoten®), enalapril (Vasotec®) and lisinopril (Prinivil®, Zestril®). Thesedrugs are commonly used to treat hypertension. The antihypertensiveeffect of ACE inhibitors is primarily due to a decrease in the formation ofangiotensin II which decreases vasoconstriction. The decreased blood pres-sure is not accompanied by increased heart rate which is a side effect ofother anti-hypertension medications. Control of blood pressure is enhancedby sodium restriction and diuretics.
ACE inhibitors are beneficial in patients with congestive heart failureand have been shown to improve survival in patients after myocardialinfarction.
ACE inhibitors also have a role in preserving and prolonging kidneyfunction in patients with diabetes mellitus and other diseases character-ized by glomerular hypertension and proteinuria.
One common and poorly-tolerated side effect of ACE inhibitors is achronic, nonproductive cough.
Ace Inhibitors? What's up with that?
captoprilDr.Spratt
MT Cup�Drugstore

74
The Fluid, Electrolyte and Acid-Base Companion
Volume regulation�Action at targets�Step three of volumeregulation is the action of signals at targets.
The targets of volume regulation are the kidney, heart and vasculature.Signals which act at the kidney affect either sodium or water resorption toincrease plasma volume. Angiotensin II, aldosterone and sympathetic ac-tivity all increase sodium resorption while ADH increases water resorption.
Signals which act at the heart and vasculature affect cardiac output andperipheral vascular resistance, respectively. Action at either of these tar-gets increases blood pressure. Sympathetic activity is the only signal whichacts at the heart to increase cardiac output. Angiotensin II and sympatheticactivity both affect the vasculature to increase total peripheral resistance.
____________ activation, angiotensin II and ___________ all causethe resorption of sodium.
_________________ increases total peripheral resistance.
Sympathetic;aldosterone
Angiotensin II
Na+
Na+
Na+
PLASMA VOLUME BLOOD PRESSURE
H2O
SODIUM RESORPTION WATER RESORPTION CARDIAC OUTPUT VASCULAR RESISTANCE
angiotensin IIaldosteronesympathetic activity
anti-diuretic hormonesympathetic activity angiotensin II
sympathetic activity
75
S. Faubel and J. Topf 4 Volume Regulation
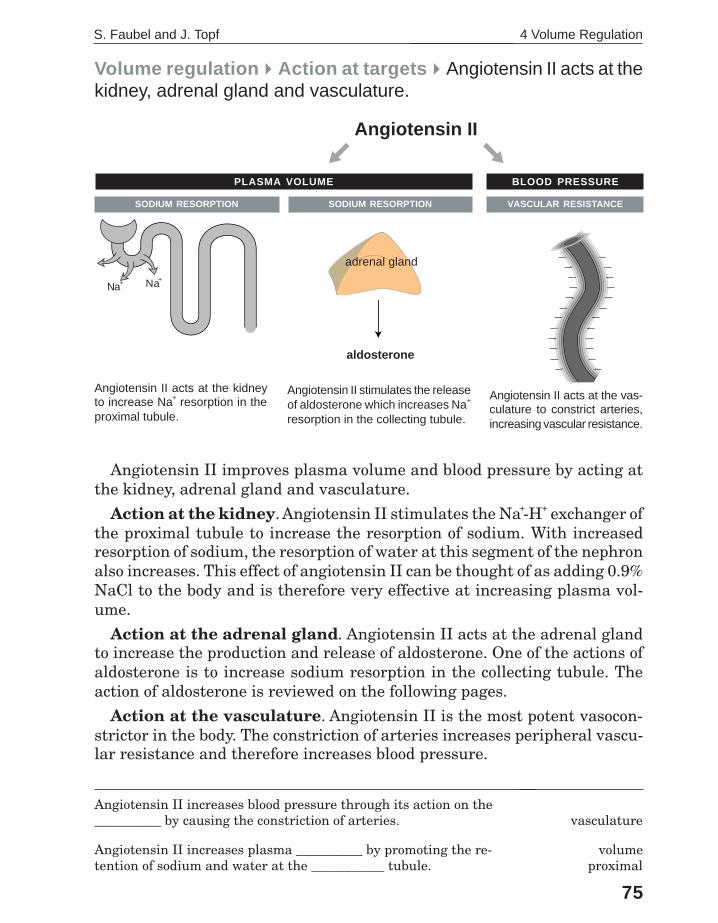
Volume regulation�Action at targets�Angiotensin II acts at thekidney, adrenal gland and vasculature.
Angiotensin II improves plasma volume and blood pressure by acting atthe kidney, adrenal gland and vasculature.
Action at the kidney. Angiotensin II stimulates the Na+-H+ exchanger ofthe proximal tubule to increase the resorption of sodium. With increasedresorption of sodium, the resorption of water at this segment of the nephronalso increases. This effect of angiotensin II can be thought of as adding 0.9%NaCl to the body and is therefore very effective at increasing plasma vol-ume.
Action at the adrenal gland. Angiotensin II acts at the adrenal glandto increase the production and release of aldosterone. One of the actions ofaldosterone is to increase sodium resorption in the collecting tubule. Theaction of aldosterone is reviewed on the following pages.
Action at the vasculature. Angiotensin II is the most potent vasocon-strictor in the body. The constriction of arteries increases peripheral vascu-lar resistance and therefore increases blood pressure.
Angiotensin II increases blood pressure through its action on the__________ by causing the constriction of arteries.
Angiotensin II increases plasma __________ by promoting the re-tention of sodium and water at the ___________ tubule.
aaavasculature
volumeproximal
Angiotensin II
Angiotensin II acts at the kidneyto increase Na+ resorption in theproximal tubule.
Angiotensin II acts at the vas-culature to constrict arteries,increasing vascular resistance.
aldosterone
adrenal gland
VASCULAR RESISTANCESODIUM RESORPTION
PLASMA VOLUME BLOOD PRESSURE
Angiotensin II stimulates the releaseof aldosterone which increases Na+
resorption in the collecting tubule.
SODIUM RESORPTION
Na+ Na+

