
© 2011 National Safety Council 17-1 SOFT-TISSUE INJURIES LESSON 17.
112
© 2011 National Safety Council 17-1 SOFT-TISSUE INJURIES LESSON 17
-
Upload
alvin-yearwood -
Category
Documents
-
view
215 -
download
0
Transcript of © 2011 National Safety Council 17-1 SOFT-TISSUE INJURIES LESSON 17.

© 2011 National Safety Council 17-1
SOFT-TISSUE INJURIESLESSON 17

© 2011 National Safety Council 17-2
Introduction
• Wounds common with trauma and burns
• In open wounds, skin is torn or cut and often bleeding
• Muscle and soft tissue may be injured
• Open wounds have risk of infection

© 2011 National Safety Council 17-3
Types of Soft-Tissue Injuries
Type and amount of bleeding depend on wound type, location, depth

© 2011 National Safety Council 17-4
Closed Wounds
• No break in skin
• Discoloration and swelling from internal bleeding
• Musculoskeletal injuries may be present
© 2011 National Safety Council 17-5
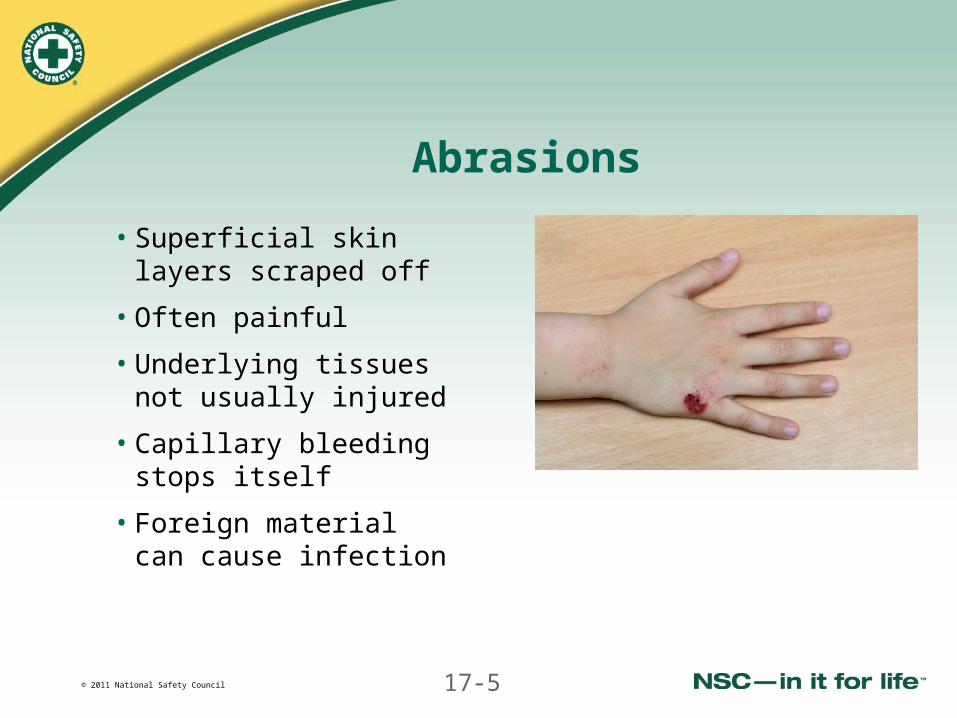
Abrasions
• Superficial skin layers scraped off
• Often painful
• Underlying tissues not usually injured
• Capillary bleeding stops itself
• Foreign material can cause infection

