Contents · Multidrug Therapy (MDT) as advised by ... The original Atlas of Leprosywas developed in...
82
Transcript of Contents · Multidrug Therapy (MDT) as advised by ... The original Atlas of Leprosywas developed in...


ContentsForeword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Flowchart for diagnosis and classification of leprosy . . . . . . . . . . . . . . . . . . . . . .2
Multidrug Therapy (MDT) as advised by the World Health Organisation . . . . . .3
Illustrations of MDT for multibacillary (MB) and paucibacillary (PB) drugs in blister calendar packs (BCPs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
‘Before and After MDT’ — results of treatment . . . . . . . . . . . . . . . . . . . . . . . . .8
Leprosy lesions 10
1. Paucibacillary leprosy (PB) leprosy; 1–5 skin lesions . . . . . . . . . . . . . . . . . .11
2. Multibacillary (MB) leprosy; 6 or more skin lesions . . . . . . . . . . . . . . . . . . . .24
Neural leprosy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .34
Reactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .35
Type 1 reactions (reversal, upgrading) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .36
Type 2 reactions (lepromatous, ENL) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .40
Disability–deformity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .42
Non-leprosy conditions of the skin 46(differential diagnosis)
(a) Simple commonly occurring conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . .47
(b) Less commonly occurring conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .62
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .73
References and Further Reading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .74
Publishing Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Inside Back Cover

Leprosy is curablewith Multidrug Therapy
which also prevents disability and deformityLet us join hands to work towards
A WORLD WITHOUT LEPROSY

1
Foreword Yo YuasaExecutive & Medical Director
Sasakawa Memorial Health Foundation, Tokyo, Japan
The original Atlas of Leprosy was developed in 1981 in close collaboration with Dr R. S. Guinto andhis colleagues of the Leonard Wood Memorial Laboratory, Cebu, Philippines. The initial 230 copies, in alarger prototype format, were practically handmade, but the response was so favourable that we decidedto produce the Atlas in a regular printed format in 1983. Our intention was to supply a collection of highquality pictures of leprosy, both clinical and histopathological, primarily for doctors and senior paramedical workers to aid their training activities, in addition to its use as reference material. As ateaching aid we also produced a colour slide version. Little did we expect, at the outset, the subsequentoverwhelming and continuous demand, even up to today, resulting in 38,000 English copies, as well as23,000 copies in six other languages – a ‘best seller’ on leprosy, though practically all are given out gratis.
The global leprosy scene was changing quite rapidly, almost concurrently with the publication of theoriginal Atlas in 1981. Starting with the historic Chemotherapy Study Group Meeting in October thatyear, multidrug therapy (MDT) has been primarily instrumental in this remarkable change. The 1991World Health Assembly resolution on the ‘Elimination of leprosy, as a public health problem’ furtheraccelerated that process. The 122 leprosy-endemic countries of the mid 80’s are likely to come down toaround 15 by the end of this year. WHO is now embarking on a ‘Final Push’, so that by the end of 2005,there should be no more leprosy-endemic countries left in the world, meaning that no country will havemore than one case in 10,000 of the population. That will indeed be a great accomplishment.
However, for those deeply involved in leprosy work, such an achievement only signifies reaching aninterim goal or a milestone, however significant it may be. Our final goal is ‘A World Without Leprosy’,in which every single new case (and new cases will undoubtedly keep arising) has been diagnosed andput on to MDT as quickly as possible. With reduced caseload, such basic leprosy control activities are likely to be handled, not by specialised vertical services, but general health services personnel.
This new Atlas, as the subtitle on the cover indicates, aims to assist frontline health workers, boththe peripheral general health workers as well as village health volunteers, to carry out case finding aseffectively as possible. Unlike the original Atlas, in which the pictures were all from the Philippines withrelatively light coloured skin, this new Atlas has pictures mostly from India and Bangladesh, an areawhich will continue to have nearly 80% of the global caseload. Our intention is to produce enoughcopies of the Atlas to equip every peripheral health facility of that immense area with one copy, probably requiring 200,000 copies or more.
Dr Colin McDougall, an eminent leprosy specialist, has kindly accepted the responsibility of producingthis volume. My name appears on the cover, primarily to take a full responsibility in choosing picturesor making statements, on which he had some doubts with regard to appropriateness in this volume.
The original Atlas was intended to strengthen leprosy control activities, at a time when no end pointof our efforts was in sight. This new Atlas is meant to serve until the end of our efforts. Ambitious? Yes, but not, I hope, altogether unrealistic.

2
*Any patient showing a positive skin smear, irrespective of the clinical classification, shouldbe treated with the multibacillary (MB) regimen. However, this depends on the availability of reliable laboratory facilities. Furthermore, the increasing prevalence of the HIV and hepatitis B infection in many leprosy-endemic countries points to the need to limit both thenumber of skin sites and the frequency of smear collection to a minimum (see references).
Flowchart for Diagnosis and Classification(Grouping for Multidrug Therapy)
SKIN LESION WITHSENSORY LOSS
LEPROSY
UP TO 5 SKINLESIONS
MORE THAN 5 SKINLESIONS
PB LEPROSY MB LEPROSY
SMEAR NEGATIVE SMEAR POSITIVE*
PB LEPROSY MB LEPROSY
Look for skin lesions compatible with leprosy and test for sensory loss
Diagnose
When skin-smears are not available or not dependable
Classify(Clinically)
When skin-smears are available and dependable
Classify(Bacteriologically)

3
From the list of activities, which are vital to the success of the Elimination Strategy, this NewAtlas concentrates on –
1. Early, correct diagnosis.
2. Differential diagnosis – i.e. a consideration of numerous other skin diseases whichmay mimic leprosy and lead to the wrong diagnosis.
3. A detailed description of the blister packs and regimens in use for the treatment of all patients with multidrug therapy (MDT).
The patient above was diagnosed by the health worker in the health centre, and is nowreceiving his first blister calendar pack (BCP) of drugs for the treatment of multibacillary(MB) leprosy.
Under WHO initiative, leprosy treatment is available for all patients, worldwide, free of charge.
Some leprosy services have used a combination of rifampicin, ofloxacin and minocycline(ROM), given as a one-time, single-dose for the treatment of single skin lesion (SSL) leprosy; see pages 6 & 18 of Reference 2. Rifampicin is an essential component of the regimens for both PB and MB leprosy, as described on the following pages. Ofloxacin andminocycline are other antibiotics with proven action against the leprosy bacillus.
Multidrug Therapy (MDT)

4
MDT (MB) – ADULT dosesFront view of the MB Adult MDTblister pack
Monthly Supervised Treatment (DAY 1– Top 2 lines break off: detachable):Clofazimine 300mg (three capsules of100mg), Rifampicin 600mg (two capsulesof 300mg) and Dapsone 100mg (one tablet
of 100mg)
Unsupervised Daily Treatment (DAYS2–28): Clofazimine 50mg (one capsule of50mg) EVERY DAY and Dapsone 100mg(one tablet of 100mg) EVERY DAY
Duration of Treatment: 12 blister packsto be taken within 12–18 months
Back view of the MB Adult MDTblister pack
R = Rifampicin: monthly supervised dose is600mg (2 capsules, each of 300mg).
C = Clofazimine 100mg: monthly supervised dose is 300mg (3 capsules).
D = Dapsone: monthly supervised dose is100mg (1 tablet).
The figures 2–28 represent 4 weeks of unsupervised Clofazimine (50mg) every day and Dapsone (100mg) daily.
Actual size of blister pack: 106mm x 140mm
5
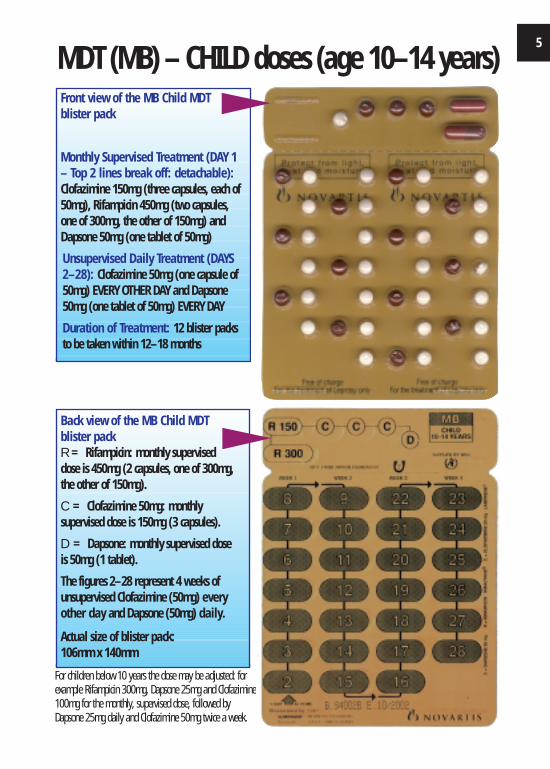
MDT (MB) – CHILD doses (age 10–14 years)Front view of the MB Child MDTblister pack
Monthly Supervised Treatment (DAY 1– Top 2 lines break off: detachable):Clofazimine 150mg (three capsules, each of50mg), Rifampicin 450mg (two capsules,one of 300mg, the other of 150mg) andDapsone 50mg (one tablet of 50mg)
Unsupervised Daily Treatment (DAYS2–28): Clofazimine 50mg (one capsule of50mg) EVERY OTHER DAY and Dapsone50mg (one tablet of 50mg) EVERY DAY
Duration of Treatment: 12 blister packsto be taken within 12–18 months
For children below 10 years the dose may be adjusted: forexample Rifampicin 300mg, Dapsone 25mg and Clofazimine100mg for the monthly, supervised dose, followed byDapsone 25mg daily and Clofazimine 50mg twice a week.
Back view of the MB Child MDTblister packR = Rifampicin: monthly superviseddose is 450mg (2 capsules, one of 300mg,the other of 150mg).
C = Clofazimine 50mg: monthly supervised dose is 150mg (3 capsules).
D = Dapsone: monthly supervised dose is 50mg (1 tablet).
The figures 2–28 represent 4 weeks of unsupervised Clofazimine (50mg) everyother day and Dapsone (50mg) daily.
Actual size of blister pack: 106mm x 140mm

