
Family rickettsiaceae: ◦ R. rickettsii ◦ R. prowazekii ◦ R. typhi ◦ Orientia tsutsugamushi ...
17
Rickettsia, Coxiella, Ehrlichia and Anaplasma
-
Upload
arnold-summers -
Category
Documents
-
view
219 -
download
1
Transcript of Family rickettsiaceae: ◦ R. rickettsii ◦ R. prowazekii ◦ R. typhi ◦ Orientia tsutsugamushi ...

Rickettsia, Coxiella, Ehrlichia
and Anaplasma

Family rickettsiaceae:◦R. rickettsii◦R. prowazekii◦R. typhi◦Orientia tsutsugamushi
All are transmitted by arthropod vectors as fleas, ticks, mites and lice.
Rickettsia

Specie Disease Mode of transmission
Geographical distribution
R. Rickettsii Rocky Mountain
spotted fever
Bite of tick North & South America
R. prowazekii Epidemic typhus
Louse faeces Africa, North& South
America
R. typhi Murine (endemic)
typhus
Flea faeces Tropics
O. tsutsugamushi
Scrub typhus Bite of mite Asia & Australia

Mite Body louse
Tick flea
All are obligate intracellular bacteria. Small coccobacilli (0.3-0.5 um) All except orientia have cell wall similar to
gram negative bacteria with LPS & peptidoglycan.
They can be seen by Giemsa stain but not Gram stain.
Do not grow on artificial media. Can be isolated in tissue culture but rarely
done because aerosol transmission can easily occur.
General characteristics
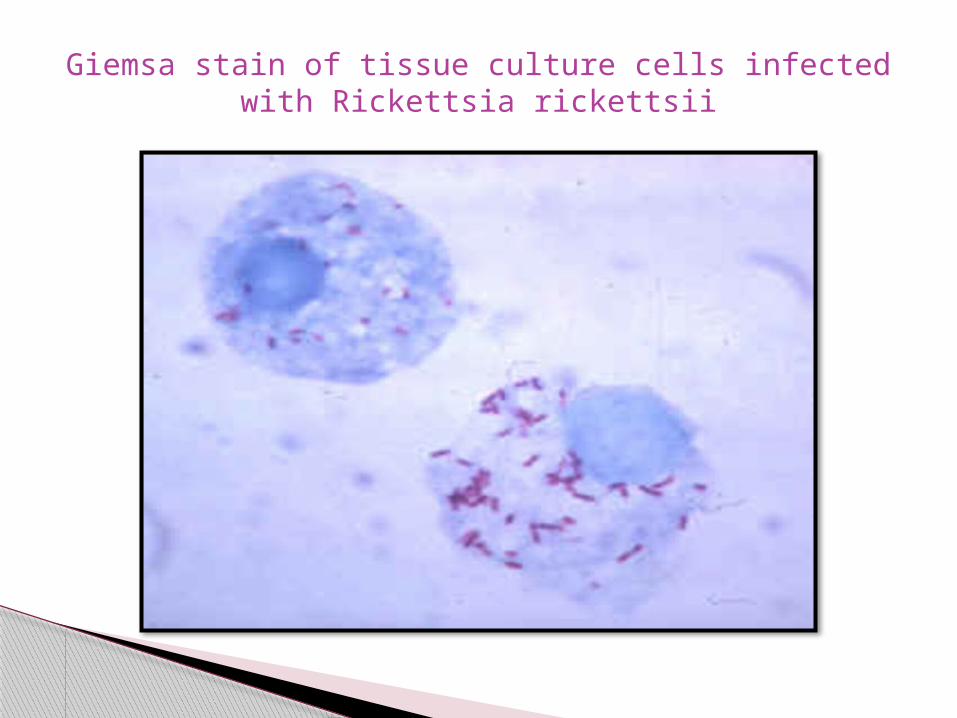
Giemsa stain of tissue culture cells infected with Rickettsia rickettsii

Enter the body through the bite or faeces of arthropod vectors.
Attach to endothelial cells, enter by induced phagocytosis, multiply intracellularly.
Endothelial damage either due to accumulation of large numbers of bacteria (R. prowazekii, R. typhi) or due to cell membrane damage by formation of actin tails and filopodia (R.rickettsii).
This result in widespread microvascular injury; increased vascular permeability with encephalitis and pulmonary edema.
Pathogenesis

Formation of actin tails and leaving the cells through filopodia (R. rickettsii).
Large number of rickettsiae in endothelial cells (R. prowazekii, R. typhi)
Epidemic typhus (R. prowazekii) : Epidemics with high mortality.Fever & macular rash first appear on the
trunk then the extremities.Mild cases resolve within 1-2 days.Sever cases: the rash become hemorrhagic
with hypotension, renal failure and coma.Early treatment is life saving.Reactivation of latent infection may happen
years later.
Clinical features

Murine (endemic) typhus (R. typhi): The same symptoms of epidemic typhus but
rarely fatal.Scrub Typhus (O. tsutsugamushi):Fever, myalgia, maculopapular rash, eschar
and enlarged lymph nodes in the site of the bite.
• Death occurs due to encephalitis and respiratory failure.

Rocky Mountain Spotted Fever:Fever, myalgia, vomiting, diarrhea,
cough and maculopapular rash develop first in the extremities.
Most of the cases are mild. Sever disease is more seen in old patient with hemorrhagic rash, encephalitis, hypovolemia, shock and death.



Timely and accurate diagnosis and appropriate treatment may mean the difference between death and recovery.
However laboratory diagnosis is difficult in the beginning of the disease.◦ Isolation is difficult & hazardous.◦ PCR tests are not always available.◦ Serology will give positive results late in the disease.
Rocky mountain spotted fever can be diagnosed by skin biopsies.
Laboratory Diagnosis

Impossible to be eradicated because they are zoonotic diseases.
Using of repellents, delousing and removing of ticks from skin reduce transmission.
Respond well to antibiotics that enter the cells esp. doxycycline and tetracycline.
Treatment & prevention

World wide distribution. Reservoir: cattle, sheep and goats. Causative agent. C. burnetii; an intracellular,
coccobacilli with gram negative cell wall. Transmission: by inhalation of aerosols
leading to infection of alveolar macrophages. Acute Q fever: fever, myalgia and pneumonia
which is usually self limiting. Chronic Q fever: reactivation of latent bacteria
in the cardiac valves leading to endocarditis. Diagnosis: antibodies detection and PCR.
Coxiella (Q fever)

Caused by ehrlichia and anaplasma respectively. Transmitted by ticks bite. Infect monocytes, macrophages and neutrophils
(low TWBC & platelets). Clinically similar to rocky mountain spotted
fever. 50% of patients need hospitalization for renal
failure, meningoencephalitis and DIC and about 3% die.
Diagnosis: Antibodies detection, Giemsa stain of neutrophils or PCR.
Ehrlichiosis & anaplasmosis
![ESC SSH2 D40 Smart Energy Plan GMCA v2€¦ · r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r d Z ] } µ u v ] u l](https://static.fdocuments.us/doc/165x107/5fefd4335a91d366af5b2c64/esc-ssh2-d40-smart-energy-plan-gmca-v2-r-r-r-r-r-r-r-r-r-r-r-r-r-r-r-r-r-r-r-r-r.jpg)

















![þ Q Éi o Q Éj - エクステリア通販【キロ本店】 · { ]*Ia â { ]*Ia G Da â G Da { ]*Ia ð r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r r rrr rr rr](https://static.fdocuments.us/doc/165x107/5f33ece46c9e825a026a2837/-q-i-o-q-j-ffeefoe-ia-ia-g.jpg)