بسم الله الرحمن الرحیم. Bordetella pertussis Roxana M.Ghanaie Ped Infectious...
107
م ی ح ر ل ا ن م ح ر ل ه ا ل ل م ا س ب
-
Upload
anna-williamson -
Category
Documents
-
view
222 -
download
5
Transcript of بسم الله الرحمن الرحیم. Bordetella pertussis Roxana M.Ghanaie Ped Infectious...

الرحیم الرحمن الله بسم

Bordetella pertussis
http://www.hhmi.princeton.edu/sw/2002/psidelsk/Microlinks.htm
Roxana M.Ghanaie
Ped Infectious Disease Subspecialist

Bordetella pertussis Basics
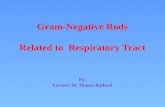
• Aerobic, Gram negative coccobacillus• Alcaligenaceae Family• Specific to Humans• Colonizes the respiratory tract
– Whooping Cough (Pertussis)

Bordetella pertussisBordetella pertussis
Jules Bordet1870-1961
is a bacterium identified in 1900 by Jules Bordet and Octave Gengou but isolated only in 1906 because of the development of a medium containing potatoes extract and rabbit blood

Source: WHO/IVB
pneumococcal (28%)
measles (21%)
rotavirus (16%)
Hib (15%)pertussis (11%)tetanus (8%)
76% 24%
yellow fever (1%)diphtheria (<1%) polio (< 1%){
Estimated annual childhood deaths, 2002
10.5 million deaths under 5 years of age1.4 million from diseases where vaccination is currently available 1.1 million from diseases where vaccines will be available by 2008
Meningococcal (< 1%)

0
50,000
100,000
150,000
200,000
250,000
300,000
1922 1930 1940 1950 1960 1970 1980 1990 2000
Year
Nu
mb
er o
f ca
ses
0
2,000
4,000
6,000
8,000
10,000
12,000
1980 1990 2000
Nu
mb
er
of
ca
se
s
Reported Pertussis Cases U.S., 1922-2003*

Pertussis in a vaccinated country vs a non vaccinated country
1-2 3-4 5-6 7-12 2 3 4 5 6 7 8-12 15-20 20-25 25-35
Nu
mb
er o
f ca
ses
Month Year
Low vaccine coverage *High morbidity and mortality in infants *Regular asymptomatic contacts throughout life *Unknown epidemiology in adults
High vaccine coverage *Low morbidity and mortality in infants *Few asymptomatic contacts throughout life *Increase in susceptible adolescents and adults

Why speaking about Pertussis?
• Iran pertussis incidence 2010 : 0.5/ 100000• DTP3 coverage more than 95%

و محتمل سرفه سياه بروز ميزان روندثالث واكسن سومنوبت پوشش
ايران) اسالمي (1370-1391جمهوري
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1370
1371
1372
1373
1374
1375
1376
1377
1378
1379
1380
1381
1382
1383
1384
1385
1386
1387
1388
1389
1390
1391
INC
ED
EN
CE
RA
TE
S/1
00.0
00
60
65
70
75
80
85
90
95
100
CO
VE
RA
GE
PERTUSSIS DTP3

سياه محتمل موارد فراوانيعلوم دانشگاه برحسب سرفه
1391پزشکی
0
50
100
150
200
250Ϫϴ
ϣϭέ
ϥΎϬ
ϔλ
ίήΒϟ
ίϮϫ
ϡϼϳ
ϞΑΎΑ
ΪϨΟΰ
ϴΑ
ΰϳήΒ
Η
ϥή
ϬΗ
ΩέϮϨ
ΠΑ
ϥΎΠ
ϧί
ϲΘθ
ϬΑ
Ϧϳϭ
ΰϗ Ϣϗ
ΝΪϨ
Ϩγ
ϩΎθ
ϧΎϣήϛ
ϥΎΘδ
Ϡ]
ϥέ
ΪϧίΎ
ϣ
ΪϬθ
ϣ
ϥΪ
Ϥϫ Ωΰϳ
ϥΎΘγ
ήϟ
ϩΎ$θϧΩ

مثبت موارد جغرافیایی توزیعدركشور سرفه سیاه 1391بیماری
0
5
10
15
20

Bordetella pertussis virulence determinantsBordetella pertussis virulence determinants
Adhesins: adhesion => multiplication and colonisation of respiratory tract
Toxins: local and systemic cytopathogenic effects
Filamentous hemagglutinin
(FHA)
Pertactin (PRN)
Fimbriae (FIM)
TCT
Adenylate cyclase hemolysin (AC-Hly)
Pertussis toxin (PT)
TCT
BrkA, Tcf, Vag8
TCT

