Imsg2018.weebly.com/uploads/1/6/1/0/16101502/muhtasibgiembryo.pdf · The epithelia that form the...
32
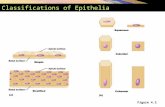
... EPITHELIAL TISSUE 79 Epithelium Proliferation of cells and their downgrowth into the subjacent connective tissue. ···· ... -·• ....... . Basal lamina ( ( I Exocrine gland Cords of cells Follicular endocrine '"Tioo Imming endrlne gland gland !ratloo Disappearance of duct cells Figure 4-21. Formation of glands from covering epithelia. Epithelial cells proliferate and penetrate the. connective tissue. They ma:t.::::;or ma,r not-maintajp contact with the surfac.e. When contact IS mamtained, exocrine glands are formed; without contact, endocrine qlands are formed. The cells of endocrine glands can be arranged in cords or in follicles. Tfie lumen of the follicles accumulates secretion; cells of the cora'S ,......._ II store only small quantities Ofsecretions in their cytoplasm. (Redrawn and reproduced, with permission, from Ham AW: Histology, 6th ed. Lippincott, 1969.) Types of Glandular Epithelia The epithelia that form the glands of the body can be classified according to various criteria. Unicellular glands consist of iso- lated glandular cells, and multicellular glands are composed of clusters of cells. An example of a unicellular gland is the goblet cell of the lining of the small intestine (Figure 4-20) or of the respiratory tract. The term "gland," however, is usually used to designate large, complex aggregates of glandular epithelial cells, such as in the salivary glands and the pancreas. Glands arise during fetal life from covering epithelia by means of proliferation and invasion of the epithelial cells into the subjacent connective tissue, followed by further differentiation (Figure 4-21). Exocrine (Gr. exo, outside, + krinein, to separate) glands retain their connection with the surface epithelium from which they originated. This connection is transformed into tubu- lar ducts lined with epithelial cells through which the glandular secretions pass to reach the surface. Endocrine (Gr. enclon, within, + krinein) glands are glands whose connection with the surface is lost during development. These glands· are therefore ducrless, and their secretions are picked up and transported to their site of action by the bloodstream rather than by a duct system. Two types of endocrine glands can be recognized based on the arrangement of their cells. The endocrine cells may form anasto- mosing cords interspersed berween dilated blood capillaries (eg, ad- renal gland, parathyroid, anterior lobe of the pimitary; Figure 4-21)
Transcript of Imsg2018.weebly.com/uploads/1/6/1/0/16101502/muhtasibgiembryo.pdf · The epithelia that form the...