6
MDT (PB) – Adult dosesFront view of the PB Adult MDTblister pack
Monthly Supervised Treatment (DAY 1– Top line breaks off: detachable):Rifampicin 600mg (two capsules, each of300mg) and Dapsone 100mg (one tablet of100mg)
Unsupervised Daily Treatment (DAYS2–28): Dapsone 100mg (one tablet of100mg) EVERY DAY
Duration of Treatment: 6 blister packs tobe taken within 6–9 months
Back view of the PB Adult MDTblister pack
R = Rifampicin: monthly supervised doseis 600mg (2 capsules, each of 300mg).
D = Dapsone: monthly supervised dose is100mg (1 tablet).
The figures 2–28 represent 4 weeks of unsupervised Dapsone (100mg) daily.
Actual size of blister pack: 72mm x 122mm

7
MDT (PB) – CHILD doses (age 10–14 years)Front view of the PB Child MDTblister pack
Monthly Supervised Treatment (DAY 1– Top line breaks off: detachable):Rifampicin 450mg (two capsules, one of300mg, the other of 150mg) and Dapsone50mg (one tablet of 50mg)
Unsupervised Daily Treatment (DAYS2–28): Dapsone 50mg (one tablet of50mg) EVERY DAY
Duration of Treatment: 6 blister packs tobe taken within 6–9 months
For children below 10 years the dose may be adjusted:for example Rifampicin 300mg monthly, and Dapsone25mg daily.
Back view of the PB Child MDTblister pack
R = Rifampicin: monthly supervised doseis 450mg (2 capsules, one of 300mg, theother of 150mg).
D = Dapsone: monthly supervised dose is50mg (1 tablet).
The figures 2–28 represent 4 weeks of unsupervised Dapsone (50mg) daily.
Actual size of blister pack: 72mm x 122mm

8
The patient presented with a highly active nodular form of MB leprosy. She was treatedfor 12 months with the MB regimen (page 4) and responded extremely well.
Before MDT
After MDT

9
This boy presented with active widespread skin and nerve lesions of MB leprosy. He wastreated with the 12 months MB regimen, child doses (page 5) and responded extremelywell.
After MDT
Before MDT

10
LEPROSY
Using the classification on page 2, the following images illustrate patientswith –
1. Paucibacillary (PB) leprosy, who by definition have 1–5 skin lesions, and
2. Multibacillary (MB) leprosy, who have 6 or more skin lesions.
With the exception of two pictures on page 34, this Atlas does not includeinformation on the mainly neural or neurological aspects of leprosy. Thereare numerous other publications on these important aspects of the disease,several of which are given under References and Further Reading, on pages74–76.
• These pictures are intended as an aid to recognitionand diagnosis
• In nearly all cases, leprosy can be diagnosed on clinical signs alone
• When in doubt about the diagnosis, send the patient to the nearest referral centre

11
1. This schoolboy has a fairly well defined, coppery patch on his left cheek, whichis flat (macular). It was his only lesion. Careful testing revealed that he could notfeel light touch or pinprick on the patch. Paucibacillary (PB) leprosy.
1. Paucibacillary (PB) Leprosy Cases

12 PAUCIBACILLARY (PB) LEPROSY
2. This young girl has a widespread area of reduced colouring (hypo-pigmentation) over the right cheek and side of the nose. Sensation testingrevealed that she could not feel cotton wool or pinprick on the patch.Paucibacillary (PB) leprosy.

13PAUCIBACILLARY (PB) LEPROSY
3. There is quite a large area on the lower part of the back of the forearm, with vague edges. This increased over a period of 2 months’ observation and eventually showed reduced response to sensory testing. Paucibacillary (PB) leprosy.

14 PAUCIBACILLARY (PB) LEPROSY
4. These vague, patches, with reducedcolouring (hypopigmentation) compared tothe surrounding skin, were found on the left shoulder region. They increased in size during a period of observation and showedloss of sensation to cotton wool and pinprick.Paucibacillary (PB) leprosy.

