بنام خداوند جان وخرد. ORTHOPAEDIC EMERGENCIES DR.Hossein Saremi Orthopaedic surgeon...
39
رد خ و ان د ج داون ام ج ن ب رد خ و ان د ج داون ام ج ن ب
-
Upload
asher-paul-spencer -
Category
Documents
-
view
221 -
download
0
Transcript of بنام خداوند جان وخرد. ORTHOPAEDIC EMERGENCIES DR.Hossein Saremi Orthopaedic surgeon...
وخرد جان خداوند وخرد بنام جان خداوند بنام
ORTHOPAEDIC ORTHOPAEDIC EMERGENCIESEMERGENCIES
DR.Hossein SaremiDR.Hossein SaremiOrthopaedic surgeonOrthopaedic surgeon
Hand&shoulder fellowshipHand&shoulder fellowship
Hamedan University of Hamedan University of medical sciencesmedical sciences
A musculoskeletal injury or A musculoskeletal injury or condition that, if missed, condition that, if missed, could result in additional could result in additional complications, significant complications, significant impairment, or death and impairment, or death and needs immediate needs immediate managementmanagement
Orthopaedic Orthopaedic EmergenciesEmergencies
DefinitionDefinition• ““missed”missed” = = LawsuitLawsuit•““additional complications”additional complications” = =
LawsuitLawsuit•““impairments”impairments” = = LawsuitLawsuit•Delaied management=Delaied management=LawsuitLawsuit•““death”death” = = LawsuitLawsuit
Emergent orthopaedic Emergent orthopaedic conditionsconditions