~~v-tliO~""~Y\\ ~ ~ ... ~~~~ ~-----------------------=~~~~~~~==--
EPITHELIAL TISSUE 79
Epithelium Proliferation of cells and their downgrowth into the subjacent connective tissue.
···· ... -·• ....... . Basal lamina
--~--···].: ( ( I
Exocrine gland Cords of cells Follicular endocrine '"Tioo Imming endrlne gland gland !ratloo
·::-::.~~.:';":~:: :~:.t:~;;::~::_-Disappearance of duct cells
Figure 4-21. Formation of glands from covering epithelia. Epithelial cells proliferate and penetrate the. connective tissue. They ma:t.::::;or ma,r not-maintajp contact with the surfac.e. When contact IS mamtained, exocrine glands are formed; without contact, endocrine qlands are formed. The cells of endocrine glands can be arranged in cords or in follicles. Tfie lumen of the follicles accumulates secretion; cells of the cora'S ,......._ II
store only small quantities Ofsecretions in their cytoplasm. (Redrawn and reproduced, with permission, from Ham AW: Histology, 6th ed. Lippincott, 1969.)
Types of Glandular Epithelia
The epithelia that form the glands of the body can be classified according to various criteria. Unicellular glands consist of isolated glandular cells, and multicellular glands are composed of clusters of cells. An example of a unicellular gland is the goblet cell of the lining of the small intestine (Figure 4-20) or of the respiratory tract. The term "gland," however, is usually used to designate large, complex aggregates of glandular epithelial cells, such as in the salivary glands and the pancreas.
Glands arise during fetal life from covering epithelia by means of proliferation and invasion of the epithelial cells into the subjacent connective tissue, followed by further differentiation
(Figure 4-21). Exocrine (Gr. exo, outside, + krinein, to separate) glands retain their connection with the surface epithelium from which they originated. This connection is transformed into tubular ducts lined with epithelial cells through which the glandular secretions pass to reach the surface. Endocrine (Gr. enclon, within, + krinein) glands are glands whose connection with the surface is lost during development. These glands· are therefore ducrless, and their secretions are picked up and transported to their site of action by the bloodstream rather than by a duct system.
Two types of endocrine glands can be recognized based on the arrangement of their cells. The endocrine cells may form anastomosing cords interspersed berween dilated blood capillaries (eg, adrenal gland, parathyroid, anterior lobe of the pimitary; Figure 4-21)

~~~-"'or'N\t~; ... ~ o\. ~~\_Ln /
. a ~~ { u-.r ·\ . ~tv~\o((."'-t·'""' , ~ ~ ~"'\t,...,. '' 'f.-,~l '-""""' 2. ~~~.~ ~\o·l!,." -= .. ~·····------"-~~~--
\ cl " L l • .. _ _ a notochord - '-f"'t.U\ .. .,. O\l\ S.--'M .. -"'~,..._.. ''""U. ""'~ t.c..\.dt I- " ·. M. .,. LL ""' ~ ..
• ll.lo\.Y'\~ ,-l'A T ~"" \~ 411'\.'?- .. '1--c~~\~,\. ~~~ o\ ~~ \\~•• '-""""' ""'U'~ 2nd P:~~Kngeal ~tv~•'f'~.,t,\ "'~- ~~ Sc..,_ ""'
\t.._.._ 2. ~..,..., Ci'IO"'~ "'" ~"~~·~,.,....-.~ buccopharyngea, \·'-· ;}~~T:.- harynx Se \,\~ (!»\\"~~"'"'\£)""" l5\ t."-\~~ ~, . .,, · ' ..J memb · ~- t~ .. -·· P t· \ ' " ~·
· J\ · " --• .» l .a ___ I ~ {f ;p'-.,(jj,,>:t. ~~ """'... ~ c~ ~·~:-•""~o"-"''~~ fr•A• -.,.-.;~ -. 0\~'""'\' ~ ~. """"'. . ''"''. ~. "1\ "''"'"'Dt- ~-.,.!Stomodel!!Jl. ; ,;fj,~i~ ~~ ,,_ w ., · .,.... 1 · ~
~~ ,,.,'t~\o..,.~ "\~o..''~""~. regi?n of /-- ~3?.~.~~~: a ( ~1 ~~;.) "" \o ''""'~fl ""'~''·"·~.\ _ . , ~ • , developing neck · . ·~.. • " "'
... '. "~ """'' ·-'e~·-,., "~'\* ,. \~\~"""\\~~ . . . \":.. ""''~'"""....,.' ~~" " ' pencardial cavity ,,.. 17JF , " 'o ~ ,
~~ '· ... 'o.a~ ~ ~f\'("'~1~ \o•H,~ A .. E-:~,\\\~J,_l v,~ JO ,
. - '·"-~ ~·~ ~ "n ., )~ "~i - ... , ' ' four plmyngeal pouches ~ ,~ • " .. '"'"''""" ........ '-'~' 4""'a.."'''·~, '~"'-4'. '- '""'~, .......... """"" "("'", ~ .... ~~ \. •'~ ~"CS"~~'flo ..... £'1\. -'-"' .... _ • ""'- '-· ... c ,,, \ ......
~ -, \ "'"'~" , ...... ~' ~-""~ o..~\4t.,., • ..t'\ \ro ,-..., ~-"' ;;;:J:~::'?~''" ,.,•'"'' J '\) 1\0. 0.''- l..'\"'.S, •
~Itt.. &~~.,~~~¥'It"~"~ ~~'-~"'~. ~~~ \ ~~\~\\'"~-& .}.(~·.:' ·:.:-:.·:";!~;.·:;, olfactory pit OIJs( ~ <~'V\oJ~\~JA}e.\-,!t' .....
.. ~ ~ ::;,:.: ... , .. ,.,. :: .. · ·.;:,,~:·': . ~ .. ~ ~- s~t·"'\.11 ·""- ·~- .. • • • • 1.
" 'S ,t\.t s •'-~- u f;:~~~~.f]J'r'. '. ,;l ~·:''~;~:~\·, maxillary ~.,... Y'l\ · , _) "" '""" ~if'~\..,, "'f'""\ .,. ·' .. ... ,!~,;;..,,..<);: ,·· .. - .. ·· process \ . ' ' . ··~ ... · .'.·... " ~' \ ... \,s ;. .. ·-<;>· ~\.~,/=-· ~""" \'\ tt~!>,~'~""' .. ~"'fA.~.,.._\ &\. ~ .. ~ . }''~~,.,~--7J}. ,_/"' .. '·~;·,. . ~
~sL...- , .. u -' ·. ~ • mandibular --~"'· --.: .. -j· ft'..:.:i·~~-i 1 _, ~ '-
..,.... '""-U"'""" S\~. •. \~ ""' ~-'.· "' .. ~ ~o~'"~.... process ~·~p.·:"!"':··,;'_': .. :.:•.:·>,!?-:·_;1}~--.. .•. buccopharygea... .._ ~ "'~"''-""'f.M~ \M~ \tt"4\ ,.N\~~ W\ 4t.. ~ . • ._,. . .. .·. .. .... ,... membrane l n -~ ~'''¥A ~ •t~t"~' ~.,,.,, .. ~~~'~ ,.~·· ~t.r-.:i:.-:::=-' ·:~ ... :.:·>:/:,.~:~)} ·a- c.~~~~s.~. ~~'·"' ~ \\
.. \, 1\ • ...» .. . . . . . -.... . C .. .n• . a • ~ M.... IM.tY c._~\,,,~,"'-~~.._ ID\ \\ ..... ~ \-O~"C.. 'Y>i . '·. : ~_:::F,~: • -,.;t•.U,., Plf '~ . 1\ •
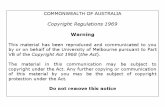
, - ~'•~~ a\~"-"-"' B .,~,;;.J:~i· :·:·:··~} •St,~ ltvtl'L '""~~·~ ~~ .. ~~~.,.-.! IC.~~~~~~t - S Lo\0«.\ tl"'.J\ \e'o\J., - 5 e\-\ri ~ . in the osition of the buccopharyngeal mem-
Figure 11-74 A. Sagittal section a: the embryo ~ho':" ~h b~ccopharyngeal membrane breaking brane. B. The face of the developing embryo s ~wing 8
_ L l . - ~ f IL.. ~ \.,.-. ' ~. f) ~ down. ,.,. ~- _ l"-u,! o~ &.(\ \\\ "'~ 1~ \ 'NV&f'\41 ~/l .
tJIIMl. -1~ ¥'~" ~' ~~~J" Cl t.~!~~ "~ \ . - s~b~~t\>.Jltul" ~ qJo\\"~'·~ ~a~: ~ t\_,'lf'~"~a ~··""-- t?."'\.o!t~\"'

A
.2
3
developing epiglottis
\ \ '
laryngotracheal groove
tuberculum impar
laryngotracheal groove
8
anterior two-thirds of tongue
foramen cecum