15PAUCIBACILLARY (PB) LEPROSY
5. This ring-like lesion was the only manifestation of leprosy. The surface, particularly round the edge was raised, slightly rough and dry. The lesion showedabsent sweating, even after exertion. Loss of sensation to cotton wool and pinprickwas demonstrated. Paucibacillary (PB) leprosy.
16 PAUCIBACILLARY (PB) LEPROSY
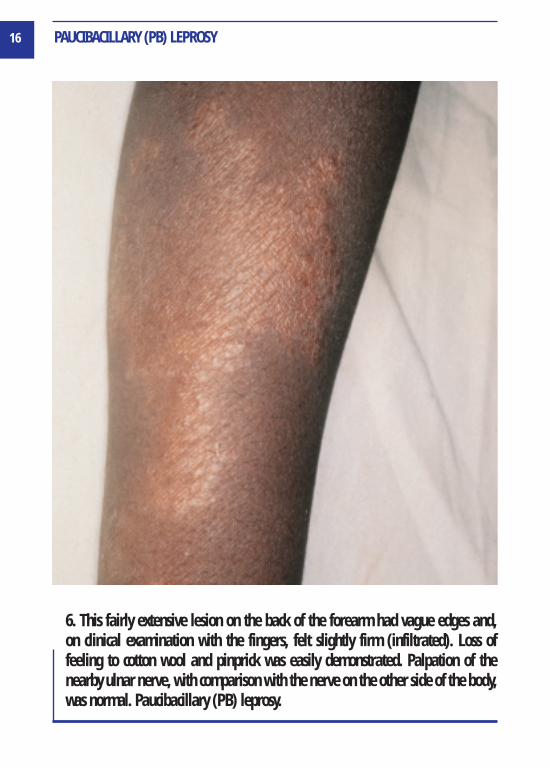
6. This fairly extensive lesion on the back of the forearm had vague edges and,on clinical examination with the fingers, felt slightly firm (infiltrated). Loss of feeling to cotton wool and pinprick was easily demonstrated. Palpation of thenearby ulnar nerve, with comparison with the nerve on the other side of the body,was normal. Paucibacillary (PB) leprosy.
17PAUCIBACILLARY (PB) LEPROSY
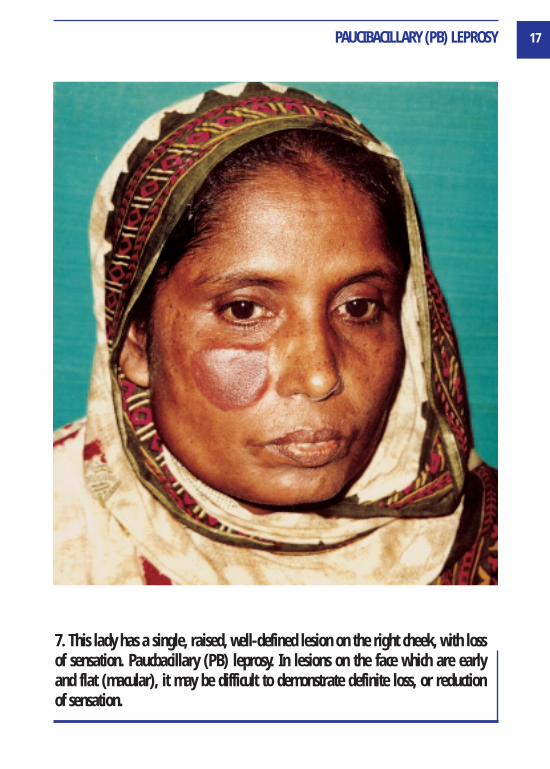
7. This lady has a single, raised, well-defined lesion on the right cheek, with lossof sensation. Paucbacillary (PB) leprosy. In lesions on the face which are early and flat (macular), it may be difficult to demonstrate definite loss, or reduction of sensation.
18 PAUCIBACILLARY (PB) LEPROSY
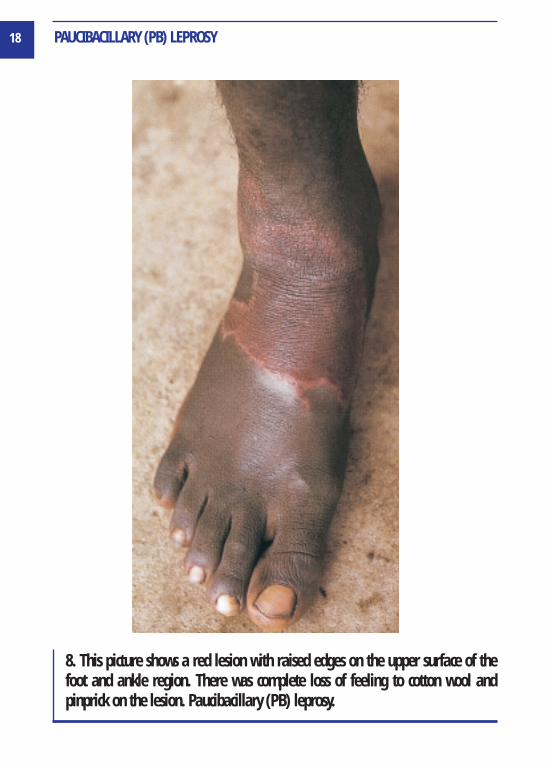
8. This picture shows a red lesion with raised edges on the upper surface of thefoot and ankle region. There was complete loss of feeling to cotton wool and pinprick on the lesion. Paucibacillary (PB) leprosy.

19PAUCIBACILLARY (PB) LEPROSY
9. This boy shows a lesion over the left shoulder with reduced colouring (hypopigmentation), with a tendency to form small ‘daughter’ or ‘satellite’lesions beyond the main edge. There was definite loss of sensation to cotton wooland pinprick. Paucibacillary (PB) leprosy.

20 PAUCIBACILLARY (PB) LEPROSY
1O. There is a large, well-defined lesion on the left buttock. The edge was raisedand firm on clinical examination with the fingers. Definite loss of sensation, especially towards the edges, to cotton wool and pinprick. Paucibacillary (PB) leprosy.
21PAUCIBACILLARY (PB) LEPROSY
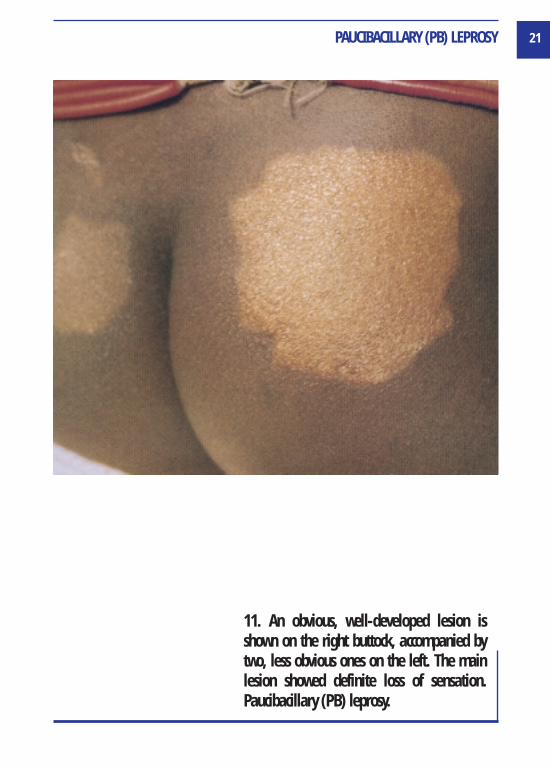
11. An obvious, well-developed lesion isshown on the right buttock, accompanied bytwo, less obvious ones on the left. The mainlesion showed definite loss of sensation.Paucibacillary (PB) leprosy.

22 PAUCIBACILLARY (PB) LEPROSY
12. Two well-defined lesions are seen, withmarked reduction of normal skin colouring(hypo-pigmentation). Loss of feeling to cottonwool and pinprick was easily demonstrated.Paucibacillary (PB) leprosy.
23PAUCIBACILLARY (PB) LEPROSY
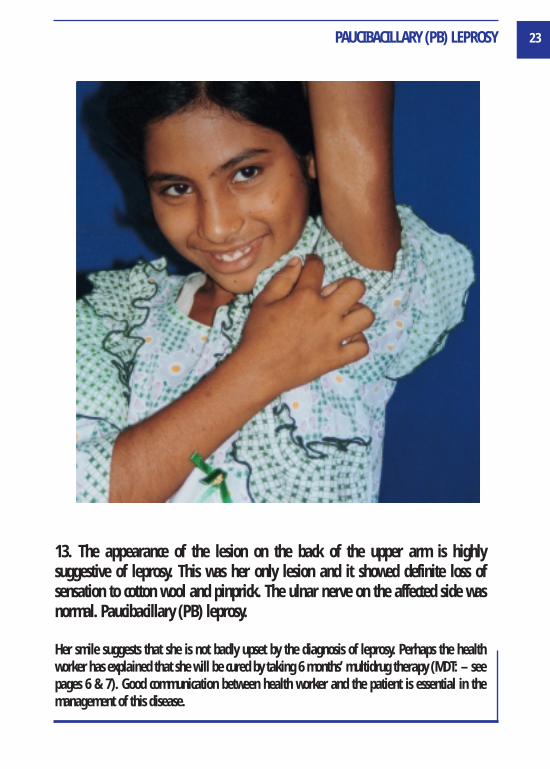
13. The appearance of the lesion on the back of the upper arm is highly suggestive of leprosy. This was her only lesion and it showed definite loss of sensation to cotton wool and pinprick. The ulnar nerve on the affected side wasnormal. Paucibacillary (PB) leprosy.
Her smile suggests that she is not badly upset by the diagnosis of leprosy. Perhaps the healthworker has explained that she will be cured by taking 6 months’ multidrug therapy (MDT: – seepages 6 & 7). Good communication between health worker and the patient is essential in themanagement of this disease.

24
14. This little boy has numerouspale patches scattered over thebuttocks and trunk and there weremany more on the front of the body and limbs. Note thatin leprosy patches or lesions, normal colouring (pigment) is reduced, but not completelylost. Loss of pigment (de-pigmentation) occurs in vitiligo(see page 57) and some otherconditions. The total of lesionsshown here is clearly higher than 5 and some peripheral nerves were affected. Multibacillary (MB)leprosy.
2. Multibacillary (MB) Leprosy Cases

25MULTIBACILLARY (MB) LEPROSY
15. A large lesion with reduced colouring (hypopigmentation) is seen between thebuttocks, including some ‘daughter’ or ‘satellite’ lesions beyond the main edgesand there are other lesions at top right of the picture. Three other skin lesionswere recorded and two peripheral nerves involved. These lesions had loss of sensation to cotton wool and pinprick. Multibacillary (MB) leprosy.

