!!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
12
REVIEW Phenotypes of childhood asthma: are they real? B. D. Spycher 1 , M. Silverman 2,3 and C. E. Kuehni 1 1 Swiss Paediatric Respiratory Research Group, Institute of Social and Preventive Medicine (ISPM), University of Bern, Bern, Switzerland, 2 Department of Infection, Immunity & Inflammation, The Leicester Children’s Asthma Centre, Division of Child Health, University of Leicester, Leicester, UK and 3 Department of Respiratory Medicine, Institute for Lung Health, University of Leicester, Leicester, UK Clinical & Experimental Allergy Correspondence: Claudia E. Kuehni, Institute of Social and Preventive Medicine, University of Bern, Finkenhubelweg 11, CH-3012 Bern, Switzerland. E-mail: [email protected] Cite this as : B. D. Spycher, M. Silverman and C. E. Kuehni, Clinical & Experimental Allergy , 2010 (40) 1130–1141. Summary It has been suggested that there are several distinct phenotypes of childhood asthma or childhood wheezing. Here, we review the research relating to these phenotypes, with a focus on the methods used to define and validate them. Childhood wheezing disorders manifest themselves in a range of observable (phenotypic) features such as lung function, bronchial responsiveness, atopy and a highly variable time course (prognosis). The underlying causes are not sufficiently understood to define disease entities based on aetiology. Nevertheless, there is a need for a classification that would (i) facilitate research into aetiology and pathophysiology, (ii) allow targeted treatment and preventive measures and (iii) improve the prediction of long-term outcome. Classical attempts to define phenotypes have been one- dimensional, relying on few or single features such as triggers (exclusive viral wheeze vs. multiple trigger wheeze) or time course (early transient wheeze, persistent and late onset wheeze). These definitions are simple but essentially subjective. Recently, a multi- dimensional approach has been adopted. This approach is based on a wide range of features and relies on multivariate methods such as cluster or latent class analysis. Phenotypes identified in this manner are more complex but arguably more objective. Although phenotypes have an undisputed standing in current research on childhood asthma and wheezing, there is confusion about the meaning of the term ‘phenotype’ causing much circular debate. If phenotypes are meant to represent ‘real’ underlying disease entities rather than superficial features, there is a need for validation and harmonization of definitions. The multi-dimensional approach allows validation by replication across different populations and may contribute to a more reliable classification of childhood wheezing disorders and to improved precision of research relying on phenotype recognition, particularly in genetics. Ultimately, the underlying pathophysiology and aetiology will need to be understood to properly characterize the diseases causing recurrent wheeze in children. What is a phenotype ? Childhood asthma, or wheezing disease, is highly variable in bot h its clinical pre sent ati on and time course [1]. Thr oug hou t the last century , there have been conflicting views of wheez- ing di sorders in ch ildhood as eit he r a gr ou p of sev er al discrete disease entities or a single although variable disease [2–6]. In particular, it was unclear whether wheezing asso- cia te d wi th rec urr en t re sp ira to ry inf ec tion in th e fir st ye ar s of life (wheezy bronchitis), is a precursor of asthma or whether it is a different disease [2–4, 7, 8]. In the past few decades, a growing numb er of cohort studies have documente d the natural history of these disorders in more detail, and results have been used to support one or the other view [2, 3, 9]. Currently, the prevailing paradigm is that asthma (and wheezing) in children consists of several discrete disease ent iti es or syndromes [1 0–13]. For lac k of a defi nite biological basis for disease heterogeneity – genetics or causal agent – classification has been based on pheno- types. Some phenotypic classifications such as that by the Tucson group into early transient, late onset and persis- tent wheeze [9] have found wide popularity. The number of publications containing the terms ‘phenotype’, ‘asthma or wheeze’ and ‘paediatric or child’ in Pubmed (excluding art icle s wit h ‘genetics’ as a key wor d, bec ause of the alt ernative use of the term phe notype) has inc reased steeply, from less than five publications annually until the mid-1990s to well over 40 in recent years (Fig. 1). EC doi: 10.1111/j.1365-2222.2010.03541.x Clinical & Experimen tal Allergy , 40, 1130–1141 c 2010 Blackwell Publishing Ltd
Transcript of !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 1/12
REVIEW
Phenotypes of childhood asthma: are they real?
B. D. Spycher1, M. Silverman2,3 and C. E. Kuehni1
1Swiss Paediatric Respiratory Research Group, Institute of Social and Preventive Medicine (ISPM), University of Bern, Bern, Switzerland, 2 Department of Infection,
Immunity & Inflammation, The Leicester Children’s Asthma Centre, Division of Child Health, University of Leicester, Leicester, UK and 3 Department of Respiratory
Medicine, Institute for Lung Health, University of Leicester, Leicester, UK
Clinical &Experimental
Allergy
Correspondence:
Claudia E. Kuehni, Institute of Social
and Preventive Medicine, University of
Bern, Finkenhubelweg 11, CH-3012
Bern, Switzerland.
E-mail: [email protected]
Cite this as : B. D. Spycher, M. Silverman
and C. E. Kuehni, Clinical &
Experimental Allergy , 2010 (40)
1130–1141.
Summary
It has been suggested that there are several distinct phenotypes of childhood asthma or
childhood wheezing. Here, we review the research relating to these phenotypes, with a focus
on the methods used to define and validate them. Childhood wheezing disorders manifest
themselves in a range of observable (phenotypic) features such as lung function, bronchial
responsiveness, atopy and a highly variable time course (prognosis). The underlying causes
are not sufficiently understood to define disease entities based on aetiology. Nevertheless,
there is a need for a classification that would (i) facilitate research into aetiology andpathophysiology, (ii) allow targeted treatment and preventive measures and (iii) improve the
prediction of long-term outcome. Classical attempts to define phenotypes have been one-
dimensional, relying on few or single features such as triggers (exclusive viral wheeze vs.
multiple trigger wheeze) or time course (early transient wheeze, persistent and late onset
wheeze). These definitions are simple but essentially subjective. Recently, a multi-
dimensional approach has been adopted. This approach is based on a wide range of features
and relies on multivariate methods such as cluster or latent class analysis. Phenotypes
identified in this manner are more complex but arguably more objective. Although
phenotypes have an undisputed standing in current research on childhood asthma and
wheezing, there is confusion about the meaning of the term ‘phenotype’ causing much
circular debate. If phenotypes are meant to represent ‘real’ underlying disease entities rather
than superficial features, there is a need for validation and harmonization of definitions. Themulti-dimensional approach allows validation by replication across different populations and
may contribute to a more reliable classification of childhood wheezing disorders and to
improved precision of research relying on phenotype recognition, particularly in genetics.
Ultimately, the underlying pathophysiology and aetiology will need to be understood to
properly characterize the diseases causing recurrent wheeze in children.
What is a phenotype?
Childhood asthma, or wheezing disease, is highly variable inboth its clinical presentation and time course [1]. Throughout
the last century, there have been conflicting views of wheez-
ing disorders in childhood as either a group of several
discrete disease entities or a single although variable disease
[2–6]. In particular, it was unclear whether wheezing asso-
ciated with recurrent respiratory infection in the first years of
life (wheezy bronchitis), is a precursor of asthma or whether
it is a different disease [2–4, 7, 8]. In the past few decades, a
growing number of cohort studies have documented the
natural history of these disorders in more detail, and results
have been used to support one or the other view [2, 3, 9].