posterior ~ third of tongue
epiglottis 0
\
lingua! swelling of first pharyngeal
arch
circumvallate papillae
sulcus terminalis .. ~ ~ [
~~'f"tk~'r~~' . '''"""~~'o-
~~s\-. tl\ .. r dW~.i
~,Y-A.
p~~
Figure 11-75 The floor of the pharynx showing the stages in the development of the tongue.
qy--1.~"'"' \Nt'-'f:-. 1 W\~k'A Swdt~~ t:Jlet1 ( -\-"'-~C4"" \"""~,.,...} ~,~! '""' "-. ~ , • ..,_ ~ ~W4c. ~ ~ "'"-"'tt~a)
,21 ()""·~~ s~dll,·~ • ..,. ~~ s~d-. ~ ~\tc..,.~M~ ~W0.~4.1r> cJJ«-cD ( 1~ \...~~~ "Sw~\~~ )lAe.-r~v.d ~- ~;,.s\ ~~W\..Jl ~).
- ~~ .. \..k~ \\'-'-~~ ~wd~~~ ~\~.._ ~ ~~ \¥.~·~ ~ k \J\"' ~c:JA ~\'-'""" w\~~ ~ ~\,~.._ \~~~ ~ ~~ \~ ~~~· "l..fi ~" \-.n3~.
'So''-'-s kv«..\•'1~ ~"- \~'\·~~~~~ ~~'~..,.~~~~~~~ftl' :_
~ ~~'-~N'· . ar ' i {_-j)~ct.c..~~ \M~ swa,"~~ ~eel U,p~ ~,-rs\~1lb. G"'ooy-~~~~~'k. ..
'--"'~ ~ "~uQ" .. ~ \'-~"' ~ ~ ec:\.u6lr ~~ o"' e.o.fl\. sUI.. e! '"'~=~ i,p,,.. ~ '-"' '-~~ V ~~ «A · :---T 1-k.t- ~f"'""~ .A.\::~~CJt\<.. \~,.~

~, .. ,...
. • ~\4.t~'N\t.'t\~ ~ ~~' ~"'~~ -·---~--------"-'~ -- ·-------··-· -·-- -----= ---~---------- ----~
- \\~'- ~\~~~~ l~v.J}.~\ \~ ~" "'~ ~ _ , \L _ \\ ___ 1stpharyngeal clift-and pouch ~·;-,., ~' 4t""-~~"'~ ~ '" ..,.~
_ 1st arch -. \'\\.~ "''""').,..\~·-"~~, \s ~~~l st~~ ~
<;) "'~'-' ~ t.),,..\c ...... ~ .._ ~·¥ .& \>.\U'"""'"~'""' 2nd arch~ ---.
- \\:..c. ""''!:-c:.,~t:.\"''!)'~ 0" ........ ~" ~""' 'o~'IM,, ~f\\~,,_,~ \~ 5'-'~?~~l\ ... ~~~ ~u
_...,e..~~'" ~\)\.,, ~ ... .;;.,\ 0..~\.W~'""~ b\4\ Cervical si
'" 'S~t..t~t.. -\ ~'IW\'o·•~o ~l e" """~\ ~ \\..... ~~s~.
4th arch ~\ ~ .
..., ~ ~C\\AJ\\ -o ~ S w~~~f\ Ot. 5'-...\t.\ ~ 5th arch
· - '~'"' ~~c._\~\.· c ...__ e ~- _ .16th arch Q p ""' ~'"" ."A '"" --~-..., C!'~\o"'l" ·~~ ..... "" """~ .. -+~"~~ul)
t~_of buccoph~ryngeal membran~
Tuberculum impar
Tubotympanic recess
-,~~~ ./"'External auditory meatus .. __ , . ~ iS __ ~~~-- Tympanic membrane
Foramen cecum
~-1_3)[;:.~ 1 ·,11 )::·-:. ,;)) Tonsil -t'. .. • •.UI\ ,.-.. , •• \\
Copula
[f:~ Parathyroid Ill
Parathyroid IV
Ultimobrancl1ial body
- ~w~ ... !).-.·-u~ ,u .... -..."'-.~~~~-\ \;\.... ~.,.\ -) ~~~._.g ~'-'<-'-'~ . 'Esophagus
Laryngotracheal tube
"""1i_"""_ ("! ____ t\ _ L -.__ • \ ___ () Figurell-80 Thepharyxshowingthefateofthepharyngealcleftsandpouches.Left,Thegreat ,. ~ ~\\Jl o..,.li\ ~"A\.' ~1-X.. downgrowth of the second pharyngeal arch, burying the pharyngeal clefts. Right, The structures
formed from the different pharyngeal pouches.
ts K"'ow'A· a.\ ~~~~ ~

190 CH/\PTER 4 The Abdomen: Part 1-Thc Abdo111inal W<lll
' o~ ~ """'--~ok.c..._) \~. W\•S.tl.1t'lll._ sv\~ \'1.1\h_,
neural tu
intra-embryonic coelom
lateral fold
developing gut
amniotic cavity
extraembryonic
coelom
lateral fold
A yolk sac
dorsal mesentery
entoderm --1!1..__
foregut
ventral mesentery
c
beginning of development of vitelline duct
yolk sac
amniotic cavity
ectoderm
body wall
splanchnic mesenchym~
Figure 4-36 Transverse sections through the embryo at different s~ages of development sh?wing the formation of the abdominal wall and peritoneal cavity. A. The 1ntra-embryon1c coelom 1n free communication with the extra-embryonic coelom (double-headed arrows). B. The devel?pment of the lateral folds of the embryo and the beginning of the closing off of the 1ntra-e~bryon1c coelo_m. C. The lateral folds of the embryo finally fused in the midline and closing off the 1ntra-e~bryon1c coelom or future peritoneal cavity. Most of the ventral mesentery will break down and d1sappear.
8

amniotic cavity
chorion laeve
extra-embryonic coelom
yolk sac
chorion frondosum
vitelline duct
proctodeum
allantois
vitelline duct
umbilical arteries
Figure 4-37 The formation of the umbilical cord. Note the expansion of the amni?!ic cavity I h (arrows) 50 that the cord becomes covered with amnion. Note also that the umbrlrcal vesse s ave been reduced to one vein and two arteries.

192 CHAPTER 4 The Abdomen: Part 1-The Abdominal Wall
structures present in the normal umbilicus
umbilicus patent urachus
umbilicus :-
umbilical cord
fecal fistula fibrous band Meckel's diverticulum
vitelline cyst fibrous band and a Meckel's diverticulum
Figure 4-38 Umbilicus and some common congenital defects.
(continued)
VrrEu.OINTESTINAL Ducr
The vitelline duct in the early embtyo connects the developing gut to the yolk sac. Normally, as development proceeds, the duct is obliterated, severs its connection with the small intestine, and disappears. Persistence of the vitellointestinal duct can result in an umbilical fecal fistula (Fig. 4-38). If the duct remains as a fib~o~s band,; loop of bowel can become wrapped around it, causing iutestinal obstructWJ1 (Fig. 4-38).
Meckel's diverticulum is a congenital anomaly rep-"--r---~-.--.-.. -~· resenlng a pers1stent portion of the vitellointestinal duct. It occurs in 2% of patients (Fig. 4-38), is located .about 2
ft. (61 em) from the ileocolic junction, and is about 2 in. (5 em) long. It can become ulcerated or cause intestinal obstruction. ·
UMBILICAL Vf.SSEL CATHETERIZATION
The umbilical cord is surrounded by the fetal membrane, amnion, and contains Wharton's jelly. Embedded in this jelly are the remains of the vitellointestinal duct and the allantois, and the single umbilical vein and the two umbilical arteries (Fig. 4-39). The vein is a larger thin-walled vessel and is located at the 12 o'clock position when facing the umbilicus; the two arteries,
(continues)

710 Chapter 19
amniotic cavity
chorion laeve
extra-embryonic coelom
amnion
chorion frondosum
amnion
vitelline duct
foregut
proctodeum
vitelline duct
remains of allantois
umbilical arteries
Figure 19-20 The formation of the umbilical cord. Note the expansion of the amniotic cavity (arrows) so that the cord becomes covered with amnion. Note also that the umbilical vessels have been reduced to one vein and two arteries.
- \a...~~ w\~ A~v~•~"-'~'X\ ~ '-'u.A 1 \3:J\ ~ \~~ ~\.1,~3 o\ (~\,.,~o ~' w\!~ ~ cJi C...\M\M\A~\ ~.,,
""~'~ ~' ~'M.\c\\~ {~ ~~.