• Open FXOpen FX• DislocationDislocation• Compartement syndromCompartement syndrom• Any FX with associated vascular Any FX with associated vascular
injuryinjury
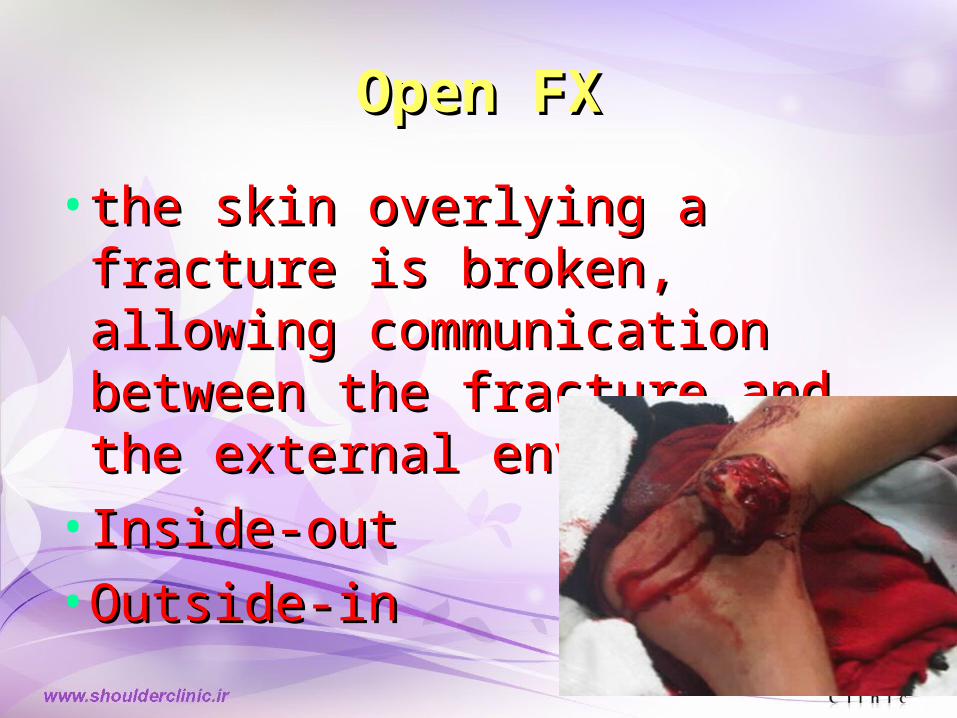
Open FXOpen FX
•the skin overlying a fracture the skin overlying a fracture is broken, allowing is broken, allowing communication between the communication between the fracture and the external fracture and the external environmentenvironment
•Inside-outInside-out•Outside-inOutside-in

Open FX complicationsOpen FX complications
•Soft tissue infectionSoft tissue infection•OsteomyelitisOsteomyelitis•Gas gangreneGas gangrene•TetanusTetanus•Crush syndromeCrush syndrome•Skin lossSkin loss•Non-unionNon-union
Open Fx ManagementOpen Fx Management
DOs:DOs:•Control the Control the
bleedingbleeding•Cover with sterile Cover with sterile
dressingdressing•SplintSplint• IV antibioticsIV antibiotics•Tetanus Tetanus
prophylaxisprophylaxis
DON’Ts:DON’Ts:•Scream and Scream and
pass outpass out•Replace Replace
protruding boneprotruding bone•Explore woundExplore wound•Clamp vesselsClamp vessels
DebridementDebridement
ConservatConservativeive
debridemdebridementent
Debridement Debridement
• Pasteur : It is the environment Pasteur : It is the environment not the bacteria that determines not the bacteria that determines whether a wound becomes whether a wound becomes infected infected

