...Contact Details...
45
SONATINA Clinical Trial Protocol Confidential Eudract No: 2010-020621-40 Page 1 of 45 Version 1.0_12 th Jul 2010 REC No: 10/H0604/61 SONATINA: A Phase II Multi-Centre Randomised Controlled S tudy O f N elfinavir A ddition to Radiotherapy T reatment I n N eo-A djuvant Therapy for Rectal Cancer Version No: Version 1.0 12 th Jul 2010 REC No: 10/H0604/61 EudraCT number: 2010-020621-40 OCTO Protocol No: OCTO_021 Short Title: Nelfinavir Addition to Radiotherapy Treatment for Rectal Cancer Sponsored by the University of Oxford
Transcript of ...Contact Details...

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 1 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
SONATINA: A Phase II Multi-Centre Randomised Controlled Study Of Nelfinavir Addition to Radiotherapy Treatment In Neo-Adjuvant
Therapy for Rectal Cancer
Version No: Version 1.0 12th Jul 2010
REC No: 10/H0604/61 EudraCT number: 2010-020621-40
OCTO Protocol No: OCTO_021
Short Title: Nelfinavir Addition to Radiotherapy Treatment for Rectal Cancer
Sponsored by the University of Oxford

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 2 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Contact Details
Trial Office (OCTO) SONATINA, Oncology Clinical Trials Office Department of Clinical Pharmacology University of Oxford Old Road Campus Research Building Roosevelt Drive Oxford OX3 7DQ, UK
Tel: +44 (0)1865 617089 Fax: +44 (0)1865 617010 Email: [email protected]
Website: http://www.octo-oxford.org.uk Statistician Susan Dutton
Centre for Statistics in Medicine Wolfson College Annexe Linton Road Oxford OX2 6UD Tel: +44(0)1865 284411 Email: [email protected]
Chief Investigator: Dr Ricky Sharma Department Gray Institute for Radiation Oncology and Biology
University of Oxford Old Road Campus Research Building Roosevelt Drive Oxford. OX3 7DQ, UK
Tel: +44 (0)1865 235209 Fax: +44 (0)1865 235981 E-mail: [email protected] Sponsor: The University of Oxford Contact details Ms Heather House
Clinical Trials and Research Governance Team Manor House John Radcliffe Hospital Oxford OX3 9DU
Tel: +44 (0)1865 222757 Fax: +44 (0) 1865 743002 E-mail: [email protected] Lead NHS Trust Oxford Radcliffe Hospitals NHS Trust
R&D Department Manor House John Radcliffe Hospital Oxford OX3 9DU
Tel: +44 (0) 1865 222147 Clinical Queries During office hours clinical queries should be directed to the SONATINA
Trial Office Tel: 01865 617000 The call will be passed on to a SONATINA Clinical Coordinator or an appropriate member of the Trial Management Group. Out of office hours, call the Churchill Hospital switchboard Tel: 01865 741841 and ask for the Oncology Ward. State that the query is for the clinician on-call for the SONATINA Clinical Trial.

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 3 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Randomisation Service
Mon-Fri 09:00-17:00 UK Time, Fax 24 hours* Tel: 0800 3891635 Fax: 0800 3891629 * Faxes received outside office hours will be dealt with the next workingday.
Central Laboratories For tissue biopsies listed in section 7.5 of the protocol:
Professor Quirke Sonatina Trial Pathology and Tumour Biology Leeds Institute of Molecular Medicine University of Leeds St James′s University Hospital Leeds LS9 7TF For Research Blood Assays listed in section 7.5 of the protocol: Sonatina Trial The Oxford Biobank Oxford Biomedical Research Centre Room 4503, Level 4 The John Radcliffe Hospital Headington, Oxford OX3 9DU

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 4 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
TABLE OF CONTENTS Contact Details .......................................................................................................................................2 PROTOCOL SYNOPSIS..........................................................................................................................6 Summary of Schedule of Events ..........................................................................................................9 GLOSSARY OF ABBREVIATIONS ......................................................................................................12 1 INTRODUCTION ........................................................................................................................14
1.1 Locally advanced rectal cancer ..................................................................................................14 1.2 Radiosensitisation by Nelfinavir..................................................................................................15 1.3 Safety of addition of Nelfinavir to standard radiotherapy............................................................16 1.4 Tumour cell density.....................................................................................................................18 1.5 Changes in tumour perfusion......................................................................................................18
2 Objectives and Endpoints........................................................................................................19 Primary objective................................................................................................................................19
3 Study Design .............................................................................................................................19 3.1 Patient numbers and recruitment................................................................................................19
4 Patient Selection .......................................................................................................................19 4.1 Inclusion criteria: .........................................................................................................................19 4.2 Exclusion criteria:........................................................................................................................20 4.3 Patient screening and enrolment ................................................................................................21
5. Protocol Treatment ...................................................................................................................21 5.1 Investigational medicinal product................................................................................................21 5.2 Radiotherapy...............................................................................................................................21
5.2.1 Simulation and Immobilization 21 5.2.2 Definition and delineation of the target volumes 22 5.2.3 Delineation of Organs at Risk 22
5.3 Treatment Planning and Verification...........................................................................................22 5.4 Treatment Delivery and Total Dose: ...........................................................................................22 5.5 Dose Volume Constraints: ..........................................................................................................23 5.6 Radiotherapy Quality Assurance ................................................................................................23
6 PHARMACEUTICAL AND PHARMACOLOGICAL INFORMATION........................................23 6.1 Supply and storage .....................................................................................................................23 6.2 Drug formulation .........................................................................................................................23 6.3 Labelling......................................................................................................................................24 6.4 Dispensing ..................................................................................................................................24 6.5 Drug accountability .....................................................................................................................24 6.6 Study Drug Administration and compliance check .....................................................................24 6.7 Study Drug ..................................................................................................................................24 6.8 Contraindications ........................................................................................................................25 6.9 Undesirable effects .....................................................................................................................25 6.10 Dose reductions ..........................................................................................................................25
7 CLINICAL AND RADIOLOGICAL EVALUATION.....................................................................25 7.1 Pre-study procedures..................................................................................................................25 7.2 Mandatory procedures while on study ........................................................................................26 7.3 Tissue donation...........................................................................................................................27 7.4 Surgery and Pathology ...............................................................................................................28 7.5 Bloods for Research Assays.......................................................................................................28 7.6 Custodianship, labelling and confidentiality of clinical samples...............................................29
8 ASSESSMENT OF SAFETY......................................................................................................29 8.1 Adverse Event Definitions...........................................................................................................29
8.1.1 Adverse Event 29 8.1.2 Serious Adverse Events (SAEs) 30
8.2 SAEs which do not require immediate reporting ........................................................................30

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 5 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Confidential
8.3 Clinical laboratory abnormalities and other abnormal assessments as AEs/SAE’s .................31 8.4 Toxicity due to Study Drug..........................................................................................................31 8.5 Adverse Drug Reaction (ADR)....................................................................................................31 8.6 Unexpected Adverse Reaction ...................................................................................................31 8.7 Suspected Unexpected Serious Adverse Drug Reaction (SUSARs) .........................................31 8.8 Causality of AEs..........................................................................................................................32 8.9 Adverse Event Reporting............................................................................................................32
Serious Adverse Events (SAEs) 32 8.10 Follow-up of adverse events.......................................................................................................33 8.11 Expedited Safety Reporting ........................................................................................................33 8.12 Safety updates ............................................................................................................................33 8.13 Annual Safety and Annual Progress Reports (ASR and APR)...................................................33
9 Early Patient Withdrawal..........................................................................................................34 10 Defining the end of trial............................................................................................................34 11 DATA ANALYSIS.......................................................................................................................34
11.1 Statistical considerations ...........................................................................................................34 11.2 Safety Cohort ..............................................................................................................................35 11.3 Measures to be taken in the case of missing, unused and false data........................................36 11.4 Choice of the patients who are included in the analysis.............................................................36
12 TRIAL ADMINISTRATION .........................................................................................................36 12.1 Regulatory and ethical considerations..................................................................................36 12.2 Regulatory authority approval .....................................................................................................36 12.3 Ethical conduct of the trial and ethics approval ..........................................................................36 12.4 Trial monitoring ...........................................................................................................................37 12.5 Quality assurance .......................................................................................................................37 12.6 Case record retention .................................................................................................................37 12.7 Patient confidentiality ..................................................................................................................38 12.8 Completion of the Case Report Form (CRF) ..........................................................................38 12.9 Clinical study report ....................................................................................................................38 12.10Funding and Indemnity Arrangements......................................................................................38 12.11Publication Policy and Acknowledgements ..............................................................................39
13 REFERENCES ...........................................................................................................................41 APPENDIX 1: ECOG PERFORMANCE STATUS EVALUATION........................................................44 APPENDIX 2: RECIST CRITERIA FOR EVALUATION OF RADIOLOGICAL RESPONSE ...............45

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 6 of 45 Version 1.0_12 Jul 2010 REC No: 10/H0604/61
Confidential
th
PROTOCOL SYNOPSIS
Title of study A Phase II Multi-Centre Randomised Controlled Study Of Nelfinavir Addition to Radiotherapy Treatment In Neo-Adjuvant Therapy for Rectal Cancer (SONATINA)
Chief Investigator Ricky Sharma Scientific rationale A broad spectrum of cancer cell lines are sensitized to radiation after treatment
with Akt inhibitors. The HIV protease inhibitor (HPI) Nelfinavir has shown synergy with ionising radiation. In addition to Akt inhibition, Nelfinavir has been shown to reduce hypoxia and to normalise tumour vasculature in preclinical models, which contribute to radiosensitisation effects.
Clinical rationale The strategy of short course radiotherapy (SCRT) followed by systemic combination chemotherapy has recently been adopted in patients with resectable metastatic disease, in whom the planning and delivery of long-course radiotherapy may delay delivery of full-dose systemic therapy and potentially compromise surgical treatment of metastatic disease. In this group of patients, the use of systemic chemotherapy during the interval between SCRT and surgery allows delivery of full dose systemic treatment and may potentially contribute to the down-sizing effect of SCRT. Several clinical studies suggest that SCRT with delayed surgery is a reasonable treatment approach for patients with metastatic disease who require palliation of symptoms from the primary tumour or down-sizing of primary tumour by a sequential combination of SCRT and systemic combination chemotherapy. This study will add a radiosensitising agent to radiotherapy treatment to try to improve the response rate, measured by tumour cell density (TCD) in the primary tumour. In order to ensure that TCD measured in the subject group of this trial is consistent with historical data from patients in larger trials who have received short-course radiotherapy (SCRT) and to ensure that it is consistent with other contemporary trials measuring TCD in patients with rectal cancer, the trial will include a control arm as a reference arm. The study drug has been tested with radiotherapy in a phase I study in pancreatic carcinoma, which showed the drug to be well tolerated at the dose proposed in this trial when the study drug was administered in conjunction with cisplatin and gemcitabine chemoradiotherapy.
Total Patient Number: 80 patients (60 patients in the active arm and 20 patients in the control arm – 3:1 allocation)
Duration of study recruitment 24 months Aims: To investigate the safety and the activity of the radiosensitising drug, Nelfinavir,
administered before and during radiotherapy in patients with rectal carcinoma. An additional aim of the study is to test the feasibility of using Tumour Cell Density (TCD) as a primary endpoint in clinical trials of radiosensitising agents administered with short-course radiotherapy (SCRT).
Primary endpoints: Tumour cell density in biopsy taken 7 days from last fraction of radiotherapy Secondary endpoints: • Incidence of any grade 3 or higher non-haematological or haematological
toxicity (according to CTCAE v 4.0) up to 6 months from last fraction of radiotherapy
• Radiological response of primary tumour at 8 weeks post SCRT • Proportion of patients proceeding to resectional pelvic surgery within 6
months from last fraction of radiotherapy Exploratory studies: • Changes in tumour perfusion on dce-MRI and pCT pre- and during
radiotherapy with and without the study drug Study design: A multi-centre, randomised phase II trial of SCRT with or without the addition of
the study drug, Nelfinavir, including a run-in period to assess safety at a single centre, before expansion to multiple centres. Since the trial is not blinded, there will be no placebo for patients in the control arm.
Inclusion criteria:
1. Histologically proven adenocarcinoma of the rectum (tumour ≤ 15 cm from anal verge)
2. Radiological evidence of M1 disease
3. Treatment intent of SCRT is either down-sizing prior to delayed surgery ≥ 8 weeks) or palliation of symptoms from rectal cancer
4. Colorectal Multidisciplinary Team (MDT) with surgical representation must

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 7 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
document that patient is suitable for SCRT as primary treatment. In patients considered for systemic chemotherapy as standard (non-protocol) therapy prior to surgery, chemotherapy should commence ≥ 14 days from the last fraction of SCRT. Patients should be imaged 8 weeks from the last fraction of radiotherapy and considered for pelvic surgery if sufficiently downsized
5. Serum bilirubin ≤ 3x normal
6. AST or ALT ≤ 3x normal
7. Creatinine clearance > 50 ml/min
8. WBC ≥ 3.5/µl; platelets ≥ 100.0/µl; haemoglobin ≥ 10 g/dl
9. Age ≥ 18 years
10. ECOG performance status 0-2
11. Able to give written informed consent
12. Willing and able to comply with the study procedures, including biopsy of the primary tumour 7 days from the last fraction of SCRT
Exclusion criteria: 1. Operable primary tumour at time of study entry, for which the Colorectal MDT decide that surgery should be the primary treatment
2. Previous pelvic radiotherapy
3. Other experimental treatment ≤ 4 weeks prior to this study (including chemotherapy and immunotherapy)
4. History of other malignancy less than 2 years before the diagnosis of rectal cancer, excluding the following: Non-melanoma skin cancer, in situ carcinoma of the cervix treated surgically with curative intent, other malignant tumours that have been treated surgically and that have a disease-free survival of ≥10 years
5. Recent (< 2 months) severe cardiac disease (e.g. arrhythmia, congestive heart failure, infarction)
6. Active infections (including chronic hepatitis type B or C and HIV infection if status known), severe immunologic defect, compromised bone marrow function
7. Haemophilia A and B, phenylketonuria
8. Known hypersensitivity to Nelfinavir or other HIV protease inhibitor
9. Concurrent use of drugs with a narrow therapeutic window and which are substrates of cytochrome P450 (CYP) 3A (CYP3A4), that cannot be substituted by other drugs and that may not be discontinued during study treatment (e.g. phenobarbital, carbamazepine, phenytoin, terfenadine, astemizole, cisapride, amiodarone, quinidine, pimozide, triazolam, midazolam, ergotamines, rifampicin, herbal preparations that contain Saint John's wort, Hypericum perforatum, omeprazole, simvastatin, lovastatin or atorvastatin, sildenafil or methadone)
10. Pregnant or breastfeeding
11. If a woman of child bearing potential, unable or unwilling to use effective contraception during participation in the trial. Contraceptives that contain norethisterone and ethinylestradiol should be replaced by an alternative contraceptive or contraceptive method
12. Major systemic co-morbidities preventing safe participation in the trial (this will be determined by the local PI)
13. Major psychiatric illness currently or within the past 12 months
14. Any other condition or therapy that may represent a risk for the patient in the judgement of the treating physician or that could interfere with the aim of the study

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 8 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Confidential
Protocol Radiotherapy Radiotherapy delivered in fractions of 5 Gy daily from Wednesday, day 1, to Tuesday, day 7. Radiotherapy will only take place between Monday to Friday and not on a Saturday and Sunday. Total dose is 25 Gy prescribed to the ICRU reference point. Radiotherapy technique can be 3D-conformal or IMRT.
Study Drug Nelfinavir is administered orally 1250 mg bd from day -7 (the Wednesday prior to Wednesday (Day 1) on which radiotherapy commences) to the last day of radiotherapy (Tuesday, day 7).
Duration of study drug treatment
14 days
Assessment of primary endpoint
Biopsy performed 7 days (+/- one day) from the last day of radiotherapy (i.e. Tuesday).
Patient care post-trial study drug
Follow-up every 4 weeks until 6 months from last fraction of radiotherapy. There will be a gap of no treatment for 14 days from last fraction of radiotherapy.
Statistical Considerations Systematic data for TCD rates following long-course chemo-radiation or short-course radiotherapy followed by systemic chemotherapy have not been published for this patient population. The reference arm of the trial (no study drug) is therefore necessary to provide reassurance that the TCD rate is acceptable as a primary endpoint compared to historical data from other patient groups. Sample size has been calculated using Fleming’s one-stage single arm phase II trial method, with 80% power, alpha=5%, TCD expected from control arm=30% (reduced from 50% at baseline), TCD expected from active arm=15% (reduced from 50% at baseline) and allowing for 10% loss-to-follow-up requires 60 patients in the active arm. With a randomisation allocation of 3:1, 20 patients are required in the control arm. Therefore a total of 80 patients will be randomised to the trial overall.
Safety Dose limiting toxicity has not been observed in a phase I trial of oral Nelfinavir 1250 mg bd performed with higher doses of radiotherapy plus concomitant chemotherapy. Since Nelfinavir has not previously been combined with 5 Gy fractions of radiotherapy delivered to the pelvis, there will be an interim analysis of the safety cohort, which consists of 8 patients on active treatment who have been followed up for 28 days from the last fraction of radiotherapy. Recruitment will be paused for 2 months while the interim analysis is carried out on these 8 patients.