© 2011 National Safety Council 17-6
Lacerations
• May damage underlying tissue
• May cause severe bleeding
• Laceration through artery may be life-threatening
© 2011 National Safety Council 17-7
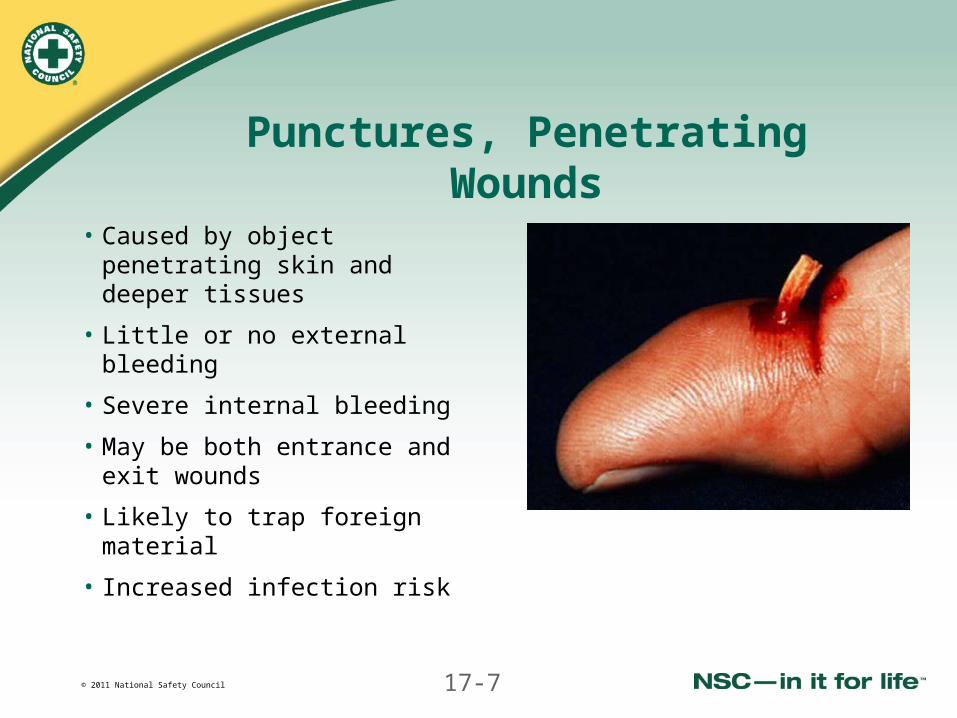
Punctures, Penetrating Wounds
• Caused by object penetrating skin and deeper tissues
• Little or no external bleeding
• Severe internal bleeding
• May be both entrance and exit wounds
• Likely to trap foreign material
• Increased infection risk
© 2011 National Safety Council 17-8
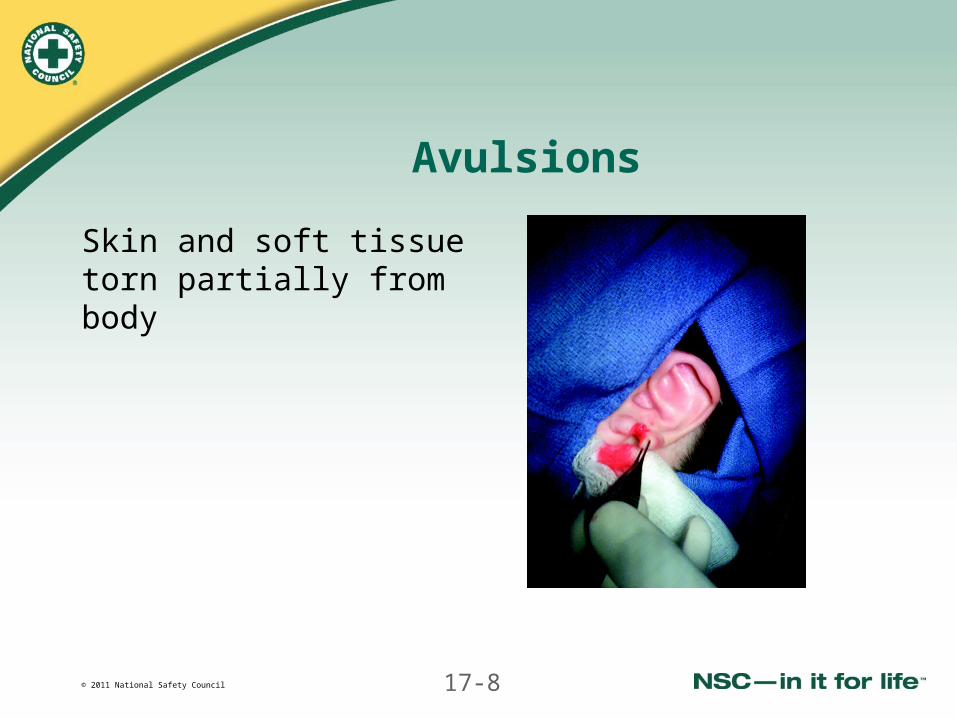
Avulsions
Skin and soft tissue torn partially from body