• The incubation period of pertussis is usually 7 to 10 days, with a range of 4 to 21 days.
• The clinical course of illness is divided into three stages.( age, vaccination, waning)
1/ The catarrhal stage is characterized by the onset of runny nose, sneezing, low-grade fever, and a mild cough. Cough gradually becomes more severe (1-2 weeks)
Classic Manifestation

• 2/ The paroxysmal stage is characterized by coughing fits (paroxysms), which may be followed by a high-pitched inspiratory whoop, vomiting, and/or apnea. (1-6 weeks), but may continue for 10 weeks
Classic Manifestation

• 3/The convalescent stage is characterized by fewer paroxysmal coughing episodes and usually disappears in 2-3 weeks, but may continue for months

Complications• Losing weight, pneumonia, otitis, seizure,
encephalopathy, apnea• Epistaxia, melena, subdural hematoma,
inguinal hernia, rectal prolapse,

Infants
The severity of pertussis and the rapidity of its progression in young infants is effected by a number of factors such as: the presence of transplacentally acquired maternal antibodies to B. pertussis, the infectious dose of bacteria that the infant receives, co-infection with respiratory viruses and perhaps genetic factors related to the pathogen or the infant.

Short catarrhal period, longer convalescence periodCough,feeding abn, res distress,apnea,cyanosis, bradycardia, whoop uncommon, paroxysms and this may lead to apnea, gasp, hypoxia and occasionally seizures Initially the chest is clear on auscultation but in fatal cases B. pertussis pneumonia is always present. Co-infection with respiratory viruses (particularly RSV and adenoviruses) can confuse the diagnoses because of a bronchiolitic picture (air trapping and expiratory distress).
Infants

Pertussis Among Adolescents and Adults
• Accounts for up to 7-30% of cough illnesses per year
• Disease often milder than in infants and children
• Infection may be asymptomatic, or may present as classic pertussis
• Cough may last 21 d, st. paroxysmal

Clinical manifestation in immunized
• Mild , unrecognized cough• Prolonged cough• Persons with mild disease may transmit the
infection• Older persons often source of infection for
children• Adults: sleep disturbances syncope, incontinence, rib Fx,pneumonia


Transmission• Very Contagious, 80% secondary attack rate among
susceptible persons( even immunized) • Transmission occurs via respiratory droplets, direct
contact with respiratory secretions from infected individuals
• Parents are a common source of B. pertussis infections for infants,
• grandparents, uncles , Aunts also provide another potential source of infection


Transmission
Pertussis Infectious Period: • Most infectious during the catarrhal (early) stage. • Infectious during the first 21 days of cough if not treated
with appropriate antibiotic. • No longer infectious after 5 days of treatment with
appropriate antibiotic• Length of communicability: age, immunization status,
appropirate antibiotic therapy• Isolation: standard, droplet

B. parapertussis• B. parapertussis infection in humans can cause
unrecognized infection, mild pertussis, or classic pertussis
• B. bronchisepica

DD prolonged cough
• Adenovirus• Para influenza• Influenza A,B• M.pneumonia• RSV• C.trachomatis• C. pneumonia

DD prolonged cough
• spasmodic attacks of coughing may be observed in children with:
• bronchiolitis, bacterial pneumonia, cystic fibrosis, or tuberculosis. Afebrile Pneumonia Syndrome
• The cough associated with: sinusitis, airway foreign body

• Laboratory confirmation of pertussis is difficult and delayed. Therefore, clinicians need to make the diagnosis of pertussis presumptively in patients with a history of intense paroxysmal or chronic coughing with or without whooping, color changes, posttussive vomiting, incomplete or absent pertussis vaccination, and finding of lymphocytosis on laboratory examination.

CXR Indications
• 1/ <1y• 2/ toxic• 3/ progressive cough>3 w• 4/ res distress• 5/ probable underlying dis( CF, CHD,forign
body, Hilar LAD)

Chest Xray
• Most common : Normal• Shaggy heart( central airway not periph)• Hyperinflation, hyper lucent lung• Micro athelectasia• Secondary bac. Pneumonia• Bronchiolitis oblitrans( adeno, influ, measles,
pertussis)• pneumothorax


Diagnosis
• Isolation by culture , preferred method of diagnosis(100% specificity)
• Although PCR more sensetive,culture may be necessary for further case analysis including evaluation for
antibiotic resistance and molecular typing
http://medinfo.ufl.edu/year2/mmid/bms5300/images/d7053.jpg

• Neg culture: • Previously immunized• Antibiotic usage• More than 3 w after cough onset• Bad-handled specimen

Definition:
Clinical Case Definition of Pertussis • A cough illness lasting at least 14 days with
one of the following: • paroxysms of coughing, • inspiratory “whoop”,• or post-tussive vomiting,• and without other apparent cause (as
reported by a health professional).