Currently, the prevailing paradigm is that asthma (and
wheezing) in children consists of several discrete disease
entities or syndromes [10–13]. For lack of a definitebiological basis for disease heterogeneity – genetics or
causal agent – classification has been based on pheno-
types. Some phenotypic classifications such as that by the
Tucson group into early transient, late onset and persis-
tent wheeze [9] have found wide popularity. The number
of publications containing the terms ‘phenotype’, ‘asthma
or wheeze’ and ‘paediatric or child’ in Pubmed (excluding
articles with ‘genetics’ as a keyword, because of the
alternative use of the term phenotype) has increased
steeply, from less than five publications annually until
the mid-1990s to well over 40 in recent years (Fig. 1).
ECdoi: 10.1111/j.1365-2222.2010.03541.x Clinical & Experimental Allergy , 40, 1130–1141
c 2010 Blackwell Publishing Ltd

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 2/12
Currently, phenotypes have an undisputed standing in the
research on childhood asthma, and their existence is often
uncritically accepted. They are also increasingly used for
clinical decision making in treatment guidelines [14–18].
Despite this widespread usage, there is confusion about
what the term phenotype actually means. In particular, it
is unclear whether phenotypes are simply pragmatic
constructs or whether they have a more fundamental
meaning, standing for separate disease entities. This
matters: if they describe something real, the classification
should be harmonized so that it best represents the ‘true’
underlying entities. If, however, asthma phenotypes aremerely utilitarian, any classification may be valid.
As introduced by Johannsen and Shull early last
century [19–20], the term phenotype was intended to
characterize different ‘types’ of organisms distinguishable
by their observable characteristics such as their shape,
structure, size or colour. Today, the term ‘phenotype’ is
used in a variety of ways. To geneticists, a phenotype can
be any observable trait of an organism, such as its
morphology, biochemical or physiological properties or
behaviour, without assuming the existence of distinct
‘types’ (Table 1, row 1). In the literature on phenotypes of
wheezing illness, the meaning of the term is vague andrarely specified. Usage ranges from the view that pheno-
types are useful but entirely artificial constructs (Table 1,
row 2) to the belief that they represent underlying disease
entities that, like biological species, await discovery (Table
1, row 3).
Here, we adopt the view that phenotypes are hypothe-
sized disease entities but use the term more loosely when
reviewing some of the literature. To qualify as a disease
entity, we would require a condition to affect a significant
number of patients and be aetiologically distinguishable
from other conditions.
This review is a critical summary of past and current
approaches to categorizing children who wheeze into
phenotypes. In particular, we: (1) briefly describe child-
hood wheezing disease with its associated symptoms and
traits; (2) explain why it might be important to distinguish
phenotypes; (3) describe different methodological ap-
proaches to define phenotypes; (4) discuss methods for
validating phenotypes as true disease entities or at least
clinically useful constructs and (5) make some suggestions
for further research.
The clinical spectrum of wheezing disease and asthma –
where are the boundaries?
Wheezing disease in children manifests itself in a wide
spectrum of measurable features, including symptoms,signs and associated traits (Table 2). These features are
not the main focus of the present review and the list in
Table 2 is not exhaustive. Important, however, are the
following observations.
First, these features are associated with each other (i.e.
they are not independent) but the associations are modest.
For instance, children with wheeze will be more likely to
have bronchial hyperresponsiveness (BHR) than children
without wheeze. This means there are more children with
both wheeze and BHR than would be expected if these
features were independent that is, if each feature were
randomly distributed among all children regardless of thepresence of other features. However, quite surprisingly,
the overlap between the features is only moderately
greater than it would be assuming independence (Fig. 2)
[21, 22]. A consequence of this is that if the definition of
asthma or of an asthma phenotype requires the presence
of more than one of these features, group sizes quickly
become small. For instance, a phenotype requiring
wheeze, atopy and BHR would include only 7.3% of
children who have any one of these features (Fig. 2).
Second, the presence of these features, particularly
symptoms, varies by age [3, 23–25] and over short periods
0
10
20
30
40
50
1 9 8 0
1 9 8 5
1 9 9 0
1 9 9 5
2 0 0 0
2 0 0 5
2 0 1 0
Fig. 1. Annual tally of articles found in Pubmed using the terms
‘ phenotypà AND (wheez à OR asthma) AND (child à OR pediatric Ã)’ (all
terms searched in all fields, excluding articles with ‘genetics’ as a
keyword).
Table 1. Different usages of the term ‘phenotype’
Usage Description Example of usage
Any observable
trait (partial
phenotype)
Includes signs, symptoms,
measurements and
biological markers
Bronchial
hyperresponsiveness
[103], see also Table 2
Clinically useful
grouping
Defines groups that differ
with respect to features of
interest: e.g. risk factors,
response to treatment,
prognosis
Difficult or severe
asthma [104] see also
Tables 3 and 4
Hypothesized
disease entity
Defines a condition that is
thought to represent a
distinct disease entity
Atopic asthma and
virus-induced wheeze
[71] see also Tables 3
and 4
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
Wheezing phenotypes in childhood 1131

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 3/12
of time [26]. Third, many of the listed measurements are
costly, difficult to perform in infants and young children
or pose ethical problems. Bronchial biopsy is an example.
There is therefore a paucity of data on children that would
allow the interdependencies of these measurements and
their association with wheezing illness throughout child-
hood to be examined.Selection of the features defining asthma has been
much debated. While the diagnosis of asthma may be easy
to make in a patient with all the classical features of
asthma such as recurrent attacks of wheeze, reversible
airway obstruction, sensitization to aeroallergens and
bronchial hyperresponsiveness, it can be quite difficult in
patients who have only some of these features. In fact,
only a few features are necessary for a clinical diagnosis
of asthma in children and none are sufficient. At some
stage, the prevailing definition of asthma has required
recurrent wheeze, reversible airway obstruction, BHR and
airway inflammation as necessary elements [27]. The
current trend is again, as proposed decades ago by Dame
Turner–Warwick, towards a simpler more pragmatic defi-
nition (variable wheeze with no other identifiable causes
and responding to asthma treatment) [28, 29] requiring
only wheeze (or dry cough assuming that a cough-variant
form of asthma exists) and evidence of reversible airway
obstruction (including bronchodilator response) [18, 30].
Even these features may be absent during long, symptom-
free intervals. Other features such as atopy, BHR and
Table 2. Features of wheezing illness in children
Dimensions Features Diagnostic process
Symptoms Wheeze Self, parental or clinical
observationCough
Shortness of breath/
difficulty breathing/
chest tightness
Symptom history/age of
onset
Signs Expiratory polyphonic
wheeze
Physical examination
Barrel chest, etc.
Lung function Reversible airway
obstruction
Spirometry plus
bronchodilator response
Air flow variability Twice daily peak flow
meter/serial spirometry
Bronchial
responsiveness
Bronchial
hyperresponsiveness
Diverse direct and indirect
bronchial challenge
tests
Atopy Skin sensitivity Skin prick testsIncreased total IgE Serum IgE
Increased specific IgE RAST, ELISA
Blood eosinophilia Differential white cell
count
Airway
inflammation
Raised exhaled nitric
oxide fraction (FeNO)
FeNO measurement
Sputum eosinophilia
and/or other
inflammatory markers
Bronchoalveolar lavage,
sputum induction or
exhaled breath
Airway wall
inflammation and/or
remodelling
Bronchial biopsy
Response to
therapy
Bronchodilator response Spirometry
Corticosteroid
responsiveness
Treatment trial
Fig. 2. Venndiagramsshowingoverlap of the features wheeze, atopy and
bronchial hyperresponsiveness (BHR) in: (a) a real general population;
and (b) a hypothetical population in which these features have the same
prevalence but are totally independent. The prevalences ( pb) in (b) were
computed by multiplying the prevalences ( pa) of respective features in
the original real population with each other, e.g. pb(Current wheeze, BHR
but no atopy) = pa(Current wheeze)Â pa(BHR)Â(1À pa(atopy)). Source :
Unpublished data from the 1990 Leicester respiratory cohorts. Current
wheeze,Z1 episode of wheeze in the past 12 months; atopy,Z1 positive
skin prick test (dog, cat, grass or house dust mite); BHR, bronchial
hyperresponsiveness (lowest quintile of PC20).