26 MULTIBACILLARY (MB) LEPROSY
16. Numerous lesions of faint coppery colourare seen over the buttocks and lower back.Although not easily demonstrated, some ofthe larger patches showed loss of sensation tocotton wool. Skin smears were positive.Multibacillary (MB) leprosy.

27MULTIBACILLARY (MB) LEPROSY
17. The patient shows numerous ‘punched out’ lesions on the buttocks and legsand there are many similar lesions on the trunk and arms. Skin smears were positive. Most of the lesions showed loss of sensation to cotton wool testing andthere were three enlarged peripheral nerves. Multibacillary (MB) leprosy.

28 MULTIBACILLARY (MB) LEPROSY
18. This is a close up view of another patient, with similar lesions to those in Figure 17. The central ‘immune’ area showed reduced sensation to cotton wooland pinprick and skin smears of the red, raised lesions were positive.Multibacillary (MB) leprosy.

29MULTIBACILLARY (MB) LEPROSY
19. Another patient with skin lesions similar to those in Figures 17 and 18. Theirregular circular or oval rings and the ‘punched out’ centres are characteristic ofthis form of leprosy and hardly ever seen in any other skin disease. The diagnosiswas confirmed by demonstrating loss of sensation on the raised rings and someof the enclosed areas of normal-looking skin. Multibacillary (MB) leprosy.

30 MULTIBACILLARY (MB) LEPROSY
20. This patient has numerous, raised red patches over the trunk and limbs andthere were also several on the face. Some peripheral nerves were enlarged andskin smears were positive. Some patches showed slight loss of sensation to cottonwool testing. Multibacillary (MB) leprosy.

31MULTIBACILLARY (MB) LEPROSY
21. This is the back of the patient shown in Figure 20. In this form of (MB) leprosy, the lesions are typically raised and slope down towards the skin level atthe edges, like an inverted saucer. This is in contrast to the findings in many of thePB patches shown in Figures 1–13. Multibacillary (MB) leprosy.

32 MULTIBACILLARY (MB) LEPROSY
22. The whole of the back and most of the arm surface show symmetrically distributed flat (macular) lesions. Skin smears were strongly positive. It was not possible to demonstrate loss of sensation in these lesions, but the skin smearswere strongly positive and three peripheral nerves were enlarged. Multibacillary(MB) leprosy.

33MULTIBACILLARY (MB) LEPROSY
23. This boy shows active MB leprosy withpatches on the face and neck, and many rounded or oval small lumps (nodules) on theright ear. The other ear was similarly affected.Always examine the ears in this form of leprosy. In some cases they are the main, oreven the only, site of swelling and/or noduleformation. Multibacillary (MB) leprosy.

34
NEURAL LEPROSYOn the left, enlarged nerves are shown inthe neck. This is a common finding in clinicalleprosy. Visibly enlarged nerves, as shownhere, are valuable in making the diagnosisof leprosy, because such enlargement doesnot occur in other conditions.
The picture below is a reminder that, in somecountries, particularly India, patients maypresent with nerve enlargement, but no skinlesions: ‘Pure Neural Leprosy’ (PNL).
The nerve illustrated and arrowed is the superficial peroneal on the upper surface ofthe foot and lower leg, but in PNL the typical nerves affected are ulnar, lateralpopliteal, median, posterior tibial and facial. This form of leprosy should not be diagnosed and treated without referral to an experienced clinician or practitioner.

35
REACTIONS
• Apart from the ‘routine’, commonly occurring forms of leprosy illustratedin pages 11–33, frontline health workers and volunteers should be able torecognise and refer patients in reaction.
• Reactions in leprosy occur when the immune system, for reasons which areessentially unknown, reacts against the bacillary infection.
• Far from being helpful or protective, these reactions are often damaging toskin, nerves and other tissues.
• Skin lesions become swollen, hot, red and painful. Ulceration may occur.
• More importantly, nerves are also inflamed and swollen and this may resultin damage to nerve fibres carrying messages for sensation and muscle power.
• In some cases, such damage may occur suddenly, either at the time of diagnosis or, during treatment, or after treatment has finished.
• The following pictures are included to help frontline health workers and volunteers to recognise reactions and refer the patient for expert advice.
• In the following pages, reactions are classified into Type 1 (Reversal or upgrading) + Type 2 (Lepromatous or ENL).

36
1. The picture shows a large patch of paucibacillary (PB) leprosy on the face and ear, with enlargement of the great auricular nerve in the neck (arrowed). A reaction developed suddenly after the start of multidrug therapy (MDT). Theprevious lesion became swollen, painful and tender. The picture is an importantreminder of the importance of nerve involvement in Type 1 reactions. The greatauricular shown here happens to have limited clinical significance, but if peripheralnerves in the limbs, or those supplying the eye region are involved, loss of sensation and/or muscle power may occur, sometimes very rapidly. Consult yoursupervisor or national guidelines on the use of analgesics, splinting or steroids (prednisolone), according to the severity of the reaction. Type 1 reaction.
Reactions – Type 1 (syn. Reversal, Upgrading)

37TYPE 1 REACTIONS
2. This large paucibacillary (PB) patch was originally almost flat, but has becomeswollen, and red, especially round the edges, due to Type 1 reaction. As seen here,the skin manifestations are striking and often lead to recognition and treatmentof this complication in leprosy, but the possibility of nerve damage, with involvement of hands, feet or eyes, is even more important. If available, reactioncases are often better treated in a referral centre, but consult your national guidelines with regard to the immediate treatment of mild or severe cases. Type 1 reaction.

38 TYPE 1 REACTIONS
3. The raised red, swollen, painful, tender lesions seen here, particularly on thehands and fingers, occurred during the course of treatment for multibacillary(MB) leprosy. A reaction of this extent and severity is best managed in a referralcentre or specialised unit, if available, but consult your national guidelines onsteps to be taken. Type 1 reaction.

39TYPE 1 REACTIONS
4. Raised red lesions are seen above and below the navel (umbilicus) in a patientwith multibacillary (MB) leprosy. There were numerous other patches of Type 1reaction on the trunk and limbs. Reactions of this kind may occur suddenly and, asalready stressed above, it is the element of peripheral nerve involvementwhich is of particular concern. Type 1 reaction.

40
Reactions – Type 2 (syn. Lepromatous, ENL)
1. Numerous cutaneous and subcutaneous lesions are shown, mostly red andraised, with pustule formation and ulceration in several places. ENL stands for‘erythema nodosum leprosum’ and is a frequent complication of types of MB leprosy near the lepromatous end of the immune spectrum. Attacks of ENL typically last for about 2 weeks, often accompanied by fever, malaise, and pain inthe nerves, joint involvement and eye complications. Mild cases may be managedunder field conditions (consult your national guidelines), but severe or persistentcases are best managed in a referral unit or special centre. Type 2 reaction.

41TYPE 2 REACTIONS
2. The pink or rose-coloured tender nodules of ENL are often seen on the face andlimbs, but may be generalised, as seen here in a patient who had lesions over thewhole trunk area. In some cases, ENL nodules may become vesicular, pustular,bullous or gangrenous and break down with considerable tissue damage. Mildcases may be handled under field conditions, but those with severe symptoms and/or involvement of peripheral nerves, eyes or testicles are usuallybetter managed in a referral centre or special unit. Type 2 reaction.