© 2011 National Safety Council 17-9
Traumatic Amputations
• Complete cutting or tearing off of all or part of extremity
• Part may be surgically reattached

© 2011 National Safety Council 17-10
Burns
Damage caused to skin and other tissue by heat, chemicals or electricity
© 2011 National Safety Council 17-11
General Principles of Wound Care
• Control serious bleeding after primary assessment
• With less serious bleeding, complete assessment and standard patient care first
© 2011 National Safety Council 17-12
Always Perform Standard Assessment
• Size up scene
• Complete primary assessment
• Take history
• Perform secondary assessment and physical examination as appropriate
• Complete reassessments

© 2011 National Safety Council 17-13
Always Perform Standard Patient Care
• Ensure EMS has been activated
• Use body substance isolation
• Maintain patient’s airway
• Provide artificial ventilation if needed
• Comfort, calm and reassure patient

© 2011 National Safety Council 17-14
Additional Care for Soft-Tissue Injuries
• Use needed BSI precautions
• Control bleeding
Cover wound with sterile gauze
Apply direct pressure

© 2011 National Safety Council 17-15
Additional Care for Soft-Tissue Injuries (continued)
• With minor wounds:
- Irrigate with large amounts of running water
- Irrigate wound to remove foreign matter from wound
- Pat area dry, apply sterile dressing, bandage
• Prevent contamination with dressing and bandage
• If stitches needed or patient’s tetanus vaccination not current, ensure patient receives medical attention
© 2011 National Safety Council 17-16
Wound Cleaning Alert!
• Do not use alcohol, hydrogen peroxide or iodine on wound
• Avoid breathing or blowing on wound
• Do not attempt to remove clothing stuck to wound; cut around clothing and leave in place
• Do not scrub wound

© 2011 National Safety Council 17-17
Purpose of Dressings
• Helps control bleeding
• Prevents infection
• Absorbs drainage
• Protects wound while healing
© 2011 National Safety Council 17-18
Types of Dressings
• Sterile gauze pads
• Roller gauze
• Non-stick gauze pads
• Adhesive strips
• Bulky
• Occlusive
• Improvised
© 2011 National Safety Council 17-19
Improvising Dressings
• If sterile dressing not available, use clean cloth
• Non-fluffy cloth less likely to stick
• Use clean towel, handkerchief, other material
• Avoid cotton balls or cotton cloth
• For bulky dressings, use sanitary pads, towels, baby diapers or many layers of gauze
© 2011 National Safety Council 17-20
Ring Dressing
• Don’t put direct pressure over:
- Skull fracture
- Fractured bone protruding from a wound
- Object impaled in wound
• Control bleeding with pressure around object or fracture
© 2011 National Safety Council 17-21
Guidelines for Using Dressings
• Wash hands and wear medical examination gloves
• Choose dressing larger than wound
• Do not touch part of dressing that will touch wound
• Lay dressing on wound, cover whole wound
© 2011 National Safety Council 17-22
Guidelines for Using Dressings(continued)
• If blood seeps through, do not remove dressing but add more on top
• Use direct pressure to control bleeding if needed
• Apply bandage to hold dressing in place

© 2011 National Safety Council 17-23
Purpose of Bandages
• Cover a dressing
• Keep dressing in place on wound
• Maintain pressure to control bleeding
• Support or immobilize musculoskeletal injury

