+ State Policy Issues: 2015 Alison Haddock, MD, FACEP Assistant Professor, Baylor College of...
30
+ State Policy Issues: 2015 Alison Haddock, MD, FACEP Assistant Professor, Baylor College of Medicine Trustee, National Emergency Medicine PAC (NEMPAC)
-
Upload
letitia-fletcher -
Category
Documents
-
view
217 -
download
0
Transcript of + State Policy Issues: 2015 Alison Haddock, MD, FACEP Assistant Professor, Baylor College of...

+
State Policy Issues: 2015
Alison Haddock, MD, FACEPAssistant Professor, Baylor College of MedicineTrustee, National Emergency Medicine PAC (NEMPAC)

+Disclosures
None
Employed at Baylor College of Medicine


State Legislative and Regulatory Committee



TODD MAISEL / NY DAILY NEWS

+End-of-Life and Palliative Care

+Costs of End-of-Life Care

+Opportunity of Palliative Care
Improve quality
Decrease costs
RCTs of palliative vs usual care at end-of-life Gade, 2008: save $4,855 per palliative pt Brumley, 2007: save $7,552 Greer, 2012: save $2,282
Non-monetary benefits Patient satisfaction Quality of life Survival?

+IOM Report: September 2014
+Recommendation #1
Government health insurers and care delivery programs as well as private health insurers should cover the provision of comprehensive care for individuals with advanced serious illness who are nearing the end of life.
Comprehensive care should
be seamless, high-quality, integrated, patient-centered, family- oriented, and consistently accessible around the clock;
consider the evolving physical, emotional, social, and spiritual needs of individuals approaching the end of life, as well as those of their family and/or caregivers;
be competently delivered by professionals with appropriate expertise and training;
include coordinated, efficient, and interoperable information transfer across all providers and all settings; and
be consistent with individuals’ values, goals, and informed preferences.
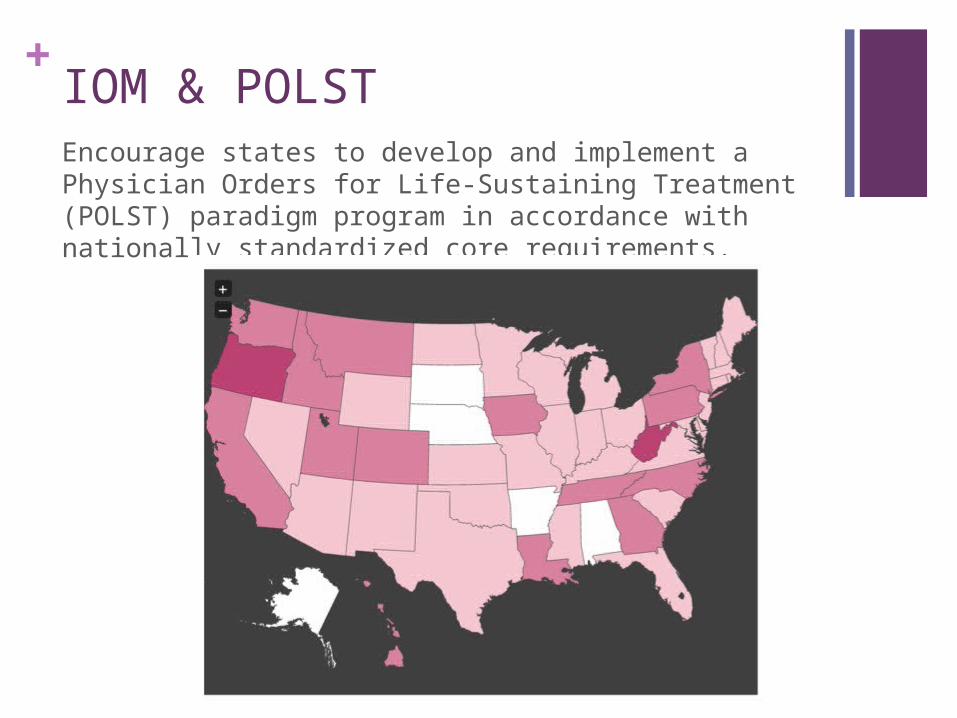
+IOM & POLSTEncourage states to develop and implement a Physician Orders for Life-Sustaining Treatment (POLST) paradigm program in accordance with nationally standardized core requirements.