Stomach
Pancreas
A 8
Figure 13.4. Embryos during the fourth (A) and fifth (B) weeks of development showing formation of the gastrointestinal tract and the various derivatives originating from the endodermal germ layer.
D·~J~~~1'~~···~ ~ ~ ..... ~SD ~~~~ ~-_,_...., ________________ _ - ~'-\e~~ ~ ..... ~'J\.C\.~ ~~ ~ ~ ~v.l ·~o.\ <;\.\Cc:.£~J.s: ~ ~-~,!'1\AC..
- ~\~\.:- -~~ ~~ "' ... ~ ~~~"A.a..~ tt-cl~~~w.. !csu.tA.!.t \~ ~-~~ ~\~\~
Respiratory diverticulum
Esophagotracheal septum
·~~-Trachea
Lung buds
A , ,, B ·• C y :c::!~:_. '-" .. .,.,.."'~"'~ ,.~.,. ~
Figure 13.5. Successive stages in development of the respiratory diverticulum and esophagus through partitioning of the foregut. A. At the end of the third week (lateral view). 8 and C. During the fourth week (ventral view).

~'
~s~ if\'fk~(~ ~'-~~~ ""\ "" cO"~" w\""couA .\-~~eceov'-'Q.~·tc.'--\ \-\~\-""'\"'~ : ~ ccu..,- \"" \{ '"\ ~> 0«.')
. ~0,,. ~'If'~~"' t-, "0 ~~.
Bifurcation
A
Proximal blindend part of esophagus
Esophagotracheal fistula
8 c
Communication of esophagus with trachea
'\.o Z ·v"''''' S
. Distal' part of ,.__ " Bronchi ~ esophagus
e '\"'•)..,_ 01.\o~o<t'~_g,'\-,~ ~ 0\S.\CCJ\~ ~ .,. ~ e,.:.,)tU ... 0 q., ~ \-"'"'\L
-.: 1. .lf'D e.s<>~l.o.!I~Jl ~\-.-d~' w \ >f',.. (!;, ~ ' "" b ;~ )i~ c\ \_ 't-r.. tJr. .\
8 S 3 ~~, u\ "'c.!c.. {.ol.i"!l. ~~~ ~ ,
aMI\' a...c. 6\, ~ .., .. ~ ~ '-'"' '
lilt ~ ~ fL "f" t).. "~ \1(~ '~'"""-~-\'"" \..&;\
' ... f>vv'\_ ~ 6o. "'.,.._ '' ...
... o...\.V\o.,...,~ S"o"'\-~~'i~ s\ '-.S.•V\:J~\'~ ~ ~\·~~L~~~ "''-~~'-.0 "~.,..""\'-
, (!_p..,.,-..~ o..c.. a.._\.. t..'"' ~ .. \. ~ '~ ~"-A. OA..""-1"~'1\A
• 'e ~"'S Jt ~,.,9"" aJ.rtSI'
• ~-o..\ ~-\N'~:~ D ' '-...... -." ~'--\).c.. c.. 'rs
c1; str.l r~'-~. E eso~\\·
... tA M K"' e w ""' ~~ .~ \l".
,. ("(C \'.\ ?\\ t':t.~C "' o\ Tt.~s ---• po~ ~~ t:P.;."M; • .s ...
. ph ~rDV\.\."-
Figure 12.3. Various types of ~LP and/or tracheoesoPhageal fistul'l. A. The most frequent abnormality (90% of cases) occurs with the upper esophagus ending in a blind pouch and the lower segment forming a fistula with the trachea. B. Isolated esophageal atresia (4% of cases). C. H-type tracheoesophageal fistula (4% of cases). D and E. Other variations (each 1% of cases) .
• (1~111' \~ ~ ~~o..c.Jk ~ ~\~~tA\..,"o"' ~,~, ~~:-~
1 E..~c ~,._~ \.',1

The Abdominal Wall, the Peritoneal Cavity, the Retroperitoneal Space, and the Aliment:1ry Tract 709
A amniotic cavity 8
neural tube amniotic cavity
extraembryonic I·
splanchnic mesenchyme
lateral fold
coelom
c yolk sac
dorsal mesentery
foregut
ventral mesentery
beginning of development of
vitelline duct
yolk sac
amniotic cavity
body wall
closed off
splanchnic mesenchyme
Figure 19-19 Transverse sections through the embryo at different stages of development showing the formation of the abdominal wall and peritoneal cavity. A. The intraembryonic coelom in free communication with the extraembryonic coelom (double-headed arrows). B. The development of the lilterill folcls of the embryo nne! the beginning of the closing off of the intraerlbryonic coelom. C. The lateral folds of the embryo finally fused in the midline and closing off the intraembryonic coelom or future peritoneal cavity. Most of the ventral mesentery will break down and disappear.
\'A\.~~""'~~o~\c.. tj,t.)..,~ \s ~~eel ~c..~U!"' ~'- <;.\M~c.t'.s~\4\\\~~'<. \~t~.:: o\;. \~~ 'M~~ .. &t.'t'l-\fA ~
~~"f"\ 'n>~e..g_ CoN\\-: ~t.'l'\~tA ~o·•·• ~4l ~'-"\.~~•'-'~t.. <!.o.&e~ ~'"~ C'.GAAJ.&l. ~ ~Ill~""'.....,.. ~'f\SV '¥",£<~," .. .,".
- \"'. e.c...,..\.-\ ~~(..: ~«..,.\ ""=''~- (,"""""~•'':-·' ~, ... ~ C..'».~~"''-·''~~~ ..... w~-.~ - -

~ .. - ~--¥"1'0~ ~-..A eS. ~ ~
-~" ~;-~t.~~~~ ~\~~~ "~"'~~ Auc.~-...1·~ ~O"A~ak ~'~'~ The Abdominal Wall, the Peritoneal Cavity, the Retroperitoneai"'Space, and the Alimentary Tract 7S5
hepatic bud
pericardium ----~,-...!!_ ventral mesentery -------.:~~-,..!.--~
yolk sac
pharynx
foregut stomach
dorsal pancreatic bud
hindgut
lffi~
tD~..,J)o~~'-''r a~ <::,~~~ ,
c\c.vt.\o~~ Cl~ A.\\~"''1\ ~ ~ ~~~~.
Figure 19-71 The foregut, midgut, and hindgut. The positions of the ventral and dorsal mesenteries, the hepatic bud, and the ventral and dorsal pancreatic buds are also shown.
Figure 19-72 Development of the stomach in relation to the ventral and dorsal mesenteries. Note how the stomach rotates so that the left vagus nerve comes to lie on the anterior surface of the stomach. Note CJiso the position of the lesser sac.

omentum
gastropl1renic ligament
~ £.1<1Sirosplenlc omenlum
~(hg,mmol)
cJ ~~- t - l1enorenal
·:~:=~~ :~_- :~. ligament -....:......-- -
_--:._ - . --
'·' dorsal mesentery umbilical vein
stomacl1 inferior vena cava
lesser omentum
liver
lesser omentum
· ~.'SStr •'A\4t~""~
greater omentum transverse colon greater omentum
Figure 19-29 The rotation of the stomach and the formation of the orcater omentum and lesser sac.

278 PART II SPECIAL EMBRYOLOGY
Lesser omentum Stomach ___ , _______ _ Spleen
i
/
A Umbilical vein
Dorsal mesogastrium
Dorsal pancreas
Falciform ligament
;·
'
B
Liver
Lesser omentum
--- ------ Lienorenal --~~~-·---------... I igament
-.. '-~\ '· .
\ ·Omental bursa
Gastrolienal ligament
Figure 13.9. A. The positions of the spleen, stomach, and pancreas at the end of the fifth week. Note the position of the spleen and pancreas in the dorsal mesogastrium. B. Position of spleen and stomach at the 11th week. Note formation of the omental bursa or lesser peritoneal sac.
Liver
Adrenal gland
Dorsal · • mesogastrium
~~~----··tfjr·Spleen
Lesser omentum
Falciform ligament peritoneum of body wall
Pancreas
Spleen Gastrolienal ligament
Figure 13.10. Transverse sections through the region of the stomach, liver, and spleen, showing formation of the lesser peritoneal sac, rotation of the stomach, and position of the spleen and tail of the pancreas between the two leaves of the dorsal mesogastrium. With further development, the pancreas assumes a retroperitoneal position.