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
1132 B. D. Spycher et al

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 4/12
measures of airway inflammation, although typical of
asthma, are often absent in children with clinically
relevant disease [31–33] and occur in many asymptomatic
children (Fig. 2).
Why distinguish phenotypes?
Ideally, we would like to define groups of patients that are
homogenous in their clinical features, risk factor profiles,
responses to treatment and prognoses. Such coherent
groups would greatly facilitate research and clinical
management by (A) improving precision in epidemiologi-
cal and clinical studies, (B) enabling targeted treatment
and preventive strategies and (C) improving the prediction
of long-term outcomes. The most coherent groups with
regard to these aspects are those representing different
underlying diseases (Table 1, row 3). If underlying biolo-
gical processes were clearly understood, precise diagnos-
tic markers could be used to define these groups. However,
in the absence of such gold standards, there is a need for a
phenotypic classification. Incidentally, even within a
well-characterized disease for which a diagnostic gold
standard exists, such as cystic fibrosis, there may be large
phenotypic variability and a need to define more homo-
genous subgroups.
(A) Improving precision in genetic and epidemiological studies
Poor phenotype definition has been recognized as one of
the main limitations for studying the genetics of asthma
[34–36]. The vast majority of genetic association studies
have used the broad category asthma (usually doctor diagnosed) as outcome [37] and only few studies [38, 39]
have focused on more specific phenotypes of childhood
wheezing. Causative genes discovered to date explain
only a small fraction of asthma heritability despite the
considerable investment in asthma genetic research
[40, 41]. Improved phenotype definition may help in
identifying the missing heritability [42].
Numerous studies have shown that phenotypes can
differ in their association with asthma risk factors [9, 33,
43–48]. Phenotypic differences in the outcomes used may
explain some of the contradictory findings from studies
relating to the effects of risk factors on the development of wheeze, such as breastfeeding [49], or exposure to pets
[50]. In the Tucson cohort, for instance, breastfeeding was
associated with a lower overall incidence of wheeze in the
first 2 years of life. However, breastfed children of atopic
mothers had an increased risk of recurrent wheeze at
age 6 [51].
(B) Improving treatment
Importantly for clinical practice, phenotypes can differ in
their response to treatment [52–54]. For instance, main-
tenance treatment with inhaled corticosteroids appears to
be more effective in children with risk factors for later
asthma than in children with intermittent wheezing [53].
Increasingly, asthma guidelines therefore recommend
phenotype-specific treatment [14–16, 55–58]. This might
be particularly important with regard to very severe
asthma. Patient selection becomes essential for cytokine-specific therapies such as monoclonal antibodies against
interleukin-5 [59, 60]. Although these therapies are cur-
rently mainly targeted at adults, future paediatric usage is
likely for children with very severe disease.
(C) Improving the prediction of long-term outcomes
Identifying phenotypes that would allow predicting long-
term disease outcome from an early age has been a long
sought goal. Phenotypes defined in early childhood have
been shown to differ markedly in their prognosis into later
childhood [61], adolescence [62] and adulthood [63, 64].
Even wheezing conditions that appear to be transient in
early childhood may be precursors of obstructive airway
disease in later life [65].
How are phenotypes defined?
Phenotype definitions have followed one of two
approaches. The first uses a single or few disease char-
acteristics to define phenotypes, here referred to as one-
dimensional. The second approach uses a wide range of
characteristics or disease dimensions, referred to as multi-
dimensional.
The one-dimensional approach
The common way to define phenotypes has been to
classify children with wheeze into groups based on simple
criteria involving one or few clinical features. Popular
criteria include triggers of wheezing episodes (or short-
term temporal pattern), severity of wheezing (usually
based on the frequency of episodes), or retrospective
symptom history since early childhood (long-term tem-
poral pattern) (Table 3). These phenotype definitions were
typically introduced in single cohort studies.
In the Melbourne cohort, one of the oldest respiratory cohort studies, children with wheeze at age 7 years were
divided into three groups based on frequency and triggers
of wheezing episodes in the past year: (1) ‘mild wheezy
bronchitis’ (less than five episodes, only associated with
apparent respiratory tract infection (RTI); (2) ‘wheezy
bronchitis’ (greater than or equal to five episodes, only
associated with RTI); and (3) ‘asthma’ (at least one episode
not associated with RTI) (Table 3, part D) [3]. Compared
with controls (asymptomatic at age 7) the groups 1–3 had
increasingly worse prognosis at later follow ups to the age
of 42 [64, 66, 67] leading to the conclusion that these
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
Wheezing phenotypes in childhood 1133

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 5/12
phenotypes represented varying grades of severity of the
same disease [3, 68, 69]. This ‘all is one’ disease concept
contradicted earlier claims that ‘wheezy bronchitis’ was a
separate disease, distinct from asthma, and propagated a
change in the treatment of ‘wheezy bronchitis’, from
antibiotics to inhaled bronchodilators and steroids.
In the early 1990s, Wilson and Silverman reintroduced
the hypothesis that several diseases exist within the
spectrum of wheezing disorders in childhood [4, 8, 26,
70]. They distinguished children who experience episodes
of wheeze only during viral RTI (exclusive viral wheeze)
from those who also wheeze between viral RTI, i.e. have
interval symptoms (multiple-trigger wheeze) and re-
viewed evidence showing that these groups differ in many
aspects, including association with atopy, measures of
bronchial inflammation, response to treatment and long-
term prognosis (Table 3, part A) [71, 72]. This phenotype
classification has been applied in different cohort studies
[65, 73, 74] and has recently been recommended as an aid
for treatment decisions [15].
In the mid-1990s, the Tucson group introduced a
classification of children based on retrospective symptom
Table 3. Summary of frequently used phenotypes of childhood wheeze and asthma
Labels Synonyms Definitions
Related but not
synonymous labels Published associations
(A) Triggers/short-term temporal pattern
Exclusive viral wheeze
[4, 71, 72]
Episodic (viral) wheeze [15]
Recurrent bronchiolitis
(USA)
Wheezy bronchitis [3]
Episodes of wheeze only
during viral RTI
Non-atopic wheeze
Early transient wheeze
Risk factors [26, 96]
Other clinical features [3]
Gene expression [93]
Prognosis [64–66, 73]
Response to treatment
[52, 53]
Multiple trigger wheeze [26] Asthma [3]
Chronic wheeze
Wheeze during but also
apart from viral RTI
Atopic asthma
(B) Long-term temporal pattern
Early transient wheeze [9] Wheeze only during the
first 3 years of life with
remission
Exclusive viral wheeze
Episodic viral wheeze
Risk factors [9, 25, 43–48,
77, 81, 82, 94, 95,
105–107]
Other clinical features
[9, 32, 44, 45, 77]
Prognosis [62, 63]
Persistent wheeze [9] Persistent early onset
wheezing
Wheeze during the first 3
years of life persisting
into school-age
Non-atopic persistent
wheeze (GINA) [30]
Intrinsic asthma
Late-onset wheeze [9] Wheeze beginning after 3
years of age
Multiple trigger wheeze
Atopic wheeze/asthma
Extrinsic asthma(C) Atopy
Non-atopic wheeze/asthma Intrinsic asthma [108]
Non-atopic persistent
wheeze [109]
Wheeze/reversible airflow
obstruction without
allergic sensitization
Exclusive viral-induced
wheeze
In older children/adults:
Exercise-induced asthma
Drug-induced asthma
Risk factors [97, 110–112]
Other clinical features [97]
Prognosis [63, 95]
Response to treatment [113]
Atopic wheeze/asthma Extrinsic asthma [108]
Atopic persistent wheeze
[109]
Wheeze/reversible airflow
obstruction with allergic
sensitization
Multiple trigger wheeze
(D) Severity
Childhood wheeze (e.g.
