רגרסי ה לינארית, ניתוח שונות ו תכנון ניסויים סטטיסטיים הרצאה 1 רגרסיה פשוטה
Upload
liatfurmanCategory
view
297download
6
HEMATOLOGY
מיכל גולן מלכי' דר
ש לילי ואדמונד ספרא"ח לילדים ע"בי

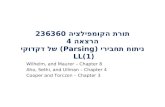
Thrombocytopoiesis
PLURIPOTENT
STEM CELL
COMMITTED
PROGENITOR
CELL
RECOGNIZABLE
BONE MARROW
PRECURSOR CELL
MATURE
BLOOD
CELL
myeloblast
monoblast
pronormoblast red cell
neutrophil
monocyte
basophil
platelet
CFU-Baso
CFU-Eos
CFU-GM
BFU-E/CFU-E
eosinophil
pre-T
pre-B
myeloid
progenitor
cell
lymphoid
lymphoblast
lymphoblast
T-cell
B-cell& plasma cell
MIXED
PROGENITOR
CELL
CFU-Meg megakaryocyte
pluripotent
stem cell

Blood
• Red Blood Cells (RBCs)
• White Blood Cells (WBCs)
• Platelets
• Plasma
• RBCs, WBCs, and Platelets Produced in Bone Marrow
• Approximately 5L of blood in adult

כדוריות אדומות

Red Blood Cells
• Carry Oxygen to Tissues
• Biconcave Disk Containing Hemoglobin
• Life Span of 120 days
• 4.4-5.9 x 1012
RBCs/L (M)
• 3.8-5.2 x 1012
RBCs/L (F)

Hemoglobin
• Oxygen Carrying Molecule
• Tetramer of 2 alpha chains and two “beta” chains (2 2) attached to Heme pocket
• Heme comprised of protoporphyrin ring and iron
• 13-18 g/dl (M)
• 12-16 g/dl (F)

Anemia
• Reduction in Oxygen Carrying Capacity of Blood
• Not enough production by Bone Marrow
• Too much peripheral destruction (hemolytic anemia)
– Reticulocyte count (0.8- 2.5%)

Reticulocyte

Rule of Thumb
Lower limit of normal for Hgb:
• 11 + 0.1*(Age in Years)
• Examples– 3 y.o. boy with a Hgb of 11.4 g/dL is normal
– 6 y.o. girl with a Hgb of 11.4 g/dL is abnormal

Rule of Thumb
Lower limit of normal for MCV:
• 70 + (Age in Years)
• Examples– 3 y.o. boy with an MCV of 74.2 is normal
– 6 y.o. girl with an MCV of 74.2 is abnormal

Classification of Anemia
• Mechanism
– Decreased production
– Hemolysis
– Blood loss
• Red blood cell size
– Too big (macrocytic)
– Too small (microcytic)
– Just right (normocytic)

MCV (Mean Cell Volume)
• 80- 100 fl
• Microcytic Anemia
• Normocytic Anemia
• Macrocytic Anemia

Hypoproliferative Anemia
• Microcytic
– iron deficiency anemia
– thalassemia
– sideroblastic anemia
– anemia of chronic disease
• Macrocytic
– Megaloblastic anemia
– reticulocytosis

Hemolytic Anemia
• Hemoglobinopathy (e.g. sickle cell)
• Membrane Abnormality (e.g. hereditary spherocyosis)
• Enzyme Defect (e.g. G6PD deficiency)
• Autoimmune hemolytic anemia
• Trauma (e.g. DIC, TTP)
• Infection (e.g. malaria)

Anemia
• Easy fatigability
• Dyspnea on exertion
• Faintness/ Vertigo
• Pallor
• Rapidly bounding pulse
• Dependent edema
• Systolic murmurs

Iron Deficiency Anemia
• Iron absorbed in GI tract, transported by transferrin to BM
• Iron absorbed by pinocytosis by RBC precursors
• After 120 days, RBC phagocytosed in spleen
– iron is reused
– hemoglobin converted to bilirubin

Iron Deficiency
• Increased Need
– Early childhood and adolescence (growth spurts)
– Pregnancy (extra 3.8 mg/day over baseline)
– Lactation
• Poor Intake/Absorption
– Milk baby
– Achlorhydria
– Inflammatory bowel disease

Iron Deficiency
• Menstruating women
• GI bleeding (most common pathologic cause)
• Tissue loss
• Urinary Loss
• Iatrogenic
• IRON DEFICIENCY IN A MALE ALWAYS NEEDS TO BE WORKED UP!!!