Laboratory Criteria for Pertussis Diagnosis • Isolation of Bordetella pertussis from a clinical
specimen (culture positive), or • Positive polymerase chain reaction (PCR) assay for B.
pertussis DNA. Note: Serological testing for B. pertussis is not
standardized • Serology and DFA results should not be relied on as a
criterion for laboratory confirmation of pertussis.
Definition:

Pertussis Case Classification
• Confirmed: a/ A positive culture for B. pertussis and cough illness of any
duration, or b/ Meets the clinical case definition and is confirmed by
PCR, or c/ Meets the clinical definition and is epidemiologically
linked directly to a case confirmed by either culture or PCR.
• Probable: A case that meets the clinical case definition, is not laboratory confirmed, and is not epidemiologically linked to a laboratory-confirmed case; also includes cases meeting the outbreak case definition

Outbreaks
• Outbreak: Two or more cases involving two or more households clustered in time (e.g., occurring within 42 days of each other) and either epi-linked or sharing a common space (e.g., in one building) where transmission is suspected to have occurred (e.g. a school).
• One case in an outbreak must be lab confirmed (PCR positive and meets case definition, or culture positive). In an outbreak setting, a case may be defined as an acute cough illness lasting ≥ 2 weeks without other symptoms.

Suspect: a clinical syndrome compatible with pertussis; an illness consistent with pertussis and without other apparent cause, such as:
• a. cough of ≥ 7 days, or • b. paroxysmal cough of any duration, or • c. cough with inspiratory whoop, or • d. cough associated with apnea in an infant, or • e. cough in a close contact of a confirmed or
probable case. Summary of Pertussis Investigation and Control Guidelines Colorado Department of Public Health and Environment Communicable Disease Epidemiology Program

سرفه سياه بيماري مراقبت
مشمول هاي بيماري دسته از سرفه سياه.فوريگزارشدهي باشد مي
اساس بر بيماري مورد مراقبت بيماري مبناي. شود مي انجام
شروع از قبل است الزم محتمل مورد هربرداري درمان نمونه مركز جهت آزمايشگاه به
شود ارجاع بهداشت مراقبت سطوح تمامي انجام گزارشدهيدر
وجود بيماري مورد كه مواردي در گيرد، ميگزارش ارسال الزامي صفرندارد بيماري
است.

Management:
• The desired outcomes are:1/ observing the severity of cough2/ limiting the number of paroxysms, 3/ providing assistance when necessary, 4/ maximizing nutrition, rest, and recovery, 5/ follow the course of disease 6/ prevent/treat complications

• Admitt:1- all infants<3 m despite severity & all 3-6 m except the
attacks are mild as observed by physician2- with complications(intractable nausea and vomiting,
failure to thrive,seizures, encephalopathy, or for patients with sustained hypoxemia during coughing paroxysms who require supplemental oxygen,) hx of prematurity in infant, with underlying cardiac, pul, neuromuscular dis

Management
• For the hospitalized patient, in addition to standard precautions, droplet precautions are recommended
• Monitor heart rate, respiratory rate, and oxygen saturation of hospitalized patients continuously,especially in relation to coughing paroxysms. Coughing, feeding, vomiting, and weight changes should be recorded.

Management:
• Oxygen,suction,hydration, nutrition• Patients who are severely ill may require treatment in an
ICU.• Investigate all probable, pertussis reports. • Recommend antibiotics for the index case (first case
reported to public health authorities), all household and close contacts. Antibiotic inspite of age, immunization Hx

Report & find contacts
• Only confirmed and probable cases are reported.• Recommend DTaP/Tdap vaccination according to
appropriate age for exposed children, adolescents and adults.
• Exposed children < 7 years of age whose last DTP ( 4th dose) was more than 3 years ago should be
vaccinated.( more than 6m after 3rd dose)