... :>.
~~----~~-------
lesser omentum
stomach
greater omentum
left triangular ligament
falciform ligament
coron<Jry lig<Jment
right triangular ligament
inferior vene~ cava
lesser omentum
liver
transvGrse colon · greater omentum
Figure 19-29 The rotation of the stom<Jch <Jnd the form<Jtion of the or·c<Jter omentum illld!t ; lesser sac. "~Lf ·
·~ \1 ~~"'' 1U ,...-u....i.\ .,~ ""'' «-Utk~e~c. !.....,"'-' •S c~.,..,~.J *"«~\ot,..~ .A.2 .... 'fL. 5flUNt. ·~ e,tl;t.~A.s ~ .. ._ ~~., ~"""' •\ ~""'L~ 'nt ~e!J.. -.\t!. w..U S"""" "" -rVU$v. ~~'<~4\'1. (»"'"'""'-"-~ . .. . . • . \-\"\• ~~· 'v.. a..~•A ... \'.k.., ~~\a"'- \~f.N" .t p~v\h~'M ~·A.\.•"' \"u.,
· ·· : ~<Nv4·!'S~ e....\o-A. ''··"'' .·.· ,.... .• ·'.", ·!.'' •

The Viscera Associated with the Alimentary Tract: The Liver, the Pancreas, and the Spleen 789
first part of duodenum
second part of duodenum
stomach
ventral pancreatic bud
third part of duodenum
dorsal mesentery
pancreatic bud
ventral pancreatic bud
hepatic bud
first part of duodenum~ stomach
dorsal pancreatic bud
fourth part of duodenum
dorsal mesentery
ventral pancreatic bud
D~ \J ~.,\'~~e., .... ~ ~~~ \.\ vt ..... 1,£_
~\ /peritoneum will fuse here 0i' and then disappear
~ - ~""'• S¥0\a.IS va.;,&\~ '"-' S\4.,
'o\,.._ &'-'c..'rs ~----------------------------
«. eCC.~"\\, g~ ~\ ~""'oA.o-t4
~"' dorsal pancreatic bud
.. \~, ~ \o\M. \._t.._., w.v.U.. \~"' ~" "-- \).. \o\sc. ..
Figure 20-20 Developmt::nt of the duodenum in r~lation to the ventral and dorsal mesen-teries. Stippled area, foregut; crosshatched area, mrdgut.
l',uf'f" ~~s ~ -..,.... ~\~~ ~ o'\ \w,~~ &~ .,_ ~o\\1 'a"l o~ q"'\.~,~~ ~dA.£ S\~ ~ o~~\.,._ \'-u ~ ~~e. o~ ~ ,.._, 4 -\'''"~~~ l.l. t.otvt.s~·"~'~~ \. ~ ~._."' \\.M.~ -'-"'~ ~ 2Ml ~~ "~,, ~ :'M4;1 !,t. "'~~c. \evA ~~ a.M.'-.~~~ ~~\o \M6.~ 0~ $~'~"~'( -.~ ... c.o.llt.~\c;!.!'-"~ . '\ - ~ r\ ~ l\ • l . ' ,n~ lt ...... ~SVCY'!'A.'N'q ~ ~~ \o,,_,. .. ,\f\6U. "W\\o "\r"'"'-"" \~ .. ~ ~ u.J~'~ c.::. .... ~~ ~ e_,,.....,~~ ~ ~ '"':"'" \)~~J, ~~ \ ~ · _,\Je .... <;\"""'~ouL ( '-~~~ "-.-. v~,.~ tt~~\c\\\iJ) ~~·"~ '"" S..,"''~~\'\1•1~~§ ~-\"-""''>.": .. ·~ ~~\o&..~ «:d.\~ > '-.\ve._- <:.o~s C..."-.~'"- \co\~\'"-~ ~ \,.\\1~ • ,~ ~ ~ 'M..~t~t;A.c...\~~"'e ~ s~~ .. ':Jo. ~·~~~"''" ~c. ""'~w. ~~~'- \t,,.}. 1L \).• i('r~£\.-\- ~.~\~ ._~~"'-'-t. ~ 'o-.c..~' CA.~-.~~··b~~'!'~-""'
t .............. - .... \. .. ,._a ... _ .1 .. • \..., .ll.--.~'~ L ...... ~· ... j, .. e....