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 9 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Confidential
Summary of Schedule of Events
Pre-treatment 6 Daily from Wed (Day -7) to Tues (Day 7) 4
Day -1 (i.e. the day before the first dose of RT)
Daily from Wed (Day 1) to Tues (Day 7), excluding Sat and Sun 5
On last day of RT (Day 7)
7 days after completion of RT11 (Day 14 +/- 1 day)
8 weeks from last fraction of radiotherapy (+/- 2 weeks)
Every 4 weeks from last day of radiotherapy for 5 months ( +/- 2 weeks)
Withdrawal14
Visit or 6 month from last fraction of radiotherapy ( +/- 2 weeks)
EVENTS CONSISTENT WITH STANDARD NHS THERAPY
History and physical exam This includes weight, height, ECOG status and vital signs
X X
X X
Histology (previously taken as part of routine care)15
X
Diagnostic MRI scan pelvis 8,9 X X
Diagnostic CT scan thorax, abdomen, pelvis X X
Treatment planning CT scan (for SCRT) X Radiotherapy treatment 5,7 X FBC+diff 1 X X
X X
Serum chemistries 2 X X X X
Pregnancy test Applicable to adults of child bearing age X
Serum tumour markers 3 X X X EVENTS SPECIFIC TO CLINICAL TRIAL:
Complete informed consent A X Diagnostic scans: perfusion CT and DCE-MRI pelvis 10 X X X
Blood for research assays13 X X X Nelfinavir dosing4 X Tumour biopsies X Optional Tumour biopsies (complete Consent Form B) 12 X
CTCAE v 4.0 X X X X X X 1 FBC: Haemoglobin, leukocytes, platelets, differential blood count 2 Clinical chemistry: electrolytes, calcium, creatinine, bilirubin, alkaline phosphatase, magnesium, ALT, albumin, glucose (non-fasting), Urea 3 CEA, CA125 and CA19.9 (only repeated if initial sample at pre treatment is elevated above normal range for each investigational site) 4 Applicable to first 8 patients in clinical trial and then only patients randomised to active treatment arm: Nelfinavir 1250 mg bd each day (7 days per week) from day -7 (Wednesday) to last day of RT (Tuesday)

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 10 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Confidential
5 5 Gy delivered daily from first (Day 1) to last day (Day 7), excluding weekends, of radiotherapy (total dose prescribed to ICRU reference point = 25 Gy) 6 Within 4 weeks of commencement of dosing with Nelfinavir 7 Any oncological intervention, including standard systemic chemotherapy, is permitted ≥14 days from the last fraction of radiotherapy. 8 RECIST measurements of primary tumour required on pre-treatment and post-treatment MRI scans (see Appendix 2) 9 Imaging must be reviewed at Multi-Disciplinary Team Meeting with surgical representation. 10 Perfusion CT and DCE-MRI scans according to standard protocols: If tolerated, both modalities will be performed. If patients are unable to tolerate both scans, only perfusion CT will be performed. Only at applicable centres where these modalities are available. 11 Prior to commencement of systemic chemotherapy 12 See section 7.3 Optional biopsy performed only in patients who offer informed consent on Consent Form B. 13 See section 7.3 Assay 1 is completed at pre treatment timepoint only, whereas assay 2 is done pre treatment, day -1 and last day of radiotherapy. 14 Visit to be done at 6 months post last fraction of radiotherapy or at any time for those patients that withdraw from the study. 15 Needs to be performed within 6 months of study entry.

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 11 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Confidential
SONATINA Trial Outline
Inoperable rectal adenocarcinoma with M1 disease: Documented at MDT as suitable for initial treatment by SCRT
R*
Biopsy to assess primary endpoint of trial
5 x 5 Gy daily in one week Plus study drug (Nelfinavir): 1250 mg bd for 7 days prior to RT and during 7 days of RT
5 x 5 Gy daily in one week
7 days from last fraction of radiotherapy
Biopsy to assess primary endpoint of trial
First 8 patients enter the safety cohort and will all receive active treatment
Systemic chemotherapy may commence ≥14 days from last fraction of radiotherapy, with re-imaging after 6 weeks of chemotherapy with a view to pelvic surgery
R* = randomisation (3:1 in favour of study drug arm)

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 12 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Confidential
GLOSSARY OF ABBREVIATIONS
5FU 5–Fluorouracil HDPE High Density Polyethylene
AE Adverse Event HIV Human immunodeficiency virus
ALT Alanine aminotransferase, ICRU International Commission on Radiation Units
APR Abdomino-peritoneal resection of the rectum IMRT Intensity Modulated Radiotherapy
AR Adverse Reaction INR International Normalisation Ratio
AST Aspartate aminotransferase ITT Intention To Treat
bd Twice daily IV Intravenous
BRC NIHR Biomedical Research Centre Oxford LFT Liver Function Tests
CCOG Colorectal Clinical Oncology Group LV Leucovorin (folinic acid)
CDK Cyclin Dependent Kinase MREC Multi-centre Research Ethics Committee
CEA Carcinoembryonic Antigen MRI Magnetic Resonance Imaging
CERES Consumers for Ethics in Research MDT Multi-Disciplinary Team
CR Complete Response MTD Maximum Tolerated Dose
CRC Colorectal Cancer NCI-CTC National Cancer Institute Common Terminology Criteria
CRF Case Report Form NHS National Health Service
CRM Circumferential resection margin NCRN National Cancer Research Network
CRT Chemoradiotherapy pCR Pathological Complete Response
CT Computed Tomography pCT Perfusion computed tomography
CTA Clinical Trial Authorisation PD Progressive Disease
CTC Cancer Trials Centre PR Partial Response
CTV Clinical Target Volume PRN As necessary
CTCAE Clinical toxicity grade adverse event scoring PTV Planned Target Volume
dce-MRI Dynamic contrast-enhanced MRI RECIST Response Evaluation Criteria In Solid Tumours
DLT Dose Limiting Toxicity RT Radiotherapy
DNA Deoxyribose Nucleic Acid SAE Serious Adverse Event
DPD Dihydropyrimidine dehydrogenase SCRT Short Course Radiotherapy
ECG Electrocardiogram SCRTds Short Course Radiotherapy followed by delayed surgery

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 13 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Confidential
ECOG Eastern Co-operative Oncology Group SD Stable Disease
ECMC Experimental Cancer Medicine Centre Network SGPT Serum glutamic pyruvic transaminase
EGF Epidermal Growth Factor SPC Summary of Product Characteristics
EGFR Epidermal Growth Factor Receptor SUSAR Suspected Unexpected Serious Adverse Reaction
ESTRO European Society for Therapeutic Radiology & Oncology TCD Tumour Cell Density
FBC Full Blood Count TGFα Transforming growth factor alpha
GFR Glomerular filtration rate TMG Trial Management Group
GI Gastrointestinal TP Thymydylate Phosphorylase
GMP Good Manufacturing Practice TS Thymidylate Synthase
GP General Practitioner U&E Urine & Electrolytes
GTV Gross Target Volume UICC International Union Against Cancer
Gy Gray ULN Upper Limit of Normal
HFS Hand-Foot Syndrome US Ultrasound
HTA Human Tissue Authority WBC White Blood Count