Open JointOpen Joint
• Any open wound over or Any open wound over or near a joint should be near a joint should be assumed to extend to the assumed to extend to the joint until proven otherwisejoint until proven otherwise
DislocationDislocation
• Displacement of bones at a joint Displacement of bones at a joint from their normal positionfrom their normal position
• May be associated with May be associated with neurovascularneurovascular
injuryinjury• Cartilage damageCartilage damage
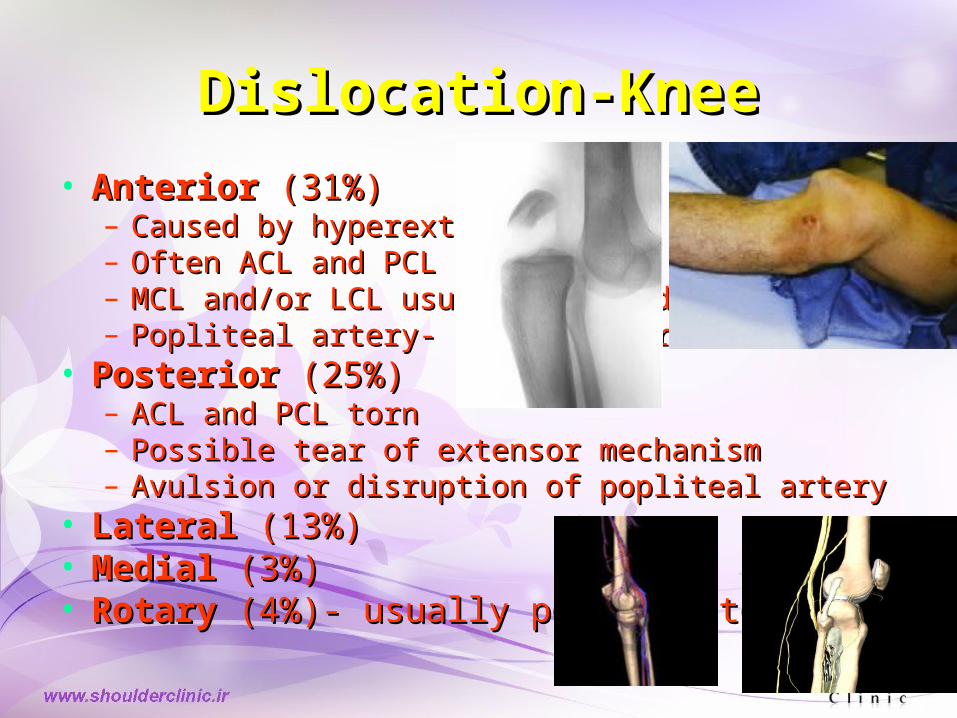
Dislocation-KneeDislocation-Knee
• AnteriorAnterior (31%) (31%)– Caused by hyperextensionCaused by hyperextension– Often ACL and PCL both tornOften ACL and PCL both torn– MCL and/or LCL usually injuredMCL and/or LCL usually injured– Popliteal artery- intimal tearPopliteal artery- intimal tear
• PosteriorPosterior (25%) (25%)– ACL and PCL tornACL and PCL torn– Possible tear of extensor mechanismPossible tear of extensor mechanism– Avulsion or disruption of popliteal arteryAvulsion or disruption of popliteal artery
• LateralLateral (13%) (13%)• MedialMedial (3%) (3%)• RotaryRotary (4%)- usually posterolateral (4%)- usually posterolateral
Dislocation-KneeDislocation-Knee