bile duct
Figure 20-18 Longitudinal sonogram of the upper part of the abdomen showing the lumen of the gallbladder. (Courtesy of Dr. M.C. Hill.)
right hepatic duct
left hepatic duct
common hepatic duct
accessory pancreatic duct
main pancreatic duct
Treitz in dorsal mesentery

.,.
CLINICAL CORRELATES
Liver and Gallbladder Abnormalities
Variations in liver lobulation are common but not clinically significant. Accessory hepatic ducts and duplication of the gallbladder (Fig. 13.18) are also common and usually asymptomatic. However, they become clinically impcrtant under pathological conditions. In some cases the ducts, which pass through a solid phase in their development, fail to recanalize (Fig. 13.18). This defect, extra he
'patic biliary atresia, occurs in 1/15,000 live births. Among patients with extra he, patic biliary· atresia, 15 to 20% have patent proximal ducts and a correctable
d~f~~ct, but the :remainder usually die unless they receive a liver transplant.
Cystic duct
Hepatic due Bile duct
B Duodenal loop
Figure 13.18. A. Obliteration of the bile duct resulting in distention of the gallbladder and hepatic ducts distal to the obliteration. B. Duplication of the gallbladder.

756 Chapter 19
head of pancreas

; /•=w~1~Hr?roiDpHJiRri0Ufi~n I Development of the Pancrcils'.----------------,,. The pancreas develops from:~ dorsnl <Inc/ ventr<ll bud
of entodermal cells thilt ;nise from tl1c~ fofC~JUl, The dor
sal bud originutes il short clistilncr~ ;1/JOvr: 1/w vrmtr<ll /Juri
and grows into the clms<il 111c~;ur11r~fy, 1-IH: vcrJtr<il IJucl
arises in common with tlw hcp;ltir:,IHrri, <:l(j,;r: rn thr: j1111r:
dorsal bud
region o/ rapid growth
vcnlml bud bile duel
tior1 of the forc~Jut with the micl9ut (Fig. 20-19). A canul
i;r:rl rlucl sy:;tcnJ IIOW devr:lup:; in cac/1 IJucL The rotiltion
of tlw stomilch <Inc\ cluocicnum, tonether with the rapid
~rowtil of tile left sicle of the cluoclenum, results in the
ventrill IJucl's coming into contact with the c/orsiJ/ bud,
<lllcl fusion occurs (FirJ, 20-25),
Fu~;ion :ilso occ1w; IJctwcen tile ducts, so thiJt the
main pancre<Jtic duct i•; rlr:i-ivcc/ from the entire ventral
~""c..'~"' l.~et lit ""'' ~\S~ ~.,...\ -\ ~~r'S.L.\ ('J ~.
bile duct
forms accessory pancreatic duct
Figure 20-25 The rotation of the duodenum and the unequal growth of the duodenal wall le<Jd to the fusing of the ventral and dorsal pancreatic buds.
foregut artery (celiac artery)
midgut artery (superior mesenteric artery)
hindgut arte,ry (inferior mesenteric artery)

Figure 13.16. Transverse sections through the region of the duodenum at various stages of development. At first the duodenum and head of the pancreas are locJted in the median plane (A). but later they swing to the right and acquire a retroperitoneal position (8).
pancreatic bud
Fi ure 13.19. Stages in development of the pancreas. A. 30 days (approximJtcly 5 9 ) B 35 days (Jpproximatelv 7 mm). Initially the ventral pancreatiC bud l1es close
mm · · · d d t ward the dorsal to the liver bud, but later it moves posteriorly around the uo enum o
pancreatic bud.
Figure 13.20. A. Pancreas during the sixth week of development. The ventral pancreatic bud is in close contact with the dorsal pancreatic bud. B. Fusion of the pancreatic ducts. The main pancreatic duct enters the duodenum in combination with the bile duct at the major papilla. The accessory pancreatic duct (when present) enters the duodenum at the minor papilla.
pancreas. Insulin secretion begins at approximately the fifth month. Glucagonand somatostatin-secreting cells also develop from parenchymal cells. Splanchnic mesoderm surrounding the pancreatic buds forms the pancreatic connective tissue.
CLINICAL CORRELATES
Pancreatic Abnormalities
.. · Theven,tral ~:~~~re~ti~ bud consists of two components that normally fuse and '.···rotate 'around the. duodenum so that they com~·to lie below the dorsal pancreatic
b~d. Occasiona.lly, however, the right portio~ of the ventral bud migrates along ·its normal route but the left migrates in the opposite direction. In this manner the duodenumissurrounded by pancreatic tissue, and an annular pancreas is
- for;;,ed (Fig. 1i21 ).The malformation sometimes constricts the du~denum and causes complete obstruction.
Accessory pancreatic tissue may be anywhere from the distal end of the esophagus to the tip of the primary intestinal I cop. Most frequently it lies in the mucosa.of the stomach and in Meckel's diverticulum, where it may show all of the histological characteristics of the pancreas itself.

288 PART II: SPECIAL EMBRYOLOGY
Hup~llic uucl
::n.::nn~uTun:-cnr,ro,,.,._,.'>•
'"""''"-'"c•c•=~··="-~") -r--Stomach
/
/ /
Dorsal pancreas
Main pancreatic
duct Accessory pancreatic duct
Figure 13.21. Annular pancreas. The ventral pancreas splits and forms a ring around the duodenum, occasionally resulting in duodenal stenosis.
Cloaca
·Lung bud
Celiac artery
Superior mesenteric artery
inferior mesenteric artery
Figure 13.22. Embryo during the.sixth week of development, showing blood supply to the segments of the gut and formation and rotation of the primary intestinal loop. The superior mesenteric artery forms the axis of this rotation and supplies the midgut. The celiac and inferior mesenteric arteries supply the foregut and hindgut, respectively.
transverse colon with the distal third. Over its entire length the midgut is supplied by the superior mesenteric artery (Fig. 13.22).
Development of the midgut is characterized by rapid elongation of the gut and its mesentery, resulting in formation of the prin1ary intestinal loop (Figs. 13.22 and 13.23). At its apex the loop remains in open connection with the yolk sac by way of the narrow vitelline duct (Fig. 13.22). The

-
cephalic limb of midgut loop )
''""'"' doct ~y -~_I~ =====::.
""''llimbo~l 2
appendix·· cecum
Figure 19-74 Stages in the development of the cecum and appendix. The final stages of development (stages 4, 5, and 6) take place after birth.
aspect, a counterclockwise rotation of approxim<ltely 90°
occurs (Fig. 19-75). Later, as the gut returns 'to the ab
dominal cavity, the midgut rotates counterclockwise an
additional 180°. Thus, a total rotation of 270° counter
clockwise has occurred (Fig. 19-76).
abdominal cavity
1 remains of
The rotation of the gut results in part of the large in
testine (transverse colon) coming in front of the superior
mesenteric artery and the second part of the duodenum;
the third part of the duodenum comes to lie behind the
artery. The cecum and appendix come into close contact

Y- ~tl~~ \.o.~ ---+ ~"-~s~"\.~~~ ""e~~~o·~ ~ .... ~ \.o v-o..Q,~ ~\1,)'~ ~
· ' "l. - Diaphragm
Uv~V' ~' ~\~'.J\.«e~-r. Liver
Falciform ligament
Allantois
Lesser omentum
Descending colon
Jejunoileal loops
A Cloacal membrane
Transve colon
Cecal bud
Vite dL
Figl rota bud inte: plac
RE
Du abd
nal lao
apf oft cav
lob
nal mo' reiT the abd iss mic

n
!I ~o~•"" ~ ~ "'~~~~ \.oop Z'\1\ "'~ \A'M~,,~ (J)~ ~ ·3..£ ~\Mf'Yo \, \\'- o.\,~o~~ <Jl..N\ " .. ~
-
Cephalic limb of primiary
intestinal loop
A
Superior mesenteric
artery
Caudal limb of primary intestinal loop
B
Figure 13.23. A. Primary intestinal loop before rotation (lateral view). The superior mesenteric artery forms the axis of the loop. Arrow, counterclockwise rotation. B. Similar view as in A. showing the primary intestinal loop after 180° counterclockwise rotation. ThiJ.ransverse colon passes in front of the duodenum:
~ i
Transverse colon
Aorta
A
F. 13 25 A Anterior view of the intestinal loops after 270° counterclockwise Jgure . . . . . f h I rotation. Note the coiling of the small intestinal loops and the_ pos1t1o~ o t ~ ceca bud in the right upper quadrant of the abdomen. B. Similar v1ew as 1n ~· w1th the intestinal loops in their final position. Displacement ofthe cecum and appendiX caudally places them in the right lower quadrant of the abdomen.
• '\ \,u ~' 'roW. oro\...."":,"" 2 "1u ~ c.o'-'\\\.t...-cJ.~U~\.S~

