04 Neurologic
96
Central Nervous System Infections
description
tianjin medical university
Transcript of 04 Neurologic

Central Nervous System InfectionsCentral Nervous
System Infections

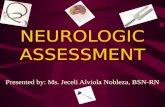
Cerebrum Frontal lobe
Parietal lobe
Temporal lobe
Occipital lobe
Cerebellum
Brain Stem

Pia mater, Arachnoid, Dura mater
Subdural space, Subarachnoid space

The meninges of the spine cord is the continuation of the meninges of the brain

Acute Bacterial Meningitis
Viral Meningoencephalitis
General Introduction

1. Acute infection of the central nervous system(CNS) is the most common cause of fever associated with signs and symptoms of CNS disease in children
2. The specific pathogen is influenced by the age and immune status of the host and the epidemiology of the pathogen.
Viruses, bacteria, fungi, parasites, rickettsiae, mycoplasma
General Introduction

3. Regardless of etiology, most patients with acute CNS infection have similar clinical syndromes.
Common symptoms and signs:
fever, headache, vomiting, photophobia, restlessness, irritability, stupor, coma, seizures
neck pain and rigidity, positive Kernig’s and Brudzinski’s signs, and focal neurologic deficits.
The severity and constellation of signs are determined by the specific pathogen, the host, and the anatomic distribution of the infection

4. The anatomic distribution of infection may be diffuse or focal
Meningitis: primary involvement of meninges
Encephalitis: brain parenchymal involvement
Meningoencephalitis: involvement of both
Diffuse
FocalBrain abscess: The neurologic expression of this infection is determined by the site and extent of the abscess(es)

5. The diagnosis of diffuse CNS infections depends on careful examination of cerebrospinal fluid(CSF) obtained by lumbar puncture(LP).
Production, circulation and function of CSF: Produced by the choroid plexus in the cerebral ventricles
Circulates in the subarachnoid space surrounding the spinal cord and brain, protect them from injury

Acute Bacterial Meningitis
Most common CNS infection in children
One of the most potentially serious infections associated with a high rate of acute complications and risk of chronic morbidity
Prompt and reasonable treatment may improve the prognosis largely

Etiology
Pathogenesis
Pathology
Clinical manifestations
Laboratory examinations
Diagnosis
Complications
Treatment
Differential diagnosis
Epidemiolgy
Purulent meningitisPurulent meningitis
Acute Bacterial
Meningitis

Most common causes : Neisseria meningitidis Streptococcus pneumoniae Haemophilus influenzae Less common pathogens: P.aeruginosa, S.aureus,
S.epidermidis, Salmonella, and L.monocytogenesIndividuals with alterations of host defense due t
o anatomic defects or immune deficits Varies by age:
Etiology

Neisseria meningitidis

Streptococcus pneumoniae

Haemophilus influenzae

Commonest Meningitis-Causing Bacteria according to Patient Age
Age Common bacteria causing meningitis
Birth to two month of age Group B
streptococcus,gram-negative enteric bacilli,Listeria monocytogenes
2 months to 12 years H. influenzae, S.pneumoniae, N. meningitidis
over 12 years N. meningitidis, S. pneumoniae

Epidemiology
Meningitis can occur at any age, but the risk is greatest among infants between 1 and 12 mo of age; 95% of cases occur between 1 mo and 5 yr of age
The lack of immunity to specific pathogens associated with young age.
The mode of transmission is probably person to person contact through respiratory tract secretions or droplets.
The predisposing season is the winter or spring

1. Bacteria reach the subarachnoid space a. By hematogenous route(bacteremia) from a dis
tant site of infection (nasopharynx) b. By invasion directly from a contiguous focus o
f infection( paranasal sinusitis, otitis media, mastoiditis, orbital cellulitis, dermal sinus tracts, cranial or vertebral osteomyelitis, penetrating cranial trauma, or meningomyeloceles)
2. Bacteria cause inflammatory responses in CSF.
Pathogenesis

Bacteria reach the subarachnoid space Bacteria reach the subarachnoid space by hematogenous routeby hematogenous route
Colonization of bacteria on nasophyrnx by pili Bacteria locally invade tissue and gain access to
the bloodstream Bacterial virulence factors (outer polysaccharid
e capsule) overcome host defense mechanisms (opsonophagocytosis)
Bacteria survive and replicate in the blood stream
Bacteria cross the blood-brain barrier and invade the subarachnoid space