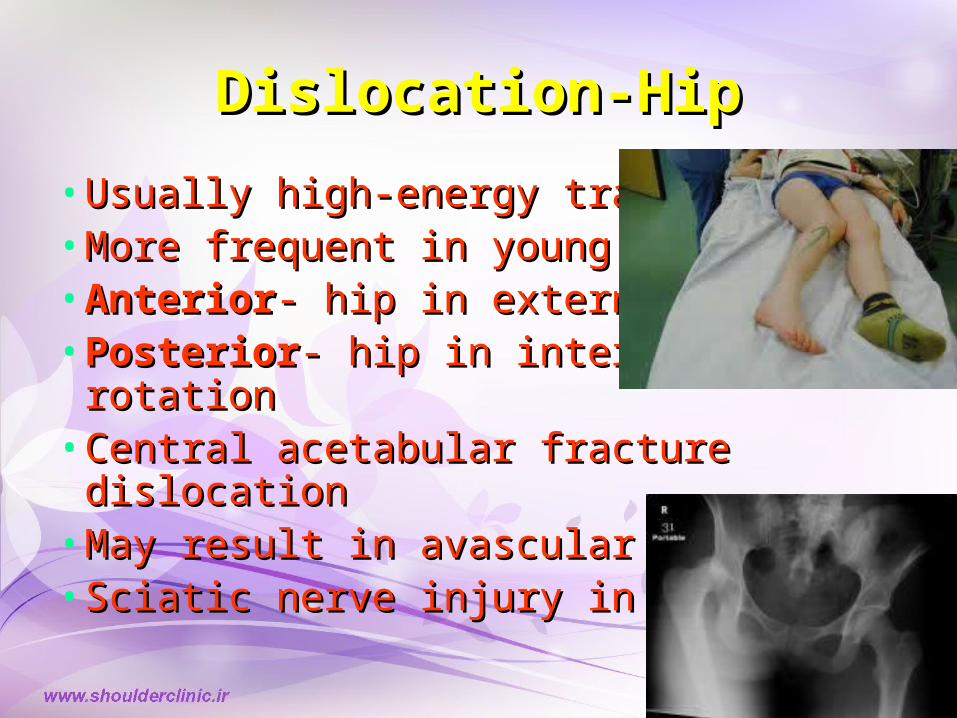
Dislocation-HipDislocation-Hip
•Usually high-energy traumaUsually high-energy trauma•More frequent in young patientsMore frequent in young patients•AnteriorAnterior- hip in external rotation - hip in external rotation •PosteriorPosterior- hip in internal rotation- hip in internal rotation•Central acetabular fracture Central acetabular fracture
dislocationdislocation•May result in avascular necrosisMay result in avascular necrosis•Sciatic nerve injury in 10-35%Sciatic nerve injury in 10-35%
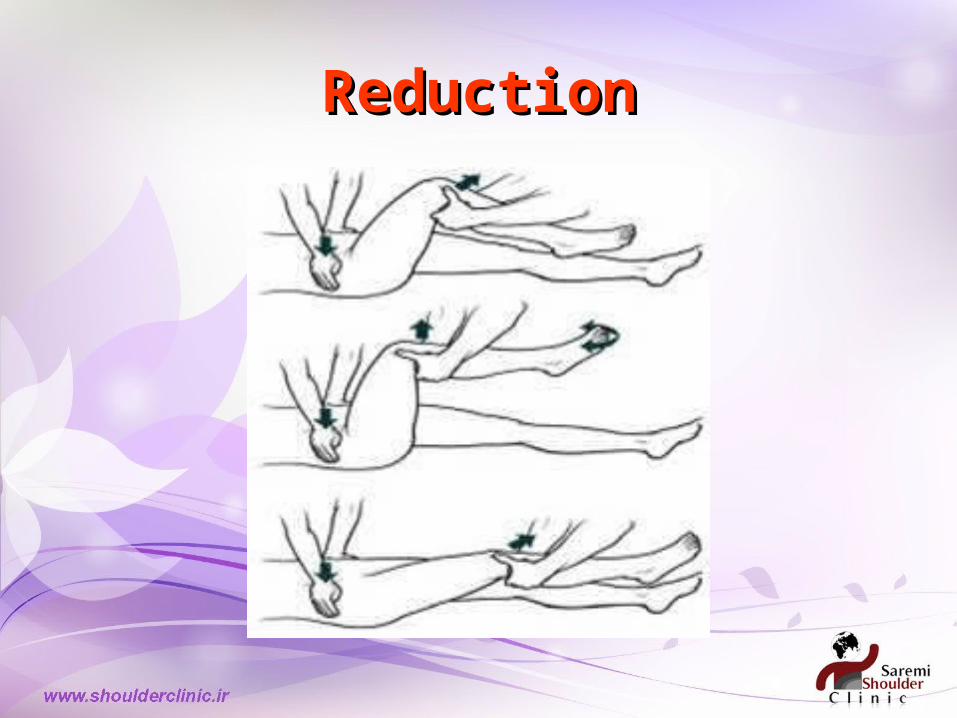
ReductionReduction
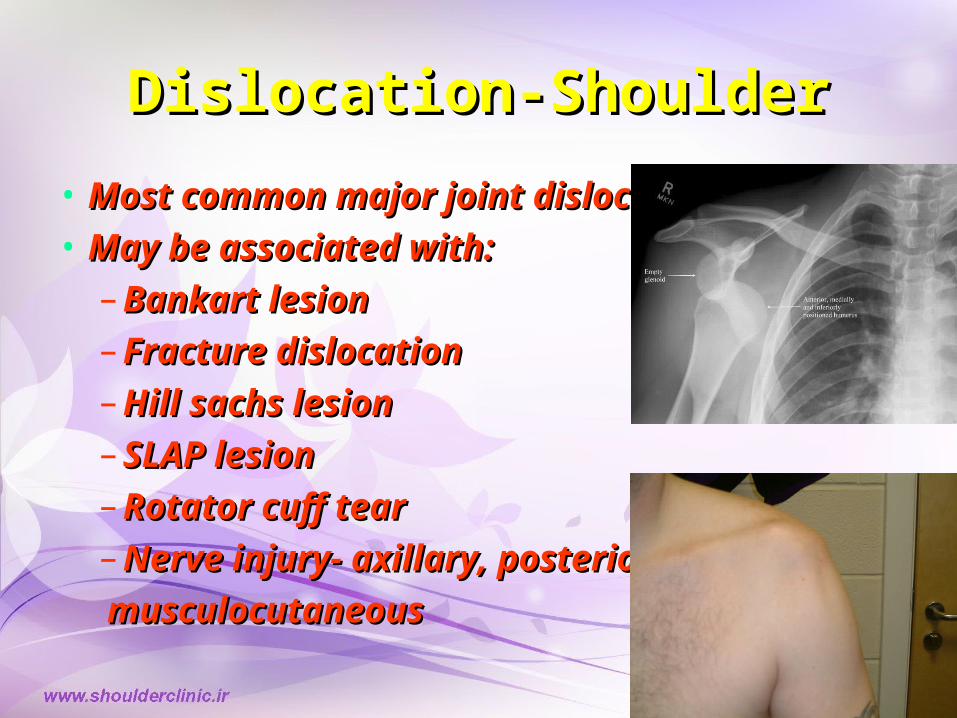
Dislocation-ShoulderDislocation-Shoulder
• Most common major joint dislocationMost common major joint dislocation• May be associated with:May be associated with:
– Bankart lesionBankart lesion– Fracture dislocationFracture dislocation– Hill sachs lesionHill sachs lesion– SLAP lesionSLAP lesion– Rotator cuff tearRotator cuff tear– Nerve injury- axillary, posterior cord,Nerve injury- axillary, posterior cord,
musculocutaneous musculocutaneous
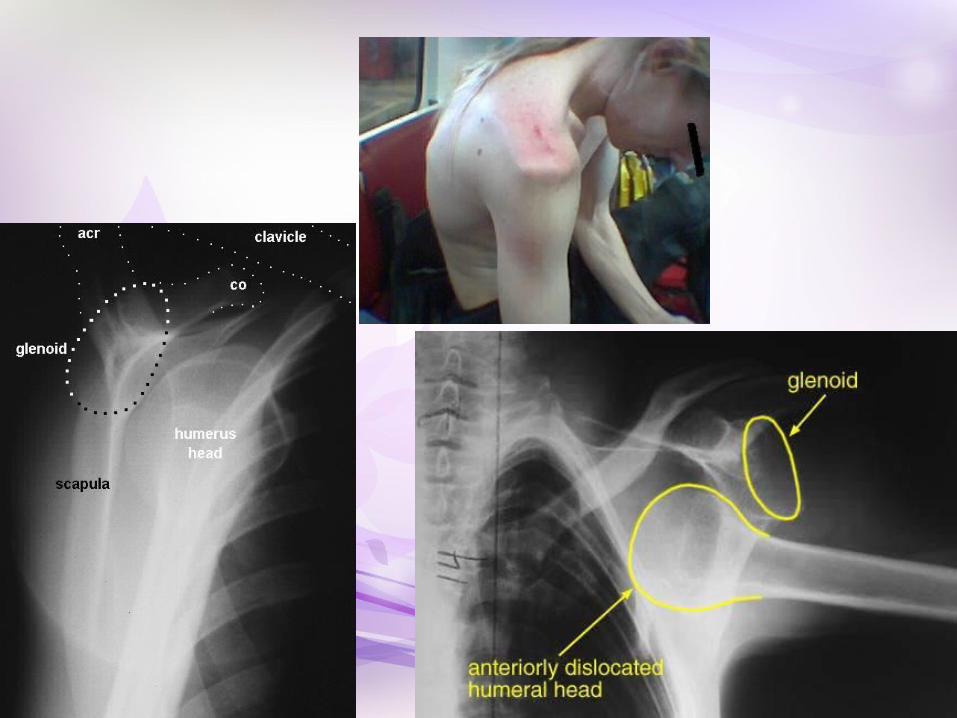
Dislocation-ShoulderDislocation-Shoulder
• AnteriorAnterior (95%) (95%)– Arm abducted and externally rotatedArm abducted and externally rotated