© 2011 National Safety Council 17-24
Types of Bandages
• Adhesive compresses
• Adhesive tape rolls
• Tubular
• Elastic roller
• Self-adhering
• Gauze roller
• Triangular
• Improvised

© 2011 National Safety Council 17-25
Guidelines for Bandaging
• Should be clean, not necessarily sterile
• Apply bandage firmly but don’t cut off circulation
• Never encircle neck
• Don’t cover fingers or toes
• Check fingers or toes for color, warmth, sensation
© 2011 National Safety Council 17-26
Guidelines for Bandaging (continued)
• If reduced circulation, unwrap bandage and reapply
• Keep checking tightness of bandage
• Be sure bandage is secure
• Anchor first end and tie, tape, pin or clip ending section
• Use elastic roller bandage to make pressure bandage around a limb to control bleeding
© 2011 National Safety Council 17-27
Guidelines for Bandaging (continued)
• Elastic roller bandages support joints and prevent swelling
• Wrap from bottom of limb upward
• Bandage joint in position it will be kept
• Use wide bandage with evenly distributed pressure for extremities
© 2011 National Safety Council 17-28
Puncture Wounds

© 2011 National Safety Council 17-29
Puncture Wounds
• May involve unseen deeper injuries
• Check for exit wound
• Carry great risk of infection
• Internal bleeding may be significant

© 2011 National Safety Council 17-30
Care for Puncture Wounds
• Follow general principles of wound care
• Remove small objects and dirt but not large impaled objects
• Irrigate the wound with large amounts of water
• With small punctures, gently press wound edges
• Don’t put medication inside or over puncture wound
• Dry the area and apply dressing and bandage
• Seek medical attention if appropriate

© 2011 National Safety Council 17-31
Impaled Objects
• Object often seals wound or damaged blood vessels

© 2011 National Safety Council 17-32
Impaled Object (continued)
• Removing object could cause more injury and bleeding
• Leave it in place and dress wound around it
• Control bleeding by applying direct pressure at sides of object

© 2011 National Safety Council 17-33
Impaled Object (continued)
• Dress wound around object
• Use bulky dressings to stabilize object
• Support object while bandaging dressings in place
• Seek medical attention

© 2011 National Safety Council 17-34
Avulsion
• With skin flap, try to move skin or tissue into normal position (unless contaminated)
• Control bleeding
• Provide wound care
• If avulsed body part completely separated – care for it like an amputation

© 2011 National Safety Council 17-35
Amputation
Control bleeding and care for wound first, then recover and care for amputated part

© 2011 National Safety Council 17-36
Care for Amputated Part
• Wrap severed part in dry sterile dressing or clean cloth; do not wash
• Place part in plastic bag and seal
• Place sealed bag in another bag or container with ice and water part should not touch water or ice directly or be surrounded by ice
• Do not let part become saturated with water
• Give part to responding EMS

© 2011 National Safety Council 17-37
Animal Bites

© 2011 National Safety Council 17-38
Seriousness of Animal Bites
• Bleeding and tissue damage can be severe
• Increased risk of infection
• All bites carry rabies risk

© 2011 National Safety Council 17-39
Care of Animal Bites
• Follow general principles of wound care
• Clean with large amounts of water with or without soap (except when bleeding severely)
• Control bleeding
• Dress and bandage

© 2011 National Safety Council 17-40
Care of Animal Bites (continued)
• Ensure patient sees health care provider as soon as possible
• Do not try to catch animal but note its appearance
• Report bite to animal control or law enforcement
© 2011 National Safety Council 17-41
Chest Injuries