• Evaluate close contacts for pertussis symptoms, and when possible collect specimens for lab testing from symptomatic persons
• Satisfactory documentation of disease: recovery of B. pertussis on culture, OR typical symptoms and clinical
course when epidemiologically linked to a culture- proven case
Report & find contacts

Treatment (cont)
During catarrhal stage ameliorate disease After cough establishment, does not generally
lessen duration; protect others Limited benefit if begun >21 days after onset/exposure Exception: high risk cases/contacts - treat up to 6 weeks

Treatment
• Antibiotic therapy– Erythromycin– Azithromycin– Clarithromycin
http://www.aboutthatbug.com/AboutThatBug/files/CCLIBRARYFILES/FILENAME/0000000032/033_lg.jpg http://www.vet.purdue.edu/bms/courses/lcme510/chmrx/macrohd.htm

Treatment
ErythromycinFor children: 40-50 mg/kg/d in 4 divided
doses;10-14 days• For adults: 1 to 2 g/day given every 6 h

Treatment
Azithromycin• for children: at 10 mg/kg on day 1 and 5
mg/kg on days 2 to 5 as a single dosefor 5 days• 10-12 mg/kg/d PO in 1 dose for a total of 5
days. ( < 6m)• for adults: 500 mg on day 1 and 250 mg on
days2 to 5

Treatment
Clarithromycin • for children: at 15 to 20 mg/kg/day in two
divided doses for 7 days • for adults: 1 g/day in two doses for 7 days

Treatments
Trimethoprim(T)/Sulfamethoxazole (S)8mg/kg T + 40 mg/kg S/d in 2divided doses; 14 days• Erythromycin and clarithromycin are not
recommended in infants younger than 4-6 w because their use has been associated with increased risk for infantile hypertrophic pyloric stenosis (IHPS).
• Resistant to macrolid: rare• Cephalosporine, PN not effective

Treatment
• Humans infected with B. parapertussis or B. holmesii
• macrolide therapy indicated above.• In contrast, however, B. bronchiseptica is usually
resistant to Erythromycin Most sensitive to aminoglycosides, extended-spectrum third-generation penicillins, tetracyclines, quinolones, and trimethoprim-sulfamethoxazole.

Treatment
• It has been observed in numerous small studies that pertussis infant deaths relate directly to the degree of leukocytosis
• double volume exchange transfusion, to lower the white blood cell count

Treatment
• Pertussis-specific immune globulin is an investigational product that may be effective in decreasing paroxysms of
cough but requires further evaluation.• The use of corticosteroids, albuterol, and
other beta2-adrenergic agents for the treatment of pertussis is not
supported by controlled, prospective data

Exclusions fromwork/school
Symptomatic: first 5 days of treatment
Symptomatic, refuses treatment: exclude for 21 days from onset of symptoms
Asymptomatic exposure: no exclusion

Complications in Infants• Pneumonia( in 22% infants)• Seizures( in 2% infants)• Encephalopathy( less than 0.5% infants)• FTT,Death 0.3%( 1% in less than 2 m-old)• SIDS( ???)

Prognosis• Prognosis for full recovery is excellent; however, patients with
comorbid conditions as previously described have a higher risk of morbidity and mortality• Leukocytosis, particularly WBC counts of more than 100,000,
has been associated with fatalities from pertussis.• Another study showed that WBC counts of more than 55, 000 and pertussis complicated by pneumonia were
independent predictors of fatal outcome in a multivariate model.

Use a narrow definition ofclose contact
Close contacts: • Household contacts; • Other persons having direct prolonged exposure to the
case while case was contagious and was coughing or sneezing.
1. Direct face-to-face contact for an undefined time period with an infectious pertussis case (case coughing < 21 days and has not completed 5 days of appropriate antibiotic treatment).

2. . Shared confined space in close proximity for a prolonged period of time, such as ≥ 1 hour, with an infectious pertussis case. For example, riding in a car with a pertussis case.
3. Direct contact with respiratory, oral, or nasal secretions from an infectious pertussis case (e.g., an explosive cough or sneeze in the face, sharing food, sharing eating utensils, kissing, mouth-to-mouth resuscitation, or performing a full medical exam including examination of the nose and throat without wearing a mask).
Summary of Pertussis Investigation and Control Guidelines Colorado Department of Public Health and Environment Communicable Disease Epidemiology Program

Exposed• Household, close contacts, health care worker:• Check immunization, initiate, complete• Chemopx for all contacts regardless age, immunization• If start later than 21 d after exposure, give only to
highrisk: young infant, pregnant, care taker of infants• Monitor for 21 d after last contact, for symptoms• Evalute symptomatic exposed persons and exclude from
public setting and report confirmed, probable cases

QUESTIONS?