Melbourne cohort [3])
Childhood asthma Childhood wheeze as a
single disorder varying
by degrees of severity
Grades defined by number
of episodes, and
association or not with
RTI
Asthma Risk factors [114]
Other clinical features [3]
Prognosis [3, 64, 66, 67, 114]
Response to treatment [115]
Asthma (e.g. GINA [30]) Asthma as a single disorder
varying by degrees of
severity
Grades defined by
frequency of symptoms,
or lung function deficit
RTI, respiratory tract infection.
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
1134 B. D. Spycher et al

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 6/12
history in the first 6 years of life into ‘transient early
wheezing’ (wheeze in first 3 years of life but no wheeze at
6 years), ‘late-onset wheezing’ (no wheeze until age 3
years of life, but wheeze at 6 years) and ‘persistent
wheezing’ (wheeze both before age 3 and at age 6) (Table
3, part B) [9]. As this classification is based on retro-
spective symptom history at the age of 6, it cannot be usedto guide treatment decisions for younger children. How-
ever, it has become the most widely used model in
epidemiological studies [25, 43–46, 75–82].
Pros and cons of the one-dimensional approach
The obvious advantage of one-dimensional phenotype
definitions is that they are simple. If they are useful,
simple phenotypic definitions are preferable to complex
ones in both clinical and epidemiological settings. More
questionable is whether they represent underlying disease
entities. It is possible, but unlikely, that disease processes
specifically affect only one or a few clinical features. And
clearly, selecting only a few features from among many to
define the phenotypes requires subjective choices.
Including more features as necessary components of
asthma phenotypes is difficult because this results in
smaller groups. For instance, if all combinations of only
three dichotomous features, say age of onset (late, early),
persistence (transient, persistent) and triggers (only with,
also without RTI), are considered, eight separate pheno-
types result. With four dichotomous features 16 pheno-
types result and so on. Of course, some of these groups
could be combined, but the choice of which ones to
combine is again subjective. To include more features, weneed a classification that is less rigid and does not require
arbitrary selection.
The multi-dimensional approach
The multi-dimensional approach attempts to include a
wide range of features (Table 2) in the definition of
phenotypes. This approach was recently proposed by
Wardlaw et al. [83] as a means to develop a new taxonomy
of asthma and airways disease in general. The authors
suggested the use of cluster analysis, a group of techni-
ques that seek to organize the subjects of a multivariatedataset into relatively homogenous groups. Such methods
allow phenotypes to be identified in a data-driven manner
and might therefore minimize the subjectivity involved in
selecting the features [61, 83–85].
Haldar and colleagues applied cluster analysis to three
independent adult asthma populations using measure-
ments of symptoms, atopy, eosinophilic inflammation,
psychological status and variable airflow obstruction
[84]. In each dataset, they identified three or four clusters,
two of which showed a feature profile that was consistent
over the three populations. We recently used latent class
analysis (LCA), a type of cluster analysis based on a formal
statistical model to identify phenotypes of childhood
wheeze using data from a cohort study in Leicester, UK
(skin prick tests, airway responsiveness, lung function
and repeated assessment of symptoms of wheeze and
cough) [61, 85]. The model distinguished two phenotypes
of chronic cough, a persistent and a transient form, andthree phenotypes of wheeze, a transient form associated
with viral infections, a persistent form associated with
other triggers, and a non-atopic but mostly persistent
form (Fig. 3). Recently Clarisse and colleagues used a
different clustering method (partitioning around medoids)
to identify phenotypes of bronchial obstructive symptoms
in infants from the Paris birth cohort [86]. Two sympto-
matic groups emerged, one characterized by dyspnoea
with sleep disturbance and the other by nocturnal dry
cough.
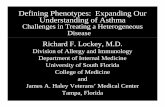
Using data from the Avon Longitudinal Study of
Parents and Children (ALSPAC), Henderson and colleagues
applied LCA to seven repeated assessments of current
wheeze during the first 6 years of life [76], thus refining
the approach from the Tucson group. Their approach was
essentially one-dimensional because it included only one
feature (the occurrence of wheeze attacks) measured at
different points. However, the phenotypes were derived in
data-driven manner from the symptom histories of a large
number of children from the general population
(n = 6265). The analysis identified five types of longitudi-
nal trajectories distinguished by age at onset and persis-
tence of symptoms (Fig. 4).
Multivariate techniques can also be used to model
variability along a continuum rather than by discretephenotypes. A commonly used method is factor analysis,
which assumes that the observed features are related
through one or few unobserved continuous variables,
called factors. Features that are highly correlated with
each other contribute to the same factor and the factor
becomes a composite measure of these features. Several
studies have applied factor analysis and related methods
to data on wheezing and asthma in childhood [87–89].
Pros and cons of the multi-dimensional approach
The main advantage of the multi-dimensional approach is
that it attempts to involve all features of the disease
without making presumptions about which features are
the most distinguishing ones. Proponents argue that
resulting phenotypes might better reflect underlying dis-
ease entities as they are defined in a more objective
manner using information contained in the data [61, 76,
84, 85]. However, these methods are not entirely objective
because the investigator needs to make choices about
which particular method to use and which variables to
include.
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
Wheezing phenotypes in childhood 1135

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 7/12
A disadvantage is that the resulting phenotypes are not
defined by a simple combination of features. The pheno-
type of a particular group identified by cluster analysis is
defined by the characteristic features of this group. Such a
definition is more like a description, and cannot be
reduced to a single feature. For example, a phenotype
might be characterized by a tendency for early onset of
wheeze, usually persisting into the school age or later,
with attacks usually occurring not only during colds but
also apart from colds. This type of ‘soft’ definition may
resemble processes going on in the minds of clinicianswho combine multi-dimensional observations to make a
clinical diagnosis.
Validating phenotypes as real clinical entities
If phenotypes were visible objects, then their existence
and characteristics would be undisputed. However, we still
lack such a gold standard against which phenotypes could
be validated. Because the underlying disease process is not
fully understood, it is not possible to prove that a
particular phenotype classification correctly represents it.
Therefore, rather than proofs, other indications that phe-
notypes could represent disease entities are sought. Such
indications include whether disease phenotypes (a) are
associated with features not used to define them (usually
physiological measurements), (b) predict future outcomes,
(c) have distinctive risk factors, (d) have specific responses
to treatment, (e) are stable over time or (f) are consistent
across populations.