758 Chapter 19
I ,bdomio.l ooWy "\
remains of extra-embryonic coelom
A
developing appendix
extra-embryonic
)~stomach 8
decent of cecum
. . (A B) f the counterclockwise.180o rotation of the midgut Figure 19-76 Left side ~Jews , o . I .t C The descent of the cecum takes loop as it is withdrawn mto the abdomina cavl y. .
place later.
~u.Sltn-~ ~~:.~~~~~A.~~~~-- . - '"'· (o\o.,. \\~ \~~~~'r o~ "'' ~~. 'rAt.S«~"'o;o\c. ~\.t..,~ ~ '2.'11\c\ ~ .\ cl_.J. -~~¥' ~61f'\ ~ ~. ~ \\-.~ 'o~\"'A ~ c;""1. "-'-u'.,_."~~ 6N'"""'~. - C.tt.c..~~4! ~tv.'-'v.ac. c..._ ... , \'A~ to"'"'-t.'r ~ t'!J \~'-« ., ""'- \.\vtv
~.,.. ~~ ~tS(_~>o\A. Wo ~~.·~c.. ~!.So.. S 0 • ~ S(. ~'A''~\ <lAo~ ~ l ~vtM-tJ. - ~"' {4\\t '\l~ I.LNC. \.
- \,..,.~t. ~~ o.~~ ~o~., \\ t. \~~"\ ~~ ~{\~<.\'-. ~ tc.-A\vo1l"
~\-.t.t.l. 4)~ ~~ • .
. • " • ~ .,_. ~\A.e~(~"'..,._ ~ ~~ w:~ \'~tt\..J. '\)tv,~t.~ '0¥\ - i'""""'\w' ..,... .. ~~ ... - ........ ""t \ • "-"' "" n..£'\. ... ~wolf\ ~ f~~C...tY-.6\\\~ ~~ ' y-- • •
!uc.t.~;.~"" ~"', 'o~c..""'c.\ ~~~u\"-"'ul o~'-.!."' - ,
~\ S'\M~ \·~\u~

Cecal bud Cecum
Appendix
Ten1a
Cecum
Vitelline duct 8 Jejunoileal loops A c
Figure 13.26. Successive stages in development of the cecum and appendix A 7 weeks. B. 8 weeks. C. Newborn. , · ·
- lAS \\_._ \'"\t~~~ ~Y''t\l ~ ~ ... Q\,.~~0~'"~ C&N'\.~ .&a. . ~..) .,~~
",~,: \ ~4. "lf;-a'M-£ "\o\;\.~ Tenia
~ S'-v-t.v-..s l-.r Cc» , Iibera • \.i \.1.... "'~ ~\'0"'
W\ ~ '~" .3~ •
Retrocecal position of vermiform
~igurc 13.27. Various positions of the appendix. In about 50% of cases the appendix IS retrocecal or retrocolic.
Dorsal mesogastrium fused with
Dorsal mesoduodenum fused with abdominal
wall
Ascending colon_.._-,,_,.,
A
Greater
Dorsal mesogastrium fused with
posterior abdominal wall
Sigmoid
Lesser curvature
Dorsal mesoduodenum
fused with posterior
abdominal """'--.-~-..· wall
Greater omentum
8
Mesentery proper
Cut edge of greater omentum
ransverse mesocolon
Figure 13.28. Frontal view of the intestinal loops with (A) and after removal of (B) the greater omentum. Gray areas, parts of the dorsal mesentery that fuse with the posterior abdominal wall. Note the line of attachment of the mesentery proper.

I. . •.. I
entodermal cloaca
• }.1\-,.¥-.. ~-.¥-~' liver
f!(._""" l,~.- ~'~~ T"~ (.o."~''" ~ ~'Wio~~ ~ ... ~~~a.,.,.~ q~ ~
\Jt;..i c..\.~'A~"A~ ~ ¥,\~~~
uroreclal septum
· l',s'-~ j.... Ji·\'"'· c ~- ... ~
~If\<. .... '" c\ ,·w\ ( ·~~ ~, S \~·J>A._,\A. u,Slo"..-.
1-'.'i»\'f! ... ,.,Ootf"\- .a\~ c..~.J.
C.."K~ .. Ac.~·-. ~ ~~~.\.~~ .l~o 'O'W"'MI ~<&. \-~"A\0"Ai ~ \,\...U~'f" '- \A.'I"t. ~"""'
- T.,.,~~"".tl ~ov'"';•~ ~\t-1~ eM\.t..,..s
~' ~~s~. ,.~~,.~" ~ cl,LCA.. --? ~1'\~,\-,V,. QMowt.'rol ~ .
... ~\-.~ t.M\c.~s ~~ ""'- ~-rrl-· f'o.,~o"" •\ '4...... 0•4-CA ~
t.k"'o~t~,~ ~~'n'-V) •
spleen
foregut artery (celiac artery)
~~, ~..l.
~~ midgut artery (superior mesenteric artery)

c
Allantois Primitive urogenital sinus
~ J ror£·C.tal septurr
, ~loacal : lindgu · m·-rane B
Chapter 14 Digestive System 225
Urinary bladder
Anorectal canal c Figure 14.3 '· Cloa~il region in embryos at successive stages of developrr. 1 .. I· T'le hindgut enters the posterior por
tion of the cloac:-. •.··.e future anorectal canal; the allantois enters the anterior portion, the future urogenital sinus. The urorec
tal septum is for'' ed by merging of the '1esoderm covering the allantois and the yolk sac (Fig. 14.1 D). T 1e cloacal membrane,
which forms the •tentral bo1mdary of the cloaca, is composed of ectoderm and e'ldoderm. B. As caudal folding of the embryo
continues, the .:rorectal ~~~~urn moves closer to the cloacal membrane. although I• ·;ever contacts this structure.
C. Lengthening vf the genita: •t'bercle pulls the urogenital portion of the cloaca antAriorly; bre;' 1:down of the cloacal membrane
creates an openi~o~. for the> htf\tf:;ut and one for the urogenital sinus. The tip of the CJrorectal s. :Jtum forms the perineal body.
Urinary bladder
J /;/\ ... · .. ! ~~~.. / !. rethru · ~ 1 _/ I ., , . . 't
A :3-:rdum ~,. "· PI
Rectum
c
Urethra_,_ -
B
A- :il pit
D
Figure 14.3 7 Urorectal (I\·. and recto vaginal (B) fistulas that result from incomplete sepa1 ~ion of the hindgut from the
urogenital sinus by the urorecto' septum. These defects may also arise if the cloaca is coo smali, which causes the opening of
the hindgut to shift anteriorly. C. Recmperineal (rectoanal atresia). These defects probably result from vascular accidents in
volving the caudal region of the hindgut, resulting in atresias and fistulas. D. Imperforate anus resulting from failure of the anal
membrane to break down.