Diphtheria

Etiology
گرم • باسیل دیفتری باکتریوم کورینهحرکت بدون شکل، چماقی باریک، مثبت،
آمیزی رنگ در که است اسپور بدون ومیگیرد رنگ نامنظم بطور
باکتریوم • کورینه زای سم های سویه ) - بندرت ) و لوفلر کلبس باسیل دیفتری
. اولسرنس باکتریوم کورینه
[1

Etiology
بلفانتی، ) 4• اینترمدیوس، میتیس، بیوتیپگراویس(.
توکسیکوژن • توانند می ها بیوتیپ این تمامیباشند.
حال • در و جوانتر های باسیل توسط بیشتر سم . شود می تولید سریع نمو و رشد
ناچیز • مقادیر در حتی دیفتری میکروگرم 130سماست کشنده بدن وزن کیلوگرم بازای
حدود 94-99/9%• و مدیوس انتر و گراویس انواع از80-88. هستند% بیماریزا تیس می انواع

Etiology
در • دیفتریه باکتریوم کورینه اصلی مخزن . بصورت عالمت بدون افراد است انسان
. کنند می عمل باسیل مخزن• : بیماری روز 7-2کمون

Clinical Manifestation
ایمنی • سطح عفونت، محل به بسته عالئم . دارد ان سم سیستمیک انتشار و میزبان
ورود • اناتومیک محل اساس بر دیفتری : دیفتری انواع به غشا ایجاد و عفونت
/ حلق ها لوزه بینی، مجاری / ) و) پوست تراکه، الرنگو حنجره ، فارنکس
. شود می تقسیم غیره

Clinical Manifestationتنفسی • بصورت دیفتری معموال
الرنگوتراکئیت یا و غشایی نازوفارنژیت . عفونت اگر نماید می بروز انسدادی
بروز و خفیف تب با باشد نداشته گسترشعرض در تظاهرات نمایان 2-1تدریجی روز
. اندامها و پشت درد استفراغ، لرز، شود می . و است خفیف گلو درد ندارد وجود معموال
. باشد داشته بیحالی و ضعف تواند می بیمارشدت به بستگی اغلب عمومی عالئم شدت
. دارد موضعی ضایعه

Clinical Manifestation
بینی : • قدامی بصورت دیفتری ابتدا دردو هر یا و یک از رقیق ترشح با سرماخوردگی
. است سیستمیک شدید عالئم بدون و است بینی . شود بومی بد و چرکی غلیظ، سپس ترشحات
. موارد در شود می دیده بینی داخل در سفید غشاقسمت و بینی های پره در ترشحی زخم شدید . معموال عمومی حال میشود دیده لب فوقانی
بینی مخاط از سم کمی مقدار زیرا است خوب . بینی، ترشح در باسیل وجود بعلت شود می جذب
. است زیاد دیگران به ابتال و بیماری انتشار خطر. دارد وجود شیرخواران در بیشتر فرم این

Clinical Manifestation• : حلق و لوزه و دیفتری تدریجی بیماری شروع
کوفتگی، اشتهایی، بی اختصاصی غیر عالئم با . روز دو تا یک غشا است فارنژیت و پایین تب
غشا کم کم و شده شروع نقطه یک از بعد،. گیرد می را لوزه دو هر اعظم بخش
ایمنی • وضعیت به بسته ان گسترش شدت. است متغیر بیمار
بوده • خاکستری به متمایل زرد رنگ غشا. دارد چسبندگی لوزه به بسختی و
•. است درگیر کوچک زبان اغلب

Clinical Manifestation
نا • و بد بسیار دهان بوی غشا نکروز اثر در . و بزرگ اکثرا لنفاوی غدد است مطبوع
. است حساسنسوج • و لنفاوی غدد تورم شدید اشکال در
گردن شدید تورم بصورت انسداد نرم با همراه . این کند می بروز فوقانی هوایی راههای
. است سفت و دردناک گذار، گوده گرم، تورمباالی • کودکان در شود 6بیشتر می دیده سال
و گراویس های سویه توسط معموال وشود می ایجاد اینترمدیوس


Clinical Manifestation
شدن • ازاد میزان به بسته عالئم شدت . دارد غشا گسترش و توکسین
• ، عروق کوالپس ، شدید موارد دربینی، از خونریزی تنفسی، کوالپس
پورپورا و منتشر خونریزی گاه دهان،ظاهر و است بد عمومی حال دارد، وجودوجود تب است رنجور و پریده رنگ بیمار
نبض تعداد ولی است خفیف یا و ندارد . است باال نامتناسب بطور