76
The Fluid, Electrolyte and Acid-Base Companion
Aldosterone is a steroid hormone synthesized in the zona glomerulosa ofthe adrenal gland. It is the final hormone in the renin-angiotensin II-aldos-terone system. Aldosterone acts only at the kidney.
Action at the kidney. Aldosterone acts at the principle cells of the col-lecting tubule to increase the resorption of sodium. The effect of aldosteroneon sodium resorption is so powerful that it can reduce the urine sodiumconcentration to as low as 1 mEq/L. The urine sodium concentration is oneof the most reliable lab tests for evaluating volume; a urine sodium concen-tration less than 20 mEq/L is essentially diagnostic of effective volume deple-tion.
The following pages present an overview of the action of aldosterone.
___________ is the final hormone in the renin-angiotensin II -____________ cascade.
Aldosterone acts at the __________ nephron to cause the resorp-tion of ________, which increases plasma volume.
Aldosteronealdosterone
distalsodium
Volume regulation�����Action at targets�����Aldosterone acts at thekidney to increase sodium resorption.
An understanding of aldosterone action is important to understanding most of the disorderscovered in this book; these include hyponatremia (Chapter 6), hypernatremia (Chapter 8),type 4 RTA (Chapter 12) metabolic alkalosis (Chapter 14), hypokalemia (Chapter 18) andhyperkalemia (Chapter 19).
Aldosterone
Na+
Na+
adrenal gland
SODIUM RESORPTION
PLASMA VOLUME