A large number of studies have tested whether different
phenotypes (varyingly defined) of wheezing or asthma in
children are differently associated with concurrent or later physiological measurements (e.g. lung function, bronchial
responsiveness, atopy and airway inflammation) [3, 9, 23,
32, 33, 44, 45, 47, 68, 69, 76, 77, 90–93], with distinctive
risk factors [9, 23, 25, 33, 43–46, 48, 81, 82, 94–96], with
later disease outcomes (prognosis) [61–66, 73] or with
response to treatment [52–54] (Table 3). A general rule is
that features used to define phenotypes cannot be used for
validation, meaning that for phenotypes defined by a
multi-dimensional approach fewer features remain for
this purpose (Table 4). However, the multi-dimensional
approach accounts for associations existing between many
of the features in the process of phenotype definition. Validating phenotypes by testing for associations with
other features can be misleading. If, for example, the
phenotype-persistent wheezing is associated with a ma-
ternal history of asthma [9] while the transient phenotype
is not [9, 82], this does not mean that the phenotypic
distinction transient vs. persistent is superior to other
distinctions. Other classifications, for instance by atopy
[97] or by triggers [26], produce similar results. The
question should rather be whether certain phenotype
classifications predict the presence of features (earlier,
concurrent or later) better than other classifications. Such
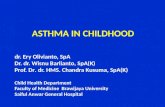
319(100)
208(65.2)
111(34.8)
159(49.8)
97(30.4)
63(19.7)
86(27.0)
86(27.0)
84(26.3)
63(19.7)
97(30.4)
82(25.7)
58(18.2)
47(14.7)
35(11.0)
Persistentcough
Transientcough
Atopicpersistent
wheeze
Non−atopicpersistent
Transientviral
wheeze
Fig. 3. Formation of phenotypes in a study of symptomatic children by
Spycher et al. [61]: Phenotypes were identified from multivariate data
including repeated symptom measurements, atopy, lung function and
BHR using latent class analysis. The branching between layers shows
how children are redistributed to new phenotypes as the number of
phenotypes in the model is increased. Box widths are proportional to
numbers of children assigned to the phenotypes (number and percentage
reported). A model with five phenotypes (bottom layer) was selected
based on statistical criteria but the branchingpattern shows that essential
differences between these phenotypes were identified in earlier stages.
The phenotypes of the final model are labelled according to their main
distinctive characteristics. Data are presented as n (%). Adapted from
Spycher BD et al. [61] with permission from European Respiratory
Society Journals Ltd.
Fig. 4. Developmental trajectories in six phenotypes of wheezing identi-
fied by Henderson et al. [76]: estimated prevalence of wheezing at each
time-point from birth to 81 months for each of the six wheezing
phenotypes identified by latent class analysis in 6265 children with
complete data on wheezing in the past 12 months over seven sequential
surveys. Reproduced from Henderson J et al. [76] with permission from
BMJ Publishing Group Ltd.
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
1136 B. D. Spycher et al

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 8/12
comparisons could be made using statistics such as
sensitivity, specificity or the likelihood ratio [98]. Because
this is rarely, if ever, done the observed associations, even
if well replicated across different studies, do not provide
support for any particular phenotypic classification over
the others.
Recently, a study investigated whether children with a
certain phenotype continued to have the same phenotype
at a later time-point, i.e. whether phenotypes were stable
over time [99]. One would expect phenotypes representing
actual diseases to persist for the duration of these diseases.
However, given the possibility of remission and relapse itis unclear over how long a period a phenotype should be
stable. Also, stability may be an artefact of phenotype
definition. For instance, a phenotype defined by the
wheezing pattern of the past year is by definition stable
over 1 year. The Tucson classification is necessarily stable
over the first 6 years of life because it is based on the
symptom history of this period.
A possibility for validating phenotypes identified by
data-driven methods is the replication of results in differ-
ent datasets. For instance, Haldar et al. [84] found similar
results of the same clustering method across three popula-
tions. Phenotypes reflecting true biological entities shouldreappear in a similar form in different populations. Such
comparisons are complicated by differences in study
design, such as differences in the age when children were
examined or in features assessed. ‘True’ phenotypes may,
however, be robust against such differences.
The way forward
In spite of its popularity, the meaning of the term
‘phenotype’, as used in the context of childhood asthma,
is vague and rarely specified. It is usually unclear whether
phenotypes are simply practical definitions or are in-
tended to represent real entities. Stating this clearly could
avoid much confusion and circular debate. If phenotypes
are just useful definitions, for instance because they are
associated with different response to treatment, then only
their usefulness needs to be shown, not whether or not
they represent real diseases. If, on the other hand, pheno-
types are thought to be real, then there is a need for
validation and for harmonization of definitions. Cur-
rently, there is a wide range of concepts among clinicians
[13] and among researchers. Despite numerous validation
studies, no phenotype model stands out as more valid thanothers.
In future, multi-dimensional approaches to phenotype
definition could complement the traditional one-dimen-
sional approach. Multi-dimensional approaches allow to
include more disease features and to define phenotypes
that can be validated across populations. They could be
used to assess the importance of the defining features of
traditional phenotypes in context with other features. For
instance, in the three wheezing phenotypes identified in
our study using LCA, both triggers and the persistence of
symptoms, the defining features of the popular classifica-
tions by the Tucson group and by Silverman and collea-gues, were important in conjunction with other features
such as atopy and BHR [61]. Such additional features
could be incorporated into traditional classifications. This
will require ‘softer’ and more complex definitions, for
instance, using decision trees or a probabilistic assign-
ment of children to phenotypes.
Different phenotypes may be needed for clinical prac-
tice and for research. One size is not likely to fit all. From
the clinician’s perspective, phenotypes should be clini-
cally useful and preferably simple. They need to be
relevant for treatment decisions or prognosis and be
Table 4. Variables used to define phenotypes or analysed for association with phenotypes (validation) in different studies
Disease variables or dimensions Description Used for phenotype definition
Examined for associations
with phenotypes
Aetiology Environmental risk factors
Genetics
Martinez et al. [9]
Silverman [26]
Disease characteristics Symptoms
Signs
Pathophysiology
Short-term time course
Silverman [26, 116]Ã
Spycher et al. [61]z‰
Martinez et al. [9]
Henderson et al. [76]
Long-term time course Previous time course (symptom
history)
Martinez et al. [9]w
Henderson et al. [76]z
Spycher et al. [61]z‰
Subsequent time course
(prognosis)
Martinez [62, 63]
Spycher et al. [61]
ÃTable 3, row A.
wTable 3, row B.
zData-driven definition using latent class analysis.
‰Multi-dimensional approach.
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
Wheezing phenotypes in childhood 1137

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 9/12
defined using readily accessible clinical information (fa-
mily and patient history, symptoms, signs and simple
measurements). Symptom control may be similar in dif-
ferent patients even if the symptoms have different under-
lying causes. In research, however, the main focus is the
underlying disease processes and their mechanisms. Hav-
ing phenotypes that are specific for the main underlyingdisease processes can greatly improve the precision of
research into mechanisms and causes.
The importance of precise phenotype definitions is
becoming increasingly clear in genetic research. Pheno-
types of childhood wheezing have rarely been used in
genetic association studies although they may reflect
important susceptibilities to respiratory disease through-
out life [63–65]. A question that should be addressed is
whether phenotypic variability between children is better
represented by discrete groups (distinct phenotypes) or by
a continuum (one or more continuous factors). This is
important because if children are categorized into discrete
groups when in fact they lie along a single continuum,
information is lost and statistical power to detect genetic
associations is reduced [100, 101]. A study by the Tucson
group demonstrated stronger associations between a con-
tinuous score of atopy obtained by factor analysis with
specific genetic markers than with individual dichoto-
mous results of skin tests [87]. Using a cross-sectional
dataset, we determined whether a model with continuous
factors or one with discrete groups better represented
variability of parent-reported symptoms. Preliminary re-
sults [102] point to a continuum of disease rather than to
discrete phenotypes; however, further work is required to
see whether the inclusion of time course and objectivemeasurements might reveal discrete patterns.
Ultimately, only knowledge of genetic and environ-
mental determinants and pathophysiological pathways
can reveal the true nature of the diseases causing recur-
rent wheeze in children. Reaching this goal is an iterative
process: better phenotype definitions increase the preci-
sion of research into causes and mechanisms, while a
better understanding of the underlying processes leads to
more meaningful labels, until eventually new diseases
might be defined based on aetiology. In this process, we
may need to discard old distinctions and possibly even
shift our focus away from wheezing as the cardinalsymptom. Like all hypotheses, current phenotypes will
eventually be superseded. In the meantime, we should
treat phenotypes as exactly that: the best current working
hypotheses.