42
DISABILITY–DEFORMITY
LATE OR DELAYED DIAGNOSIS AND TREATMENT OF LEPROSY:DISABILITY AND DEFORMITY
● If leprosy is detected and diagnosed early, multidrug therapy(MDT: see pages 3–7) will cure the disease and prevent disabilityand deformity.
● If diagnosed late, and either not treated, or inadequately treated,various nerves will be damaged, leading to loss of sensation andmuscle power.
● The following pictures illustrate the end-results of late diagnosisand treatment. They are included in this New Atlas in order to emphasise the crucial role of early detection and MDT in preventing disability and deformity.
● Deformities are the end result of untreated, or poorly treated leprosy. Unfortunately, because of the long-standing damage tonerve fibres, they do not respond to multidrug therapy (MDT).However, proper recognition of these conditions is essential andshould lead to intensified case-detection activities in both familycontacts and people in the locality.
43DISABILITY–DEFORMITY
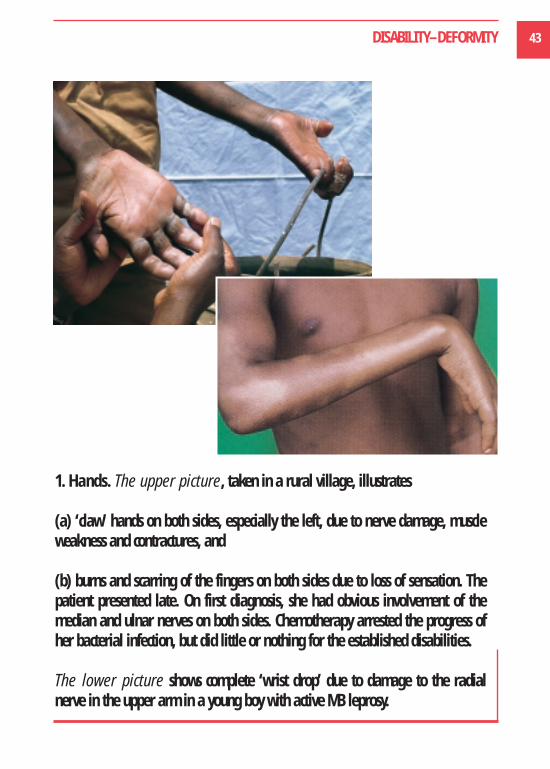
1. Hands. The upper picture, taken in a rural village, illustrates
(a) ‘claw’ hands on both sides, especially the left, due to nerve damage, muscle weakness and contractures, and
(b) burns and scarring of the fingers on both sides due to loss of sensation. Thepatient presented late. On first diagnosis, she had obvious involvement of themedian and ulnar nerves on both sides. Chemotherapy arrested the progress ofher bacterial infection, but did little or nothing for the established disabilities.
The lower picture shows complete ‘wrist drop’ due to damage to the radialnerve in the upper arm in a young boy with active MB leprosy.

44 DISABILITY–DEFORMITY
2. Feet. The pictureopposite (right) shows a complete left ‘drop foot’due to involvement of thelateral popliteal nerve inthe leg during a reaction.The patient presented in reaction, with muscleweakness and loss of sensation.
The picture opposite (left) shows theplanter (under) surface of a patient’sfoot with ulceration at the base of the bigtoe, on one of the main pressure pointsin walking. There is also deformity andsome ‘clawing’ of the toes. He presentedlate with established damage to theperipheral nerve supplying sensation and muscle power to the foot. EARLY DIAGNOSIS and treatment with MDTwould have PREVENTED this situation.

45DISABILITY–DEFORMITY
3. Face and eyes. Upper picture; active MB leprosy showing thickened (infiltrated) and shiny skin on the face. The ears on both sides show infiltrationand nodule formation. Eyebrows have disappeared (‘madarosis’; common inwell-established MB leprosy of this kind, uncommon in other diseases). Lowerleft; active nodular MB leprosy with collapse of the cartilage of the nose(arrowed). Lower right; elderly patients with a long history of leprosy are mostat risk to eye complications and blindness. This patient is unable to close the eyesto protect them, due to damage to the facial nerves on both sides. This condition(‘lagophthalmos’) is the most common eye complication in leprosy. Exposure ofthe cornea (front covering of the eye) may lead to infection and ulceration.

46
Some of the pictures, particularly those which are of ‘simple’ or commonly occurring conditions, may be valuable to peripheral health care workers.
Other less common conditions have been included since the overall distribution anduse of this NEW ATLAS OF LEPROSY may include experienced observers in government and non-government health facilities, qualified doctors at district orreferral level and dermatologists.
Failure to keep leprosy in mind, leading to under-diagnosis (missing the diagnosis)is a serious matter. Over or wrong diagnosis is equally serious and may be occurringto a significant extent in programmes which undertake intensive case-finding activities over a limited period of time. Particularly under these circumstances,WHO has advised
“....greater emphasis should be placed on the specificity of diagnosisand it is already becoming important that every new case detectedbe thoroughly investigated for correctness of diagnosis of the disease and possible identification of index case(s).”
We have divided the pictures into two groups:
(a) Relatively ‘simple’ (straightforward) conditions which occur commonly in mostcountries, 1–15, and
(b) Less commonly occurring conditions, including a few which may rarely be seenin some areas, mainly as a reminder of the wide range of skin (dermatological)conditions which can, under different circumstances, cause confusion and lead towrong diagnosis, 16–25.
NON-LEPROSY CONDITIONS OF THE SKIN (DIFFERENTIAL DIAGNOSIS)

47NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
Simple commonly occurring conditions
1. Birthmark. Typically single or few in number. Present from birth, unchangingover long periods of observation. Edges may be very sharply defined and jagged,as shown here. Hypopigmented, but with normal sweating and sensation. Sometimes called naevus anaemicus.

48 NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
2. Birthmark. Left shoulder region. Present since birth; normal sensation andsweating. Take a history; ask the parents or close relatives about the durationof the lesion; test for loss or reduction of sensation.

49NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
3. Post-inflammatory hypochromia. Reduction of normal pigment at the siteof previous (possibly recent) inflammation from wounds and simple inflammatoryconditions as shown here is common and may occasionally mimic early leprosy.Take a history; examine for loss or reduction in sensation.

50 NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
4. Scar tissue. Scars are seen very commonly in patients in leprosy-endemicareas. They may be caused by cutting, burning or simple trauma (physical damage). Those shown here followed the application of native medicine. Somescars may show loss of sensation and resemble a patch of PB leprosy.
51
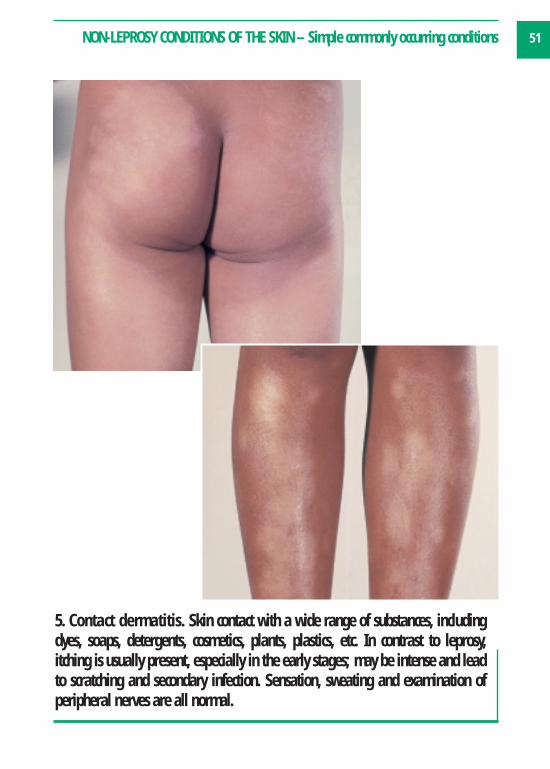
5. Contact dermatitis. Skin contact with a wide range of substances, includingdyes, soaps, detergents, cosmetics, plants, plastics, etc. In contrast to leprosy, itching is usually present, especially in the early stages; may be intense and leadto scratching and secondary infection. Sensation, sweating and examination ofperipheral nerves are all normal.
NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions

52 NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
6. Seborrhoeic dermatitis. The lesions are widespread, scaly and itchy. Thehairy scalp may be involved with lesions behind the ears. Sensation and sweating are normal and the condition should respond to simple treatment.
53NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
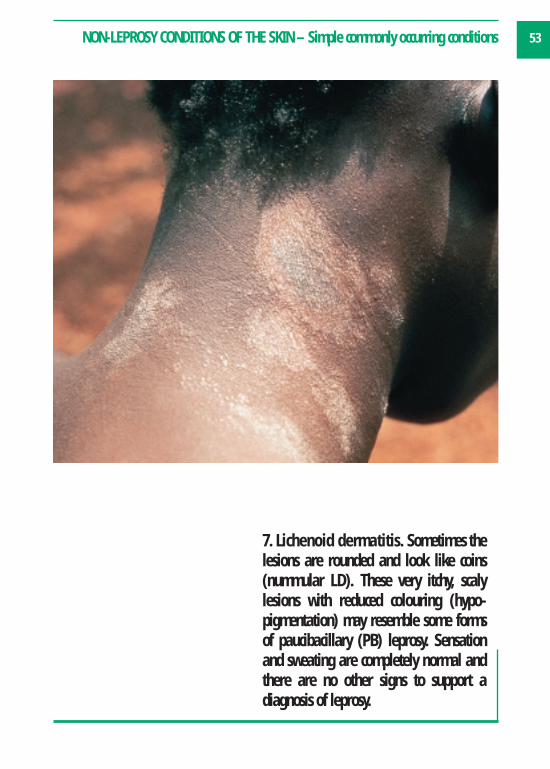
7. Lichenoid dermatitis. Sometimes thelesions are rounded and look like coins(nummular LD). These very itchy, scalylesions with reduced colouring (hypo-pigmentation) may resemble some formsof paucibacillary (PB) leprosy. Sensationand sweating are completely normal andthere are no other signs to support a diagnosis of leprosy.