77
S. Faubel and J. Topf 4 Volume Regulation
Aldosterone acts at the principle cell to:• increase Na+ resorption• increase Na-K-ATPase activity• increase the secretion of K+
Aldosterone acts at the intercalated cell to:• increase H+-ATPase activity• increase H+ secretion• increase HCO3
– resorption
Aldosterone acts at two types of cells in the collecting tubule, principleand intercalated. The action of aldosterone at the principle cell is importantin volume regulation as well as potassium balance; its action at the interca-lated cell is important in acid-base balance.
Principle cell. Aldosterone acts at the principle cell to cause the resorp-tion of sodium and the secretion of potassium. Aldosterone increases thenumber of sodium channels in the luminal membrane and increases theactivity of the Na-K-ATPase pumps in the basolateral membrane. The Na-K-ATPase pumps create a concentration gradient between the tubular lu-men and the principle cell which favors the movement of sodium into thecell (sodium resorption). As sodium resorption increases, the secretion ofpotassium increases in order to maintain electroneutrality. Therefore, al-dosterone affects both volume regulation and potassium regulation.
Intercalated cell. Aldosterone acts at the H+-ATPase pump of the inter-calated cell to increase the secretion of hydrogen ion into the tubule lumen.As hydrogen ion is secreted into the lumen, new bicarbonate is formed in-side the cell. This new bicarbonate is resorbed and added to plasma. Theaction of aldosterone here is important in acid-base balance. Increased al-dosterone activity results in metabolic alkalosis and decreased activity re-sults in metabolic acidosis (type 4 RTA).
Overview: Aldosterone acts at the principle and intercalated cellsof the collecting tubule.
Na+
K+
3 Na+ATP
AMP
2 K+
K+
principle celltubule lumen
OH
CO2
ATP
AMP
NEW!
HCO3
H+H+
intercalated celltubule lumen
__________ acts at the principle and intercalated cells of the collect-ing tubule.
Aldosterone

78
The Fluid, Electrolyte and Acid-Base Companion
Overview: There are two stimuli for the release of aldosterone.
The two primary stimuli for release of aldosterone are volume depletionand hyperkalemia.
Effective volume depletion. Decreased blood pressure detected bybaroreceptors initiates the renin-angiotensin II-aldosterone system.
Hyperkalemia. Aldosterone is the primary factor which regulates plasmapotassium concentration. Aldosterone increases the excretion of potassiumin the collecting tubule. An increase in the plasma potassium concentrationof 0.1 mEq/L is enough to stimulate the release of aldosterone.
Although aldosterone release is not affected by acid-base disorders, al-dosterone plays an important role in the generation and maintenance ofmany acid-base disorders.
F
E
Effective PerfusionHypoperfusion
HyperkalemiaEffective volume depletion
Aldosterone
angiotensin II
renin
adrenal gland
Aldosterone
There are ________ stimuli for the release of aldosterone.
Aldosterone release is stimulated by ______-volemia and_____-kalemia.
two
hypohyper

79
S. Faubel and J. Topf 4 Volume Regulation
Sympathetic activity increases plasma volume and blood pressure by af-fecting the kidney, the production of renin, the heart and the vasculature.
Action at the kidney. Increased sympathetic activity directly increasessodium resorption.
Action on renin production. Increased sympathetic activity stimulatesrenin release and initiates the renin-angiotensin II-aldosterone cascade.
Action at the heart. Increased sympathetic activity increases cardiacoutput by increasing heart rate and strength of contraction. As cardiac out-put increases, so does blood pressure.
Action at the vasculature. Increased sympathetic activity causes theconstriction of both arteries and veins. Constriction of arterial vessels in-creases total peripheral resistance and directly raises blood pressure. Con-striction of venous vessels increases blood return to the heart which boostsstroke volume, further supplementing cardiac output and blood pressure.
Sympathetic stimulation increases _________ rate and contractility.
Increased sympathetic activity occurs when effective circulating vol-ume is _____.
heart
aalow
Volume regulation�����Action at targets�����Sympathetic activityincreases plasma volume and blood pressure.
VASCULAR RESISTANCESODIUM RESORPTION
PLASMA VOLUME BLOOD PRESSURE
• increased heart rate• increased contractility
• constriction of arteries• constriction of veins
aldosterone
angiotensin II
• renin stimulation
Sympathetic activity
• Na+ resorption
CARDIAC OUTPUTSODIUM RESORPTION
CO = HR x SV
renin
Na+ Na+