Acknowledgements
The authors would like to thank: all the children and
families participating in Leicestershire cohort studies for
contributing data; Urs Frey and Philip Latzin for critical
discussions on this topic; and Lutz Dumbgen, John
Thompson and Marie Pierre Strippoli for their methodo-
logical and technical support in our work on phenotypes
of wheeze.
Funding:
The work was supported by Asthma UK (grant 07/048)
and the Swiss National Science Foundation (PROSPER
grant 3233-069348 and 3200-069349, and SNF grant823B - 046481).
Competing interests:
There are no competing interests.
References
1 Silverman M. Childhood asthma and other wheezing disorders.
London: Arnold, 2002.
2 Boesen I. Asthmatic bronchitis in children; prognosis for 162
cases, observed 6–11 years. Acta Paediatr 1953; 42:87–96.
3 Williams H, McNicol KN. Prevalence, natural history, and
relationship of wheezy bronchitis and asthma in children. Anepidemiological study. BMJ 1969; 4:321–5.
4 Silverman M. Out of the mouths of babes and sucklings: lessons
from early childhood asthma. Thorax 1993; 48:1200–4.
5 Silverman M, Wilson N. Asthma – time for a change of name?
Arch Dis Child 1997; 77:62–4.
6 The Lancet. A plea to abandon asthma as a disease concept.
Lancet 2006: 368–705.
7 Sporik R, Holgate ST, Cogswell JJ. Natural history of asthma in
childhood – a birth cohort study. Arch Dis Child 1991;
66:1050–3.
8 Wilson NM. The significance of early wheezing. Clin Exp
Allergy 1994; 24:522–9.
9 Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M,Morgan WJ. Asthma and wheezing in the first six years of life.
N Engl J Med 1995; 332:133–8.
10 Saglani S, Bush A. Asthma in preschool children: the next
challenge. Curr Opin Allergy Clin Immunol 2009; 9:141–5.
11 Henderson J, Granell R, Sterne J. The search for new asthma
phenotypes. Arch Dis Child 2009; 94:333–6.
12 Castro-Rodriguez JA, Garcia-Marcos L. Wheezing and asthma
in childhood: an epidemiology approach. Allergol Immuno-
pathol (Madrid) 2008; 36:280–9.
13 Spycher BD, Silverman M, Barben J et al. A disease model for
wheezing disorders in preschool children based on clinicians’
perceptions. PLoS One 2009; 24:e8533.
14 Gold DR, Fuhlbrigge AL. Inhaled corticosteroids for young
children with wheezing. N Engl J Med 2006; 354:2058–60.
15 Brand PL, Baraldi E, Bisgaard H etal. Definition, assessment and
treatment of wheezing disorders in preschool children: an
evidence-based approach. Eur Respir J 2008; 32:1096–110.
16 Kuehni CE. Phenotype specific treatment of obstructive airways
disease in infancy and childhood: new recommendations of the
Swiss Paediatric Pulmonology Group. Swiss Med Wkly 2005;
135:95–100.
17 Global Initiative for Asthma (GINA) Global strategy for the
diagnosis and management of asthma in children 5 years
and younger, 2009. Available at http://www.ginasthma.org
(accessed 22 October 2009).
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
1138 B. D. Spycher et al

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 10/12
18 British Thoracic Society (BTS). British guideline on the manage-
ment of asthma. Thorax 2008; 63 (Suppl. 4):iv1–121.
19 Johannsen W. The genotype conception of heredity. Am Nat
1911; 45:129–5.
20 Shull GH. ‘‘PHENOTYPE’’ and ‘‘CLONE’’. Science 1912; 35:
182–3.
21 Guerra S. Asthma and chronic obstructive pulmonary disease.
Curr Opin Allergy Clin Immunol 2009; 9:409–16.
22 Sherrill DL, Guerra S, Cristina Minervini M, Wright AL,
Martinez FD. The relation of rhinitis to recurrent cough
and wheezing: a longitudinal study. Respir Med 2005; 99:
1377–85.
23 Sears MR, Greene JM, Willan AR et al. A longitudinal, popula-
tion-based, cohort study of childhood asthma followed to
adulthood. N Engl J Med 2003; 349:1414–22.
24 Brooke AM, Lambert PC, Burton PR, Clarke C, Luyt DK, Simpson
H. The natural history of respiratory symptoms in preschool
children. Am J Respir Crit Care Med 1995; 152:1872–8.
25 Matricardi PM, Illi S, Gruber C et al. Wheezing in childhood:
incidence, longitudinal patterns and factors predicting persis-
tence. Eur Respir J 2008; 32:585–92.26 Wilson NM, Dore CJ, Silverman M. Factors relating to the
severity of symptoms at 5 yrs in children with severe wheeze
in the first 2 yrs of life. Eur Respir J 1997; 10:346–53.
27 International consensus report on diagnosis and treatment of
asthma, 1992, 1–5.
28 Turner-Warwick M. Respiratory tract disease. Diagnosis and
management of asthma. Br Med J 1966; 1:403–4.
29 Turner-Warwick M. Recent advances in asthma. Trans Med Soc
Lond 1972; 88:198–204.
30 Global Initiative for Asthma (GINA). Global strategy for asthma
management and prevention, 2008 (update). Available at
http://www.ginasthma.org (accessed on 22 October 2009).
31 Stein RT, Holberg CJ, Morgan WJ et al. Peak flow variability,methacholine responsiveness and atopy as markers for detect-
ing different wheezing phenotypes in childhood. Thorax 1997;
52:946–52.
32 Martinez FD, Stern DA, Wright AL, Taussig LM, Halonen M.
Differential immune responses to acute lower respiratory illness
in early life and subsequent development of persistent wheez-
ing and asthma. J Allergy Clin Immunol 1998; 102:915–20.
33 Kurukulaaratchy RJ, Fenn M, Matthews S, Arshad SH. Char-
acterisation of atopic and non-atopic wheeze in 10 year old
children. Thorax 2004; 59:563–8.
34 Koppelman GH, Meijer GG, Postma DS. Defining asthma in
genetic studies. Clin Exp Allergy 1999; 29 (Suppl. 4):1–4.
35 Vercelli D. Discovering susceptibility genes for asthma and
allergy. Nat Rev Immunol 2008; 8:169–82.
36 Guerra S, Martinez FD. Asthma genetics: from linear to multi-
factorial approaches. Annu Rev Med 2008; 59:327–41.
37 Ober C, Hoffjan S. Asthma genetics 2006: the long and winding
road to gene discovery. Genes Immun 2006; 7:95–100.
38 Simpson A, Maniatis N, Jury F et al. Polymorphisms in a
disintegrin and metalloprotease 33 (ADAM33) predict impaired
early-life lung function. Am J Respir Crit Care Med 2005;
172:55–60.
39 Goetghebuer T, Isles K, Moore C, Thomson A, Kwiatkowski D,
Hull J. Genetic predisposition to wheeze following respiratory
syncytial virus bronchiolitis. Clin Exp Allergy 2004; 34:801–3.
40 Los H, Postmus PE, Boomsma DI. Asthma genetics and inter-
mediate phenotypes: a review from twin studies. Twin Res
2001; 4:81–93.
41 Weiss ST, Raby BA, Rogers A. Asthma genetics and genomics
2009. Curr Opin Genet Dev 2009; 19:279–82.
42 Manolio TA, Collins FS, Cox NJ et al. Finding the missing
heritability of complex diseases. Nature 2009; 461:747–53.
43 Sherriff A, Peters TJ, Henderson J, Strachan D, Team AS. Risk
factor associations with wheezing patterns in children followed
longitudinally from birth to 3 (1/2) years. Int J Epidemiol 2001;
30:1473–84.