© 2011 National Safety Council 17-42
Care for Impaled Object in Chest
• Follow general principles of wound care
• Keep patient still, seated or lying down
• Do not remove object unless it interferes with chest compressions when CPR is needed
© 2011 National Safety Council 17-43
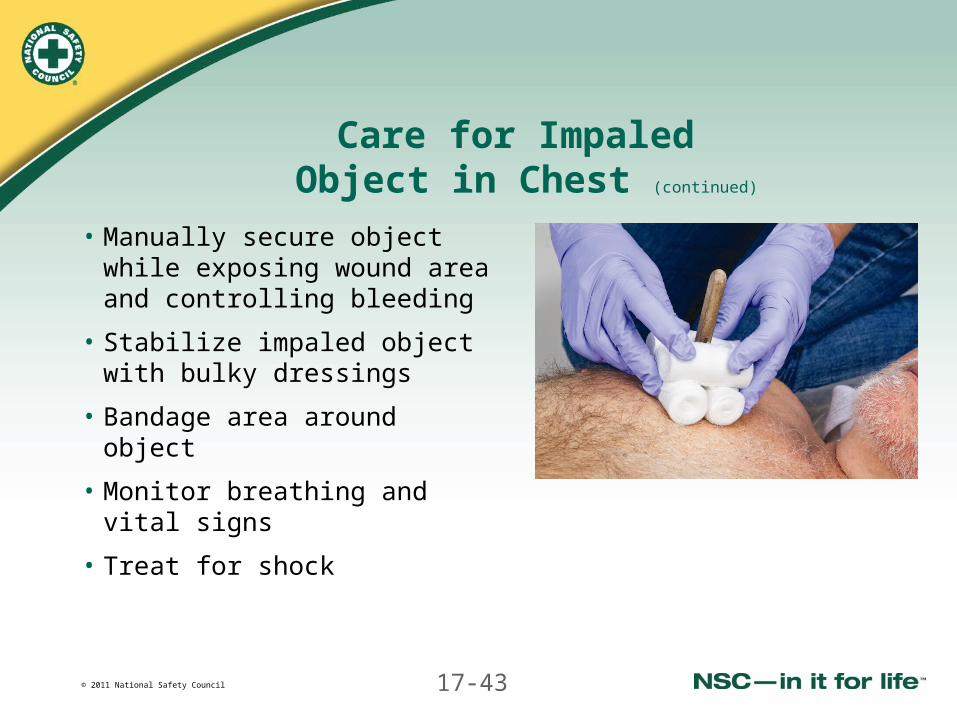
Care for Impaled Object in Chest (continued)
• Manually secure object while exposing wound area and controlling bleeding
• Stabilize impaled object with bulky dressings
• Bandage area around object
• Monitor breathing and vital signs
• Treat for shock

© 2011 National Safety Council 17-44
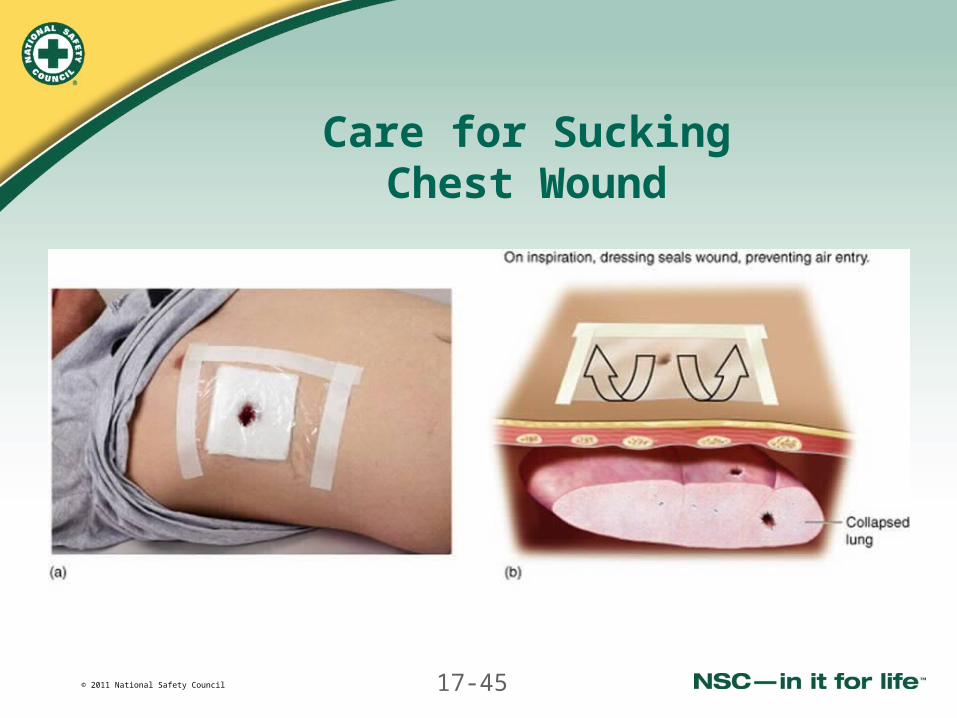
Sucking Chest Wound
• Open wound in chest caused by penetrating injury
• Wound lets air move in and out of chest during breathing
• Can be life-threatening
• Use special dressing to allow air to escape through the wound but prevent air from being sucked in
© 2011 National Safety Council 17-45
Care for SuckingChest Wound