80
The Fluid, Electrolyte and Acid-Base Companion
The final signal which is released in response to hypovolemia is antidi-uretic hormone. ADH acts at the collecting ducts of the distal nephron toincrease the resorption of water.
ADH release should be thought of as a secondary defense in the fightagainst volume depletion. ADH is only released when a substantial (10-15mmHg) fall in blood pressure occurs. Although it is an emergency defense,ADH is not a very effective defense against hypovolemia. Because waterdistributes among all three body water compartments, water resorption atthe collecting tubules causes only a minimal rise in plasma volume. Theprimary function of ADH is the regulation of plasma osmolality. The detailsof the actions and effects of ADH are reviewed in the next chapter, Osmo-regulation.
Renin-angiotensin II-aldosterone and sympathetic activity are the pri-mary defenses against volume depletion. If ADH is released, renin-angio-tensin II-aldosterone and sympathetic activity are already employed.
ADH is reviewed in more detail in the ________ chapter.
The name of the next chapter is _______________.
Volume regulation�����Action at targets�����ADH acts at the kidneyto cause the resorption of water.
H2O
H2O
H2O
ADH��
��
WATER RESORPTION
PLASMA VOLUME
next
Osmoregulation

81
S. Faubel and J. Topf 4 Volume Regulation
Atrial natriuretic peptide (ANP) is the only volume regulatory hormonewhich acts to decrease volume. ANP is a peptide hormone secreted by theheart in response to volume overload as detected by stretch receptors in theatria. ANP increases the excretion of sodium from the kidney by blockingthe sodium resorption in the distal nephron. It also increases glomerularfiltration rate (GFR).
The physiologic significance of ANP is uncertain. Although congestive heartfailure is associated with volume overload and elevated levels of ANP, thekidney still excretes minimal amounts of sodium. This contradiction is ex-plained by the theory that ANP activity requires a normal blood pressure.Since CHF is typically associated with a lower than normal blood pressure,the effect of ANP is blocked.
ANP
Volume regulation�ANP�Atrial natriuretic peptide is the onlyvolume regulatory hormone that decreases effective volume.
Na+
Na+
The clinical role of ____ in volume regulation is unclear.
_____ increases the excretion of sodium by the kidney.
ANP
ANP

The Fluid, Electrolyte and Acid-Base Companion
82
The volume status of a patient that is apparent from the clinical as-sessment (e.g., physical exam, lab tests) is clinical volume status. It isdivided into three categories: hypovolemia, euvolemia and hypervolemiawhich refer to a low, normal and high volume status, respectively.
Effective volume depletion is associated with both hypovolemia andhypervolemia. Understanding the difference between the two requiresremembering that effective circulating volume consists of two compo-nents, plasma volume and blood pressure. Clinical hypovolemia is dueto the loss of plasma volume, while clinical hypervolemia is due to inad-equate blood pressure.
Loss of plasma volume causing hypovolemia and effective circulatingvolume depletion is due to disorders associated with fluid loss such asvomiting, diarrhea and blood loss. Hypovolemia is characterized by drymucus membranes, tachycardia and orthostatic vital signs.
Hypervolemia is characterized primarily by peripheral edema and isassociated with CHF and liver disease. In these disorders, peripheraledema is a result of effective circulating volume depletion from inad-equate blood pressure (peripheral edema is explained further on thefollowing pages). In CHF, inadequate blood pressure is due to inad-equate cardiac output (BP= CO x PVR); in liver disease, inadequateblood pressure is due to low peripheral vascular resistance.
In both hypovolemia and hypervolemia, inadequate effective circu-lating volume stimulates renin-angiotensin II-aldosterone, sympatheticactivity and, if severe, ADH release.
Clinical correlation: Low effective circulating volume can beassociated with either clinical hypovolemia or hypervolemia.
Assessing volume status is important in the evaluation of many disorders (e.g., hy-ponatremia, hypernatremia, metabolic alkalosis). A thorough list of history, physicalexam findings and lab tests that can help identify hypovolemia and hypervolemia is inChapter 7, page 147. For the remainder of the book, hypovolemia, euvolemia andhypervolemia will refer to clinical hypo-, eu- and hypervolemia, respectively.
HypovolemiaLow effectivecirculating volume
HypervolemiaLow effectivecirculating volume