44 Lowe LA, Simpson A, Woodcock A, Morris J, Murray CS,
Custovic A. Wheeze phenotypes and lung function in preschool
children. Am J Respir Crit Care Med 2005; 171:231–7.
45 Lau S, Illi S, Sommerfeld C et al. Transient early wheeze is not
associated with impaired lung function in 7-yr-old children.
Eur Respir J 2003; 21:834–41.
46 Midodzi WK, Rowe BH, Majaesic CM, Saunders LD, Senthilsel-
van A. Predictors for wheezing phenotypes in the first decade of
life. Respirology 2008; 13:537–45.
47 Kurukulaaratchy RJ, Fenn MH, Waterhouse LM, Matthews SM,Holgate ST, Arshad SH. Characterization of wheezing pheno-
types in the first 10 years of life. Clin Exp Allergy 2003; 33:
573–8.
48 Rusconi F, Galassi C, Corbo GM et al. Risk factors for early,
persistent, and late-onset wheezing in young children. SIDRIA
Collaborative Group. Am J Respir Crit Care Med 1999;
160:1617–22.
49 Duncan JM, Sears MR. Breastfeeding and allergies: time for a
change in paradigm? Curr Opin Allergy Clin Immunol 2008;
8:398–405.
50 Takkouche B, Gonzalez-Barcala FJ, Etminan M, Fitzgerald M.
Exposure to furry pets and the risk of asthma and allergic
rhinitis: a meta-analysis. Allergy 2008; 63:857–64.51 Wright AL, Holberg CJ, Taussig LM, Martinez FD. Factors
influencing the relation of infant feeding to asthma and
recurrent wheeze in childhood. Thorax 2001; 56:192–7.
52 McKean M, Ducharme F. Inhaled steroids for episodic viral wheeze
of childhood. Cochrane Database Syst Rev 2000; 2:001107.
53 Kaditis AG, Winnie G, Syrogiannopoulos GA. Anti-inflamma-
tory pharmacotherapy for wheezing in preschool children.
Pediatr Pulmonol 2007; 42:407–20.
54 Castro-Rodriguez JA, Rodrigo GJ. Efficacy of inhaled corticos-
teroids in infants and preschoolers with recurrent wheezing and
asthma: a systematic review with meta-analysis. Pediatrics
2009; 123:e519–525.
55 Bush A. Phenotype specific treatment of asthma in childhood.
Paediatr Respir Rev 2004; 5:S93–101.
56 Frey U, von Mutius E. The challenge of managing wheezing in
infants. N Engl J Med 2009; 360:2130–3.
57 Bacharier LB, Boner A, Carlsen KH et al. Diagnosis and treat-
ment of asthma in childhood: a PRACTALL consensus report.
Allergy 2008; 63:5–34.
58 Wolthers OD. Anti-inflammatory treatment of asthma:
differentiation and trial-and-error. Acta Paediatr 2009; 98:
1237–41.
59 Haldar P, Brightling CE, Hargadon B et al. Mepolizumab and
exacerbations of refractory eosinophilic asthma. N Engl J Med
2009; 360:973–84.
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
Wheezing phenotypes in childhood 1139

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 11/12
60 Nair P, Pizzichini MM, Kjarsgaard M et al. Mepolizumab for
prednisone-dependent asthma with sputum eosinophilia. N
Engl J Med 2009; 360:985–93.
61 Spycher BD, Silverman M, Brooke AM, Minder CE, Kuehni CE.
Distinguishing phenotypes of childhood wheeze and cough
using latent class analysis. Eur Respir J 2008; 31:974–81.
62 Morgan WJ, Stern DA, Sherrill DL et al. Outcome of asthma and
wheezing in the first six years of life: follow-up through
adolescence. Am J Respir Crit Care Med 2005; 172:1253–8.
63 Stern DA, Morgan WJ, Halonen M, Wright AL, Martinez FD.
Wheezing and bronchial hyper-responsiveness in early child-
hood as predictors of newly diagnosed asthma in early adult-
hood: a longitudinal birth-cohort study. Lancet 2008;
372:1058–64.
64 Horak E, Lanigan A, Roberts M et al. Longitudinal study of
childhood wheezy bronchitis and asthma: outcome at age 42.
BMJ 2003; 326:422–3.
65 Edwards CA, Osman LM, Godden DJ, Douglas JG. Wheezy
bronchitis in childhood: a distinct clinical entity with lifelong
significance? Chest 2003; 124:18–24.
66 Oswald H, Phelan PD, Lanigan A, Hibbert M, Bowes G, Olinsky A. Outcome of childhood asthma in mid-adult life. BMJ 1994;
309:95–6.
67 Phelan PD, Robertson CF, Olinsky A. The Melbourne Asthma
Study: 1964–1999. J Allergy Clin Immunol 2002; 109:189–94.
68 McNichol KN, Macnicol KN, Williams HB. Spectrum of asthma
in children. I. Clinical and physiological components. BMJ
1973; 4:7–11.
69 McNichol KN, Williams HE. Spectrum of asthma in children. II.
Allergic components. BMJ 1973; 4:12–6.
70 Silverman M. Childhood asthma and other wheezing disorders .
London: Chapman & Hall, 1995.
71 Silverman M, Grigg J, Mc Kean M Virus-induced wheeze in
young children – a separate disease? In: Johnston S, Papado-poulos N, eds. Respiratory infections in allergy and asthma. New
York: Marcel Dekker, 2002; 427–71.
72 Grigg J, Silverman M. Wheezing disorders in young children:
one disease or several phenotypes? In: Frey U, Gerritsen J , eds.
Respiratory diseases in infants and children. European Respira-
tory Monthly, 2006; 153–69.
73 Godden DJ, Ross S, Abdalla M et al. Outcome of wheeze in
childhood symptoms and pulmonary function 25 years later.
Am J Respir Crit Care Med 1994; 149:106–12.
74 Kuehni CE, Davis A, Brooke AM, Silverman M. Are all wheezing
disorders in very young (preschool) children increasing in
prevalence? Lancet 2001; 357:1821–5.
75 Young S, Arnott J, O’Keeffe PT, Le Souef PN, Landau LI. The
association between early life lung function and wheezing
during the first 2 yrs of life. Eur Respir J 2000; 15:151–7.
76 Henderson J, Granell R, Heron J et al. Associations of wheezing
phenotypes in the first 6 years of life with atopy, lung function
and airway responsiveness in mid-childhood. Thorax 2008;
63:974–80.
77 Melen E, Kere J, Pershagen G, Svartengren M, Wickman M.
Influence of male sex and parental allergic disease on child-
hood wheezing: role of interactions. Clin Exp Allergy 2004;
34:839–44.
78 Jedrychowski W, Perera FP, Jankowski J et al. Early wheezing
phenotypes and cognitive development of 3-yr-olds. Commu-
nity-recruited birth cohort study. Pediatr Allergy Immunol
2009; 21:550–6.
79 Jedrychowski W, Perera FP, Maugeri U et al. Length at birth and
effect of prenatal and postnatal factors on early wheezing
phenotypes. Krakow epidemiologic cohort study. Int J Occup
Med Environ Health 2008; 21:111–9.
80 Jedrychowski W, Perera FP, Maugeri U et al. Early wheezing
phenotypes and severity of respiratory illness in very early
childhood: study on intrauterine exposure to fine particle
matter. Environ Int 2009; 35:877–84.
81 Muino A, Menezes AM, Reichert FF, Duquia RP, Chatkin M.
Wheezing phenotypes from birth to adolescence: a cohort
study in Pelotas, Brazil, 1993–2004. J Bras Pneumol 2008; 34:
347–55.