Iron Deficiency Anemia
• Hypochromic microcytic anemia
• low iron, high transferrin, low ferritin
• small ragged RBC precursors
• lack of stainable iron

Iron Deficiency Anemia

Anemia of chronic disease
• Impaired Fe utilization
– low Fe, low transferrin, high ferritin
• Increased iron stores

Megaloblastic Anemia
• B12 binds with intrinsic factor, absorbed in terminal ileum
– Schilling test
– 7-12 year supply
• Folate is not stored in body

Megaloblastic Anemia
• Macrocytic anemia with hypersegmented neutrophils
• Neurologic symptoms (dorsal columns)
• Nuclear/cytoplasmic asynchrony in BM
• Ineffective erythropoiesis
– High indirect bilirubin
– Very high LDH

Megaloblastic Anemia

Hemolytic Anemia
• Hemoglobinopathy (e.g. sickle cell)
• Membrane Abnormality (e.g. hereditary spherocyosis)
• Enzyme Defect (e.g. G6PD deficiency)
• Autoimmune hemolytic anemia
• Trauma (e.g. DIC, TTP)
• Infection (e.g. malaria)

Laboratory Evidence of Hemolysis
• Increased bilirubin
• low serum haptoglobin
• Hemoglobinemia/ Hemoglobinuria
• Hemosiderinuria
• Increased LDH
•Increased reticulocyte count

Hereditary Spherocytosis
• Defect of spectrin-Protein 4.1 interaction or in ankyrin
– decreased deformability
– sluggish transversing of splenic cords
• Clinical triad of anemia, splenomegaly, and jaundice
• Spherocytes on smear
• Osmotic fragility test

Hereditary Speherocytosis

Enzyme Deficiencies
• G6PD
• Pyruvate Kinase

Autoimmune Hemolytic Anemia
• Antibody attaching to RBCs
– Direct or indirect Coombs test
• May be associated with thrombocytopenia (Evan’s syndrome)
• Idiopathic, drugs, infection
• Treatment
– treat underlying cause
– steroids

Autoimmune Hemolytic Anemia

Sickle Cell Anemia
• Autosomal recessive -hemoglobinopathy
– Symptomatic at 6 months
• Irreversible sickling upon deoxygenation
– pain crises
– infarcts of spleen (asplenia), kidneys, brain
• Hemolytic vs. aplastic crisis (Parvovirus B19)

Sickle Cell Anemia

Thalassemia
• Imbalance of globin chain production
• - vs. -thalassemia
• anemia due to both decreased production and increased hemolysis in spleen
• - thalassemia has decreased/absent Hgb A, increased Hgb F, and increased Hgb A2
• Treatment- hypertransfusion with chelation, splenectomy, bone marrow transplantation

Hemolytic disease of the newborn
Rhאנטיגנים של מערכת
קימים גורמים המגבירים את הסיכון לדימום אימהי עוברי
(.דיקור מי שפיר וכדומה, CS, הפלה, הפרדות שליה)
דימום עוברי אימהי גורם לריגוש המערכת החיסונית
האימהית
בכמות רבה IGGבחשיפה חוזרת יווצרו -נוצרים נוגדנים

KELL(10%)אי התאמה של המערכת •
ויילוד Oאם -ABOהמוליזה בגל אי התאמה מסוג •A אוB .לרוב אינם גורמים להמוליזה משמעותית .(1%.)
נשים המצויות בסיכון ריגוש מערכת החיסון •עלייה , נמצאות במעקב הכולל עלייה בכייל נוגדנים
ירידה בהמוגלובין , הידרופס -US, בבילירובין.כורדוצנטזיס -העוברי

חיוורון , צהבת -ממצאים קליניים תלויים בחומרת המחלה•.והגדלה של כבד וטחול
:אתיולוגיה •
ישיר חיובי COOMBS -צהבת על רקע אימוני•
-צהבת שלא על רקע אימוני•
חסר , פגמים מבניים,זיהום תוך רחמי -המוליטית .אנזימתי
חסימת , היפותירואידיזם, המטומות -שאינה המוליטית .פגמים מטבוליים, מעיים