S. Faubel and J. Topf 4 Volume Regulation
83
Clinical correlation: Peripheral edema is maintained by so-dium retention.
Peripheral edema is the swelling and/or pitting of the skin due to anincrease in the volume of the interstitial compartment. Knowledge of bothStarling’s law (Chapter 3) and volume regulation is required to fully un-derstand this common clinical entity. An alteration in Starling’s law ini-tiates edema formation but activation of the volume regulatory system isrequired for clinically significant edema to persist.
Peripheral edema begins when there is an increase in the movement ofwater from the plasma into the interstitium. As revealed by Starling’s law,three factors govern the movement of fluid between the plasma and inter-stitial compartments: membrane permeability, hydrostatic pressure andosmotic pressure. In addition, since interstitial fluid is normally removedby the lymphatic system, lymphatic obstruction (e.g., infiltrating tumor)can also cause peripheral edema.
Approximately three liters of fluid must move from the plasma into theinterstitium to generate clinically significant edema. This is approximatelyequal to the volume of the entire plasma compartment. To replace this lossof fluid from the plasma compartment, the volume regulatory mechanismmust be engaged. Sodium retention initiated by the renin-angiotensin-aldosterone system and sympathetic activity maintains peripheral edemaby replacing the plasma fluid lost into the interstitium.
increased capillarymembrane permeability
increased plasmahydrostatic pressure
Na+
Na+
Na+
Generation of peripheral edemaA change in one of the factors of Starling’s law fa-vors the movement of water from the plasma intothe interstitial compartment.
Maintenance of peripheral edemaThe renal resorption of sodium serves to in-crease plasma volume as it is lost into theinterstitial compartment.
decreased plasmaosmotic pressure
angiotensin IIsympathetic activity
aldosterone

The Fluid, Electrolyte and Acid-Base Companion
84
Clinical correlation: Peripheral edema formation in CHF is avicious cycle.
The peripheral edema associated with CHF is due to the retention ofsodium stimulated by low effective circulating volume. As previously dis-cussed, low effective circulating volume in CHF is due to inadequateblood pressure with adequate plasma volume.
Continued sodium retention in CHF causes the plasma volume torise above normal which increases hydrostatic pressure. In the venoussystem, increased hydrostatic pressure is transmitted to the capillar-ies, favoring the movement of plasma fluid into the interstitium to causeedema. Sodium retention continues and replaces the plasma fluid thatleaks into the interstitium.
This cycle of sodium retention, increased hydrostatic pressure andleakage of fluid in the interstitium can result in the accumulation of alarge amount of fluid in the interstitial compartment.
Because it takes up to 3 liters for edema to be detectable, it is important to considera patient's weight. One liter of water weighs 1 kg or 2.2 pounds. Thus, a patient withdecompensating CHF may gain 6.6 pounds before edema is detectable. At home, aswell as in the hospital, it is important for patients with disorders predisposing to edemato have their weights measured daily.
Increased plasmahydrostatic pressure
reninangiotensin IIaldosteronesympathetic
activityC.O.
Sodium retention
Peripheraledema
Low cardiac output triggers the releaseof the volume regulation hormones.
Before heart failure, thevolume status is normal.
If effective circulatingvolume is not restored,
the cycle continues.
S. Faubel and J. Topf 4 Volume Regulation
85
renin�angiotensin II�aldosterone�sympathetic �
activity
C.O.
ACE inhibitors
spironolactone
beta-blockers
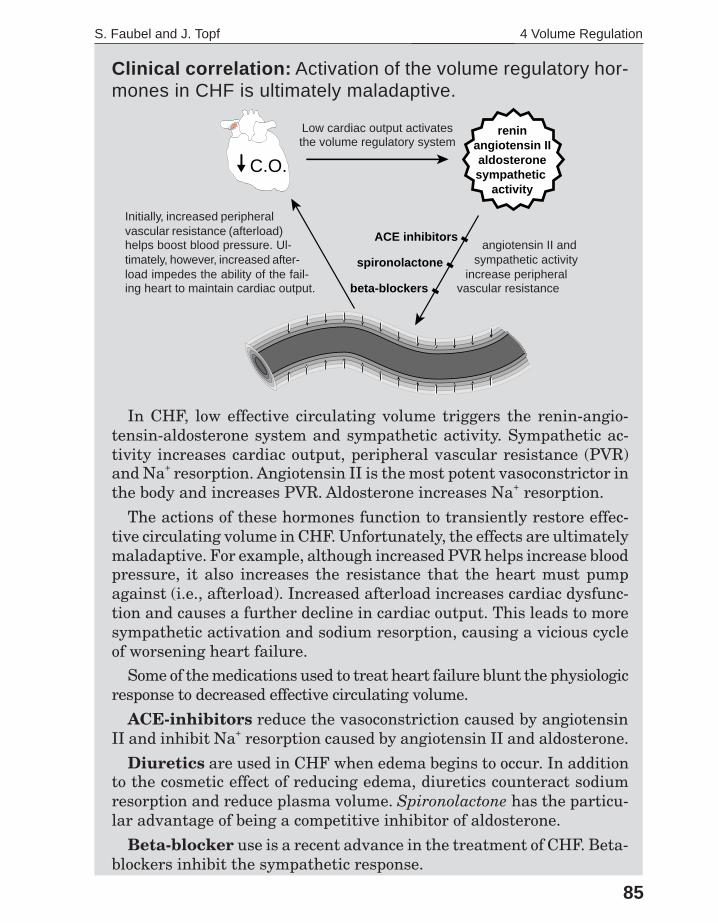
In CHF, low effective circulating volume triggers the renin-angio-tensin-aldosterone system and sympathetic activity. Sympathetic ac-tivity increases cardiac output, peripheral vascular resistance (PVR)and Na+ resorption. Angiotensin II is the most potent vasoconstrictor inthe body and increases PVR. Aldosterone increases Na+ resorption.
The actions of these hormones function to transiently restore effec-tive circulating volume in CHF. Unfortunately, the effects are ultimatelymaladaptive. For example, although increased PVR helps increase bloodpressure, it also increases the resistance that the heart must pumpagainst (i.e., afterload). Increased afterload increases cardiac dysfunc-tion and causes a further decline in cardiac output. This leads to moresympathetic activation and sodium resorption, causing a vicious cycleof worsening heart failure.
Some of the medications used to treat heart failure blunt the physiologicresponse to decreased effective circulating volume.
ACE-inhibitors reduce the vasoconstriction caused by angiotensinII and inhibit Na+ resorption caused by angiotensin II and aldosterone.
Diuretics are used in CHF when edema begins to occur. In additionto the cosmetic effect of reducing edema, diuretics counteract sodiumresorption and reduce plasma volume. Spironolactone has the particu-lar advantage of being a competitive inhibitor of aldosterone.
Beta-blocker use is a recent advance in the treatment of CHF. Beta-blockers inhibit the sympathetic response.
Clinical correlation: Activation of the volume regulatory hor-mones in CHF is ultimately maladaptive.
Low cardiac output activatesthe volume regulatory system
Initially, increased peripheralvascular resistance (afterload)helps boost blood pressure. Ul-timately, however, increased after-load impedes the ability of the fail-ing heart to maintain cardiac output.
angiotensin II andsympathetic activity
increase peripheralvascular resistance