Large occipital encephalocele Small encephalocele high in the occipital region
Posterior parietal encephalocele Lumbar myelomenigocele

Inflammatory responses in CSF caInflammatory responses in CSF caused by baterial invasionused by baterial invasion
Bacterial replication and accumulation of WBCs
Production and release of inflammatory mediators: cytokine, interleukins, TNF, prostaglandins, leukotrienes
Vasculitis (increased capillary permeability, obstruction of blood flow),
Damage to CSF circulation system.

Meningeal exudatesCerebral edemaCerebral vascular inflammatory changesDamage to the cerebral cortex(vasculitis, bacterial i
nvasion, toxic encephalopathy, raised ICP)
Subdural effusionHydrocephalus(communicating, obstructive)Changes of protein and glucose levels in CSF
Pathology
•Raised CSF protein levels, Hypoglycorrhachia



Cerebral edemaCerebral edema
Mechanism:1.cytotoxic cerebral edema(cell death)2.vasogenic cerebral edema(increased permeability)3.interstitial cerebral edema(increased hydrostatic pressure)
4.ISADH(inappropriate secretion of anti-diuretic)
Cerebral edema
Increased intracranial pressure(ICP)
Brain herniation

Frontal subdural effusions









Raised CSF protein levels:
increased vascular permeability of the blood-brain barrier
Hypoglycorrhachia(reduced CSF glucose levels) :
decreased glucose transport by the inflamed meninges and
increased glucose utilization by the inflamed cerebral tissue and bacteria which may produce a local lactic acidosis.

1. Mode of onset
2. Symptoms and signs: Systemic Neurologic Features of neonatal meningitis
Clinical Manifestations

Mode of onsetSudden onset (fulminant type) Most common in meningococcal sepsis with meningitis Rapidly progressive manifestations of shock, purpura,
DIC (disseminated intravascular coagulation), and reduced levels of consciousness, it may evolve to death within 24 hr
Subacute onset Most common in H. Influenzae type b and pneumococ
cal meningitis Often preceded by several days of upper respiratory t
ract or gastrointestinal symptoms


Systemic symptomsSystemic symptoms
Fever 90%Headache 90%PhotophobiaLethargyAnorexia, nausea, vomitingMyalgia, arthralgiaShock, rash, petechiae or purpura, DICTache Cerebrale - stroke skin with a blunt inst
rument -> 30-60 sec ->raised red rash

Neurologic manifestationNeurologic manifestation
Signs of meningeal irritation(50%) neck stiffness(nuchal rigidity) Brudzinski’s sign Kernig’ signIncreased ICPGeneralized or focal seizures(30%)Cranial nerve palsies and focal cerebral signs(hemi
paresis, quadriparesis) (10-20%) Papilledema (1%)

DefinitionsDefinitions Nuchal rigidity Passive or active flexion of the neck will usually result i
n an inability to touch the chin to the chest Brudzinski’s sign The Brudzinski sign refers to spontaneous flexion of the
hips during attempted passive flexion of the neck Kernig’ sign The Kernig sign refers to the inability or reluctance to
allow full extension of the knee when the hip is flexed 90 degrees



Symptoms and signs of increased ICP
Headache Emesis(projectile vomiting) progressive decreased consciousness, may become co
ma,seizures Bulging fontanel or diastasis(widening) of the suture
s In severe cases, the respiratory and circulatory funct
ions may be damaged (a combination of hypertension and bradycardia with apnea or hyperventilation), even coma or herniation (anisocoria, respiratory and cardic arrest) occurs.