دو • یا و یکطرفه بطور کام فلج است ممکنوجود بینی از غذا برگشت و بلع اشکال ، طرفه
. باشد داشتهعرض • در ومرگ هشیاری،کوما 10تا 7اختالل
. افتد می اتفاق روز• . موارد در دارد محیطی نوروپاتی و میوکاردیت
منجر وگاه است تر آهسته بهبود ، کمتر شدت با . موارد در شود می نوریت و میوکاردیت به
عرض در غشا و است متغیر بهبود زمان خفیف7-10. شود می کنده روز
حلق • دیفتری در توکسین جذب از ناشی عوارضاست قسمتها سایر دیفتری از تر شدید لوزه و

حنجره :دیفتری•. دارد فوری اقدام به نیاز ،گاه طب اورژانسمی • وندرتا است حلق دیفتری به ثانویه اغلب
. تیس می سویه بدنبال اغلب باشد اولیه تواندشود می فارنژیت ایجاد خالف بر اینموارد در
ومی نیست متصل بسختی غشا دیفتری،تنفسی مجرای انسداد باعث و شده جدا تواند
. است. کروپ موارد سایر شبیه عالئم شودعوارض • و بوده کم توکسین جذب اینموارد در
. شود می دیده بندرت آن

Transmission
و • قطرات طریق از انتشار معمول بطوراز پوست و ،بینی حلق ترشحات با تماس
. شود می انجام ناقل فرد یا و بیمارتواند • می باسیل درمان عدم صورت در
زخم در یا و حلق یا و بینی شحات تر دراز چشم یا و از 6تا 2پوست بعد هفته. بماند زنده آلودگی
برای • سرایت مناسب درمان صورت دراز کمتر است 4مدت پذیر امکان روز

Transmission
بیماران • با نزدیک ازتماس ناشی انتقالمناطق به سفر در بخصوص ناقلین یا و
اندمیک مناطق از مسافرین یا و اندمیکاست.
آلوده، • اشیائ طریق از دیفتری بندرتمی منتقل لبنیات سایر ویا شیرخام
بین. از باسیل شیر جوشیدن اثر در شودرود می

بیماری مورد تعریفبیماری • مورد بالینی که: تعریف بیماری هر
فارنژیت، باچسبنده غشائ بهمراه تونسیلیت یا و رنژیت ال
. نماید مراجعه بینی یا و حلق ها، لوزه روی

ازمایشگاهی اثبات معیار:بیماری
از • دیفتری باکتریوم کورینه کردن جداچهار حداقل افزایش یا و بالینی نمونه
دو در سرم بادی آنتی تیتر در برابرنمونه ( دو هر صورتیکه در متوالی نمونه
انتی یا و توکسوئید تجویز از قبل( باشد توکسین

موارد بندی گروه محتمل • داشته: مورد را بالینی معیار که است موردی
باشد.قطعی • دارای: مورد بالینی معیارهای بر عالوه که موردی
اپیدمیولوژیک ارتباط یا و باشد نیز ازمایشگاهی معیارهای . باشد داشته بالینی شده ثابت مورد با شده تایید
هستند: • بالینی عالیم فاقد که را مواردی تبصره ( نباید ( سالم ناقلین است مثبت انها در کشت ولی
. نمود گزارش قطعی یا و محتمل موارد بعنوان

Management
1/ Critical care needs 2/ Neutrilize toxin3/ Eradicate C. diphtheria4/ Complications• Mechanical ventilation (combination of
airway obstruction by the diphtheritic membrane and peripharyngeal edema )

Anti toxin
• Specific antitoxin is the mainstay of therapy and should be administered on the basis of clinical diagnosis
• neutralizes free toxin only. • Efficacy diminishes with elapsing time after
the onset of mucocutaneous symptoms. • Only an equine preparation is available

Anti toxin
• Antitoxin is administered once at an empiric dose based on the degree of toxicity, site and size of the membrane, and duration of illness.
• Most authorities prefer the intravenous route, with infusion over 30-60 minutes.

Anti toxin• Antitoxin is probably of no value for local
manifestations of cutaneous diphtheria, but its use is prudent because toxic sequelae can occur.
• Commercially available IVIG ,contain antibodies to diphtheria toxin; is not proved or approved
• Antitoxin is not recommended for asymptomatic carriers.