• PosteriorPosterior (2-4%) (2-4%)– Arm adducted and internally rotatedArm adducted and internally rotated– Electrocution, seizureElectrocution, seizure
• InferiorInferior (1%) (1%)– HyperabductionHyperabduction– Usually associated with significant traumaUsually associated with significant trauma

Dislocation-shoulderDislocation-shoulder
•Reduction (ant disloc)Reduction (ant disloc)•Stimson (hanging weight Stimson (hanging weight technique)technique)•Scapular ManipulationScapular Manipulation•Leidelmeyer (external Leidelmeyer (external rotation)rotation)•MilchMilch•Traction-CountertractionTraction-Countertraction
•Reduction (post disloc)Reduction (post disloc)•Traction on internally Traction on internally rotated and adducted arm rotated and adducted arm with pressure on humeral with pressure on humeral headhead
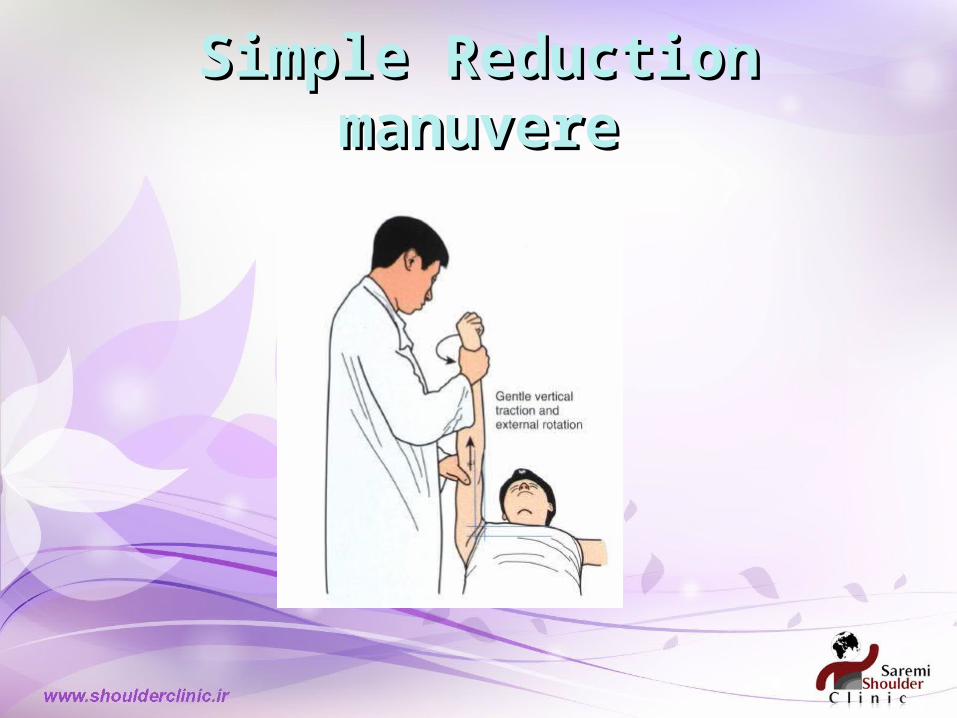
Simple Reduction Simple Reduction manuveremanuvere
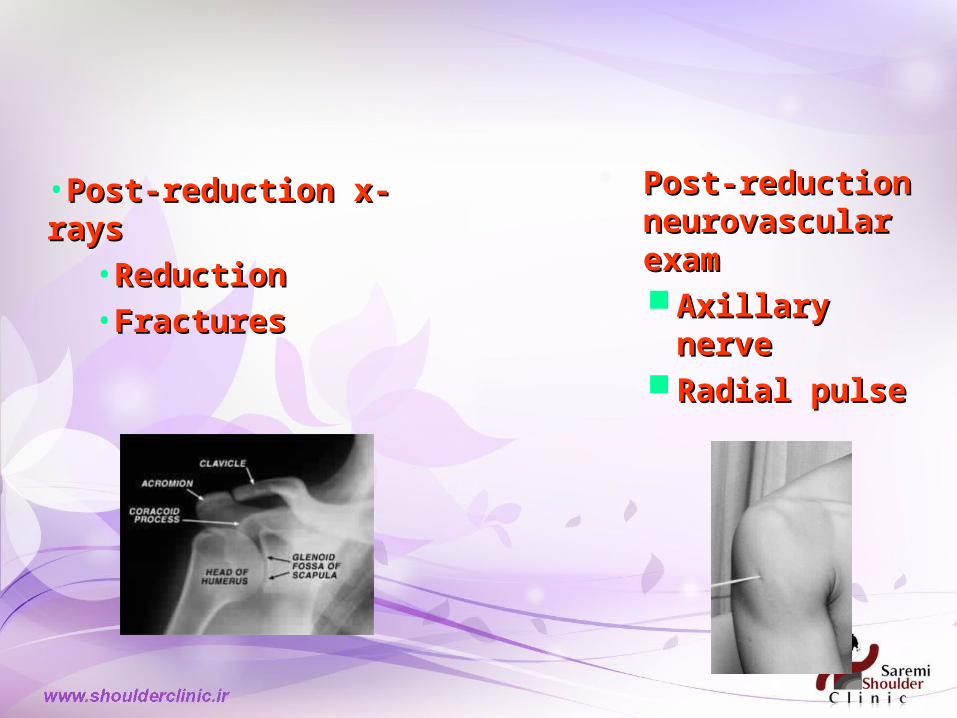
Post-reduction Post-reduction neurovascular neurovascular examexam Axillary Axillary
nervenerve Radial pulseRadial pulse
•Post-reduction x-Post-reduction x-raysrays
•ReductionReduction•FracturesFractures

Follow upFollow up
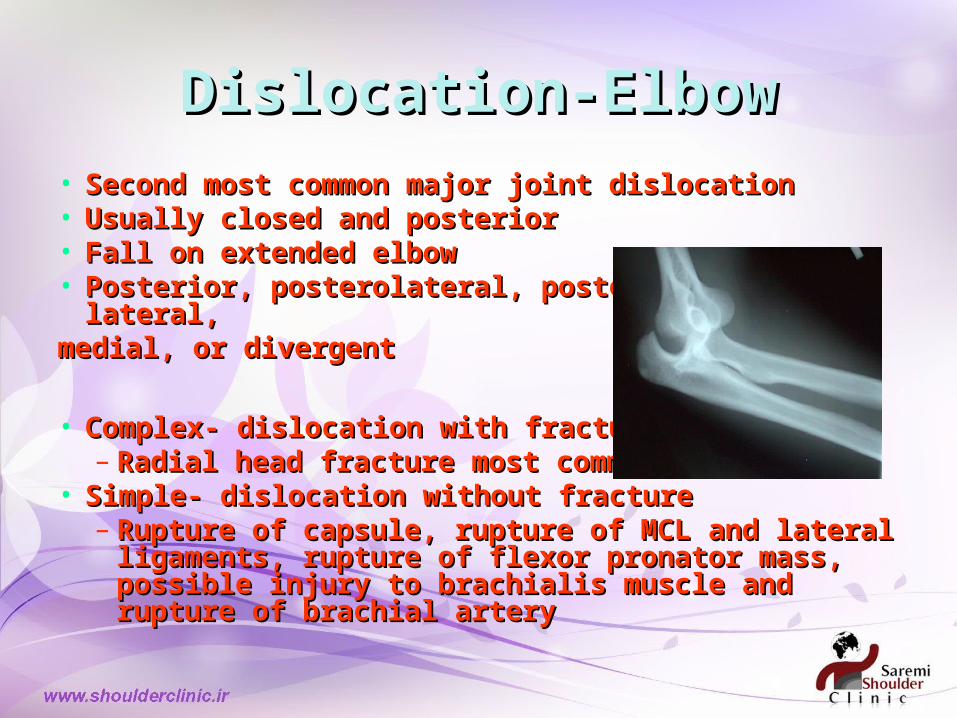