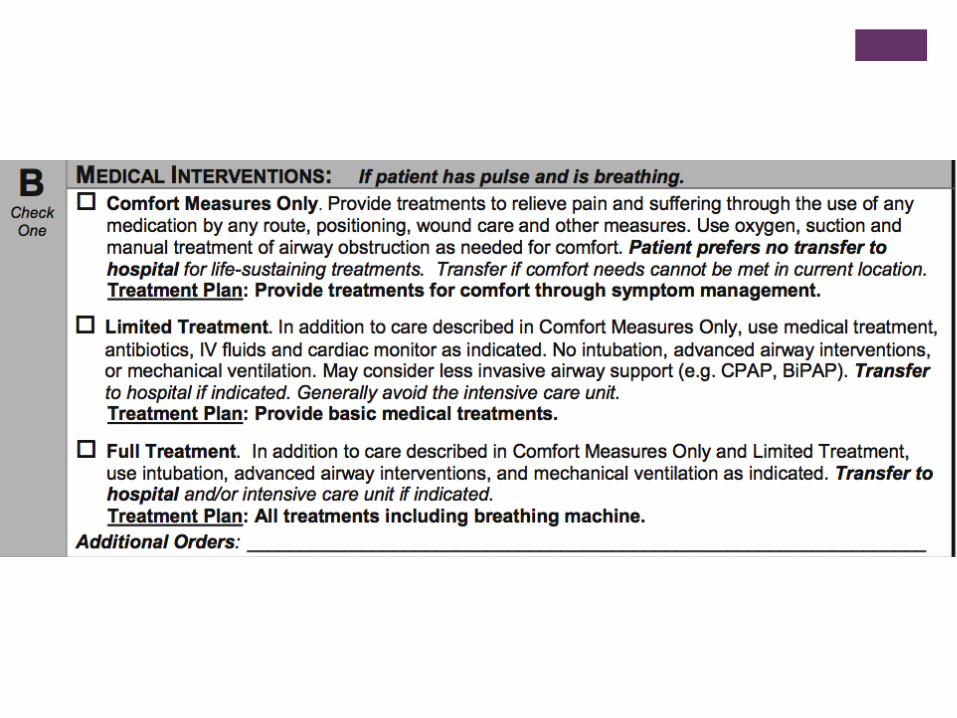

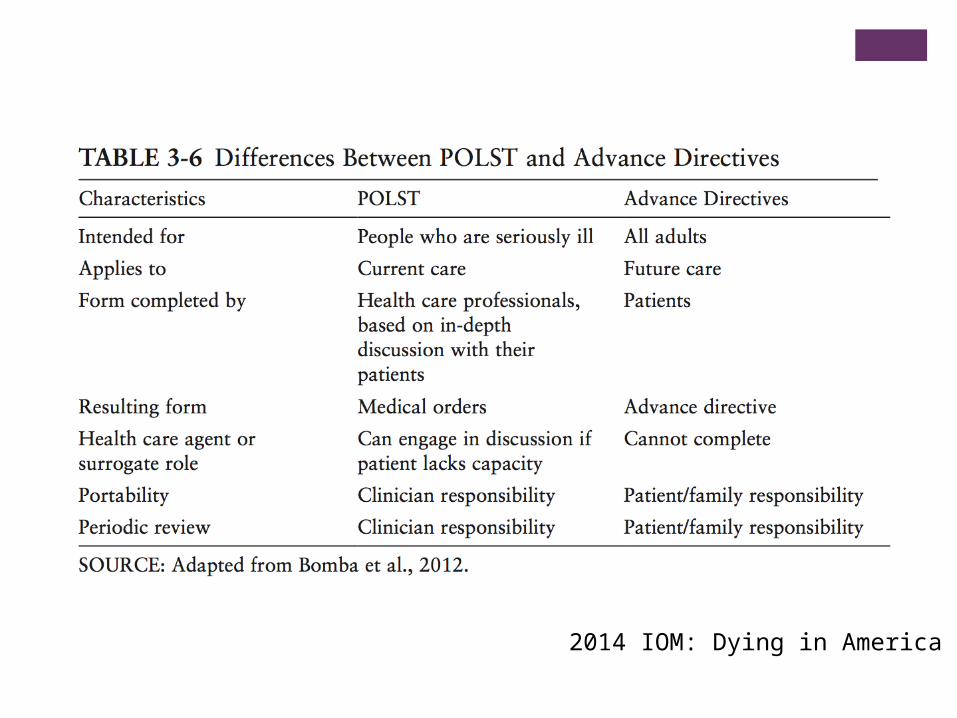
2014 IOM: Dying in America

+POLST & Oregon Experience
Fromme, 2014 studied Oregon deaths in 2010 & 2011
58,000 deaths; 31% had POLST form in registry
Scope of Treatment: 66% comfort measures only (CMO) 27% limited interventions 6% full treatment
Only 6% of CMO patients died in hospital vs 44% of full treatment patients 34% of those with no POLST form in registry

+POLST in Texas
Program not yet mature
No standard form

+Psychiatric Boarding




+Behavioral Health Care in EDs
Identified as one of top three challenges
Some EDs not well equipped to handle patients Cannot offer treatment or monitoring over time Exacerbate existing crowding issues
Community MH/SA resources insufficient
Access for uninsured & Medicaid pts

+WA Experience: Case
2013: 10 patients sue WA state for being involuntarily held in ED and acute care medical beds awaiting psychiatry care
WA-ACEP (and WSMA, WSHA, WSNA, W-ENA) filed amicus briefs in support
August 2014: state Supreme Court upholds
Difficult to uphold without violating EMTALA
SOURCE: Seattle TimesOctober 5th, 2013

+WA Experience: Results
$30 million in emergency funding of state psych hospital beds
Plan for 150 additional state funded beds
New certificate-of-need approvals for psych beds
Clear definition of “single bed” certifications
Future possibilities: Increased use of telemedicine Additional mental health resources

+Next Steps

+Contact: Alison [email protected]