Antitoxin
اساس • بر سم ضد تزریقی اندازه دوز و محلزمان مدت و سم اثرات شدت دیفتری، غشای
بیماری :شروع شود می تعییننشاندهنده • نرم و منتشر گردنی لنفادنوپاتی وجود
است سم شدید تا متوسط جذبمساوی • یا و کمتر بمدت حنجره یا و حلق درگیری
واحد 40000-20000ساعت، 48فارنژیال • نازو واحد 60000-40000درگیریبمدت • یا گسترده یا شدید یا 3بیماری و روز
گردن شدید تورم یا و واحد 120000-80000بیشتربعضی • ولی ندارد اثر معموال پوستی دیفتری در
کنند 20000-40000 می توصیه را واحد

Antimicrobial• Eradication, prevent transmission, halt toxin production• C diphtheriae is usually susceptible to various agents in vitro,
including penicillin,erythromycin, clindamycin, rifampin, and tetracycline.
• Penicillin and erythromycin are only recommended for treatment.
• Erythromycin is marginally superior to penicillin for eradication of nasopharyngeal infection.
• Resistance to erythromycin is common in closed populations if the drug has been used broadly

Antimicrobial
تزریقی • یا و خوراکی مایسین 14بمدت اریتروحداثر 50-40روز( وزن، کیلوگرم هر 2بازای
( روز در گرمسیلین • واحد 100-150000- تزریقی Gپنی
در منقطع وزن کیلوگرم هر ) 4بازای داخل دوزمدت برای روز 14وریدی
سیلین • عضالنی پروکایین Gپنی تزریقیبدن 50000-25( وزن کیلوگرم هر بازای واحد
( بمدت منقسم دوز دو در روز 14روزانه

Antimicrobial
• Antibiotic therapy is not a substitute for antitoxin therapy.
• Elimination of the organism should be documented by at least 2 successive cultures from the nose and throat (or skin) obtained 24 h apart after completion of therapy.
• Treatment with erythromycin is repeated if culture results remain positive

Vaccine
• Diseases dose not produce immunity, vaccinate the patient in convalescent period

Surgical Care
• Otolaryngeal assessment is needed in patients with severe respiratory or neurologic complications or as part of critical care.

Consultation
Cardiologist: Elevation of serum SGOT closely parallels the severity of
myonecrosis.arise during the first 10 days of illness or may be delayed
until 2-3 weeks after In electrocardiographic tracings, a prolonged PR
interval, changes in the ST-T wave, and single or progressive cardiac dysrhythmias can occur, such as first-degree, second-degree, and third-degree heart block, atrioventricular dissociation, and ventricular tachycardia. Toxic cardiomyopathy and myocarditis

• Neurologist: • parallel the extent of primary infection and are
multiphasic in onset.• Hypersthesia and local paralysis of the soft
palate • Weakness of the posterior pharyngeal,
laryngeal, and facial nerves , causing a nasal tone in the voice, difficulty in swallowing, and risk of death from aspiration.

Neuropathy
• Cranial neuropathies characteristically occur in the fifth week and lead to oculomotor and ciliary paralysis, which manifest as strabismus, blurred vision, or difficulty with accommodation.
• Symmetric polyneuropathy begins within 10 days to 3 months after oropharyngeal infection, motor function deficit with diminished deep tendon reflexes. DD polyneuropathy of Landry-Guillain-Barré syndrome.
• Paralysis of the diaphragm can ensue.

Close contact
• Promptly identify close contacts of patients in whom diphtheria is suspected. in the household and other persons with a history of habitual close contact with the patient.

Close contact
• For close contacts, irrespective of their immunization status, the following measures should be taken:
• Surveillance for 7 days for evidence of disease• Culture for C diphtheriae• Antimicrobial prophylaxis with oral erythromycin
(40-50 mg/kg/d for 10 d; not to exceed 2 g/d) or a single intramuscular injection of penicillin G benzathine (600,000 U for children who weigh < 30 kg and 1.2 million U for children weighing >30 kg and adults)

Contacts
• Obtain repeated pharyngeal cultures from contacts proven to be carriers at a minimum of 2 weeks after completion of therapy.
• Asymptomatic, previously immunized, close contacts should receive a booster dose of a preparation containing diphtheria toxoid (DTaP, DT, Tdap, or Td, depending on age) if they have not received a booster dose of diphtheria toxoid within 5 years. Immunize children in need of the fourth dose.
Contacts who cannot be kept under surveillance should receive benzathine penicillin G (not erythromycin),
• and a dose of , DT, or Td (administered if the patient has not received a booster injection within 1 year)