86
The Fluid, Electrolyte and Acid-Base Companion
Summary�����Volume regulation.Volume regulation is the simultaneous adjustment of plasma volume and
blood pressure in order to maintain adequate perfusion of tissues.
Plasma volume is affected by signals which influence sodium and waterresorption. Blood pressure (CO × PVR) is affected by signals which influ-ence cardiac output and peripheral vascular resistance. Volume regulationoccurs in three steps:
Baroreceptors, the monitors of volume status, respond to changes in bloodpressure. Even though low blood pressure can be associated with low, nor-mal or high plasma volume, low blood pressure always triggers the releaseof signals which increase blood pressure and plasma volume.
The primary signals which regulate effective circulating volume are: re-nin-angiotensin II-aldosterone, sympathetic activity and ADH. These sig-nals act at the kidney, heart and vasculature. Action at the kidney increasesplasma volume through the resorption of sodium and water while action atthe heart and vasculature increases blood pressure.
Renin-angiotensin II-aldosterone and sympathetic activity are the pri-mary signals involved in volume regulation. If effective volume is very low,ADH is also released as a secondary defense. ADH acts at the collectingtubules of the distal nephron to increase the resorption of water.
3L
2L
1L
plasma volume
andvolume(effective circulating volume)
blood pressure
Monitoringbaroreceptors
ADH
Signalingthree types of signals
sympatheticactivation
aldosterone
angiotensin II
renin
Action at targetsplasma volume blood pressure
Na+
Na+
H2O
H2O


