Normal papilla of optic nerve Papilledema

Clinical features of neonatal meningitis
Symptoms and signs at onset can be variable and quite nonspecific(Apnea and bradycardia, cyanosis, diarrhea, disinterest in feeding, jaundice, lethargy, respiratory distress, temperature instability (hypothermia or fever), vomiting ,high-pitched crying)
The maneuvers to test meningeal irritation are often not available .And the symptoms and signs of increased ICP are less common .
High index of suspicion:• Fever (50%) • Seizure (40%) • Bulging fontanelle (33%) • Irritable +/- change in consciousness & poor muscle tone (33
%)

Subdural effusions and empyemaISADH with hyponatremiaVentriculitis and ependymitis With bacteria and inflammatory cells in ventricular
fluidHydrocephalus Others: Neurological deficits( deaf, blindness, epilepsy or
mental retardation,etc)
Complications

Subdural effusions and empyemaSubdural effusions and empyema Accumulation of excess fluid or pus in the subdural
space Develop 30%; 85%-90% asymptomatic Most common under 12 mo and H. Influenzae ty
pe b meningitis. Clinical features: Diagnosis of subdural effusion:
History and associated symptoms and signs Transillumination test CT scan Subdural aspirate Diagnostic

Clinical features of Clinical features of of subdural effusion
Fever is persistent or reappears several days after the patient has become afebrile during the therapy for bacterial meningitis.
Progressive bulging fontanel, diastasis of sutures, enlarging head circumference , emesis ,seizures and abnormal consciousness develop during the course of bacterial meningitis


ISADH with hyponatremia
Inflammatory changes in the hypothalamus and pituitary
30-50% of cases of meningitis
Exacerbate cerebral edema
Produce hyponatremic seizures.
hyponatremia reduced serum osmolarity

Hydrocephalus
Communicating
adhesive thickening of the arachnoid villi lack of absoption of CSF
Obstructive
fibrosis and gliosis of the narrow outlets of the cerebral ventricular system after Ventriculitis and ependymitis an obstruction to flow of CSF

1. CSF Analysis Can be diagnostic, and every patient with
meningitis should have CSF obtained by lumbar puncture(LP)unless the procedure is contraindicated
Features of normal CSF
Typical CSF features of bacterial meningitis:
2. Other investigations
Laboratory Findings


Changes in the appearance, composition or the pressure of the CSF indicates diseases of CNS First drop appearance First tube culture Second biochemistry test Third tube cell count, Gram stain
Skin
subcutaneous tissue
yellow ligament(first feel of reduced resistance suddenly)
dural mater and arachnoid(second feel)

Indication of LP: LP should be performed when diffuse infection of CNS is suspected
Contraindications for an immediate LP :
cardiorespiratory compromise increased intracranial pressure (ICP) infection in the area of needle insertion bleeding diathesis (low platelet, hemophilia,DIC)

Features of normal CSF: A clear colourless fluid,
contains little protein(<40mg/dl),
glucose(2.8~4.4mmol/L or 50~80mg/dl) and
some other components (chlorides:118~128mmol/L),
and few cells(0-8/mm3 in infants and 0-5/mm3 in adults, 0-30 mm3 in neonates; lymphocytic or monocytic predominance)
Pressure of CSF is 25-70mmH2O in infants, 65-195mmH2O in adults

Typical CSF features of bacterial meningitis:
Appearance: cloudy (turbid), puric
Pressure: >200-300mmH2O
Cells: pleocytosis 1000- 10,000 WBC/mm3
Neutrophilic predominance 75-95%
Protein: Elevated protein concentration (100-1000mg/dL)
Glucose: Hypoglycorrhachia(<1.1mmol/L)
Glucose level Ratio of CSF to serum<0.4
(Continued)

Gram stain
Bacterial cultrueDefine the specific pathogen
Special test for CSF:
Countercurrent immunoelectroporesis Latex particle agglutination antigens
Determination of CSF C-reactive
protein and tumor necrosis factor levels

Other investigations:
Peripheral WBC: leukocytosis(20000-40000/mm3), neutrophilic predominant( >80%) But in very severe cases, WBC may be low.
Blood culture:
Culture and staining of petechial lesions:
meningcoccal meningitis.
Head CT scan: brain abscesses subdural effusions or empyemas ventriculitis hydrocephalus

reviewreview
Most common causes for acute bacterial meningitis
Complications of acute bacterial meningitis
Typical CSF features of acute bacterial meningitis

History taking suspected symptoms and signsLP CSF analysis confirm the diagnosis:Head CT scan confirms the
complications
Diagnosis