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 14 of 45 Version 1.0_12th Jul 2010
1 INTRODUCTION
1.1 Locally advanced rectal cancer
Colorectal cancer is the third most frequently occurring cancer in the UK. Over 36,000 new cases of colorectal cancer are diagnosed each year in the UK (Cancer Research UK website, accessed 1st December 2009). At least half of all patients with operable or potentially operable rectal cancer are currently considered for preoperative radiotherapy as a routine part of their optimum management. Short course radiotherapy (SCRT), consisting of 25 Gy delivered in 5 daily fractions in one week, followed by surgery within 5-7 days is currently offered to patients with operable rectal cancer since it has been shown to halve the risk of local recurrence [1,2]. Long-course pre-operative chemo-radiotherapy [LCCRT] with delayed surgery at 6-12 weeks has been shown to lead to tumour down sizing, tumour regression by histological grade and pathological complete responses, which correlate with improved outcome for patients [3-5]. In the UK, current indications for pre-operative LCCRT (i.e. a total dose of radiotherapy 45-50.4 Gy delivered in 1.8 Gy fractions over 5-6 weeks, with concomitant fluoropyrimidine chemotherapy) include: Advanced primary tumour where the surgeon is unlikely to perform a R0 resection; tumour beyond or ≤ 2 mm from mesorectal fascia; tumours that may be amenable to low anterior resection rather than abdomino-perineal excision if clinically downsized by RT. Although the combination of radiotherapy and capecitabine (or infusional 5-fluorouracil) is generally well tolerated, some patients are not fit for concomitant chemotherapy with radiotherapy and those patients are treated with radiotherapy alone. Across the UK, the clinical management of patients who have a locally advanced primary tumour and synchronous resectable or potentially resectable metastatic disease is not uniform. A wide range of treatment options are currently practised. These include LCCRT first, although this strategy often results in progression of metastatic disease during planning and delivery of LCCRT, or systemic chemotherapy first, although this strategy may not rapidly palliate symptoms from the primary tumour, nor may it achieve adequate downsizing of the primary tumour without prolonged (> 3 months) of treatment. Concerns have been raised in the treatment of several solid cancers that the use of systemic chemotherapy prior to radical radiotherapy may compromise the efficacy of the latter [6]. The biologically effective dose of SCRT is of a similar magnitude to 45 Gy in 25 fractions [7]. The CR07 study of SCRT followed by immediate surgery suggested that a significant T-stage downstaging effect [p=0.0001] occurred in the SCRT group despite the short time interval (i.e. days) between the last fraction of RT and surgery. Several clinical trials are currently ongoing to study SCRT followed by delayed surgery at 6-8 weeks [SCRTds] to study if sufficient downstaging occurs with this treatment to enable curative resection. A retrospective series studied 46 patients with non-resectable rectal cancer [+/- synchronous metastasis] who were treated with SCRTds because of advanced age, comorbidities or synchronous metastatic disease: 70% [32/46] of the patients were able to undergo resection and pCR was documented in 12.5% of the resected patients [8]. A further series of 43 patients with resection margin-threatened disease on MRI who underwent SCRTds has been reported; all patients were not considered fit for LCCRT [9].The median age was 82 years and 26 patients subsequently underwent surgery. R0 resection was achieved in 22/26 patients and median survival and 18-month local disease free survival was reported as 44 months and 0%, respectively, in patients undergoing R0/R1 resection. With regard to toxicity, only 2 patients were admitted with diarrhoea and late bowel toxicity was reported in 1 patient only. Further to these published series, the downsizing effect of SCRT has been reported in an interim analysis of the Stockholm III, prospective randomised Phase III study [10]. In this study, patients were randomised between a) SCRT, immediate surgery b) SCRTds and c) long course RT [50 Gy in 25 fractions] followed by delayed surgery at 6 weeks (LCRTds). Concomitant chemotherapy was not offered in this trial. In the interim analysis, there was no statistical difference between acute radiation toxicity, surgical complication rates and rates of re-operation between the SCRTds and LCRTds arms. Pathological complete response (pCR) was documented in 12.5% [15/120] of patients in the SCRTds arm and 5% [3/65] in the LCRTds arm [10]. These pCR rates are consistent with a recent, randomised Phase III study comparing neoadjuvant LCRTds and LCCRTds in un-resectable rectal cancer, which reported pCR rates of 7% and 16%, respectively [11]. Considered collectively, these data suggest that SCRTds is at least as efficacious as LCRTds, and one may speculate that it is an acceptable alternative to LCCRT if it is followed sequentially with systemic combination chemotherapy.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 15 of 45 Version 1.0_12th Jul 2010
The strategy of SCRT followed by systemic combination chemotherapy has recently been adopted in patients with resectable M1 disease, in whom the planning and delivery of long-course radiotherapy may delay delivery of full-dose systemic therapy and potentially compromise surgical treatment of metastatic disease. In this group of patients, the use of systemic chemotherapy during the interval between SCRT and surgery allows delivery of full dose systemic treatment and may potentially contribute to the down-sizing effect of SCRT. A recent study has reported tumour regression in resectable patients treated with pre-operative systemic therapy alone – all patients [n=27] who completed 6 weeks of FOLFOX with bevacizumab [Cycles 1-4] showed tumour regression and proceeded to R0 resection; pCR was documented in 26% of the resected cases [12]. Moreover, a separate recent study of SCRT followed by CAPOX-bevacizumab has shown that radical resection and/or RFA of primary and all metastatic disease was possible in 85% cases. Consistent with the previous report, these investigators reported a pCR rate of 22.5% in resected rectal specimens [13]. The clinical studies reviewed above suggest that SCRTds is a reasonable strategy to treat patients with metastatic disease who require palliation of symptoms from the primary tumour or down-sizing of primary tumour by a sequential combination of SCRT and systemic combination chemotherapy. The early and late toxicity profile of SCRT is well documented in patients proceeding to immediate surgery [reviewed in 2], including quality of life indices [14]. Notable long-term toxicities of SCRT include loss of fertility in men and premenopausal women, sexual dysfunction, long-term impairment of bowel function and incontinence, a significant delay in healing of the perineal wound after abdominoperineal excision and an increased risk of second malignancy with the use of adjuvant radiotherapy [15,16]. Interestingly, long-term toxicity does not appear to differ between SCRT and long-course chemo-radiotherapy when both are used in the neo-adjuvant setting [17,18]. With regard to acute radiation-induced toxicity, interim analysis of the Stockholm III study stated that equivalent toxicity rates were seen with SCRT plus delay versus long-course radiation therapy [10]. In that study, approximately 4-5% of patients treated with either SCRT or with long-course radiation required admission to hospital for vomiting, diarrhoea with dehydration, constipation, vaginal bleeding or lower back pain. Other common early side effects of pelvic radiotherapy include fatigue, weight loss, and radiation skin reaction.
1.2 Radiosensitisation by Nelfinavir
A known factor increasing cellular resistance to radiation is the over-expression of activated oncogenes, such as the epidermal growth factor receptor (EGFR) [19], RAS [20] or the loss of the tumour suppressor gene PTEN [21]. An important observation in this respect is that these mutations share a common molecular signal pathway that activates the phosphatidylinositol 3-kinase (PI3K)-Akt-pathway. It has been shown that the blockage of PI3K can augment response to radiation in vitro and in vivo. This effect is only present in cells which have a constitutive activation of this pathway, however not in cells with a non-activated pathway [22-24]. Down regulation of Akt with siRNA also leads to radiosensitisation of these cells [25]. Since this signalling pathway is often activated in tumour cells, yet not in host cells, it is a good target candidate to increase radiation sensitivity. Two PI3K-inhibitors, LY294002 and wortmannin, which are often used in vitro for inhibition and provide radiation sensitizing effects, are poorly tolerated in vivo and of very limited clinical use [26]. These findings have led to the suggestion of the possibility of using HIV-protease inhibitors (HPIs) as clinical radiosensitisers, since they interfere with the PI3K-Akt-signalling pathway. These compounds are currently used in therapeutic schedules for patients with HIV infections. Nelfinavir, a synthetic antiretroviral agent, is a nonpeptidic HPI. Nelfinavir is approved for use in combination with other antiretroviral agents for the treatment of HIV infection in adults and children 2 years of age or older. HPIs are peptidomimetics that inhibit the HIV-aspartylprotease, a retroviral enzyme, which cleaves the viral gag-pol polyprotein and which is necessary for the production of infectious virus particles [27]. A side effect of long term HPI treatment is resistance to insulin and consequent diabetes mellitus [28,29]. The inhibition of the PI3K-Akt signalling axis in tumour cells by HPIs was tested, because Akt, particularly the isoform Akt2 [30], play a key role in the coordinated regulation of growth and metabolism [31,32]. An initial study [32] used the HPI, saquinavir, in tissue culture to sensitize to radiation. Another study [26] demonstrated that three out of five analysed HPIs are capable of inhibiting Akt in their routinely used clinical doses. These compounds were found to sensitize tumour cells in vitro and in vivo to ionizing radiation.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 16 of 45 Version 1.0_12th Jul 2010
The antitumour effects of HPIs have been attributed to several effects (reviewed in [33]). Among the proposed molecular tumour targets of HPIs are the proteasome, matrix metalloproteases (MMPs) and integrins. Non-Akt related effects of proteasome inhibition include elevated ER stress, increased protein turnover, reduced clearance of misfolded proteins, apoptosis induction, degradation of tumour-suppressor gene products, altered function of CDK-inhibitors and of NF-κB, and blockage of the inflammatory response. HIV protease-induced MMP inhibition also has immunomodulatory effects, as well as antiangiogenic effects. A recent study reported the sensitization of endothelial cells to radiation by Nelfinavir mediated by up-regulation of apoptosis in this cell type, with a significant reduction of tumour vessel density after combined treatment [34]. Other antitumour mechanisms of HPIs include the inhibition of inflammatory cytokine production, immunomodulation, induction of apoptosis and of autophagy [35]. In summary, these data demonstrate a number of potential mechanisms of the radiosensitizing effects of HPIs that have been identified in the laboratory. In vitro data with seven pancreatic carcinoma cell lines that have activating KRAS-mutations have shown radiosensitisation with the PI3-kinase inhibitor LY249002. Furthermore, a pancreatic carcinoma line of the panel of the cell lines tested for radiosensitisation with Nelfinavir was described to be sensitised [26]. Since approximately 40% of colorectal cancer is KRAS mutant (and approximately 60% is wild type), it should be noted that radiosensitisation of cell lines by Nelfinavir in this study was independent of KRAS status [26]. This feature is an important factor in considering the potential of radiosensitising drugs for clinical use in the treatment of colorectal cancer. Nelfinavir, when added to the mucosal or serosal side of HT-29/B6 colon cancer cell monolayers, has been shown to induce apoptosis of tumour cells [36].
1.3 Safety of addition of Nelfinavir to standard radiotherapy
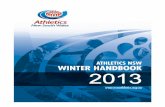
Nelfinavir is well tolerated in patients with HIV infection and has a good safety profile with low rates of toxicity and treatment-related discontinuations [37]. The most common acute side effects of Nelfinavir are gastrointestinal. The diarrhoea related to Nelfinavir is generally mild or moderate in intensity, occurs at the initiation of therapy and is generally easily managed. Patients who are on long-term Nelfinavir for HIV infection may develop problems with dyslipidemia [38] and insulin resistance [29], but this adverse effect is rarely problematic in patients treated for the short timescale proposed in this trial. HPIs have been used in HIV-positive patients for over 2 decades and their pharmacokinetics are well characterised. These drugs are generally well tolerated, including in HIV-positive patients who have received concomitant radiotherapy for a variety of malignancies. In a report by Oehler-Jänne et al., treatment with chemoradiation of HIV-negative patients and HIV-positive patients undergoing HAART was compared [39]. There was no difference in acute nor in late toxicity between both groups. Phase I trials of Nelfinavir with radiation A phase-I-study of Nelfinavir for 7 weeks plus chemo-radiation has been performed in 12 patients receiving cisplatin and gemcitabine plus 50.4 Gy in 28 daily fractions for locally advanced pancreatic cancer [40]. Nelfinavir reduced Ser473-phospho-Akt levels in the leukocytes of evaluable patients, as shown in Figure 1.
Figure 1 Determination of the Ser473-phosphorylation status of Akt prior to treatment with Nelfinavir and during treatment in peripheral blood mononuclear cells in 8 / 10 patients who completed therapy. β-actin was used to control for loading on Western blots. Quantification was related to β-actin. One patient at dose level 1 (DL1) discontinued treatment after week 2 because of clinical depression; the patient had a history of psychiatric illness. Metastasis-related acute cholecystitis in another patient (DL2) caused treatment to be aborted after week 3 (see below) in favour of palliative chemotherapy. The other 10 patients completed chemo-radiation as planned. No dose reductions of gemcitabine or cisplatin were necessary. Mean Nelfinavir intake was 94% at DL1 and 96% at DL2. DL2 in this phase I trial [40] is consistent with the dose of Nelfinavir (1250 mg bd) to be applied in the SONATINA
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 17 of 45 Version 1.0_12th Jul 2010
trial. One patient at each DL had reduced Nelfinavir intake because of non-compliance (82%) and loss of appetite (87%), respectively. The frequencies of grade 3 and 4 toxicities observed during chemoradiation are outlined in Table 1. Observed haematological toxicities reached grade 3 and consisted mostly of leukopenia. Patients in DL2 did not experience more severe haematological toxicity, and no dose limiting haematological toxicities (grade 4) were observed. Non-haematological toxicities did not occur at a higher frequency at DL2. Grade 3 nausea and vomiting occurred in one patient at each dose level, and grade 3 upper abdominal toxicity occurred in one patient at DL1. This patient experienced grade 3 abdominal pain on days 10 to 12 of protocol therapy. Biliary obstruction due to stent blockage (a common occurrence in patients with advanced pancreatic cancer) occurred in 2 patients, unlikely to be related to protocol therapy. All symptoms quickly disappeared after replacement of the biliary stent in both patients. Grade 4 cholecystitis occurred in another patient at DL2 during week three, and treatment had to be interrupted after 27 Gy. This patient was re-evaluated and diagnostic procedures revealed progressive malignant disease. Another patient at DL 2 had grade 3 nausea and an episode of vomiting after chemotherapy. The symptoms responded to therapy with a 5-HT3-receptor antagonist. Table 1. Acute toxicity recorded in phase I trial of Nelfinavir (7 weeks) plus chemo-radiation (total dose radiotherapy 50.4 Gy with concomitant cisplatin and gemcitabine chemotherapy) in 12 patients with pancreatic cancer NCIC–CTC Grade Parameter
0-2* 3 4
Leukopaenia DL1 DL2
8 3 5
4 3 1
- - -
Neutropaenia DL1 DL2
9 4 5
3 2 1
- - -
Thrombocytopaenia DL1 DL2
10 5 5
2 1 1
- - -
Anaemia DL1 DL2
12 6 6
- - -
- - -
NCIC–CTC Grade Parameter
0-2* 3 4
Nausea/Vomiting DL1 DL2
10 5 5
2 1 1‡
- - -
Upper GI DL1 DL2
11 5 6
1 1‡ -
- - -
Diarrhoea DL1 DL2
12 6 6
- - -
- - -
Transaminases DL1 DL2
10 5 5
1 1† -
1 - 1†
Bilirubin DL1 DL2
10 4 6
2 2† -
- - -
Alkaline phosphatase DL1 DL2
11 5 6
1 1† -
- - -
Infection DL1 DL2
9 5 4
2 1† 1†
1 - 1†
Abbreviations: DL, dose level; GI, gastrointestinal. *Toxicity was defined according to the National Cancer Institute Common Toxicity Criteria. †Not graded as DLT (for details see text), ‡graded as DLT, acute cholecystitis.
Since the incidence of adverse events described above was in keeping with those expected from standard chemo-radiation therapy for this disease, none of the observed toxicities were thought to be related to Nelfinavir treatment. A maximim tolerated dose (MTD) was not defined and DL2 was identified as the recommended dose for a phase II trials. No further dose escalation has been
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 18 of 45 Version 1.0_12th Jul 2010
performed in this trial because Nelfinavir was reliably found to inhibit phosphorylation of Akt at 2 x 1250 mg per day [33] (figure 1 above).
1.4 Tumour cell density
Similar to all other malignant epithelial tumours, CRC is composed of carcinoma cells admixed with stromal fibroblasts, lymphatic and vascular channels, and inflammatory cells, often referred to as the tumour microenvironment. This microenvironment is becoming increasingly recognised as having an important role in tumour cell invasion and the ability to metastasise. A few studies in selected cancer subtypes, such as breast, lung, skin and prostate cancer have quantified the cellular components of primary tumours and demonstrated that the tumour composition is associated with patient survival [reviewed in 41]. In CRC, the number of stromal myofibroblasts [42], vimentin expression [43] and degree of stromal desmoplasia [44] have been associated with patient prognosis in the past. More recently, two studies have suggested that the proportion of tumour cells in CRC may be important as a prognostic factor [41,45].