54 NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
8. Tinea versicolor. A very common tropical condition. Well-defined, scalylesions are often widely scattered over the trunk, neck and limbs. Often co-existsin patients with leprosy. Sensation and sweating normal; fungal elements easilyseen under the microscope.

55NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
9. Tinea circinata. Typical lesions are shown on the face and leg. This is a fungal disease with normal sensation and sweating, which responds to simple anti-fungal treatment.
56 NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
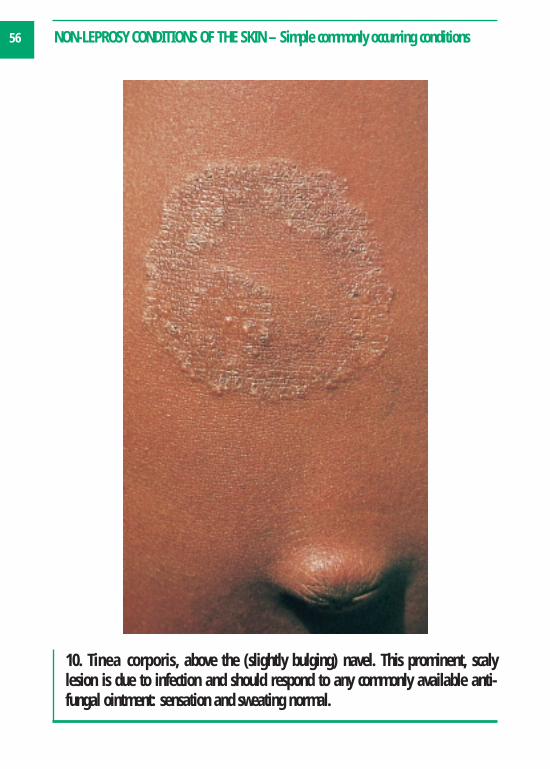
10. Tinea corporis, above the (slightly bulging) navel. This prominent, scalylesion is due to infection and should respond to any commonly available anti-fungal ointment: sensation and sweating normal.

57NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
11. Vitiligo. The remarkably white lesions seen here are due to de-pigmentation,(i.e. complete loss of colour) as opposed to the much more typical hypo-pigmentation (reduction of pigment) seen in leprosy. However in the early stageof this disfiguring disease, incomplete loss of pigment may lead to confusion withleprosy. Sensation, sweating and skin texture are normal.

58 NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
12. Pityriasis rosea. Occurs typically in adolescents or young adults. ‘Pityriasis’means bran and individual lesions are red, with a collar of fine scales pointingtowards the centre. The condition often starts with a ‘herald’ patch, (lower picture),which is larger than the subsequent lesions, which are widely distributed, especially on the trunk. Sensation, sweating, peripheral nerves — all normal.
59NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
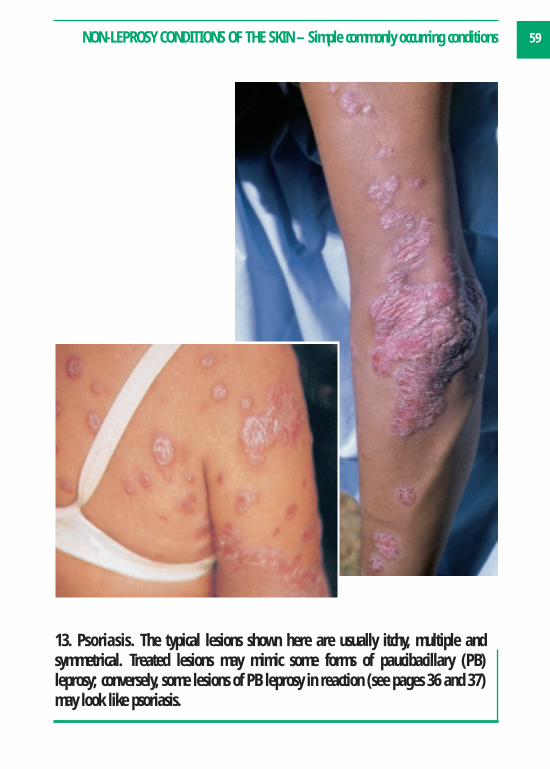
13. Psoriasis. The typical lesions shown here are usually itchy, multiple and symmetrical. Treated lesions may mimic some forms of paucibacillary (PB) leprosy; conversely, some lesions of PB leprosy in reaction (see pages 36 and 37)may look like psoriasis.

60 NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
14. Granuloma annulare. As shown here, the lesions may closely resemblesome forms of PB leprosy. Affects mainly children and young adults. The upperpicture shows the common localised form. The lower picture illustrates a muchless common widely distributed form. Papules or nodules appear in a ring-like(annular) pattern. Lesions are symptomless and there are no enlarged peripheral nerves. Sensation and sweating are normal.
61NON-LEPROSY CONDITIONS OF THE SKIN – Simple commonly occurring conditions
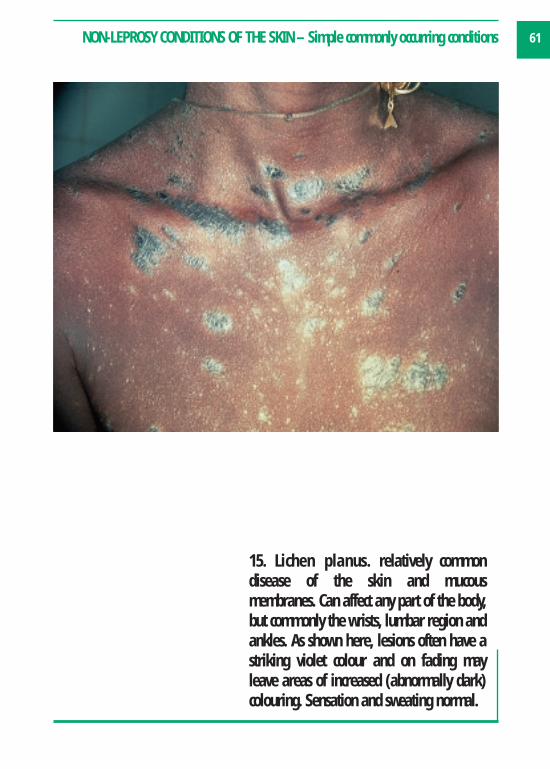
15. Lichen planus. relatively common disease of the skin and mucous membranes. Can affect any part of the body,but commonly the wrists, lumbar region andankles. As shown here, lesions often have astriking violet colour and on fading mayleave areas of increased (abnormally dark)colouring. Sensation and sweating normal.