טיפול•
רובם ,ללא אנמיה בילוד, המחלה קלה 50%-ב•. יזדקקו לטיפול באור
הבילירובין יעלה כבר ביממה , אנמיה בינונית-25%•הגדלת כבד , רטיקולוציטים מרובים, ראשונה לחיים
לעיתים צורך בעירוי . בסיכון לאנצפלופטיה,וטחול. דם או החלפת דם
.עלולים להוולד מתים או עם הידרופס-25%•

RHמניעת מחלה המוליטית מאי התאמה במערכת •
המוזרק לאימהות בסיכון RhIGכולל חיסון סביל ב
.שעות מהלידה 72תוך
RHלאימהות 28הגישה המקובלת מתן בשבוע •
.חיובי RHומנה לאחר לידה אם הילוד , שלילי
, רובם יסתפקו בטיפול באור-ABOאי התאמה ב •
.בשעות הראשונות IVIG -ניתן להשתמש ב





טסיות



Platelet formation
megakaryocyte formation of
demarcation
membranes
platelets
(pro)platelets

PLATELET ACTIVATION
vWFRestingPlatelets Platelet
Adhesion

PLATELET ACTIVATION
TxA2, ADP, Serotonin, Fibrinogen, Thrombospondin
PlateletActivation
PlateletRelease

PLATELET ACTIVATION
PlateletPlug


אבחנה מבדלת
– הפרעה בתפקוד כלי הדם
הפרעה בטסיות–
– הפרעה בתפקוד חלבוני הקרישה
– , סמני דמם בעור -דימומים בריריות
וסת, פה, אף
– , דימום בפרקאיבר , בשריר
פנימי

HEMOSTATIC DEFECTS
BleedingProblem
PlateletDisorder
CoagulationAbnormality
Petechiae + -
BleedingSites
MucousMembrane
Deep Tissue
Time ofonset ofbleeding
Immediate Delayed
Ecchymoses/Hematomas
+ +



הפרעה בטסיות
Thrombocytopeniaמספר נמוך •
Platelet function disorderתפקוד לקוי•
von Willebrand factor ((vWFחסר או תפקוד לקוי של •

טרומבוציטופניה
העצם-בעיה בייצור של טסיות במח•
מולד –
נרכש–
תרופות•
הסננה של מח העצם •
אידיופטי•
של טסיות מכלי הדם" משיכה"•היפוטרמיה, הגדלת הטחול–

טרומבוציטופניה
הרס של טסיות•
• Immune– Idiopathic thrombocytopenic purpura (ITP)– Secondary
• Non immune– Microangiopathic hemolytic anemia
• Hemolytic uremic syndrome (HUS)• Thrombotic thrombocytopenic purpura (TTP)• Disseminated intravascular hemolysis (DIC)

ITP Idiopathic thrombocytopenic purpura
לרב לאחר מחלת חום וירלית•
שנים 2-4כ בגיל "בד•
הופעת שטפי דם קטנים על פני העור•
, במערכת השתן או העיכול, מהפה, דמם מהאף•
דימום וסת רב או מאורך
דימום –) <<<1%)לעיתים נדירות ביותר •
במערכת העצבים המרכזית

ITP- המשך
-חריף •
מהילדים 80%–
חולף תוך חצי שנה–
אך לעיתים אירועים חוזרים, לרב אירוע בודד–
-כרוני•
שנתיים-אחוז גבוה חולף לאחר שנה–
עלול להתפתח להפרעות אוטואימוניות נוספות–

- ITP טיפול
פרט במצבי דמם משמעותיים, ללא טיפול•
סטרואידים•
•IVIg
•Anti D
כריתת טחול•
•Immunosuppression
•Anti CD20

Approach to thrombocytopenia
• aplasia
• infiltration
• ineffective megakaryopoiesis
eg. MDS
• selective impairment of platelet
production
Causes of splenomegaly
• infection
• inflammation
• congestion
• maligancy
• red cell disorders
• storage diseases
• immune
auto-immune (ITP, SLE
drugs
infections
allo-immune
• non-immune
sepsis
DIC, TTP, HUS
hypertensive disorders of pregnancy
look for splenomegaly bone marrow investigation
review meds
look for underlying disorders
review meds
THROMBOCYTOPENIA
rule out pseudothrombocytopenia
SEQUESTRATION PRODUCTION DESTRUCTION