The co-investigators of this study have developed a reproducible method for assessment of the number of tumour cells per unit area of standard haematoxylin and eosin-stained tissue sections prepared according to standard protocols from tumour blocks. This method involves application of a grid with a systematic random sample of 300 points which is then superimposed on the selected area using newly developed virtual graticule software (RandomSpot, University of Leeds, Leeds, UK) to count the number of times the point fell over each of the categories. Large areas of necrosis and mucus at the surface are avoided when selecting the area. The following categories can be studied in the scoring system: tumour (the point falls onto a viable cancer cell), stroma, tumour lumen, necrosis, vessel, inflammation and non-informative (unclassifiable). To assess inter-observer variation, a random sample of 20 cases will be double scored by a second pathologist. This method has been successfully applied to the study of large series of colorectal cancer specimens [41] and is currently being measured in several NCRN clinical trials in patients with colorectal cancer.
Based on preliminary data obtained from the co-investigators of this study, it has been agreed to use TCD as a biomarker of the efficacy of radiosensitisation in the trial proposed here. The Trial Development Group at the back of this protocol and the NCRI Colorectal Cancer Clinical Study Group (Subgroup meeting, Leeds, April 2010) feel that sufficient data exist from the analysis of TCD in several large series of patients with colorectal cancer to justify its application as the primary endpoint for the phase II component of this trial.
1.5 Changes in tumour perfusion
Angiogenesis is an important process in the natural history of tumour evolution and response to therapy [46]. The measurement of tumour blood flow in vivo can provide important information about tumour biology and behaviour. In particular, measurement of tumour blood flow using perfusion computed tomography (pCT) scanning and dynamic contrast-enhanced magnetic resonance imaging (dce-MRI) in colorectal cancer have been shown to correlate with clinicopathological findings and to be prognostic indicators [47,48]. It has been shown previously that chemo-radiotherapy can affect tumour perfusion: De Vries and colleagues [49] demonstrated significant on-treatment increases in tumour perfusion after 1-2 weeks of chemoradiotherapy, and post-therapy studies have reported reduced tumour perfusion on pCT and dce-MRI [50-52]. Since measurement of tumour perfusion characteristics in patients may result in improved understanding of tumour biology and behaviour, there is a need to incorporate pCT and dce-MRI into the pre-operative assessment of patients with rectal cancer before and during protocol therapy. It is not currently known whether pCT or dce-MRI represent the optimal methodology for imaging tumour perfusion in rectal cancer. Though one study has reported some degree of correlation between pCT and dce-MRI perfusion parameters [53], there are variable reported correlations of both modalities with histological markers in rectal cancer [54-57].
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 19 of 45 Version 1.0_12th Jul 2010
2 Objectives and Endpoints
Primary objective
To investigate the activity of Nelfinavir (the study drug) administered before and during short-course radiotherapy (SCRT) in patients with rectal adenocarcinoma. For the purposes of this trial, radiotherapy is defined as a total dose of radiotherapy 25 Gy, which is delivered in 5 Gy fractions on 5 days over a 7-day period. Secondary objectives
• Safety of Nelfinavir when combined with SCRT assessed up to 6 months from last fraction of radiotherapy
• Radiological response of primary tumour at 8 weeks post-SCRT Primary endpoint
• TCD in biopsy taken 7 days from last fraction of protocol radiotherapy. Secondary endpoints
• Incidence of any grade 3 or higher non-haematological or haematological toxicity (according to CTCAE v 4.0) up to 6 months from last fraction of radiotherapy
• RECIST (version 1.1) assessment of primary tumour on MRI at 8 weeks post-SCRT • Proportion of patients proceeding to pelvic surgery within 6 months from last fraction of
radiotherapy
Exploratory studies • Changes in tumour perfusion on dce-MRI and pCT pre- and during radiotherapy with and
without the study drug Safety cohort analysis
• Safety measured by incidence of any grade 3 or higher non-haematological or haematological toxicity (according to CTCAE v 4.0) up to 28 days post-SCRT
3 Study Design
A prospective multi-centre open label phase II randomised trial of Short Course Radio-Therapy (SCRT) with or without the addition of the Investigational Medicinal Product (IMP), Nelfinivir, including an initial safety cohort assessment to assess safety in a single centre before expansion to a further 4 centres.
3.1 Patient numbers and recruitment
It is anticipated that the duration of recruitment into the study will be 24 months, and that the recruitment rate for the study will be an average of 1.5 patients per month. The study will end when the last patient to be recruited has completed 6 months of follow-up from the end of radiation treatment along with any applicable monitoring and analysis of the data.
4 Patient Selection
Potential patients will be identified at Colorectal MDTs with surgical representation, when histology and radiology results are reviewed and discussion outcomes are documented. When patients attend the out-patients department to be told the outcome of the MDT meeting, the details of the trial will be explained. Patients will also receive an information leaflet to read and take home at least 24 hours prior to written informed consent being obtained. The Investigator will determine patient eligibility on the basis of the inclusion and exclusion criteria listed below.
4.1 Inclusion criteria:
1. Histologically proven adenocarcinoma of the rectum (tumour ≤ 15 cm from anal verge)
2. Radiological evidence of M1 disease
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 20 of 45 Version 1.0_12th Jul 2010
3. Treatment intent of SCRT is either down-sizing prior to delayed surgery ≥ 8 weeks) or palliation of symptoms from rectal cancer
4. Colorectal Multidisciplinary Team (MDT) with surgical representation must document that patient is suitable for SCRT as primary treatment. In patients considered for.systemic chemotherapy as standard (non-protocol) therapy prior to surgery, chemotherapy should commence ≥ 14 days from the last fraction of SCRT. Patients should be imaged 8 weeks from the last fraction of radiotherapy and considered for pelvic surgery if sufficiently downsized
5. Serum bilirubin ≤ 3x normal
6. AST or ALT ≤ 3x normal
7. Creatinine clearance >50 ml/min
8. WBC ≥ 3.5/µl; platelets ≥ 100,0/µl; haemoglobin ≥ 10 g/dl
9. Age ≥ 18 years
10. ECOG performance status 0-2
11. Able to give written informed consent
12. Willing and able to comply with the study procedures, including biopsy of the primary tumour 7 days from the last fraction of SCRT
4.2 Exclusion criteria:
1. Operable primary tumour at time of study entry, for which the Colorectal MDT decide that surgery should be the primary treatment
2. Previous pelvic radiotherapy
3. Other experimental treatment ≤ 4 weeks prior to this study (including chemotherapy and immunotherapy)
4. History of other malignancy less than 2 years before the diagnosis of rectal cancer, excluding the following: Non-melanoma skin cancer, in situ carcinoma of the cervix treated surgically with curative intent, other malignant tumours that have been treated surgically and that have a disease-free survival of ≥10 years
5. Recent (< 2 months) severe cardiac disease (e.g. arrhythmia, congestive heart failure, infarction)
6. Active infections (including chronic hepatitis type B or C and HIV infection if status known), severe immunologic defect, compromised bone marrow function
7. Haemophilia A and B, phenylketonuria
8. Known hypersensitivity to Nelfinavir or other HIV protease inhibitor
9. Concurrent use of drugs with a narrow therapeutic window and which are substrates of cytochrome P450 (CYP) 3A (CYP3A4), that cannot be substituted by other drugs and that may not be discontinued during study treatment (e.g. phenobarbital, carbamazepine, phenytoin, terfenadine, astemizole, cisapride, amiodarone, quinidine, pimozide, triazolam, midazolam, ergotamines, rifampicin, herbal preparations that contain Saint John's wort, Hypericum perforatum, omeprazole, simvastatin, lovastatin or atorvastatin, sildenafil or methadone)
10. Pregnant or breastfeeding
11. If a woman of child bearing potential, unable or unwilling to use effective contraception during participation in the trial. Contraceptives that contain norethisterone and ethinylestradiol should be replaced by an alternative contraceptive or contraceptive method
12. Major systemic co-morbidities preventing safe participation in the trial (this will be determined by the local PI)
13. Major psychiatric illness currently or within the past 12 months
14. Any other condition or therapy that may represent a risk for the patient in the judgement of the treating physician or that could interfere with the aim of the study
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 21 of 45 Version 1.0_12th Jul 2010
4.3 Patient screening and enrolment
Screening and study enrolment logs will be maintained by the clinical study team. A patient registration/randomisation check-list will be completed and a trial number will be assigned in conjunction with the Oncology Clinical Trials Office whose details for randomisation are at the beginning of the protocol.
For inclusion of a patient into the study the following criteria must be fulfilled: • Checklist of inclusion and exclusion criteria • Explanation of the aims and of the procedures of the trial to the patient • Obtaining written informed consent from the patient • Registration/randomisation of the patient and subsequent patient numbering
Additional travel expenses due to study participation may be refunded. This is not expected since there are very few extra visits to hospital over and above those for standard treatment.
5. Protocol Treatment
5.1 Investigational medicinal product
The study drug, Nelfinavir, will be administered orally at a dose of 1250 mg twice daily from the morning of Day -7 to the final day of radiotherapy (this corresponds to 5 tablets in the morning, 5 tablets in the evening, each day for 14 days in total). Patients will be advised to swallow the tablets whole and to take them with food or within 30 minutes of the end of a meal. The first dose of the drug should be taken on the morning of Day -7 [i.e. 7 days prior to the day of the first fraction of radiotherapy (Day 1)]. There is no Day 0: The day after Day -1 is Day 1. In other words, the patient should complete 7 days of treatment with Nelfinavir prior to the first day of radiotherapy (Day 1). The dose of Nelfinavir selected for use in this trial (i.e. 1250 mg bd PO) corresponds to one of the two daily dosing schedules laid out in the summary of product characteristics (SPC). The chosen schedule has a higher area under the curve24 h compared to the thrice daily schedule. Day Number -7
Wed -6 Thu
-5 Fri
-4 Sat
-3 Sun
-2 Mon
-1 Tue
1 Wed
2 Thu
3 Fri
4 Sat
5 Sun
6 Mon
7 Tue
Nelfinavir taken twice a day for 14 days
Radiotherapy*
*Starting on a Wednesday and continuing for 5 week days (excluding the weekend).
Figure 2 Schema outlining protocol therapy
5.2 Radiotherapy
It should be noted that radiotherapy will be performed to be consistent with current NHS treatment for all patients in participating centres, summarised below.
5.2.1 Simulation and Immobilization
⎯ Patients will be immobilised and simulated on a flat table-top CT Simulator in a supine or prone position
⎯ Planning CT +/- motion imaging (fluoroscopy or 4D CT) will be performed in the radiotherapy department
⎯ Patients should be advised to drink fluids prior to simulation in order to have a comfortably full bladder during the CT planning scan and intravenous contrast may be administered at the discretion of the treating oncologist. Fasting for 2 hours prior to the CT planning scan is recommended, except clear fluids
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 22 of 45 Version 1.0_12th Jul 2010
⎯ A radio-opaque marker will be placed to demonstrate the position of the anal verge
⎯ CT simulation: 2.5-3.0 mm slices at 2.5-3.0 mm intervals. Patient should be scanned from L3 space to at least 4 cm below the anal marker.
5.2.2 Definition and delineation of the target volumes All volumes are defined on planning CT images. At the discretion of the treating oncologist, image fusion with MRI may be utilised to assist in target and normal tissue delineation. It is the responsibility of the treating oncologist to confirm appropriate image registration for treatment planning purposes. A planning atlas will be provided to participating centres as a step-by-step guide to creating the target volumes and to illustrate examples of target volumes: Gross Tumour Volume (GTV) is the primary tumour and radiologically involved nodes. To avoid complicated volumes and multiple GTVs, the primary tumour and the nodes along with the intervening mesorectal envelope between the primary tumour and the mesorectal nodes should all be considered as a one single GTV. If any part of the tumour or pathological lymphadenopathy extends outside the mesorectum, this should be encompassed within the GTV. The GTV should be delineated using information obtained from per rectal examination and all imaging modalities (particularly MRI) which have been performed. The Clinical Target Volume (CTV) includes elective irradiation of at-risk pelvic subsites and draining lymph nodes. Full details and colour illustrations will be provided in the planning atlas. In brief, the at-risk pelvic subsites to be considered for inclusion in the CTV are: [1] Mesorectum beyond that defined in GTV [2] Pre-sacral space, which includes lateral and median sacral vessels, lymphatics and pre-sacral nerves and inferior hypogastric plexus [3] Lateral subsite - this is the area lateral to the mesorectal fascia, includes lateral pelvic side wall and lymph node chains along pelvic vessels (including internal iliac, obturator nodes) [4] Inferior pelvic subsite (only for tumours involving the levators or the ischiorectal fossa) – perineum, anal sphincter complex, ischiorectal fossa [5] Anterior subsite – includes organs/structures in front of the mesorectum. The Planning Target Volume (PTV) is defined as:
• CTV + 1 cm in all directions
5.2.3 Delineation of Organs at Risk The following structures are considered to be organs at risk [OARs] and will be delineated separately: Right femoral head Left femoral head Small intestine within the radiotherapy fields Bladder
5.3 Treatment Planning and Verification
Radiotherapy will be applied to ensure target localisation and normal tissue avoidance according to local policy. CT based 3D-conformal treatment planning or IMRT will be used for all patients. Generally 3-7 beams will be required to meet the planning criteria. The entire plan will be displayed in physical dose. Dose Volume Histograms (DVHs) shall be calculated for the targets and organs at risk (see below). The treating physician (PI or designate), a planner and a physicist must approve the plan prior to radiotherapy. Verification imaging to localize the treatment volume is required prior to every fraction. The technique of verification imaging will be determined by local policy: A minimum of one pair of orthogonal verification images must be acquired to confirm the position of the isocentre. These images may be kV or MV. If available, cone beam CT is preferred. Repositioning will be recommended for all target offsets greater than 3 mm from planned position.
5.4 Treatment Delivery and Total Dose:
All fields will be treated daily. • Total dose delivered: 25 Gy in 5 fractions in 7 days.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 23 of 45 Version 1.0_12th Jul 2010
If a dose of radiotherapy is not delivered on a treatment day due to technical problems, treatment should be administered on one of the days of the weekend so that the total dose is administered in 7 days as prescribed above. Since the dose of radiotherapy is delivered with radical intent and must be completed in 7 days, patients should receive radiotherapy on bank holidays as for Category 1 patients.
5.5 Dose Volume Constraints:
The aim should be to encompass the PTV within the 95% isodose; the dose constraints are set such that at least 99% of the PTV should receive 95% of the prescription dose. The PTV maximum should be no more than 107% of the prescribed dose to the ICRU reference point; this maximum dose is determined in accordance with ICRU definitions whereby a region of dose is considered clinically meaningful if its minimum diameter exceeds 15 mm. Dose volume constraints region of interest/organ at risk
Dose constraint
PTV V95% > 99.0% DMAX < 107% (to a volume of approximately
2 cm as per ICRU guidelines) Femoral head [left] V20 Gy < 40% Femoral head [right] V20 Gy < 40% Small intestine Document volume (cc) receiving
103%, 105% and 107% of dose Bladder Document volume (cc) receiving
105% and 107% of dose All protocol treatment will be administered on an out-patient basis. After the final day of radiation treatment (with or without Nelfinavir dependent on the randomisation arm of the trial), the patient has an interval without any cancer-specific treatment for 7 days. At this timepoint, a biopsy will be performed (see section 7.3 below). Thereafter, chemotherapy or any other oncological intervention may be administered as indicated by local policy at each participating centre.
5.6 Radiotherapy Quality Assurance
To audit the consistency of radiotherapy delivery in participating centres, a Radiotherapy QA team will be established for this trial, to include a Consultant Clinical Oncologist, a Senior Research Radiographer, a Radiologist and RT-QA Advisor. It will be a requirement for clinicians to complete a detailed Plan Assessment Form for each patient entered into the trial and this will be an integral part of the trials CRF. The Plan Assessment Form will need to be approved by the trials unit before the first dose of radiotherapy is administered to the first patient at each participating centre. This will ensure compliance with the local radiotherapy protocol, and allow identification of major deviations prior to start of radiotherapy.
6 PHARMACEUTICAL AND PHARMACOLOGICAL INFORMATION
6.1 Supply and storage
Nelfinavir (VIRACEPT®) will be sourced and funded locally from hospital own stock. It will be stored and temperature monitored in line with GCP and standard policy at each individual site. Nelfinavir should be stored in its original container below 30°C.
6.2 Drug formulation
Nelfinavir is available as 250 mg film coated tablets. It is available in HDPE plastic bottles containing 300 tablets, fitted with HDPE child resistant closures with polyethylene liners. Other ingredients of the coated tablets are calcium trimetasilicate, crospovidon, magnesium stearate, indigocarmin (E132), hypromellose, triacetin. For further information, please refer to the current version of the SPC for Nelfinavir at the following website: www.medicines.org.uk
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 24 of 45 Version 1.0_12th Jul 2010
6.3 Labelling
All Nelfinavir will be labelled in line with EU GMP Volume 4, Annex 13 requirements and local dispensing requirements. A copy of the label will be sent with the Clinical Trial Application to the MHRA for approval. Labelling will take place in the local pharmacy department.