© 2011 National Safety Council 17-46
Closed Chest Injury
• Organ damage or internal bleeding can be serious
• Consider possibility of pneumothorax or hemothorax with any trauma to chest
© 2011 National Safety Council 17-47
Pneumothorax
• Air escapes from injured lung into thoracic cavity causing collapse of some or all of lung
• Results in respiratory distress

© 2011 National Safety Council 17-48
Hemothorax
• Blood from injury accumulates in thoracic cavity, compressing the lung
• Causes respiratory distress and possibly shock

© 2011 National Safety Council 17-49
Signs and Symptoms of Pneumothorax or Hemothorax
• Little or no external evidence of injury
• Signs and symptoms of shock
• Respiratory distress
© 2011 National Safety Council 17-50
Care for Chest Injuries
• Perform standard patient care
• Help responsive patient to position of easiest breathing
• Treat for respiratory distress
• Follow local protocol for oxygen
© 2011 National Safety Council 17-51
Abdominal Injuries

© 2011 National Safety Council 17-52
Open Abdominal Wound
• Usually injures internal organs (intestines, liver, kidneys or stomach)
• Large wound may cause evisceration
Abdominal organs protrude through wound
Serious emergency

© 2011 National Safety Council 17-53
Care for Open Abdominal Wounds
• Follow general principles of wound care
• Position patient on back
• Loosen tight clothing
• Cover wound and organs with thick moist dressing

© 2011 National Safety Council 17-54
Care for Open Abdominal Wounds (continued)
• Cover dressing with large, occlusive dressing
• Cover area with blanket or towel
• Monitor vital signs, and treat for shock

© 2011 National Safety Council 17-55
Genital Injuries

© 2011 National Safety Council 17-56
Genital Injuries
• Rare because of protected location
• Occur from blunt trauma, an impact or sexual abuse
• Provide privacy

© 2011 National Safety Council 17-57
Care for Genital Injuries
• Injured testicles – support with towel between legs
• Vaginal bleeding – have woman press sanitary pad or clean folded towel to area

© 2011 National Safety Council 17-58
Head and Face Injuries
© 2011 National Safety Council 17-59
Head and Face Injuries
• Consider possible neck or spinal injury
• Do not move patient’s head while giving emergency care

© 2011 National Safety Council 17-60
Scalp Wound
Before controlling bleeding, confirm no signs of skull fracture:
• Deformed area of skull
• A depressed or spongy area in skull
• Blood or fluid from ears or nose
• Eyelids swollen shut or bruising
• Raccoon eyes
• Battle’s sign
• Unequal pupils
• Object impaled in skull
© 2011 National Safety Council 17-61
Care for Scalp Wound
• With no signs of skull fracture:
- Apply dressing
- Use direct pressure to control bleeding
• Follow general principles of wound care
• Never wrap bandage around neck

© 2011 National Safety Council 17-62
Scalp Wound Without Suspected Skull Fracture
• Replace skin flaps and cover wound with sterile dressing
• Control bleeding with direct pressure
• Secure dressing with roller bandage or triangular bandage

© 2011 National Safety Council 17-63
Neck Injuries
• Bruising, swelling, difficulty speaking, airway obstruction may result
• Treat minor wounds like other wounds
• Significant open wounds are medical emergencies bleeding can be profuse