62
The preceding pictures 1–15 illustrated relatively simple, straightforward,commonly occurring conditions.
The following pictures (16–25) deal with less common conditions, some ofwhich may in fact be rare in your country or area. They are intended mainly as a reminder of the wide group of non-leprosy conditionswhich may resemble or mimic leprosy.
● All the conditions shown here have been reported as giving rise to awrong diagnosis of leprosy.
● It is hoped that at least some of the pictures will help you to avoid thismistake, which can have grave consequences for the individual patientand the family. As already noted above, it is important for you to findout which conditions are known to cause confusion in your area.
● As with the list of References and Further Reading (pages 74–76), pictures 16–25 of less commonly occurring conditions are included in this NEW ATLAS OF LEPROSY mainly for the benefit of supervisors,teachers/trainers, district hospitals, or referral centres.
Non-leprosy conditions of the skin –less commonly occurring conditions A check-list for supervisors, programme managers
and referral centres
63NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
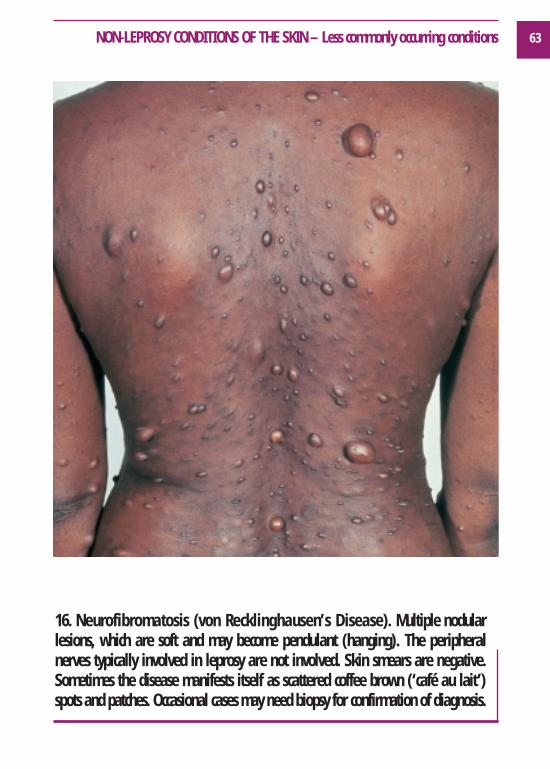
16. Neurofibromatosis (von Recklinghausen’s Disease). Multiple nodularlesions, which are soft and may become pendulant (hanging). The peripheralnerves typically involved in leprosy are not involved. Skin smears are negative.Sometimes the disease manifests itself as scattered coffee brown (‘café au lait’)spots and patches. Occasional cases may need biopsy for confirmation of diagnosis.

64 NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
17. Sarcoidosis. Skin appearances areextremely variable and may closelyresemble leprosy. This lady has a large,single, slightly hypopigmented patch covering most of the left side of her face,with some infiltration and small noduleson the rim of the nose. Sensation was normal and there was no enlargement ofnerves near the patch, or in the peripheralnerves typically affected by leprosy.

65NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
18. Lupus Vulgaris (skin tuberculosis). Skin manifestations are variable andmay be confusing in the diagnosis of leprosy, mimicking some forms of PB leprosy. Lesions are red (erythematous), infiltrated, slow growing, well definedand symptomless, but with a tendency to ulceration and scar formation. Nervesare not involved and (apart from scars), sensation on the lesions is normal. This little girl has a well developed lesion on the arm, but the most commonlyaffected areas are the face, neck and buttocks.

66 NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
19. Discoid lupus erythematosus. The pictures shown here are from two different patients. The upper picture shows typical ‘bat-wing’ distribution oflesions on the face, with some tendency towards de-pigmentation (i.e. loss of pigment). This is shown much more markedly in the lower picture of lesions on the upper chest and shoulders. Sensation and sweating are normal andperipheral nerves not affected.

67NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
20. Xanthomatosis. Not a common condition,but the nodules, as shown here, may causeconfusion. The disease is usually associatedwith high levels of blood cholesterol andappears more commonly in young people.The elbow region illustrated is a common sitefor nodules.

68 NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
21. Dermal leishmaniasis. The patient (above, right) shows lesions of disseminated leishmaniasis which resemble some forms of multibacillary (MB)leprosy. The patient (below, left) shows nodular lesions of post-kala-azar dermalleishmaniasis (PKDL), which may also be mistaken for leprosy. Leishmaniasis hasa markedly regional distribution worldwide. It is a good example of the importanceof finding out which conditions, in your own area or country, actually give rise todiagnostic problems in practice.

69NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
22. Granuloma multiforme. This condition,which clearly mimics leprosy to a remarkable degree, was originally described,and occurs mainly in Nigeria, but has occasionally been found elsewhere. Its causeis unknown; possibly a variant of granulomaannulare (see picture 14 on page 60). Initialstages are characterised by itching (not typicalfor leprosy). Lesions disappear sooner or laterand do not respond to any form of treatment.Sensation, sweating and peripheral nerves –all normal.

70 NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
23. Pellagra. Patches may simulate paucibacillary (PB) leprosy in reaction (seeReactions). Lesions are typically symmetrical,symptomless, and often associated with malnutrition, alcoholism and poverty.Sensation, sweating and peripheral nervesare all normal. Lesions (and the general condition) rapidly respond to nicotinic acid.

71NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
24. Lymphoma. (Also called mycosis fungoides, granuloma fungoides or cutaneous T-cell lymphoma.) Included as a reminder that the typical shiny nodules seen here on the face may occasionally cause diagnostic confusion. Occursmostly in adult males and is commonly fatal.

72 NON-LEPROSY CONDITIONS OF THE SKIN – Less commonly occurring conditions
25. Kaposi’s sarcoma. Various forms of this malignant condition may occur in leprosy-endemic countries, some of them associated with HIV-AIDS. The lesionsshown here are from two different patients. The lesions on the forearm (upperpicture) are from a patient who later died of AIDS. The hard bluish, vascular nodules bleed easily. Feet (lower picture) and hands are the commonest site of involvement. Sensation, sweating and peripheral nerves — all normal.

73
Acknowledgements
We are extremely grateful to the following for permission to use published images and transparencies from their collections:
1. The Leprosy Mission International, 80 Windmill Road, Brentford, Middlesex, TW8 0QH, United Kingdom (Contents, Foreword (facing page), pp. 8, 9, 11, 12, 23, 24, 27, 38, 57).
2. Dr Peter Stingl, Lechbrucker Strasse 10, 86989 Steingaden, Germany and Cassella-Riedel Pharma GmBH, Frankfurt am Main, Germany, publishers of Dermatosen im Bild, 1984 (pp. 18, 20, 21, 43 (lower), 47, 48, 50, 54, 56).
3. Professor S.J. Yawalkar, Formely Ciba-Geigy Ltd, Basle, Switzerland and the Novartis Foundation for Sustainable Development, Basle, Switzerland (pp. 33, 34 (lower), 39, 45 (upper), 55 (lower), 58 (lower), 59 (left), 60 (upper), 65, 66 (upper), 68, 70, 71, 72 (upper)).
4. Leprosy Elimination Group, Strategy Development and Monitoring for Eradication and Elimination, World Health Organization, CH-1211, Geneva 27, Switzerland (pp. 3, 15).
5. Professor W. Jacyk, Department of Dermatology, University of Pretoria, PO Box 667, 0001 Pretoria, Republic of South Africa and the German Leprosy Relief Association, Würzburg, Germany (pp. 16, 52, 53, 58 (upper), 60 (lower), 61, 63, 64, 66 (lower), 69, 72 (upper)).
6. Dr A. Thomas, Chittagong Leprosy Control Project, The Leprosy Mission, Bangledesh, India (pp. 17, 30, 31, 37).
7. Dr T.T. Fajardo, Leonard Wood Memorial–Eversley Childs Sanitarium Laboratory for Leprosy Research, Cebu, The Philippines (pp. 13, 28, 32, 40, 49, 51, 67).
8. International Centre for Eye Health, Institute of Ophthalmology, 11–43 Bath Street, London, EC1V 9EL. Professor I.S. Roy and Dr S. Samanta, West Bengal, India (p. 45 (lower right)).
9. E. Nunzi and D.L. Leiker, A Manual of Leprosy, O.C.S.I., Bologna, Italy, 1990 (p. 72 (lower)).
10. American Leprosy Missions, Inc., 1 ALM Way, Greenville, SC 29601, USA (p. 36).
11. W.H. Jopling, previously Hospital for Tropical Diseases, London, United Kingdom (p. 22).
Images of blister packs on pages 4–7 were supplied by Novartis, Basle, Switzerland. Photographs of the reverse of the packs were produced by Chris Walter, Grosvenor Studios, Abingdon, Oxon, UK.
All other images are from the first author’s collection.