6.4 Dispensing
At day -7, the patient will be dispensed the full 2 weeks of Nelfinavir supply. Each patient will receive one bottle of Nelfinavir which contains 300 tablets, although they will only need 140 tablets. Each participating centre will provide a trial specific prescription in line with local requirements.
6.5 Drug accountability
Accountability records will be kept by pharmacy to account for the amount of Nelfinavir dispensed and returned per patient, batch and expiry.
6.6 Study Drug Administration and compliance check
Patients should be directed to return all unused drug to pharmacy so that it may be checked for compliance. All unused medication returned will not be reused. Following this, the study drug will be destroyed locally in line with local destruction policies. Patients will receive the amount of Nelfinavir tablets for the entire study (2 weeks supply) upfront and shall return any unused medication. Upon completion of Nelfinavir treatment, the balance of drug handed out and drug returned will be recorded to check compliance.
6.7 Study Drug
Investigators are advised to consult the SPC at the following website: www.medicines.org.uk A copy of the SPC will also be held in the trial master file and site file of each investigator. Nelfinavir (trade name Viracept®, manufacturer Roche) belongs to a class of antiretroviral compounds, the protease inhibitors. Other drugs of this class are amprenavir, atazanavir, indinavir, lopinavir, ritonavir and saquinavir. The mode of action of these substances against HIV is the inhibition of the viral enzyme, HIV-protease. This inhibition results in immature, non-infectious viruses. Nelfinavir is licensed for combination therapy of HIV infection in adults if therapy is indicated. In the SONATINA protocol for this trial, it is being used as an IMP as it is being studied outside its terms of authorisation. After single or repeated oral administration of 500 to 750 mg of Nelfinavir (two to three film tablets containing 250 mg of the compound, each) with meals the maximum concentration of Nelfinavir in the plasma was reached at 2 to 4 hours. The maximum plasma concentration (Cmax) was on average between 3 and 4 µg/ml after repeated dosing of 750 mg at 8 hourly intervals for 28 days (steady-state). The nadir concentration in plasma (i.e prior to administration of the following dose) was between 1 and 3 µg/ml. The absolute bioavailablity of Nelfinavir has not been determined. The pharmacokinetics of Nelfinavir are similar whether administration is twice or thrice daily, except the AUC24 h after twice daily administration of 1250 mg is increased by a factor of 1.27. The Cmax is significantly higher after 1250 mg bd i.e. by a factor of 1.49. The maximum plasma concentrations and the AUC is increased by a factor of 2 to 3 when Nelfinavir was taken with food (as opposed to fasting). The elevated plasma concentrations that were observed with simultaneous intake of food were independent of the fat content of the food. In both animals and man, the volume of distribution (2-7 L/kg) is greater than the total body water. This suggests considerable diffusion of Nelfinavir into extravascular tissues. Nelfinavir has penetration into the brain. Nelfinavir is strongly bound to protein in the serum (98%). In vitro, several cytochrome P450 isoforms including CYP3A, CYP2C19/C9 and CYP2D6 are responsible for the metabolism of Nelfinavir. The clearance of Nelfinavir after single and repeated oral administration was 24-33 L/h and 26-61 L/h, respectively, showing that Nelfinavir is a drug with an intermediate to high hepatic bioavailability. The terminal half time in the plasma was 3.5 to 5 hours. The majority of the radioactivity (87%) after an orally administered dose of 750 mg of 14C-Nelfinavir was excreted in faeces. Unmetabolized Nelfinavir accounted for 22% and a several oxidized metabolites accounted for 78% of the faecal radioactivity. Only 1 to 2% of the radioactivity was detected in urine, and this was mainly in the form of unmetabolized Nelfinavir.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 25 of 45 Version 1.0_12th Jul 2010
6.8 Contraindications
Nelfinavir is metabolized in part by the cytochrome P450 system (CYP3A). Caution is advised when concurrent drugs, that induce CYP3A or potentially toxic drugs that are partially metabolized by CYP3A, are taken. Inhibitors of HMG-CoA-reductase (statins) and Nelfinavir can have a synergistic effect and can increase the risk for myopathy, including rhabdomyolysis, considerably. The concomitant administration of Nelfinavir with simvastatin or lovastatin or atorvastatin is not permitted in this clinical trial. Although the interaction with sildenafil (Viagra) and Nelfinavir has not been investigated, a substantial elevation of the AUC and of the Cmax of sildenafil is expected. During treatment with Nelfinavir, the use of hypericum extracts is not recommended. Nelfinavir should not be taken together with the following compounds: omeprazole, astemizole, cisaprid, midazolam, rifampicin, terfenadine, triazolame.
6.9 Undesirable effects
The tolerability of Nelfinavir was investigated in patients who were given the drug either alone or together with nucleoside analogues. The majority of the side effects were of mild intensity. The most frequently observed side effect of patients who received Nelfinavir at the recommended dosage was diarrhoea. This diarrhoea is usually mild and can be controlled by anti-diarrhoeals. In 20-30% of the patients, the diarrhoea was graded as intermediate or severe. Other potential side effects of Nelfinavir (which must be reported if observed in this clinical trial): Skin and skin appendages: Rash. Gastrointestinal complaints: Flatulence, nausea, abdominal pain. General complaints: Feeling of weakness.
Changes in values of laboratory tests: Low neutrophil count, elevated lymphocytes, elevated ALT/AST. Eyes: In clinical studies, one case of acute iritis and one case of mononuclear loss of vision as a
consequence of optical nerve damage have been reported. New cases of hyperglycaemia, as well as exacerbations of existing diabetes mellitus, were reported in patients who were treated with HIV protease inhibitors (HPI) including Nelfinavir. Hyperglycaemia so severe as to be associated with ketoacidosis occurred in some cases. However, due to co-morbidities, these patients took drugs which were diabetogenic, i.e. no causal link that HIV protease inhibitors are diabetogenic could be proven. Hyperglycaemia is not expected in the short timescale of treatment proposed in this clinical trial.
6.10 Dose reductions
No dose reduction of the Nelfinavir is allowed. If a patient is unable to tolerate Nelfinavir due to side effects, then Nelfinavir will be stopped. Every effort should be made to continue with the planned radiotherapy, as prescribed.
7 CLINICAL AND RADIOLOGICAL EVALUATION
The first 8 patients to be recruited to the SONATINA trial will be analysed for safety and will be termed “Safety cohort.” Once the eighth patient has been followed up for 28 days, an analysis will take place to look at the safety data from the first eight patients recruited to the trial (i.e. before further recruitment can occur). All patients will have assessments as per the summary of the schedule of events above, with follow-up for 6 months from the last fraction of radiotherapy. More information on the safety cohort is documented in section 12.
7.1 Pre-study procedures
a) The following examinations are mandatory within 4 weeks prior to commencement of
Nelfinavir dosing in the study: • Medical history • Physical examination (including examination per rectum), body weight, height, temperature,
blood pressure and pulse (Vital signs) • Assessment of ECOG performance status (see appendix 1) and of the disease-related
symptoms
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 26 of 45 Version 1.0_12th Jul 2010
• Imaging routinely performed for standard NHS treatment of the subject group: CT scan of the thorax, abdomen and pelvis and MRI scan of the pelvis. RECIST (see Appendix 2) measurements of the primary tumour should be performed on MRI scan.
• Perfusion CT of the pelvis and DCE-MRI scan of the pelvis (only at participating centres able to perform these imaging modalities).
• Optional tumour biopsies for research purposes in participants who sign Consent Form B • Haematology: haemoglobin, leukocytes, platelets, differential white cell count. • Biochemistry: electrolytes, Albumin, calcium, magnesium, creatinine, urea, bilirubin, alkaline
phosphatase, ALT, Glucose (non fasting) • CEA, CA125 and CA19.9 (only repeated thereafter if initially elevated above normal range at
the pre treatment sample) • Pregnancy test (for females of reproductive age) • Blood for research assays ( See section 7.5) • Assessment of CTCAE according to version 4.0
7.2 Mandatory procedures while on study
Daily from Wednesday (Day -7) to Tuesday (Day 7) (14 days)
• Nelfinavir dosing (for active arm) no additional drugs for control arm.
Day -1 ( i.e the day before the first dose of RT)
• Perfusion CT of the pelvis and DCE-MRI scan of the pelvis (only at participating centres able to perform these imaging modalities)
• Blood for research assays • CTCAE v4.0
Daily from Wednesday to Tuesday (day 1 to day 7) excluding Saturday and Sunday
• Radiotherapy Treatment On last day of RT (Tuesday): day 7
• Medical history • Physical examination, including body weight, height, temperature, blood pressure and pulse • Assessment of ECOG performance status (see appendix 1) and of the disease related
symptoms • Haematology: haemoglobin, leukocytes, platelets, differential white cell count. • Biochemistry: electrolytes, albumin, calcium, magnesium, creatinine, urea, bilirubin, alkaline
phosphatase, ALT, glucose (non fasting) • Perfusion CT of the pelvis and DCE-MRI scan of the pelvis (only at participating centres able
to perform these imaging modalities) • Blood for research assays • CTCAE v4.0
Seven days after completion of RT: day 14
• Tumour Biopsies • CTCAE v4.0
Eight weeks from last fraction of RT:
• Imaging routinely performed as standard NHS treatment: CT scan of the thorax, abdomen and pelvis and MRI scan of the pelvis. RECIST (see Appendix 2) measurements of the primary tumour should be performed on MRI scan to assess radiological response.
Every 4 weeks up to and including 6 months after last dose of radiotherapy. The assessments carried out at 6 months will be the same as those for patients who withdraw from the study at anytime
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 27 of 45 Version 1.0_12th Jul 2010
• Medical history • Physical examination (including examination per rectum), body height and weight,
temperature, blood pressure and pulse (vital signs) • Assessment of ECOG performance status (see appendix 1) and of the disease related
symptoms • Haematology: haemoglobin, leukocytes, platelets, differential white cell count. • Biochemistry: electrolytes, albumin, calcium, magnesium, creatinine, urea, bilirubin, alkaline
phosphatase, ALT, glucose (non fasting) • CEA, CA125 and CA19.9 (only repeated if initially elevated above normal range for each
investigational site) • CTCAE v4.0
Following completion of protocol therapy, follow-up of the patients is performed at intervals of 4 weeks until 6 months from the last day of radiation therapy. This frequency of follow-up is consistent with local policy for routine follow-up of patients receiving standard radiotherapy. As per local policy, further oncological intervention may be performed at any time ≥14 days after last dose of radiotherapy. Serum tumour markers (CEA, CA125 and CA19.9) are only to be checked on study if that particular tumour marker was elevated in the pre-treatment test. Tumour markers should be checked every 4 weeks from the end of RT until the off-study visit (6 months post-RT). Since measurement of tumour perfusion characteristics in patients may result in improved understanding of tumour biology and behaviour, patients treated in Oxford will be expected to have pCT and dce-MRI as additional pre-study assessments and during protocol therapy. On account of lack of availability of these dynamic imaging modalities at other centres, patients treated in participating centres outside Oxford will not be expected to have these additional tests but they may be offered the tests should they become available at other participating centres. The pCT and dceMRI scans will be combined, where possible, with routine scans. The scans will require 2 additional visits to the Radiology Department, but these will be combined with routine hospital visits, where possible. Both modalities will be performed pre-treatment, on day -1, and on the last day of radiotherapy. For both MRI and CT scans, the patient will lie supine on the scanner table and an intravenous cannula will be placed in the antecubital fossa. As for routine CT scans, the patient will remain nil-by-mouth for 2 hours prior to the procedure and, for the staging scan, oral contrast agent will be administered 30 minutes before scanning. The pCT component of the CT scan, routine MRI and dce-MRI studies do not require oral contrast. Perfusion CT is performed during and after the administration of iodinated contrast material and can be performed during the routine pre-treatment contrast CT study. dceMRI sequences are performed during and after the administration of paramagnetic MR contrast agent, and can be performed immediately after routine MRI. Patients intolerant of either iodinated or gadolinium-based contrast media will not be scanned for the purposes of this exploratory endpoint, but these patients will be included in the analysis of the primary endpoint of the SONATINA trial.
7.3 Tissue donation
Consent Form A: Since the primary endpoint for this trial relates to histology, all patients participating in this study will be asked if they wish to gift tissue samples already obtained as part of their routine NHS care and those that may be removed at surgical operation as part of their routine care to the University of Oxford. These samples may be transferred to an HTA licensed biobank while the study is open to recruitment and up to 24 months from closure of the study to recruitment for possible use in future ethically approved research. All patients who enter the study will already have had pre-treatment biopsies which confirmed the diagnosis of rectal adenocarcinoma. These samples will be used to assess TCD at baseline (pre-treatment). Patients will also be asked to consent to an additional out-patient endoscopy procedure 7 days from the last day of radiotherapy. The purpose of this procedure is to obtain biopsy tissue, to be used purely for research purposes (i.e. to assess the primary endpoint of this trial, which is TCD post-treatment). The risks of this procedure are rare, but include perforation (1 in 10,000), bleeding or infection. As is standard for colonoscopy procedures, 7 biopsies will be taken during the procedure (6 from malignant tissue and one from the normal mucosa). From 6 biopsies, 1 biopsy will be snap frozen in liquid nitrogen using standard procedures, 1 biopsy will be stored in RNAlater and 4 biopsies will be fixed in paraffin by standard local procedures. The biopsy of normal mucosa will be fixed in paraffin by local standard procedures. Diagnostic biopsy needs to be performed within 6 months prior to study entry.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 28 of 45 Version 1.0_12 Jul 2010 REC No: 10/H0604/61
Confidential
th
Consent Form B: All patients will also be asked for voluntary consent for an additional out-patient proctoscopy procedure prior to commencement of the study drug to obtain biopsy tissue to be used purely for research purposes. This additional procedure is not mandatory for inclusion in the trial. The risks of this procedure are rare, but include perforation (1 in 10,000), bleeding or infection. As is standard for colonoscopy procedures, 7 biopsies will be taken during the procedure (6 from malignant tissue and one from the normal mucosa). From 6 biopsies, 1 biopsy will be snap frozen in liquid nitrogen using standard procedures, 1 biopsy will be stored in RNAlater and 4 biopsies will be fixed in paraffin by standard local procedures. The biopsy of normal mucosa will be fixed in paraffin by local standard procedures.
7.4 Surgery and Pathology
The date and type of surgery occurring during the follow-up period must be recorded in the CRF. Surgical complications occurring within 30 days of surgery must be recorded in detail. Pathological response to treatment is evaluated in all patients who undergo resection or biopsy after protocol therapy. The histopathological stage and grade must be recorded (ypTN classification). The surgical notes and the histological status of the resection margins must also be recorded in the CRF (distance to nearest margin) and whether or not R0 resection was achieved.
7.5 Bloods for Research Assays
Blood samples for storage as whole blood (genotype analysis to be determined by ongoing preclinical research) or for isolation of PBMCs and platelets (for phospho-Akt, see below) will be taken as shown in the table below. Blood samples will be collected, labelled and transferred as per the procedure of the Oxford Radcliffe Biobank. The date and time of collection will be recorded on the CRF. Samples will be stored at -70 °C and analysed within the timeframe after collection for which the stability in the samples has been validated and found acceptable. As shown in Figure 1 in section 1.3, to demonstrate the pharmacodynamic efficacy of Nelfinavir treatment, phospho-Akt expression will be analysed by immunoblotting of protein extracted from peripheral blood mononuclear cells (PBMC) or in platelets from the same blood sample. Descriptive statistics will be generated for each time point. These will be compared with values obtained from samples obtained prior to treatment. Assay sample handling and storage will be managed according to written instructions. The following table summarises the arrangements for collection, handling, timings, and analytical laboratories responsible. ASSAY 1 ASSAY 2 ASSAY 3
(7 days post-radiotherapy)
ASSAY 4 (voluntary biopsy pre-treatment)
Purpose of Assay
Genotype analysis
Phospho-Akt expression
Fixation/storage of biopsy tissue
Fixation/storage of biopsy tissue
Assay To be determined by ongoing preclinical research
Western blot To be determined by ongoing preclinical research
To be determined by ongoing preclinical research
Type of sample Whole blood PBMC and platelets Biopsy tissue Biopsy tissue Vials Used 7.5 ml EDTA 10 ml EDTA Standard Standard Total volume per visit
15 ml 20 ml Standard TruCut biopsy
Standard TruCut biopsy
Total volume per patient
15 ml 60 ml Seven biopsies obtained at proctoscopy (note that one biopsy is from non-malignant mucosa)
Seven biopsies obtained at proctoscopy(note that one biopsy is from non-malignant mucosa)
Timepoints Pre-treatment only
pre-treatment, day -1, last day of radiotherapy
Pre-treatment and 7 days post-RT
Pre-treatment
Clinical Handling /Storage/ Transport
To Sample handling/GCLP lab at room
On ice to Sample handling/GCLP lab for immediate PBMC isolation,
Five biopsies formalin fixed using standard procedures, one
Five biopsies formalin fixed using standard procedures, one