Mortality/Morbidity
• Death due to mechanical airway obstruction or cardiac involvement with circulatory collapse
• In at least 10% of patients with respiratory tract diphtheria

Mortality/MorbidityPrognosis depends on:• The virulence of the organism (with the gravis
strain usually accounting for the most severe disease),
• The age and immunization status of the patient, • The site of involvement, • The speed with which antitoxin is administered

Mortality/Morbidity
• Airway obstruction by the diphtheritic membrane and peripharyngeal edema combine to pose a risk of death in patients with diphtheria.

Mortality/Morbidity
• For patients in whom disease is recognized on day 1 and therapy is promptly initiated, the mortality rate is approximately 1%.
• If appropriate treatment is withheld until day 4, the mortality rate rises to 20%

Mortality/Morbidity
• Toxic cardiopathy occurs in approximately 10-25% of patients with diphtheria and is responsible for 50-60% of deaths.
• Neurologic complications parallel the extent of primary infection and are multiphasic in onset.

دیفتری بیماری مراقبت
پائین • بیماری بروز میزان که کشورما دراز بیش ایمنی پوشش میزان و 90است
و محتمل مورد هر اطالعات است درصدبرمورد قطعی و مبتنی سطوح بوده از
فوری گزارش بصورت باال به پائین . اطالعات از شود می انجام تلفنی
و پایش جهت توان می مراقبت سیستمبخشی اثر نتیجه عنوان به بیماری بروز
. کرد استفاده کنترل های برنامه

اولين در الزم اقداماتبه بيمارمحتمل با برخورد
-ديفتري فوري دهي بيماريگزارش- بيمار سازي از جدا نمونه دو كشت كه وقتي تا
وبيني حلق ترشحات . امكان اگر شوند منفي باسيل نظروجود از
نباشد موجود روز14كشتمناسب هاي بيوتيك آنتي با درمان اتمام از پس
داد خاتمه را بيمار سازي جدا توان .ميبيمار توكسين - به آنتي محل تزريق برحسب
بيماري ت شد و ضايعهبيوتيك - آنتي با تزريق جي پروكائين سيلين پني
به بالغ افراد و كودكان براي مربوطه دزهاي.روز 14مدت

TREND OF PROBABLE DIPHTERIA CASES INCEDENCE RATES
& DTP3 COVERAGE (I.R.IRAN 1370-1391)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1370
1371
1372
1373
1374
1375
1376
1377
1378
1379
1380
1381
1382
1383
1384
1385
1386
1387
1388
1389
1390
1391
INC
ED
EN
CE
RA
TE
/100
.000
82
84
86
88
90
92
94
96
98
100
CO
VE
RA
GE
DIPHTERIA DTP3

دیفتری محتمل موارد فراوانيپزشکی علوم دانشگاه برحسب
1391
0
20
40
60
80
100
120
140
Ϫϴϣϭ
έϞ
ϴΑΩέ
ϥΎϬ
ϔλ
ίϮϫ
ϡϼ
ϳϞΑ
ΎΑήϬ
ηϮΑ
ΪϨΟή
ϴΑΰϳ
ήΒΗ
ϥή
ϬΗϡή
ϬΟ
aέΎϴΘ
ΨΑΩέ
ϮϨΠΑ
ϥΎΠ
ϧίέ
ϭΰΒγ
ϥΎϨϤ
γΩϭ
ήϫΎη
gΘθ
ϬΑΪϴϬ
ηί
ήϴη
Ϧϳϭΰ
ϗ ϢϗϥΎ
ηΎk
Νήk
ΝΪϨ
Ϩγϥ
Ύϣήk
ϩΎθϧ
Ύϣήk
ϥΎΘδ
Ϡo
ϥϼ
ϴo
ϥΎΘγ
ήϟ
aέΎγ
q έ
ΪϬθϣ
ϥΎ
oΰϣήϫ
ϥΪϤ
ϫϪϴ
ϣϭέ
ϲΑΩέ
ϥ
ΎϬϔλ
ί
Ϯϫ
ϡϼϳ
ϞΑΎΑ
ήϬηϮ
ΑΪϨ
ΟήϴΑ
ΰϳήΒ
ΗϞΑ
ίϦϳ
ϭΰϗ
Ωΰϳ



QUESTIONS?