74
References and Further Reading
From the Leprosy Elimination Group,World Health Organization, CH-1211Geneva 27, Switzerland
1. Chemotherapy of Leprosy for Control Programmes.Report of a WHO Study Group. TRS 675, 1982.2. WHO Expert Committee on Leprosy, SeventhReport. TRS 874, 1998.3. Chemotherapy of Leprosy, Report of a WHO StudyGroup. TRS 847, 1994.4. Risk of Relapse in Leprosy. WHO/CTD/LEP/94.1.5. Progress towards Leprosy Elimination. WHO WeeklyEpidemiological Record, June 1997.6. Global Strategy for the Elimination of Leprosy as aPublic Health Problem. WHO/CTD/LEP/94.2.7. A Guide to Leprosy Control. Second Edition. WHO,Geneva, 1988.8. Managing Programmes for Leprosy Control. WHOTraining Modules, 1993.9. Prevention of Disabilities in Patients with Leprosy.A Practical Guide. WHO, Geneva, 1993.10. Elimination of Leprosy, Questions and Answers.WHO/CTD/LEP/96.4.11. MDT – Questions and Answers, WHO/CTD/LEP/97.8.12. Guidelines for Personnel in Collection of SkinSmears in Leprosy Control Programmes for the Prevention and Control of Possible Infection with HIV.WHO/CDS/LEP/87.1 Rev 1.13. On Being in Charge – A guide to management inprimary health care. Second Edition, WHO, Geneva,1992.14. Leprosy Elimination Campaigns (LEC) and SpecialAction Projects for the Elimination of Leprosy (SAPEL).Questions and Answers. WHOLEP/97.3.
15. Shortening Duration of Treatment of Multi-bacillary leprosy. WHO Weekly EpidemiologicalRecord, May 1997.16. The Final Push Towards Elimination of Leprosy.Strategic Plan 2000–2005. CDS/CPE/CEE/2000.1.WHO, 1211-Geneva 27, Switzerland.17. A Guide to Eliminating Leprosy as a Public HealthProblem. Second Edition 1997. WHO/LEP/97.7.18. Guide for General Health Workers to EliminateLeprosy as a Public Health Problem. First Edition2000. CDS/CPE/CEE/2000.
From Teaching and Learning Materials forLeprosy (TALMILEP), InternationalFederation of Anti-Leprosy Associations(ILEP), 234, Blythe Road, London, W14 0HT,United KingdomTel. +44 (0) 20 7602 6925 Fax +44 (0) 20 7321 1621 e-mail ilep.org.uk Website http://www.ilep.org.uk
1. Leprosy: A Bryceson and R E Pfaltzgraff (1989) –a readable reference book for medical students, general practitioners and physicians. Price £2.002. A Guide to Eliminating Leprosy as a Public HealthProblem (1997), WHO – a pocket guide to diagnosisand management. FREE3. Leprosy for Field Staff: Alison Summers (1993) –this excellent book is aimed at health workers in specialized leprosy programmes or general healthworkers who see leprosy on a regular basis. FREE4. Atlas of Leprosy: Guinto et al. (1997) SasakawaMemorial Health Foundation, Tokyo, Japan. This book ofcolour photographs is most suitable for use in areas suchas East Asia where leprosy is seen in lighter skins. FREE

75REFERENCES & FURTHER READING
5. Leprosy in Africans: Jacyk (1986)* – a booklet containing colour photographs with short notes inEnglish and French. Arabic translation available onrequest. A popular and practical reference guide forhealth workers. FREE6. Care of the Eye in Hansen’s Disease: M Brand(1993)* – outlines the management of eye complications in leprosy for ophthalmologists andother health workers. FREE7. Insensitive feet: P Brand (1994) – a good background to the problems of insensitive feet. FREE8. Prevention of disabilities in patients with leprosy: apractical guide. H Srinivasan (WHO, 1993) – forthose involved in patient assessment, treatment andteaching self-care to people with leprosy. Price (foruse in developing countries) £9.509. Essential action to minimize disability in leprosypatients: J Watson (1994)* – an excellent book withclear text and illustrations written for general healthworkers caring for people with leprosy. FREE10. Leprosy Surgery for General Hospitals: H Srinivasan, WHO. FREE for use in developing countries11. Guide to health education in leprosy: P J Neville(1993) – contains messages for patient education.FREE12. Don’t treat me like I have leprosy: Frist – a bookabout the history of leprosy and the importance ofsocial issues. FREE
*Also available in French
These books and details of other materials can beordered directly from TALMilep. TALMilep is currentlyreviewing and updating the materials it supplies as aresult some titles may be replaced by new or revisedpublications.
TALMilep also distributes a catalogue of trainingcourses and a video catalogue that reviews leprosy
related videos and gives information on how to orderthem.
For people developing health training materials local-ly for leprosy in general, combined or specialist pro-grammes, TALMilep can help by sharing information onwhat has been produced elsewhere and can provide technical and editorial advice.
INFOLEP, TALMilep’s sister organization based atthe Netherlands Leprosy Relief, provides an informationservice on leprosy related literature. It also holds adatabase of available materials on leprosy (includingmaterials in languages other than English). INFOLEPcan be accessed at
http://infolep.antenna.nl or by e-mail at
In association the Leprosy Division of theDirectorate General of Health Services,Ministry of Health and Family Welfare,Government of India, New Delhi1. Facilitators Guide. Training Programme for PrimaryHealth Care Staff, 1999 (paperback, 48 pages).2. Learning Material on Leprosy for Capacity Buildingof General Practitioners (postcard size booklet, spiralbinding, 36 pages).3. Learning Material on Leprosy for Capacity Buildingof Health Assistants and Other Supervisory Staff(postcard size booklet, spiral binding, 36 pages).4. Learning Material on Leprosy for Capacity Buildingof Medical Offices Working, In Hospital/PHC/CHC anddispensaries (postcard size booklet, spiral binding, 84pages).5. Guidelines on Leprosy for Village Health Workers(fold out photo card).6. Clinical pictures, blister calendar packs for MDT,short explanatory text.

76 REFERENCES & FURTHER READING
From Teaching Aids at Low Cost (TALC)PO BOX 49, St Albans, Hertfordshire, AL1 5TX,United KingdomTel.: +44 (0) 1727 853869 Fax: +44 (0) 1727 846852e-mail: [email protected] Website: www.talcuk.org
Books1. Leprosy for Medical Practitioners and ParamedicalWorkers: S Yawalkar, 1994. Provides basic informationon leprosy and its treatment together with details ofprevention, control and rehabilitation. For medicalstudents and doctors. FREE with paid orders2. Leprosy for Field Staff: A Summers, 1993. Ideal forhealth workers responsible for the diagnosis treatmentand education of leprosy patients. Clearly written withmany excellent illustrations. Price £1.003. Disabled Village Children: D Werner, 1994. Aguide for community health workers, rehabilitationworkers and families written especially for those wholive in rural areas where resources are limited. Alsoavailable in Spanish. Price £10.954. I Can Do It Too (Child-to-Child Reader No 10. Level2), 1989. Three stories which help children recognizethat all children, handicapped or otherwise, havestrengths and weaknesses. It shows disabled childrenhow they can learn to overcome physical disabilitieswith the help and support of other children. Price £2.005. Techniques for the Care of Leprosy Patients: J Harris,1993. A 30-page workbook with checklists of 30important tasks relating to patient care. FREE withpaid orders
Slides (Transparencies)1. Care of the Nerve Damaged Limb: (LPN)1986.Describes how leprosy can cause nerve damage tolimbs, in order to teach patients how to care for theirlimbs and to preserve residual function. Also ideal forhealth workers who care for those with nerve damagefrom any cause. Price £5.00 mounted, £7.00 file/folder or bar
2. Community Based Rehabilitation: (CBR) 1989. Ageneral introduction to the needs of disabled childrenand their families, and the role of the CBR worker.Aimed at health and community workers concernedwith the care of disabled children in Africa. £5.00mounted, £7.00 file/folder or bar3. Leprosy in Childhood: (LP) 1998. A general introduction to leprosy, with particular reference tochildren. Describes treatment with multi-drug therapyAimed at health workers in leprosy areas. Revisedscript. Price £5.00 mounted, £7.00 file/folder or bar
From the Wellcome Trust, Topics inInternational Health, London, UnitedKingdomCD-ROM, Covering the main aspects of leprosy with10 interactive tutorials and approximately 1000images. Includes overview diagnosis, histopathologyand classification, clinical features and classification,prevention and control, immunology, epidemiology,physical and social management. For orders andenquiries: CABI Publishing, CAB International,Wallingford, Oxon, OX10 8DE, United Kingdom. Tel.: +44 (0)1491 832111 Fax: +44 (0)1491 829292 E-mail: [email protected]
From International Resource CentreInternational Centre for Eye Health,Institute of Ophthalmology, 11–43 BathStreet, London, EC1V 9EL, United KingdomTel.: +44 (0) 207 608 6923Fax: +44 (0) 207 250 3207e-mail: [email protected]
Slide text on Leprosy and the Eye. Twenty-four slides(color transparencies) with text on the recognition andtreatment of eye disease in leprosy.