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 29 of 45 Version 1.0_12th Jul 2010
temperature for immediate freezing as whole blood.
following isolation freeze PBMCs and platelets immediately
biopsy snap frozen in liquid nitrogen and one biopsy stored in RNAlater
biopsies snap frozen in liquid nitrogen and one biopsy stored in RNAlater
Storage Conditions
-70oC Freezer
– 70°C Freezer Liquid nitrogen for biopsies, vials of cultured cells stored in – 700C Freezer
Liquid nitrogen for biopsies, vials of cultured cells stored in – 700C Freezer
Person responsible for analysis
Chief Investigator of Trial
Chief Investigator of Trial
Professor Quirke, St James Institute, Leeds
Professor Quirke, St James Institute, Leeds
Frequency of analysis
Batch and analyse every 20 patients
Batch and analyse every 8-10 patients
Batch and analyse every 8-10 patients. Examine 3 tissue levels in each biopsy block.
Batch and analyse every 8-10 patients. Examine 3 tissue levels in each biopsy block.
7.6 Custodianship, labelling and confidentiality of clinical samples
The Sponsor has overall responsibility for custodianship of samples. Laboratories are instructed to retain any surplus samples pending instruction from the Chief Investigator on use, storage or destruction. It is possible that new or alternative assays may be of future scientific interest. At the end of the research study any surplus samples may be retained for use in other projects that have received ethical approval. Hence, any surplus study samples may be transferred to a licensed tissue bank where they will be managed in accordance with applicable host institution policies and the Human Tissue Act (HTA) requirements. A patient may withdraw consent at any time. In this event, any samples and data that have already been provided for the research trial will be retained and used in the analysis. No further samples will be taken. All samples sent to analytical laboratories will be labelled with the Trial code, trial patient number, dosing cohort and date taken. Should a lab receive any samples carrying unique patient identifiers the recipient must immediately obliterate this information and re-label. The Investigator site/ Chief Investigator will be informed of their error.
8 ASSESSMENT OF SAFETY
All patients who receive at least one dose of Nelfinavir will be considered evaluable for all safety analyses and these analyses continue for 28 calendar days after the last study drug treatment. This is regardless of whether the event is observed by the Investigator or reported by the patient during the study. Should an Investigator become aware of any drug-related SAEs following this period, these must also be reported within the expedited timelines stated below.
8.1 Adverse Event Definitions
8.1.1 Adverse Event Any untoward medical occurrence in a patient or clinical investigation subject administered a pharmaceutical product and which does not necessarily have a causal relationship with this treatment. An adverse event (AE) can therefore be any unfavourable and unintended sign (including an abnormal laboratory finding), symptom, or disease temporally associated with the use of a medicinal (investigational) product, whether or not related to the medicinal (investigational) product]. For marketed medicinal products, this also includes failure to produce expected benefits (i.e. lack of efficacy), abuse or misuse. An AE includes but is not limited to:
• Significant or unexpected worsening or exacerbation of the condition/indication under study thought by the investigator to indicate lack of the expected treatment efficacy. N.B. disease progression per se is not an AE.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 30 of 45 Version 1.0_12th Jul 2010
• A clinically significant worsening of a chronic or intermittent pre-existing condition including either an increase in frequency and/or intensity of the condition.
• Signs, symptoms, or the clinical sequelae of a suspected overdose of either IMP or a concurrent medication (overdose per se, whether accidental or intentional should not be reported as an AE/SAE).
Other reportable events that must be treated as AEs are as follows: • Any pregnancy occurring in a patient or a patient’s partner occurring within six months of the
last trial IMP administration. These should be reported (even if the patient was withdrawn from the study) in the same timelines as a serious adverse event (SAE).
Examples of an AE does not include a/an: • Medical or surgical procedure (e.g., endoscopy, appendectomy); the condition that leads to
the procedure is an AE.
• Situations where an untoward medical occurrence did not occur (social and/or convenience admission to a hospital).
• Anticipated day-to-day fluctuations of pre-existing disease(s) or condition(s) present or detected at the start of the study that do not worsen.
• The disease/disorder being studied or expected progression, signs, or symptoms of the disease/disorder being studied, unless more severe than expected for the subject’s condition.
8.1.2 Serious Adverse Events (SAEs) To ensure no confusion or misunderstanding of the difference between the terms "serious" and "severe", which are not synonymous, the following note of clarification is provided: The term "severe" is often used to describe the intensity (severity) of a specific event (as in mild, moderate, or severe myocardial infarction); the event itself, however, may be of relatively minor medical significance (such as severe headache). This is not the same as "serious," which is based on patient/event outcome or action criteria usually associated with events that pose a threat to a patient's life or functioning. Seriousness (not severity) serves as a guide for defining regulatory reporting obligations.
A Serious Adverse Event (SAE) is any AE, regardless of dose, causality or expectedness, that:
• Results in death • Is life-threatening* • Requires in-patient hospitalisation or prolongation of existing hospitalisation • Results in persistent or significant disability/incapacity • Is a congenital anomaly/birth defect
• Other important medical event(s)
*The term ‘life-threatening’ in the definition of ‘serious’ refers to an event in which the patient was at risk of death at the time of the event. It does not refer to an event that hypothetically might have caused death if it were more severe.
Other events that may not result in death, are not life threatening, or do not require hospitalisation, may be considered a serious adverse event when, based upon appropriate medical judgment, the event may jeopardise the patient and may require medical or surgical intervention to prevent one of the outcomes listed above.
8.2 SAEs which do not require immediate reporting
These events will be recorded in the CRF: An event which is part of the natural course of the disease under study (i.e., disease progression and /or death due to progressive disease). However, if the progression of the underlying disease is greater than that which would normally be expected, or if the investigator considers that there may be a causal relationship between the IMP or protocol design/procedures and the disease progression, then it must be reported immediately.
Hospitalisation for a pre-existing condition, including elective procedures, which has not worsened
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 31 of 45 Version 1.0_12th Jul 2010
Patients may be hospitalised for the following reasons, which will not be regarded as adverse events:
Patients who are unable to travel daily from their home because of the distance to the treating unit
Patients admitted for supportive care (e.g. pain control).
8.3 Clinical laboratory abnormalities and other abnormal assessments as AEs/SAE’s
Abnormal laboratory findings (e.g., clinical chemistry, haematology, urinalysis) or other abnormal assessments (e.g. ECGs, X-rays and scans) that are judged by the investigator as clinically significant will be recorded as AEs or SAEs if they meet the definitions given above. All Grade 3 & 4 laboratory abnormalities judged by the investigator to be clinically significant will be reported as SAEs. Clinically significant abnormal laboratory findings or other abnormal assessments that are detected during the study or are present at baseline and significantly worsen following the start of the study will be reported as AEs or SAEs. However, clinically significant abnormal laboratory findings or other abnormal assessments that are associated with the disease being studied, unless judged by the investigator as more severe than expected for the patients condition, or that are present or detected at the start of the study and do not worsen, will not be reported as AEs or SAEs. The investigator will exercise his or her medical and scientific judgment in deciding whether an abnormal laboratory finding or other abnormal assessment is clinically significant.
8.4 Toxicity due to Study Drug
If toxicity is experienced and the investigator deems that the adverse event is causally linked to the study drug, Nelfinavir, doses may be omitted at the discretion of the investigator. No dose modification of the study drug is permitted. There is no upper limit to the number of doses of Nelfinavir that can be omitted before the patient is withdrawn from the study, but all doses omitted must be recorded on the CRF. Regardless of the number of doses of Nelfinavir omitted, every effort should be made to continue the administration of daily fractions of radiotherapy. If radiotherapy fractions are delayed or omitted, the Chief Investigator must be consulted immediately since modifications of radiotherapy dosing or fractionation may be indicated to compensate for gaps in radiation treatment. Fourteen days after radiation treatment is completed as per protocol, any additional therapy according to local policy is permitted. Since several cytotoxic regimes are currently used in this setting, with no standardisation across centres, the toxicity of additional therapies will not be evaluated in this study.
8.5 Adverse Drug Reaction (ADR)
All untoward and unintended responses to a medicinal product related to any dose.
The phrase "responses to a medicinal product" means that a causal relationship between a study medication and an AE is at least a reasonable possibility, i.e., the relationship cannot be ruled out.
8.6 Unexpected Adverse Reaction
An adverse reaction, the nature or severity of which is not consistent with the applicable product information (e.g. Investigator’s brochure or summary of product characteristics).
8.7 Suspected Unexpected Serious Adverse Drug Reaction (SUSARs)
A serious adverse drug reaction, the nature or severity of which is not consistent with the applicable product information (e.g. Summary of Product Characteristics (SPC) for Nelfinavir. A copy of the SPC will be filed in the trial master file.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 32 of 45 Version 1.0_12th Jul 2010
When determining the expectedness of an adverse event, consideration should be given to: • the underlying condition of the subject
o co-morbidity o concomitant medications
• patient population • severity and frequency of the occurrence
An unexpected adverse event meets one or more of the following criteria:
• not attributed to the underlying condition of the subject being studied • not attributed to the patient population being studied • not anticipated on the basis of prior experience with the drug under investigation or with
related drugs • not identified in the product information (e.g., Investigator’s Brochure for an unapproved
investigational product or package insert/summary of product characteristics for an approved product)
not defined in the study protocol All SUSARs will be reported by OCTO to the Medicines and Healthcare Products Regulatory Agency (MHRA), the main REC, the (The University of Oxford) within specified time periods. Sites must report SUSARs to OCTO and to their Trust R&D departments. Refer to section 8.11 with regard to reporting timelines.
8.8 Causality of AEs
The Investigator must endeavour to obtain sufficient information to determine the causality of the adverse event (i.e. study drug, other illness, progressive malignancy etc) and must provide his/her opinion of the causal relationship between each AE and study drug. This may require instituting supplementary investigations of significant AEs based on their clinical judgment of the likely causative factors and/or include seeking a further opinion form a specialist in the field of the AE. Expected AEs are AEs that have been assessed as expected events for the IMP, based upon previous experience in man. The list of expected AEs for the IMP in this trial can be found in the SPC for Nelfinavir.
8.9 Adverse Event Reporting
All adverse events should be noted in the CRF.
Serious Adverse Events (SAEs) Reporting of Adverse Events All concomitant medications and any therapy used to treat the event must be recorded. The CRF will be reconciled with the SAE log and copy SAE forms / correspondence by the monitor, during or at the end of the trial. SAEs must be recorded in the patient CRF and reported within one working day of becoming aware of the event to the Oncology Clinical Trials Office. As a minimum the following vital elements must be listed on the OCTO SAE form in order for OCTO to send the SAE out to pre determined clinicians for clinical review. Vital elements:
• Identifiable patient • Identifiable drug • Identifiable event • Identifiable reporter • Causality • Expectedness
Each separate episode of an SAE must be recorded on a separate OCTO SAE Report Form. For example, if an SAE resolves completely or resolves to baseline and then worsens again, this must be
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 33 of 45 Version 1.0_12th Jul 2010
recorded as a separate SAE. The NCI CTCAE Version 4.0 must be used to grade each SAE, and the worst grade recorded. All Serious AEs should be documented on the approved trial Serious Adverse Event Report Form (SAE Report Form), using the completion guidelines provided. These should be faxed within one working day of site staff becoming aware of event to the SONATINA Clinical Trial Coordinator at OCTO. Fax: +44 0800 389 1629 All SAEs arising from the SONATINA clinical trial will be reviewed by the predetermined clinicians on the SONATINA trial . SAEs will be e-mailed by the SONATINA trial team to the attention of the clinicians and a response will be needed within 3 working days. Any SUSARS will be identified by the SONATINA trial team before sending out to the clinicians and the clinicians asked to confirm whether or not it is a SUSAR within the same timeframe. All SUSARS will be reported by the SONATINA trial team in OCTO to the competent authority (MHRA) and the main ethics committee and any other applicable institutions will be informed. The investigator team should also refer to the information given in the Investigator Site File and local trust procedures for details on the Trust Policy on incident reporting in research.
8.10 Follow-up of adverse events
Follow up will continue until all the necessary safety data for the event has been gathered and until the AE has either resolved or stabilised. SAEs should be reported until 28 days after the last study drug administration. If new or amended information on a previously reported SAE becomes available, the Investigator should report this to the Sponsor on a new SAE Report Form using the completion guidelines. In addition, the Sponsor may make requests for further information to the study site at regular intervals. Requested follow-up information should be reported to in a timely manner and as soon as possible after receipt of the follow up request. For follow-up information on fatal or life-threatening cases of SUSARs, see below (‘Expedited Safety Reporting’).
8.11 Expedited Safety Reporting
The Sponsor is responsible for the identification and expedited reporting of SUSARs to the Medicines and Healthcare products Regulations Agency (MHRA) and the Main Research Ethics Committee (REC) as required under the applicable UK GCP legislation. For this study, this task has been delegated back to the Chief Investigator by the Sponsor. For the purposes of this study the Oncology Clinical Trials office will carry out this activity. Fatal or life-threatening SUSARs must be reported to the MHRA and the Main REC within 7 calendar days of OCTO receiving the report. Follow up information for fatal or life-threatening SUSARs must be reported to the MHRA and REC within 8 calendar days of submitting the initial report. All other SUSARs are reportable within 15 calendar days of receipt.
8.12 Safety updates
The Chief Investigator is responsible for ensuring that emerging new safety data is assessed and communicated to the Sponsor, responsible oversight bodies and participating centres as appropriate. Local Investigators will review safety updates and ensure that the information is acted on and retained as instructed in accordance ICH-GCP practice and any local requirements.
8.13 Annual Safety and Annual Progress Reports (ASR and APR)
The Chief Investigator is responsible for submitting Annual Safety Reports to the MHRA, REC, Sponsor and the R&D department of each participating Trust. The ASR and the APR will be submitted to the applicable bodies by OCTO on behalf of the Chief Investigator.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 34 of 45 Version 1.0_12th Jul 2010
9 Early Patient Withdrawal
If the patient is withdrawn from the trial, for any of the reasons indicated below and declines attendance for a final off-study visit, a withdrawal assessment should be performed on the day the decision is made to take the patient off-study if feasible or as soon as possible. All the results of the evaluations and observations, together with a description of the reasons for study withdrawal, must be recorded in the medical records and CRF. Patients who are removed from the study due to AEs (clinical or laboratory) will be treated and followed up according to accepted medical practice. All pertinent information concerning the outcome of such treatment must be recorded in the CRF. The following are justifiable reasons for the Investigator to withdraw a patient from study:
• Unacceptable toxicity. • Adverse event requiring discontinuation of treatment. • Unforeseen events: any event that in the judgement of the Investigator makes further
treatment inadvisable. • Serious violation of the study protocol (including persistent patient attendance failure and
persistent non-compliance). • Any situation signifying that continuation of the treatment would be detrimental for the patient
as judged by the investigator (e.g. distant metastasis during treatment)
10 Defining the end of trial
The ‘end of trial’ is defined as the last follow-up visit of the last patient on the trial. This will be the 80th patient. The last follow-up visit per patient is planned to take place 6 months from the end of radiation therapy as per protocol. The responsibility to inform the MHRA and the Main REC within 90 calendar days of the ‘end of the trial’ that the study has closed, has been delegated to the Chief Investigator and will work with OCTO for submission of the appropriate documents. Apart from the planned safety assessment after 8 patients, in cases of early termination of the trial (e.g. due to toxicity or valid new findings) or a temporary halt to the study, the UK Chief Investigator will notify the MHRA and the Main REC within 15 calendar days of the decision and a written explanation for the termination/halt will be given. The entire trial will be stopped when:
• The stated number of patients to be recruited is reached and follow-up completed. • If the interim analysis of the first 8 patients shows that there are safety issues as defined in
the statistical section below. These patients will complete follow up. Regardless of the reason for termination, all data available for the patients at the time of discontinuation of follow-up must be recorded in the CRF. All reasons for discontinuation of treatment must be documented. In terminating the study, the Sponsor and the Chief Investigator will consider the protection of the patients’ interests.
11 DATA ANALYSIS
11.1 Statistical considerations
Primary endpoint • TCD in biopsy taken 7 days from last fraction of protocol radiotherapy.
Secondary endpoints
• Incidence of any grade 3 or higher non-haematological or haematological toxicity (according to CTCAE v 4.0) up to 6 months from last fraction of radiotherapy
• RECIST (version 1.1) assessment of primary tumour on MRI at 8 weeks post-SCRT
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 35 of 45 Version 1.0_12th Jul 2010
• Proportion of patients proceeding to pelvic surgery within 6 months from last fraction of radiotherapy
Variables will be analysed to determine whether the criteria for the study conduct are met. This will include a description of patients who did not meet all the eligibility criteria, an assessment of protocol violations, study drug accountability and other data that impact on the general conduct of the study. Baseline characteristics will be summarised for all enrolled patients and separately for the two treatment arms. Patients who died or withdraw before treatment starts or do not complete the required safety observations will be described and evaluated separately. Treatment administration will be described for all protocol therapy. Dose administration, dose modifications or delays and the duration of therapy will be described. TCD will be summarised at 7 days post-SCRT and also the reduction from baseline TCD will be presented. This may be represented graphically. As TCD has not been fully validated as a surrogate for clinical response, association of TCD with response will be investigated. Toxicities will be summarised up to 28 days post-SCRT and up to 6 months post-SCRT overall and separately by treatment arm Note: no comparison of the two treatment arms is planned. Details from the control arm will provide information to enable the follow-on Phase III trial to be designed if this trial is successfully completed. Systematic data for TCD rates following long-course chemo-radiation or short-course radiotherapy followed by systemic chemotherapy have not been published for this patient population. The reference arm of the trial (no study drug) is therefore necessary to provide reassurance that the TCD rate is acceptable as a primary endpoint compared to historical data from other patient groups. The reference arm will also ensure that TCD measured in the subject group of this trial is consistent with data to be obtained from other contemporary trials currently ongoing in which investigators are measuring TCD in patients with rectal cancer. Sample size has been calculated using Fleming’s one-stage single arm phase II trial method. With 80% power, alpha=5%, TCD expected from control arm=30% (reduced from 50% at baseline), TCD expected from active arm=15% (reduced from 50% at baseline) and allowing for 10% drop-out (see below) requires 60 patients in the active arm. With a randomisation allocation of 3:1, 20 patients are required in the control arm. Therefore a total of 80 patients will be randomised to the trial overall. Recruitment rate should average 1-2 patients per month per site in order to accrue to the projected accrual target within 24 months. Biopsies from about 10% of the patients will not be interpretable (due to necrosis, excessive mucin or other technical problems). The total sample size has therefore been increased by 10% to account for this dropout rate.
11.2 Safety Cohort There will be an interim analysis of the safety cohort of the trial, which consists of the first 8 patients (all of whom will receive Nelfinavir) and followed up for 28 days after completion of protocol therapy. Recruitment will be interrupted while the safety analysis of this cohort takes place. This safety interim analysis will be reviewed by an internal safety monitoring committee including an oncologist independent from the clinical trial, statistician and a member of the trials office. The number of toxicities of grade 3 & 4, during treatment and for 28 days after completion of protocol therapy (post-SCRT), will be summarised and listed in detail. Incidence rates of grade 3/4 toxicities and grade 4 toxicities will be compared with the historical rates associated with short course radiotherapy in this patient group (see below).
• If toxicity rates for the first 8 patients on active treatment are ≤ historical rates (≤ 1 subject with grade 4 toxicity and ≤ 3 subjects with grade 3/4 toxicity), then the safety cohort is complete and further patients will be recruited to the trial as per protocol.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 36 of 45 Version 1.0_12th Jul 2010
• If toxicity rates for the first 8 patients on active treatment exceed historical rates (>1 subject with grade 4 toxicity and/or > 3 subjects with grade 3/4 toxicity over and above those expected from SCRT treatment), then the study will be stopped on safety grounds.
11.3 Measures to be taken in the case of missing, unused and false data
Missing data will be chased up and supplemented where possible after consultation with the investigator. The control of the correctness of the data is performed with ranking tests, validity tests and consistency checks. Unused data will be kept for at least 10 years while respecting the data protection guidelines. The originals of the total of the central study documents will be kept at the investigating centre for at least 15 years after the final report has been generated. Measures for the report of deviations from the original statistical plan. Any necessary changes of the protocol can only be performed with the consent of the Chief Investigators. Proposals for any changes must be submitted in written form to the ethics committee. A statistical analysis plan will be finalised prior to the final datalock and any deviations from this original statistical plan will be described in the final report and will be justified.
11.4 Choice of the patients who are included in the analysis