Typical CSF features confirming the diagnosis of bacterial meningitis :
Turbid appearance Increased pressure Neutrophilic pleocytosis Elevated protein Reduced glucose content Microorganisms on Gram stain and culture
Conditions in which CSF analysis shows normal or atypical:
Severe overwhelming sepsis and meningitis
The early stage (bacteremia stage) Partial and short-term antibiotic treatment

Pyogenic meningitis must be distinguished from meningitis caused by other microorganisms ( viral, tuberculous and fungal) This differentiation is mainly dependent on a careful examination of CSF .
Differential Diagnosis

Pleocytosis
protein glucose stain culturenumber predominance
Bacterial neutrophils Gram
+
bacterial
+
Tuberculous lymphocytes * Acid-fast+
M.tuber-culosis+
Viral lymphocytes normal – Viral
+
Fungal ~ lymphocytes Ink+ Fungal
+
*: Concurrently decreased glucose and chloride in CSF is a hallmark of TB-M
CSF features in various infectious meningitis

Antibiotic therapySupportive careSymptomatic treatmentDexamethasone treatmentTreatment of complications
Treatment

Antibiotic therapyAntibiotic therapy
Principles
Initial(Empiric) therapy without defining the etiologic agent:
Subsequent antibiotic therapy after defining the etiologic agent

Principles of antibiotic therapyPrinciples of antibiotic therapy
Early, intravenouslyAdministered immediately after LP in the absence
of increased ICPAdministered immediately before LP in the
presence of increased ICP which should be treated simultaneously.
Highly lipid soluble to cross the inflamed blood -brain barrier and achieve bactericidal levels in the CSF and, if given in combination, should not be antagonistic

Initial(Empiric) therapy without defining the etiologic agent:
Ampicillin (300mg/kg.d) and Chloramphenicol(100mg/kg.d)( less recommended)
Ampicillin and penicillin(400,000~800,000u/kg.d)
Third or fourth-generation cephalosprin: Cefotaxime(200mg/kg.d), Ceftriaxone(10
0mg/kg.d)The treatment course: at least 10~14d.

Subsequent antibiotic therapy after defining the etiologic agentThe choice of antibiotics should be based on the r
esults of the bacterial susceptibility test.
H.influenza : ampicillin, cephalosprin(2~3w) S. Pneumoniae: penicillin-G, cephalosprin(2~3w) Meningococcus : penicillin-G(7~10d) Gram-negative bacteria : aminoglycosides, cephalos
porins S.aureus: nafcillin, aminoglycosides, cephlosporins,
vancomycin

Supportive care
Reapted medical and neurological assessments pulse rate, blood pressure, and respiratory rate pupillary reflexes, level of consciousness, motor strengt
h, cranial nerve signs and evaluation for seizures important laboratory studies : BUN, serum sodium,
chloride possium, and bicarbonate levels, urine output and specific gravity, complete blood and platelet counts, and coagulation factors in the presence of petechiae, purpura, or abnormal bleeding.
Maintenance of the fluid and electrolyte balance

Symptomatic treatment Control high fever Control infectious shock Control increased ICP to prevent herniation 20% Mannitol(0.5-1g/kg/dose) furosemide(1mg/kg)
controlled ventilation to keep PCO2 30~35mmHg
Control seizures
Intravenous diazepam(0.1-0.2mg/kg/dose) or lorazepam(0.05mg/kg/dose), phenytoin or phenobarbital(15-20mg/kg loading dose, 5mg/kg/24hr maintenance)for further control.
Specific therpay for hypoglycemia, hypocalcemia, or hyponatremia

Dexamethasone treatment
Limit the overproduction of inflammatory mediators and may have a beneficial effect on the outcome of bacterial meningitis
Intravenous dexamethasone(0.15mg/kg/dose, given every 6 hr for 4 days) is suggested to be given at the same time as antibiotics

Treatment of complications
Aspiration for subdural effusion, drainage for vasculitis and ependymitis
fluid restriction and supplement of sodium for hyponatremia due to ISADH
Surgical shunt for hydrocephalus

Neurodevelopmental sequelae(20%) include hearing deficit, seizures, language disorder, mental retardation, motor abnormalities, visual impairment, behavior disorders learning disorders, attention deficits, etc.
Hearing loss is the most common. All children should undergo hearing evaluation after meningitis
Prognosis

Viral Meningoencephalitis
Relatively common
An acute inflammatory process involving the meninges and brain tissue
Caused by a number of different viral agents
Most cases are mild and self-limited, but in severe and progressive cases death or severe sequence may occur.