-----~
i~f\!}~~~~;'~~~~Z,'~;~~: ;;ek::vn1~:na~6u:~~~~t f:~:u~a~ ~; 1 ~;~:mnc fi;tula I f;g. j
· ... G'ut Rotation. Defects ;·,/i:.~. ~ .. " '·· .. ~ .. '.. . me;~·~ _.':_~·normal rotation .of the intestinal L~ may result in twisting of the intestine \':;(volvulus) and a compromise of the blood supply. Normally the primary intestinal . '.loop rotates270° counterclockwise. Occasionally, however, rotation amounts to :~~~!~~nJ,{,V'Jll~n-thisoccurs, the colon and cecum are the first portions vfthe gut ··to, return from the umbilical cord, and they settle on the left sLQ;e of the abdpmiJJ&~J : .. :'>52iif~· .. (f,i_g.1~_.~1Al:,.Thojaterroturning loops then move more and more to tho :':;{right;'r~s1Jiting in left~sided. colon. . · ~Y/iCt1~R~~r~~d rotation otthe intestinal loop occurs when the primarv loop rotates . 90°7ockWise: lnthis abnormality the transverse colon passes behind the duode
)'Q'Y'RI:tfig; __ ,~~~JB) '<lr.d ljes ·behind the su~erior mesenteric artery.
i(liM:~;H~p,l,i~~~i,?O,S,!J~· ipt~~!.!~a~}pops and cysts may occur anywhere along the ~.:::,'length'oJthe guttube. The'yare most frequently found in the region of the ileum, ;.·;<where theylllay_.var}r,f~oma long segment to a small diVert.iculum. Symptoms i"'','i~~,d~uv:'o'c~ur ~-~~~~;;:j~'life; 'and :33% a~e- associated with other def~cts, such as ~;:;j~-t~~tinai'at~esias/irriperfo~ate a~us, gastroschisis, and omphalocele. Their ori('\q'9'ir11i~'u~kn~\:v~;~lthbugh:th~Y.rnay re.sult from abnormal p;oliferations of gutpa-
lij~tsias a~d ~tenose3 . . . :-:'Atresiasa-nd stenoses may. occur anywhere along the intestine. Most occur. in . < th~ duodenum, fewest. occur in the colon, and· equal numbers occur in the
'c .. ', .... <J: . . ' '
··- jejunum arid ileum (1/1500 births). Atresias in the upper duodenum are probably
Transverse colon
B
Transverse colon
Descending colon
Figure 13.31. A. Abnormal rotation of the primary intestinal loop. The colon is on the left side of the abdomen, and the small intestinal loops are on the right. The ileum enters the cecum from the right. B. The primary intestinal loop is rotated 90° clockwise {reversed rotation). The transverse colon passes behind the duodenum.

- I u It·,. J~ sc.~t-..8 ~ '"'-"'~' '\\.e. \)~.; 1.!. 1;1. ~'"\ , ... ~ .... ,0 (' ~~.·-~ J.w,.~ ~Ac. '1- "'"' Cjl i'~>- 'M~~~s J5 ~~ \~\4. ..
• ~~ "'•~~ .... ~ S\-hM~fW' ~•'~'" "...,._ J '( !c:.t-.J.s ~ -~ \-~ h ~~~'-''-,.. '-a,)'"~ v..-, ~u ~~ ~~ \-..~ '"-' ~~" • .
- ~-- ~"-'u. \o\~ow\ ~" ~ '-'"-u·'~'""•'-·~tA'tA t:J J.ecc.._~ ~ .... ~,~ \~ ._
~ .. "it~!.·~ V~,"~' ~"~~ ~v..\\.1 ~·" '..i-.1 l"J...~ J'c\ • .,.1 ve~..J~ 1
~..........., ... , --'.. '~'\M~"~'- v~u..,s} ... ,~ ~ - \,~ ""'""• """" ... ~""" ~ ~:.,"..! ~'*~~ ..... ,\ ... ~ ~~\("'0~ .. ~~, 'o~ ~~A
~ ~. cs~ ¥AO"'"-' . .. .. ~ t\ ...... " .. ,. ""'- $ ~c..-"""·o.\.~c. ~~ U,..uo ~At.. '"'9"'"'-'~ ~ o...(..(\.'A\~
~:~~ ~~ ~ te<H< A ~ ""Y
P'"'""' ,gimli< :_ D b I m ~ 9"'""''"'"m ~ w 9" '"""" \ /'
8
c
round ligarr.ent of ovary
round ligament of uterus
d f t of tile processus vaginalis in tile two sexes. Figure 19-16 Origin, clevelo~ment, an a e cl tile descent of tile ovary into tile pelvis. Note tile descent of tile testiS Into tile scrotum an

H
A
Respiratory diverticulum
Stomach
Liver bud ~-:::-~·---~
. 0
Septu transversum
Liver ~ - -~.-- ..
8
Larynx
Esophagus
Stomach
Figure 13.13. A. A 3-mm embryo (approximately 25 days) showing the primitive gastrointestinal tract and formation of the liver bud. The bud is formed by endoderm lining the foregut. B. A 5-mm embryo (approximately 32 days). Epithelial liver cords penetrate the mesenchyme of the septum transversum.
A Cloacal membrane
Lesser Bare area of liver omentum Dorsal
Tracheobronchial diverticulum
Esophagus"
Stomach
Pancreas
8
mesogastrium
as
m
Figure 13.14. A. A 9- mm embryo (approximately 36 days). The liver expands caudally into the abdominal cavity. Note condensation of mesenchyme in the area between the liver and the pericardia! cavity, foreshadowing formation of the diaphragm from part of the septum transversum. B. A slightly older embryo. Note the falciform ligament extending between the liver and the anterior abdominal wall and the lesser omentum extending between the liver and the foregut (stomach and duodenum). The liver is entirely surrounded by peritoneum e>..cept in its contact area with the diaphragm. This is the bare area of the liver.