All patients who have completed at least day 1 of protocol therapy shall be included in the Intention to treat (ITT) analysis.
12 TRIAL ADMINISTRATION
12.1 Regulatory and ethical considerations
The Sponsor and UK Chief Investigator will ensure that this protocol will be conducted in compliance with the Medicines for Human Use (Clinical Trials) Regulations 2004 and amendments thereafter, the guidelines for Good Clinical Practice and the applicable policies of the Sponsor, the University of Oxford. Together, these regulations implement the ethical principles of the Declaration of Helsinki (2008) and the regulatory requirements for clinical trials of an investigational medicinal product as set out in the European Union (EU) Directives 2001/20/EC (Clinical Trials) and 2005/28/EC (GCP).
12.2 Regulatory authority approval
This study will be conducted under a UK Medicines and Healthcare Products Regulatory Agency (MHRA) Clinical Trials Authorisation (CTA). MHRA approval to conduct the study will be obtained prior to initiating the study.
12.3 Ethical conduct of the trial and ethics approval
The Investigator will ensure that the protocol, Patient Information Sheet, Consent Form, GP Letter and any other information that will be presented to potential trial patients (e.g. advertisements or information that supports or supplements the informed consent) are reviewed and approved by an appropriately constituted, independent Research Ethics Committee (REC). The Investigator is responsible for applying for local Trust management approval to conduct the trial in accordance with local arrangements and policies. Trust approval and indemnity must be confirmed in writing before patient recruitment commences at an Investigator site. The University of Oxford will provide written confirmation of Sponsorship in the UK. A separate study delegation agreement, setting out the responsibilities of the Chief Investigator and Sponsor is available for inspection within the study essential documentation. Protocol amendments Amendments to the protocol or other documentation that has been approved by the REC and/or regulatory authority may only be made with the written approval (in email format is sufficient) of the Chief Investigator and the Sponsor. Each protocol amendment will be submitted to the appropriate REC for information and approval. Depending on the type of protocol amendment, the MHRA approval may also be required. The Investigator will submit full details of the amendment to the host (NHS) Trust for
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 37 of 45 Version 1.0_12th Jul 2010
confirmation of continued local management approval and indemnity in accordance with local requirements. Written documentation of the Ethics Committee ‘favourable opinion’ (and if appropriate the MHRA and Trust approval) must be received before the amendment can be implemented. The only exceptions are for changes necessary to eliminate an immediate hazard to study patients, or when the change(s) involves only minor logistical or administrative aspects of the study (e.g., change in monitor(s), change of telephone number(s). It is the Chief Investigator’s responsibility to update patients (or their authorised representatives, if applicable) whenever new information (in nature or severity) becomes available that might affect the patient’s willingness to continue in the trial. The Chief Investigator must ensure this is documented in the patient’s medical notes and the patient is re-consented. Informed consent It is the responsibility of the investigator, or a person designated by the investigator, to obtain written informed consent from each individual participating in this study after adequate explanation of the aims, methods, objectives, anticipated benefits and potential hazards of the study. A written patient information sheet will be given to the participant to read and take home. The content and process of obtaining informed consent will be in accordance with the applicable regulatory requirements and good practice guidelines.
12.4 Trial monitoring
The trial will be monitored according to a prospectively agreed monitoring plan and using standard operating procedures in order to verify that (ICH GCP section 5.18):
1. The rights and wellbeing of the human subjects are protected 2. The reported trial data are accurate, complete and verifiable from source documents 3. The conduct of the trial is in compliance with the approved protocol, with GCP and with
applicable regulatory requirements Additional monitoring to oversee the progress of the trial and accordance with the relevant regulatory requirement includes: Prior to commencement of enrolment, a site initiation meeting will take place to review the protocol and data collection procedures with key site staff. In addition, the monitor will contact the site to confirm that the necessary organisational preparations have been completed and that the personnel, technical and clinical facilities assigned to the trial are adequate. Following completion of the last patient’s last visit a final monitoring contact will be arranged to close down the clinical study site. Unless agreed in writing, all data collected on the CRF must be verifiable against the source data. The Investigator and members of the study team shall ensure that all relevant data is recorded in the medical records. Entries in the CRF will be compared with patients’ medical records and the results will be documented on the Source Data Verification (SDV) Form and the monitoring report. Frequency and extent of monitoring will be detailed in the monitoring plan. The investigator agrees to allow the monitor direct access to all relevant documents and to allocate his/her time and the time of his/her staff to the monitor to discuss findings and any relevant issues.
12.5 Quality assurance
The Sponsor or host NHS organisations may audit the conduct of the study. Regulatory agencies may also conduct a regulatory inspection of this study. Such audits/inspections can occur at any time during or after completion of the study. If an audit or inspection occurs, the investigator and institution agree to allow the auditor/inspector direct access to all relevant documents and to allocate his/her time and the time of his/her staff to the auditor/inspector to discuss findings and any relevant issues.
12.6 Case record retention
Investigators must maintain adequate and accurate records to enable the conduct of a clinical trial and the quality of the research data to be evaluated and verified. These essential documents (as detailed in Section 8 of the ICH GCP Guidelines), include source documents such as scans, study related
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 38 of 45 Version 1.0_12th Jul 2010
documents and copies of the CRFs, Data Clarification Forms and SAE forms. These files need to be archived for at least 10 years after the conclusion of the trial. All essential documents required to be held by the Investigator must be stored in such a way that ensures that they are readily available, upon request, to the Regulatory Agency or Sponsor, for the minimum period required by national legislation. The medical files of trial subjects shall be retained in accordance with national legislation and in accordance with the maximum period of time permitted by the host institutions.
12.7 Patient confidentiality
The investigator will ensure that the patient’s anonymity is maintained. Details will remain confidential and patients’ names will not be recorded outside of the study site. On the case report listings or other documents that may be submitted to external bodies (such as safety committees), patients will be identified only by their initials and a study number. Documents that are not for external submission will be kept in strict confidence by the investigator.
12.8 Completion of the Case Report Form (CRF)
Each site participating in the trial will be responsible for data entry. Patient data will be entered, on a regular basis, direct from source documents into the trial database via an electronic Case Report Form (eCRF). An eCRF will be completed for each patient enrolled into the trial. If a patient is withdrawn early, the reason will be noted on the eCRF. If a patient is withdrawn from the study because of a treatment-limiting AE, thorough efforts should be made to document the outcome. The eCRF will not contain any source data. All appropriate laboratory data, summary reports and Investigator observations will be transcribed by the study site staff into the eCRF from the relevant medical record(s). OCTO staff will raise data queries with the principal investigator or co-investigators at appropriate, periodic intervals in accordance with OCTO procedures. Queries concerning the source data or medical interpretation will be resolved and documented by authorised members of the clinical study team. Corrections, whether to the source data or to data query listing for entry into the eCRF, must only be made by striking out any errors, with a single stroke, and not by using correction fluid. The incorrect figure must remain visible and the correction should be initialled and dated by the person authorised by the Investigator to make the correction. A reason for the change or correction should be given as appropriate. This cycle will be repeated as necessary until the patient data are declared clean. The Principal Investigator (or deputy) is responsible for ensuring the accuracy and completeness of the key trial data for analysis and will wet- sign a printout of the eCRFs to confirm this prior to data lock and analysis. The Investigator approved listings will be archived with the trial master file. It is understood that the source data verification of the eCRF data by the trial monitor is a separate, quality assurance activity that also requires direct inspection of source documents. The Investigators must retain all original reports, traces and films for future reference.
12.9 Clinical study report
All clinical data will be presented at the end of the study on final data listings. The Chief Investigator and statistician will prepare a clinical study report based on the final data listings. The report will be submitted to the Investigator(s) for review and signature to confirm that it accurately represents the data collected during the course of the study. At this point the trial data will be locked for analysis and publication. A summary of the final clinical report will be provided by the OCTO to the MHRA and to the Research Ethics Committee.
12.10 Funding and Indemnity Arrangements
This study is funded by the NIHR Oxford Biomedical Research Centre (BRC) and the Experimental Cancer Medicine Centre Network (ECMC). Any additional NHS clinical service support costs of patient care while on-study should be met by the host medical institution. Indemnity
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 39 of 45 Version 1.0_12th Jul 2010
Arrangements for NEGLIGENT harm. Indemnity and/or compensation for negligent harm arising specifically from accidental injury for which the University is legally liable as the Research Sponsor will be covered by the University of Oxford. The NHS will owe a duty of care to those undergoing clinical treatment, with Trust Indemnity available through the NHS Litigation Authority Scheme. Arrangements for NON-NEGLIGENT harm Indemnity and/or compensation for harm arising specifically from an accidental injury and occurring as a consequence of the research subjects’ participation in the trial for which the University is the research Sponsor may be covered by the University of Oxford.
12.11 Publication Policy and Acknowledgements
The Investigators will retain ownership of all data arising from this trial. The intention is to publish this research in a specialist peer reviewed scientific journal on completion of the study. The results may also be presented at scientific meetings and/or used for a thesis. The Investigators will be involved in reviewing drafts of the manuscripts, abstracts, press releases and any other publications arising from the trial and investigators will retain final editorial control. Study publications and presentations should acknowledge:
• protocol development by the Rectal Subgroup of the NCRI Colorectal Clinical Study Group • funding and additional support from the NIHR Oxford BRC and the ECMC • Sponsorship by the University of Oxford • advice on protocol development from the NCRI CTRad Working Group • Oxford Clinical Trials Research Unit (OCTRU) • support from other funding bodies as appropriate.
The current rectal cancer portfolio for NCRI trials comprises early tumours (TREC clinical trial), resectable patients with M0 disease (COPERNICUS and BACCHUS trials) and M0 disease with margins at risk (ARISTOTLE). SONATINA is the only clinical trial being developed by the NCRI Rectal Subgroup for patients with M1 disease who require downsizing of the primary tumour.
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 40 of 45 Version 1.0_12th Jul 2010
SONATINA Trial Development Group
This protocol was developed by the Rectal Subgroup of the NCRI Colorectal Clinical Study Group. The Chief Investigator acknowledges the individuals who have contributed to the development of this Protocol. The membership of the Trial Development Group is as follows:
Chief Investigator: Ricky Sharma (1,2)
Radiation Oncology/Radiobiology:
Thomas Brunner (1), Gillies McKenna (1), Kate Vallis (1)
Radiation Quality Assurance Cynthia Eccles (1,2), Martin Scott-Brown (1), Helen Winter (1,2), Somnath Mukherjee (1,2)
Surgery: Neil Mortensen (2), Chris Cunningham (2), Shazad Ashraf (2)
Medical and Clinical Oncology:
Esme Hill (1), Richard Adams (7), Rachel Midgley (4), Claire Blesing (2), Andrew Weaver (2), Clare Jacobs (2), David Sebag-Montefiore (8)
Pathology: Bryan Warren (2), Nick West (8), Phil Quirke (8)
Radiology: Mark Anderson (2), Fergus Gleeson (2), Jamie Franklin (2)
Medical Statistics: Susan Dutton (3)
Pharmacy Adviser: Katherine Jacob (2)
Protocol Quality Assurance: OCTO (5) and CTRG (6)
1 Gray Institute for Radiation Oncology and Biology, University of Oxford 2 Oxford Radcliffe Hospitals NHS Trust 3 Centre for Statistics in Medicine, Oxford 4 Dept Medical Oncology, University of Oxford 5 Oncology Clinical Trials Office (OCTO), University Oxford 6 Clinical Trials and Research Governance team, University of Oxford 7 Velindre Cancer Centre, Cardiff 8 St James’ Institute, Leeds
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 41 of 45 Version 1.0_12th Jul 2010
13 REFERENCES
1. Kapiteijn E, Corrie MD, Marijnen AM. Pre-operative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med, Vol. 345: No. 9, (2001).
2. Sebag-Montefiore D, Stephens RJ, Steele R. Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer. (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. Lancet, 373(9666): 811–820, (2009).
3. Vironen, J., et al. Tumour regression grading in the evaluation of tumour response after different preoperative radiotherapy treatments for rectal carcinoma. Int J Colorectal Dis, 20(5): p. 440-5, (2005).
4. Theodoropoulos, G., et al. T-level downstaging and complete pathologic response after preoperative chemoradiation for advanced rectal cancer result in decreased recurrence and improved disease-free survival. Dis Colon Rectum, 45(7): p. 895-903, (2002).
5. Bouzourene, H., et al. Importance of tumor regression assessment in predicting the outcome in patients with locally advanced rectal carcinoma who are treated with preoperative radiotherapy. Cancer, 94(4): p. 1121-30, (2002).
6. Hoskin P, Glynne-Jones R. Neoadjuvant cisplatin chemotherapy before chemoradiation: A flawed paradigm? J Clin Oncol, 25(33): 5281-5286, (2007).
7. Glimelius B, Isacsson U. Pre-operative radiotherapy for rectal cancer. Is 5 x 5 Gy a good or a bad schedule? Acta Oncologica, 40[8]: 958–967, (2001). 8. Radu C, Berglund A, Pahlman L, Glimelius B. Short-course preoperative radiotherapy with delayed surgery in rectal cancer – a retrospective study. Radiother Oncol 87: 343-349, 2008). 9. Hatfield P, Hingorani M, Radhakrishna G, et al. Short-course radiotherapy, with elective delay prior to surgery, in patients with unresectable rectal cancer who have poor performance status or significant co-morbidity. Radiother Oncol, 92(2): 210-214, (2009). 10. Pettersson, D., et al., Interim analysis of the Stockholm III trial preoperative radiotherapy regimens for rectal cancer. British J of Surgery, 97: p 580-587, (2010). 11. Braendengen M, Tveit KM, Berglund A, Birkemeyer E, Frykholm G, Påhlman L, Wiig JN, Byström P, Bujko K, Glimelius B. A randomised Phase III comparing preoperative radiotherapy with chemoradiotherapy in non-resectable rectal cancer. J Clin Oncol, Aug 1;26(22): 3687-94, (2008). 12. Schrag D. Weiser MR, Goodman KA et al. Neoadjuvant FOLFOX-bev, without radiation, for locally advanced rectal cancer. Proc Gastrointestinal Cancer Symposium, Abstr 434, (2010). 13. van Dijk TH, Hospers G, BeukemaJ. Short-course radiation therapy, neoadjuvant bevacizumab,
capecitabine, and oxaliplatin, and radical resection of primary tumor and metastases in primary stage IV rectal cancer: A phase II multicenter study of the Dutch Colorectal Cancer Group. Proc Gastrointestinal Cancer Symposium Abstr 427, (2010).
14. Sebag-Montefiore D et al. J Clin Oncol, in press. 15. Marijnen CA, Kapiteijn E, van de Velde CJ et al. Acute side effects and complications after short-term preoperative radiotherapy combined with total mesorectal excision in primary rectal cancer: report of a multicenter randomized trial. J Clin Oncol, 20: pp. 817–825, (2002). 16. Birgisson H, Pahlman L, Gunnarsson U and Glimelius B, Occurrence of second cancers in patients treated with radiotherapy for rectal cancer. J Clin Oncol, 23: pp. 6126–6131, (2005). 17. Bujko K, Nowacki MP, Nasierowska-Guttmejer A, Michalski W, Bebenek M, Kryj M. Long-term results of a randomized trial comparing preoperative short-course radiotherapy with preoperative conventionally fractionated chemoradiation for rectal cancer, Oct;93(10):1215-23, (2006). 18. Bujko K, Kolodziejczyk M. The 5 x 5 Gy with delayed surgery in non-resectable rectal cancer: a new treatment option. Radiother Oncol, Jun;87(3):311-3, (2008). Epub 2008 Jan 18. 19. Bonner, J.A., et al. Epidermal growth factor receptor as a therapeutic target in head and neck
cancer. Semin Radiat Oncol, 12(3 Suppl 2): p. 11-20, (2002). 20. McKenna, W.G., et al. Synergistic effect of the v-myc oncogene with H-ras on radioresistance.
Cancer Res, 50(1): p. 97-102, (1990). 21. Rosser, C.J., et al. Adenoviral-mediated PTEN transgene expression sensitizes Bcl-2-
expressing prostate cancer cells to radiation. Cancer Gene Ther, 11(4): p. 273-9, (2004). 22. Grana, T.M., et al. Ras mediates radioresistance through both phosphatidylinositol 3-kinase-
dependent and Raf-dependent but mitogen-activated protein kinase/extracellular signal-regulated kinase kinase-independent signaling pathways. Cancer Res, 2002, 62(14): p. 4142-50, (2002).
23. Gupta, A.K., et al. The Ras radiation resistance pathway. Cancer Res, 61(10): p. 4278-82, (2001).
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 42 of 45 Version 1.0_12th Jul 2010
24. Gupta, A.K., et al. Local recurrence in head and neck cancer: relationship to radiation resistance and signal transduction. Clin Cancer Res, 8(3): p. 885-92, (2002).
25. Kim, I.A., et al. The influence of Ras pathway signaling on tumor radiosensitivity. Cancer Metastasis Rev, 23(3-4): p. 227-36, (2004).
26. Gupta, A.K., et al. HIV protease inhibitors block Akt signaling and radiosensitize tumor cells both in vitro and in vivo. Cancer Res, 65(18): p. 8256-65, (2005).
27. Deeks, S.G., et al. HIV-1 protease inhibitors. A review for clinicians. Jama, 277(2): p. 145-53, (1997).
28. Carr, A., et al. Diagnosis, prediction, and natural course of HIV-1 protease-inhibitor-associated lipodystrophy, hyperlipidaemia, and diabetes mellitus: a cohort study. Lancet, 353(9170): p. 2093-9, (1999).
29. Powderly, W.G. Long-term exposure to lifelong therapies. J Acquir Immune Defic Syndr, 29 Suppl 1: p. S28-40, (2002).
30. Bae, S.S., et al. Isoform-specific regulation of insulin-dependent glucose uptake by Akt/protein kinase. B. J Biol Chem, 278(49): p. 49530-6, (2003).
31. Cross, D.A., et al. Insulin activates protein kinase B, inhibits glycogen synthase kinase-3 and activates glycogen synthase by rapamycin-insensitive pathways in skeletal muscle and adipose tissue. FEBS Lett, 406(1-2): p. 211-5, (1997).
32. Pajonk, F., et al. The human immunodeficiency virus (HIV)-1 protease inhibitor saquinavir inhibits proteasome function and causes apoptosis and radiosensitization in non-HIV-associated human cancer cells. Cancer Res, 62(18): p. 5230-5, (2002).
33. Monini, P., et al. Antitumour effects of antiretroviral therapy. Nat Rev Cancer, 4(11): p. 861-75, (2004).
34. Cuneo, K.C., et al. HIV protease inhibitors enhance the efficacy of irradiation. Cancer Res, 67(10): p. 4886-93, (2007).
35. Gills, J.J., et al. Nelfinavir, A lead HIV protease inhibitor, is a broad-spectrum, anticancer agent that induces endoplasmic reticulum stress, autophagy, and apoptosis in vitro and in vivo. Clin Cancer Res, 13(17): p. 5183-94, (2007).
36. Bode H et al. The HIV protease inhibitors saquinavir, ritonavir, and Nelfinavir induce apoptosis and decrease barrier function in human intestinal epithelial cells. Antivir Ther, 10(5):645-55, (2005).
37. Saag, M.S., et al. Randomized, double-blind comparison of two Nelfinavir doses plus nucleosides in HIV-infected patients (Agouron study 511). Aids, 15(15): p. 1971-8, (2001).
38. Grover, S.A., et al. Impact of dyslipidemia associated with Highly Active Antiretroviral Therapy (HAART) on cardiovascular risk and life expectancy. Am J Cardiol, 95(5): p. 586-91, (2005).
39. Oehler-Janne, C., et al., Local tumor control and toxicity in HIV-associated anal carcinoma treated with radiotherapy in the era of antiretroviral therapy. Radiat Oncol, 1: p. 29, (2006).
40. Brunner TB, et al. Phase I trial of the human immunodeficiency virus protease inhibitor Nelfinavir and chemoradiation for locally advanced pancreatic cancer. J Clin Oncol, 26(16): 2699-2706, (2008).
41. West NP, Dattani M, McShane P, Hutchins G, Grabsch J, Mueller W, Treanor D, Quirke P, Grabsch H. The proportion of tumour cells is an independent predictor for survival in colorectal cancer patients. Brit J Cancer, in press.
42. Tsujino T, Seshimo I, Yamamoto H, Ngan CY, Ezumi K, Takemasa I, Ikeda M, Sekimoto M, Matsuura N, Monden M. Stromal myofibroblasts predict disease recurrence for colorectal cancer. Clin Cancer Res, 13: 2082–2090, (2007).
43. Ngan CY, Yamamoto H, Seshimo I, Tsujino T, Man-i M, Ikeda J-I, Konishi K, Takemasa I, Ikeda M, Sekimoto M, Matsuura N, Monden M. Quantitative evaluation of vimentin expression in tumour stroma of colorectal cancer. Br J Cancer, 96: 986–992, (2007).
44. Sis B, Sarioglu S, Sokmen S, Sakar M, Kupelioglu A, Fuzun M. Desmoplasia measured by computer assisted image analysis: an independent prognostic marker in colorectal cancer. J Clin Pathol, 58: 32–38, (2005).
45. Mesker WE, Junggeburt JMC, Szuhai K, de Heer P, Morreau H, Tanke HJ, Tollenaar RAEM. The carcinoma–stromal ratio of colon carcinoma is an independent factor for survival compared to lymph node status and tumour stage. Cell Oncol, 29: 387–398, (2007).
46. Sharma RA, Harris AL, Dalgleish AG, Steward WP, O’Byrne KJ. Angiogenesis as biomarker and target in cancer chemoprevention. Lancet Oncol, 2: 726-732, (2001).
47. Goh, V., et al., Functional imaging of colorectal cancer angiogenesis. Lancet Oncol, 8: p. 245-55, (2007).
48. Hayano, K., et al. Quantitative Measurement of Blood Flow Using Perfusion CT for Assessing Clinicopathologic Features and Prognosis in Patients with Rectal Cancer. Dis Colon Rectum, 52(9): p. 1624-9, (2009).
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 43 of 45 Version 1.0_12th Jul 2010
49. de Vries, A., et al. Tumour Microcirculation and diffusion predict therapy outcome for primary rectal carcinoma. Int J Rad Oncol Biol Phys, 56(4): p. 958-65, (2003).
50. de Lussanet, QG., et al. Dynamic contrast-enhanced magnetic resonance imaging of radiation therapy-induced microcirculation changes in rectal cancer. Int J Radiat Oncol Biol Phys, 63: p. 1309–15, (2005).
51. Bellomi, M., et al. CT perfusion for the monitoring of neoadjuvant chemoradiation therapy in rectal carcinoma. Radiology, 244:486–93, (2007).
52. Sahani, DV., et al. Assessing tumor perfusion and treatment response in rectal cancer with multisection CT: initial observations. Radiology, 234: p. 785–35, (2005).
53. Kierkels, RG., et al. Comparison Between Perfusion Computed Tomography and Dynamic Contrast-Enhanced Magnetic Resonance Imaging in Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009. Article in Press.
54. Tuncbilek, N., et al. Dynamic MRI in indirect estimation of microvessel density, histologic grade, and prognosis in colorectal adenocarcinomas. Abdom Imaging, 29: p. 166–72, (2004).
55. Atkins, G.. et al. Dynamic contrast-enhanced magnetic resonance imaging is a poor measure of colorectal cancer angiogenesis. Br J Surg, 93: p. 992–1000, (2006).
56. Li, ZP., et al. Tumor angiogenesis and dynamic CT in colorectal carcinoma: radiologic-pathologic correlation. World J Gastroenterol, 11: p .1287–91, (2005).
57. Goh, V., et al., Colorectal tumor vascularity: quantitative assessment with multidetector CT: do tumor perfusion measurements reflect angiogenesis? Radiology, 249: p. 510–7, (2008).
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol Confidential
Eudract No: 2010-020621-40 Page 44 of 45 Version 1.0_12th Jul 2010
APPENDIX 1: ECOG PERFORMANCE STATUS EVALUATION
0 Fully active, able to carry on all pre-disease performance without restriction
1 Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g., light house work, office work
2 Ambulatory and capable of all selfcare but unable to carry out any work activities. Up and about more than 50% of waking hours
3 Capable of only limited selfcare, confined to bed or chair more than 50% of waking hours
4 Completely disabled. Cannot carry on any selfcare. Totally confined to bed or chair
REC No: 10/H0604/61