Dislocation-ElbowDislocation-Elbow• Second most common major joint dislocationSecond most common major joint dislocation• Usually closed and posteriorUsually closed and posterior• Fall on extended elbowFall on extended elbow• Posterior, posterolateral, posteromedial, Posterior, posterolateral, posteromedial,
lateral, lateral, medial, or divergentmedial, or divergent
• Complex- dislocation with fracture (35-40%)Complex- dislocation with fracture (35-40%)– Radial head fracture most commonRadial head fracture most common
• Simple- dislocation without fractureSimple- dislocation without fracture– Rupture of capsule, rupture of MCL and Rupture of capsule, rupture of MCL and
lateral ligaments, rupture of flexor pronator lateral ligaments, rupture of flexor pronator mass, possible injury to brachialis muscle mass, possible injury to brachialis muscle and rupture of brachial arteryand rupture of brachial artery

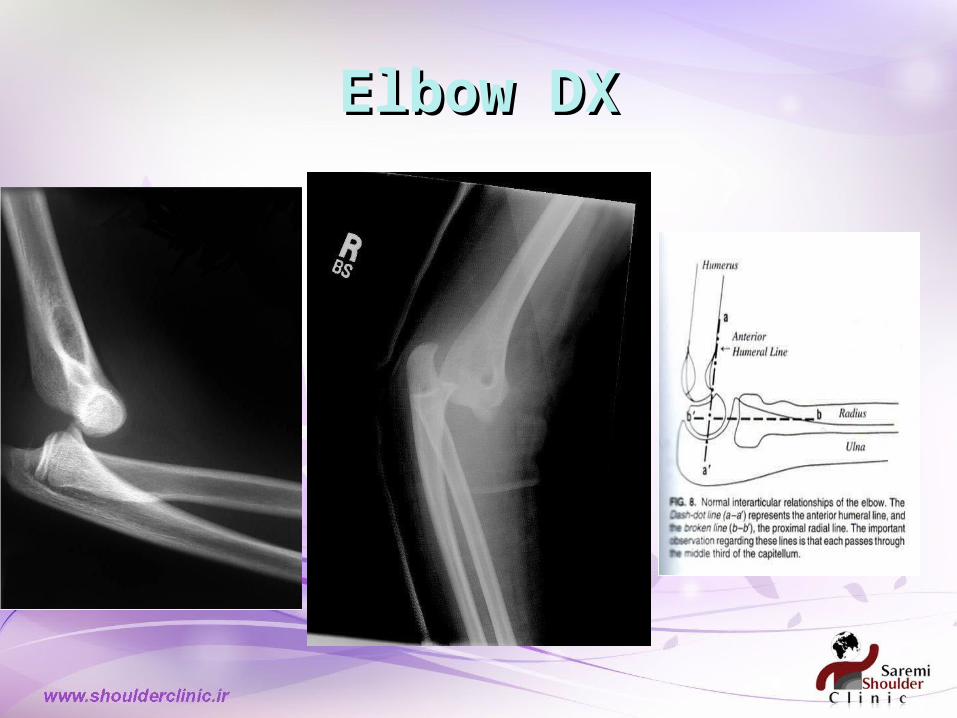
Elbow DXElbow DX
Dislocation-ElbowDislocation-Elbow•Nerve inuryNerve inury
•Neuropraxia Neuropraxia involving involving median or ulnar median or ulnar nerve in 20% of nerve in 20% of elbow elbow dislocationsdislocations•Ulnar nerve Ulnar nerve palsies more palsies more common in common in pediatricpediatric•Most neuro Most neuro deficits are deficits are transienttransient
Dislocation-ElbowDislocation-Elbow•Nerve inuryNerve inury