Laboratory Evaluation of Bleeding
CBC and smear Platelet count ThrombocytopeniaRBC and platelet morphology TTP, DIC, etc.
Coagulation Prothrombin time Extrinsic/common pathwaysPartial thromboplastin time Intrinsic/common pathwaysCoagulation factor assays Specific factor deficiencies50:50 mix Inhibitors (e.g., antibodies)Fibrinogen assay Decreased fibrinogenThrombin time Qualitative/quantitative
fibrinogen defectsFDPs or D-dimer Fibrinolysis (DIC)
Platelet function von Willebrand factor vWDBleeding time In vivo test (non-specific)Platelet function analyzer (PFA) Qualitative platelet disorders
and vWDPlatelet function tests Qualitative platelet disorders

הפרעות בתפקודי קרישה

XIIa
Coagulation cascade
IIa
Intrinsic system (surface contact)
XII
XI XIa
Tissue factor
IX IXa VIIa VII
VIII VIIIa
Extrinsic system (tissue damage)
X
V Va
II
Fibrinogen Fibrin
(Thrombin)IIa
Vitamin K dependant factors
Xa

בדיקת תפקודי קרישה
INR- international normalized ration PT(patient)/PT (control)[ISI]


PTT מאורך

A +Bהמופיליה
, זכרים 20/100,000חסר פקטורים מולד הכי שכיח •
Aמתוכם המופיליה 80%
X-linked recessiveתורשה •
(<1%)קשה , (5%-1%)בינוני , (30%-6%)חסר קל •
, אף, פה, תוך שרירי, פרקים, דימום לאחר הברית•
מערכת עצבים המרכזית, מערכת עיכול ושתן
הפקטור החסרמתן •
•DDAVP

Cהמופיליה
XIחסר פקטור •
יהודים ממוצא אשכנזי•
מתבטא בדמם קל בעיקר בעקבות ניתוח או •
טראומה
FFPלעיתים יש צורך במתן פקטור או •




Transfusion guidelines: non-bleeding
>50 x 109 No transfusionStable, <50 x 109 No transfusionStable, <20-30 x 109 TransfuseUnstable, 30-50 x109 Transfuse
– <1000g in first week – fluctuating vital signs in intensive care– previous significant bleed (IVH/pulmonary)– bruising, petechiae, oozing, blood in ET secretions– coagulopathy– high risk e.g. surgery, exchange Tx

Transfusion guidelines: bleeding
• Major active hemorrhage
– Pulmonary hemorrhage
– Macroscopic hematuria
– Rapidly evolving IVH
• Transfuse at count <100 x109/L

Disseminated Intravascular Coagulation (DIC)
• DIC is characterized by
– the systemic activation of the coagulation system followed by activation of fibrinolytic system
– high thrombin and plasmin generation
• DIC is not a disease itself, but is a manifestation of a serious underlying disorder.

Causes of DIC
• Infection - bacterial sepsis, viral infections
• Neoplasm - AML, adenocarcinoma
• Obstetrical disorders - retained dead fetus, abruption, etc
• Trauma/surgery - brain injury, crush, burns, etc.
• Others - acute hemolytic transfusion reaction, etc.

depletion of clotting factors
prolonged PT, PTT
increased FDP and D-dimer
thromboctyopenia (consumption)
LABORATORY
MANIFESTATIONS
microangiopathic hemolytic anemia
decreased fibrinogen
depletion of physiologic anticoagulants
tissue factor release
activation of intrinsic
pathway of coagulation
(systemic thrombin
generation)
generalized intravascular
fibrin deposition
underlying disorder
activation of
fibrinolytic system
(systemic plasmin
generation)
PATHOPHYSIOLOGIC
EVENTS
Pathophysiology of DIC
hemorrhage
thrombosis/infarction
CLINICAL
MANIFESTATIONS


Treatment of DIC
• treat the underlying disease
• replacement therapy
– cryoprecipitate
– FFP
– platelet concentrate
– packed red cells
• consider additional pharmacologic therapy
– controversial or investigational agents
• AT, APC, PC concentrate, heparin, antifibrinolytic agents.





נויטרופניה

• ירידה במספר הנויטרופילים –נויטרופניה
• 1500מתחת ל
• דורש אשפוז וטיפול –עם חום 500מתחת ל
אנטיביוטי