SONATINA Clinical Trial Protocol
Eudract No: 2010-020621-40 Page 45 of 45 Version 1.0_12th Jul 2010 REC No: 10/H0604/61
Confidential
APPENDIX 2: RECIST CRITERIA FOR EVALUATION OF RADIOLOGICAL RESPONSE
Revised RECIST guidelines (version 1.1) will be used in the assessment of disease response of the primary tumour or radiological N1-2 disease on MRI scans at baseline and at 8 weeks post-SCRT. The full guidelines can be found at http://www.eortc.be/Recist/Default.htm Summary of RECIST guidelines: Baseline Measurements a) Baseline documentation of ‘target’ and ‘non-target’ lesions: up to 2 target lesions/organ involved (up to 5). b) Longest axis for target non-nodal lesions and shortest axis for target nodal lesions should be measured and recorded. Nodes must be ≥15 mm in short axis diameter to qualify as measurable target lesions. c) Sum of target lesion diameters calculated and reported as baseline sum diameter. Response Evaluation a) Target Lesions Complete Response (CR): Disappearance of all target lesions. Any pathological lymph nodes
(whether target or non-target) must have reduction in short axis to <10 mm.
Partial Response (PR): At least a 30% decrease in the sum of diameters of target lesions, taking as reference the baseline sum diameters.
Progressive Disease (PD): At least a 20% increase in the sum of diameters of target lesions. In addition to the relative increase of 20%, the sum must also demonstrate an absolute increase of at least 5 mm. The appearance of 1+ new lesions is also considered progression.
Stable Disease (SD): Neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD,
b) Non-target Lesions Complete Response (CR): Disappearance of all non-target lesions and normalisation of tumour
marker level. All lymph nodes must be non-pathological in size (<10mm short axis).
Non-CR/Non-PD: Persistence of one or more non-target lesion(s) and/or maintenance of tumour marker level above the normal limits.
Progressive Disease (PD): Unequivocal progression of existing non-target lesions. The appearance of 1+ new lesions is also considered progression).
Overall Response Assessment Based on a time point response assessment of target and non-target lesions at 8 weeks. Target lesions
Non-target lesions New lesions
Overall response
CR CR No CR CR Non-CR/Non-PD No PR CR Not evaluated (NE) No PR PR Non-CR/Non-PD or NE No PR SD Non-CR/Non-PD or NE No SD NE Non-PD No NE PD Any Any PD Any PD Any PD Any Any Yes PD








![[MS-OXOCNTC]: Contact Object Protocol Specification · Contact Object Protocol Specification Release: Wednesday, August 6, 2008 Contact object propertiesContact Contact Contact .](https://static.fdocuments.us/doc/165x107/5f02431d7e708231d40362fd/ms-oxocntc-contact-object-protocol-specification-contact-object-protocol-specification.jpg)