•Neuropraxia Neuropraxia involving median involving median or ulnar nerve in or ulnar nerve in 20% of elbow 20% of elbow dislocationsdislocations•Ulnar nerve Ulnar nerve palsies more palsies more common in common in pediatricpediatric•Most neuro Most neuro deficits are deficits are transienttransient

Dislocation-ankleDislocation-ankle

Dislocation-ankleDislocation-ankle
• Described by relationship of talus to tibiaDescribed by relationship of talus to tibia• Usually associated with fractureUsually associated with fracture• Pre/post-reduction neurovascular exam Pre/post-reduction neurovascular exam
and x-raysand x-rays• Adequate analgesia vs conscious Adequate analgesia vs conscious
sedationsedation• Reduction (even if open)Reduction (even if open)• SplintSplint• Ortho for washout if openOrtho for washout if open
Fractures ,Examine Fractures ,Examine vascular statusvascular status

Compartement syndromCompartement syndrom
• Limb threateningLimb threatening• Increased pressure in tight fascial Increased pressure in tight fascial
compartmentcompartment• Muscle necrosis at > 30mm HgMuscle necrosis at > 30mm Hg• Ischemic injury at 4 hrsIschemic injury at 4 hrs• Irreversible injury 4-8 hrsIrreversible injury 4-8 hrs• Signs: Signs: disproportionate pain, disproportionate pain, 5 P’s5 P’s