Etiology
Enteroviruses 80%
Arboviruses
Herpesviruses An important cause of severe encephalitis with a high mortality and severe sequence.
Mumps

Pathology
Meningeal congestion,
Mononuclear (lymphocytic) infiltration
Vascular and perivascular inflammatory changes
Demyelination and damaged neurons.
The involvement of brain tissues, spinal cord, nerve roots, and peripheral nerves is quite variable the clinical neurologic presentations are often variable.

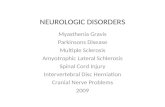
Synapse
Dendrites
Axon(with myelin)
Soma
The structure of a neuron

Pathogenesis
Virus lymphatic system(first multiplication) bloodstream (extraneural phase, systemic symptoms) CNS(secondary multiplication, neurologic disease)
Neurologic damage is caused by:
A direct invasion and destruction of neural tissues by actively multiplying viruses Neuronal destruction
A reaction of the patient’s nervous tissue to antigens of the virus. Demyelination and vascular and perivascular destruction.



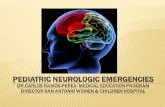
Normal conduction along a myelinated axon
Effects of demyelination on impulse conduction

Clinical Manifestations
A wide range of severity, several patterns of onset:
Non-specific initial manifestations :fever, headache, nasopharyngitis, abdominal pain, nausea and vomiting, or in infants, screaming spells
Mildly affected initially, only to lapse into coma and die suddenly.
Ushered in by high fever, violent convulsions, bizarre movement, and hallucinations
Signs of meningeal irritation, increased ICP, local neurologic signs
Specific forms: acute transverse myelitis, Guillain-Barre syndrome, acute hemiplegia , and acute cerebellar ataxia.

Laboratory Findings
1. Analysis of CSF: Pressure: normal~ elevated.
Appearance: generally clear
Leukocyte count: none~ several hundred/mm3, mononuclear or lymphocytic predominance(but during the first 8-12 hr of the onset may be polymorphonuclear predominance).
Protein concentration: normal~ slightly elevated( but may be very high if brain destruction is extensive HSV encephalitis.
Glucose level: usually normal(but may be depressed in mumps infection
Gram stain or bacterial culture: no bacteria recovered.

2. Virological examinations
3. Electroencephalogram(EEG):
typically shows diffuse slow wave activity
4. Neuroimaging studies(CT or MRI):
may show swelling of the brain parenchyma or focal lesions.

Diagnosis
1. Clinical manifestations
2. Features of CSF
3. Virological findings
4. EEG
5. CT or MRI appearance

Differential Diagnosis
which sometimes present acute onset, and has the similar CSF changes to that in viral meningoencephalitis. Cytological examination of CSF and neurological roentgenogram should be done.
1. Partial treated pyogenic meningitis The special antigen identification and gram stain of CSF may help the diagnose.
2. Other nonbacterial CNS infections Fungi, rickettsiae, Mycoplasma, protozoa and other parasites
3. Primary or secondary brain tumor,or brain abscess

Treatment
1.Antiviral agents: Acyclovir for herpes simplexGancrclovir for CMV, EBVVirazole(ribavirin), interferon
2. Antibiotics:When bacterial cause cannot be excluded definitely.
3. General treament:Controlling fever, reducing intracranial pressure, maintenance of fluid and electrolyte balance, improving the cadiopulmonary function,etc.Supportive and rehabilitative efforts are very important after the patient recovers.

Prognosis
Depends on the severity of clinical illness, the specific cause, and the age of the child.
Most patients completely recover
Various, degree of neurologic sequence may be left in some cases( especially in those with infection caused by Herpes simplex virus


questionsquestions
Causative organism of acute bacterial meningitis
Clinical manifestations of acute bacterial meningitis (definition)
Complications of acute bacterial meningitis
Analysis of cerebral spinal fluid(CSF findings in several infectious meningitis)

questionsquestions
Principals of antimicrobial therapy for acute bacterial meningitis