82 Simon MR, Havstad SL, Wegienka GR, Ownby DR, Johnson CC.
Risk factors associated with transient wheezing in young
children. Allergy Asthma Proc 2008; 29:161–5.
83 Wardlaw AJ, Silverman M, Siva R, Pavord ID, Green R. Multi-
dimensional phenotyping: towards a new taxonomy for airway
disease. Clin Exp Allergy 2005; 35:1254–62.
84 Haldar P, Pavord ID, Shaw DE et al. Cluster analysis and clinicalasthma phenotypes. Am J Respir Crit Care Med 2008;
178:218–24.
85 Spycher BD, Minder CE, Kuehni CE. Multivariate modelling of
responses to conditional items: New possibilities for latent class
analysis. Stat Med 2009; 28:1927–39.
86 Clarisse B, Demattei C, Nikasinovic L, Just J, Daures JP, Momas
I. Bronchial obstructive phenotypes in the first year of life
among Paris birth cohort infants. Pediatr Allergy Immunol
2009; 20:126–33.
87 Holberg CJ, Halonen M, Solomon S et al. Factor analysis of
asthma and atopy traits shows 2 major components, one of
which is linked to markers on chromosome 5q. J Allergy Clin
Immunol 2001; 108:772–80.88 Pillai SG, Chiano MN, White NJ et al. A genome-wide search
for linkage to asthma phenotypes in the genetics of asthma
international network families: evidence for a major suscept-
ibility locus on chromosome 2p. Eur J Hum Genet 2006; 14:
307–16.
89 Smith JA, Drake R, Simpson A, Woodcock A, Pickles A,
Custovic A. Dimensions of respiratory symptoms in preschool
children: population-based birth cohort study. Am J Respir Crit
Care Med 2008; 177:1358–63.
90 Bacharier LB, Phillips BR, Bloomberg GR et al. Severe
intermittent wheezing in preschool children: a distinct pheno-
type. J Allergy Clin Immunol 2007; 119:604–10.
91 Turato G, Barbato A, Baraldo S et al. Nonatopic children
with multitrigger wheezing have airway pathology comparable
to atopic asthma. Am J Respir Crit Care Med 2008; 178:
476–82.
92 Stevenson EC, Turner G, Heaney LG et al. Bronchoalveolar
lavage findings suggest two different forms of childhood
asthma. Clin Exp Allergy 1997; 27:1027–35.
93 Kapitein B, Hoekstra MO, Nijhuis EH et al. Gene expression in
CD41 T-cells reflects heterogeneity in infant wheezing pheno-
types. Eur Respir J 2008; 32:1203–12.
94 Kurukulaaratchy RJ, Matthews S, Arshad SH. Does environ-
ment mediate earlier onset of the persistent childhood asthma
phenotype? Pediatrics 2004; 113:345–50.
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
1140 B. D. Spycher et al

8/3/2019 !!!!!!!! Phenotypes of Childhood Asthma - Are They Real 2010
http://slidepdf.com/reader/full/-phenotypes-of-childhood-asthma-are-they-real-2010 12/12
95 Kurukulaaratchy RJ, Matthews S, Holgate ST, Arshad SH.
Predicting persistent disease among children who wheeze
during early life. Eur Respir J 2003; 22:767–71.
96 Kuehni CE, Strippoli M-PF, Low N, Brooke AM, Silverman M.
Wheeze and asthma prevalence and related health-service use
in white and south Asian pre-school children in the UK. Clin
Exp Allergy 2007; 37:1738–46.
97 Halonen M, Stern DA, Lohman C, Wright AL, Brown MA,
Martinez FD. Two subphenotypes of childhood asthma that
differ in maternal and paternal influences on asthma risk. Am J
Respir Crit Care Med 1999; 160:564–70.
98 Peat JK, Toelle BG, Mellis CM. Problems and possibilities in
understanding the natural history of asthma. J Allergy Clin
Immunol 2000; 106:S144–152.
99 Schultz A, Devadason S, Savenije O, Sly P, Le Souef P, Brand P.
The transient value of classifying preschool wheeze into episo-
dic viral wheeze and multiple trigger wheeze. Acta Paediatr
2009; 99:56–60.
100 Morton N. Quantitative scores for asthma and atopy. Clin Exp
Allergy 1998; 28:95–7.
101 Bouzigon E, Siroux V, Dizier MH et al. Scores of asthma andasthma severity reveal new regions of linkage in EGEA families.
Eur Respir J 2007; 30:253–9.
102 Spycher BD, Silverman M, Strippoli M-PF, Kuehni CE. Child-
hood wheeze: one or several diseases? Eur Respir J 2009;
34 (Suppl. 53):756s.
103 Van Eerdewegh P, Little RD, Dupuis J et al. Association of the
ADAM33 gene with asthma and bronchial hyperresponsive-
ness. Nature 2002; 418:426–30.
104 Busse WW, Banks-Schlegel S, Wenzel SE. Pathophysiology of
severe asthma. J Allergy Clin Immunol 2000; 106:1033–42.
105 Shaheen SO, Northstone K, Newson RB, Emmett PM, Sherriff A,
Henderson AJ. Dietary patterns in pregnancy and respiratory
and atopic outcomes in childhood. Thorax 2009; 64:411–7.
106 Shaheen SO, Newson RB, Sherriff A et al. Paracetamol use in
pregnancy and wheezing in early childhood. Thorax 2002;
57:958–63.
107 Nicolaou NC, Simpson A, Lowe LA, Murray CS, Woodcock A,
Custovic A. Day-care attendance, position in sibship, and early
childhood wheezing: a population-based birth cohort study.
J Allergy Clin Immunol 2008; 122:500–6, e5.
108 Sibbald B, Turner-Warwick M. Factors influencing the preva-
lence of asthma among first degree relatives of extrinsic and
intrinsic asthmatics. Thorax 1979; 34:332–7.
109 Taussig LM, Wright AL, Holberg CJ, Halonen M, Morgan WJ,
Martinez FD. Tucson Children’s Respiratory Study: 1980 to
present. J Allergy Clin Immunol 2003; 111:661–75.
110 Scholtens S, Wijga AH, Brunekreef B et al. Breast feeding,
parental allergy and asthma in children followed for 8 years.
The PIAMA birth cohort study. Thorax 2009; 64:604–9.
111 Tariq SM, Hakim EA, Matthews SM, Arshad SH. Influence of
smoking on asthmatic symptoms and allergen sensitisation in
early childhood. Postgrad Med J 2000; 76:694–9.
112 Tariq SM, Matthews SM, Hakim EA, Stevens M, Arshad SH, Hide
DW. The prevalence of and risk factors for atopy in early childhood: a whole population birth cohort study. J Allergy Clin
Immunol 1998; 101:587–93.
113 Pao CS, McKenzie SA. Randomized controlled trial of flutica-
sone in preschool children with intermittent wheeze. Am J
Respir Crit Care Med 2002; 166:945–9.
114 Dawson B, Illsley R, Horobin G, Mitchell R. A survey of child-
hood asthma in Aberdeen. Lancet 1969; 1:827–30.
115 Roorda RJ, Mezei G, Bisgaard H, Maden C. Response of pre-
school children with asthma symptoms to fluticasone propio-
nate. J Allergy Clin Immunol 2001; 108:540–6.
116 Wilson NM, Phagoo SB, Silverman M. Atopy, bronchial respon-
siveness, and symptoms in wheezy 3 year olds [see comments].
Arch Dis Child 1992; 67:491–5.
c 2010 Blackwell Publishing Ltd, Clinical & Experimental Allergy , 40 : 1130–1141
Wheezing phenotypes in childhood 1141