o PainPaino PallorPalloro ParaesthesiaeParaesthesiaeo ParalysisParalysiso PulselessPulseless
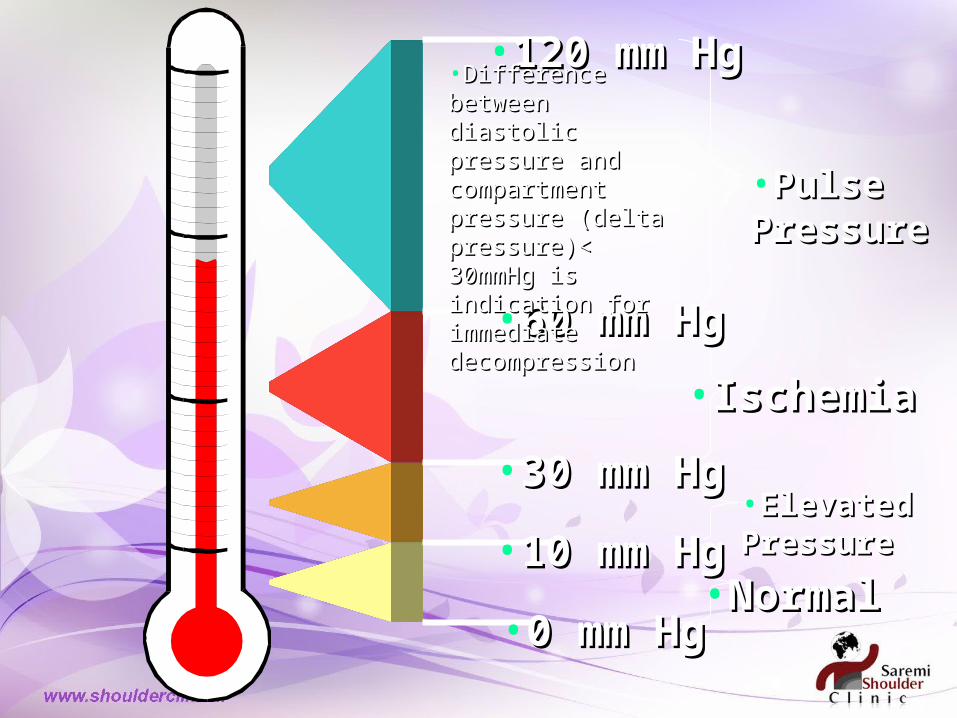
•0 mm Hg0 mm Hg
•10 mm Hg10 mm Hg
•30 mm Hg30 mm Hg
•60 mm Hg60 mm Hg
•120 mm Hg120 mm Hg
•Pulse Pulse PressurePressure
•IschemiaIschemia
•Elevated PressureElevated Pressure
•NormalNormal
•Difference between Difference between diastolic pressure and diastolic pressure and compartment compartment pressure (delta pressure (delta pressure)< 30mmHg pressure)< 30mmHg is indication for is indication for immediate immediate decompressiondecompression
Causes of compartement Causes of compartement syndromsyndrom
• Fractures ~75%Fractures ~75%• Crush injuryCrush injury• BurnsBurns• Extravasation Extravasation • Tourniquets, constrictive Tourniquets, constrictive
dressings/plastersdressings/plasters• Snake bitesSnake bites


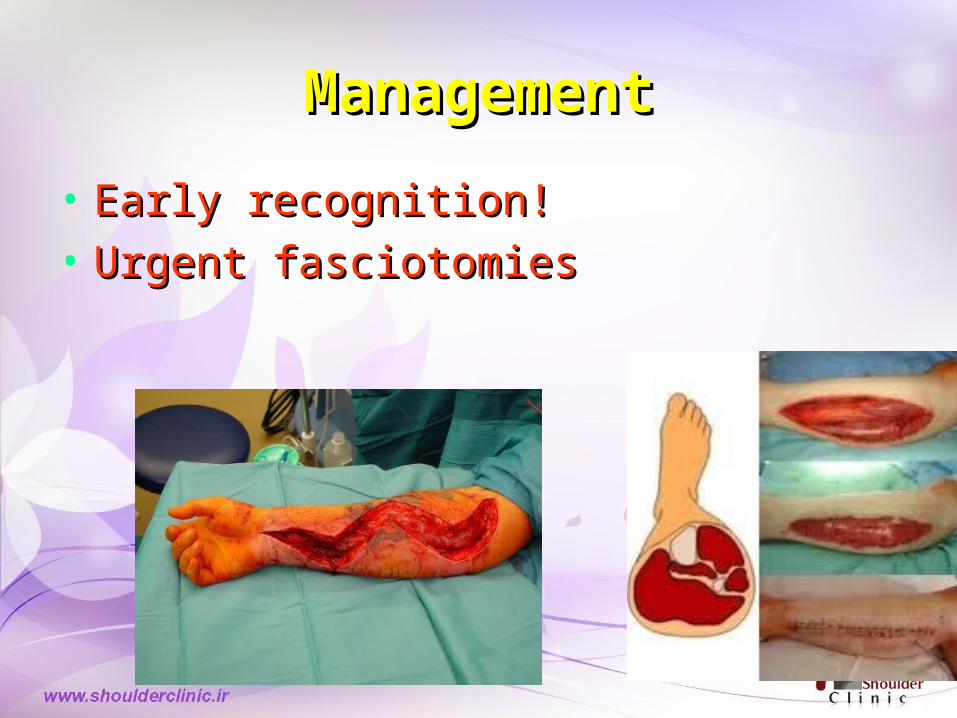
ManagementManagement
• Early recognition!Early recognition!• Urgent fasciotomiesUrgent fasciotomies
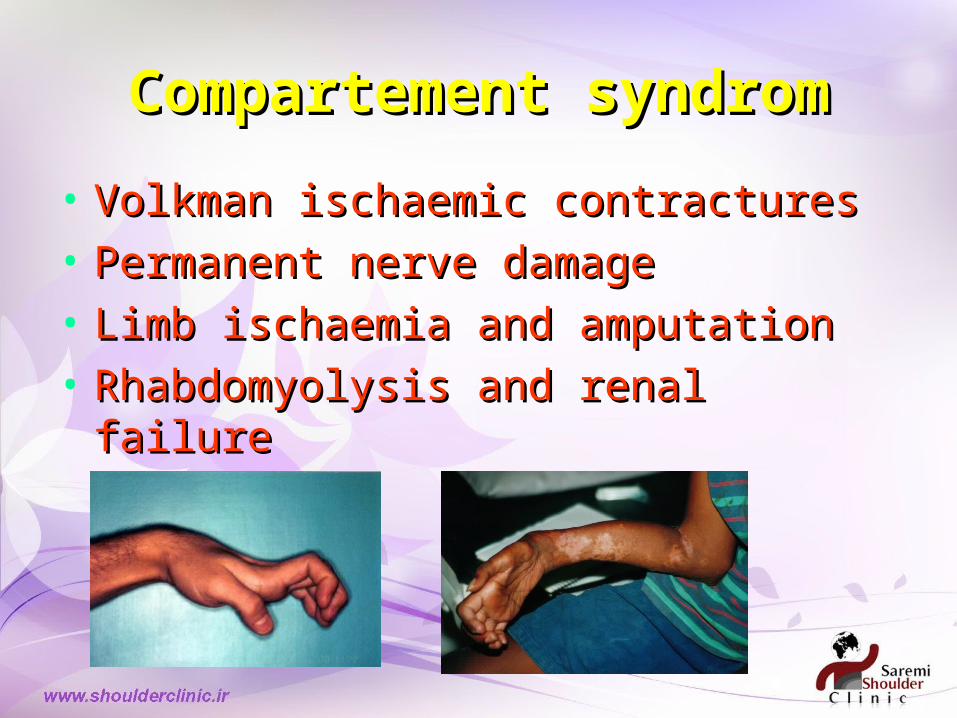
Compartement syndromCompartement syndrom
• Volkman ischaemic contracturesVolkman ischaemic contractures• Permanent nerve damagePermanent nerve damage• Limb ischaemia and amputationLimb ischaemia and amputation• Rhabdomyolysis and renal failureRhabdomyolysis and renal failure