© 2011 National Safety Council 17-64
Care for Neck Injuries
• Follow general principles of wound care
• Control bleeding with direct pressure
• Place occlusive dressing over wound and tape on all sides
• Apply pressure on dressing to control bleeding
• When bleeding is controlled, apply pressure dressing over occlusive dressing
• Do not obstruct airway or compress other blood vessels in neck

© 2011 National Safety Council 17-65
Eye Injuries
• Serious because vision may be affected
• Avoid putting pressure on eyeball
• Movement of eye will worsen injury
• Keep unaffected eye covered

© 2011 National Safety Council 17-66
For a Blow to the Eye
• Follow general principles of wound care
• If eye is bleeding or leaking fluid, patient needs emergency medical care immediately
• Put cold pack over eye with a barrier, but do not put pressure on eye
• Do not try to remove a contact lens
• Cover both eyes

© 2011 National Safety Council 17-67
Care for a Large Object Embedded in the Eye
• Follow general principles of wound care
• Do not remove object
• Stabilize with dressings or bulky cloth (paper cup for large object)
• Cover both eyes
© 2011 National Safety Council 17-68
Dirt or Small Particle In Eye
• Do not let patient rub eyes• Wait to see if patient’s tears
flush out object• Gently pull upper eyelid out and
down over lower eyelid to catch particle on lashes
• If particle remains and is visible, try to brush it out
• If particle still remains or patient has any vision problems or pain, cover both eyes and seek medical care
© 2011 National Safety Council 17-69
For Chemical or Substance Splashed in Eye
• Follow general principles of wound care
• Have patient lie flat with head tilted to affected side
• Hold eyelid open with gloved hand
• Flush eye with running water or saline until additional EMS providers arrive use specialized solution if available
• Follow local protocol to consult PCC
© 2011 National Safety Council 17-70
Ear Injuries
• Bleeding or cerebrospinal fluid from ear is sign of serious head injury
• Do not use direct pressure to stop fluid coming out of ear
• Do not remove any foreign object
• If insect in ear, gently pour lukewarm water into ear to float it out

© 2011 National Safety Council 17-71
Care for External Ear Injuries
• Control bleeding with direct pressure
• Dress wound
© 2011 National Safety Council 17-72
Care for Internal Ear Injuries
• Follow general principles of wound care
• Help patient sit up
• Tilt affected ear lower than unaffected ear
• Cover ear with loose sterile dressing
• Don’t apply pressure or plug ear closed

© 2011 National Safety Council 17-73
Nose Injuries
• Nose trauma can cause heavy bleeding
• Bleeding from back of nose down throat needs immediate medical attention
• Allow blood to drain from mouth

© 2011 National Safety Council 17-74
Care for Nose Injuries
• Follow general principles of wound care
• Patient sits with head slightly forward with mouth open
Don’t remove objects from nose
Don’t tilt patient’s head backward
• Pinch nostrils just below bridge of nose for 10 minutes

© 2011 National Safety Council 17-75
Care for Nose Injuries (continued)
• Place cold compress on nose
• After 10 minutes release pressure slowly
• If bleeding continues, pinch nostrils for another 10 minutes
• Put unresponsive patient on side and pinch nostrils
• Don’t pack nostrils with dressing

© 2011 National Safety Council 17-76
Cheek Injuries
• Object impaled in cheek (possible airway obstruction)
- Remove it only if airway cannot be controlled
- Place dressing inside mouth between wound and teeth
- Place another dressing on outside of wound
- Apply pressure as needed
• Position unresponsive patient with head turned to side
© 2011 National Safety Council 17-77
Teeth and Mouth Injuries
• Control bleeding with direct pressure on dressing
• Priorities:
Ensure airway is open
Ensure blood drains from mouth

© 2011 National Safety Council 17-78
Bleeding in Mouth
• Have patient sit with head tilted forward to let blood drain out
• Wound penetrating lip:
- Put rolled dressing between lip and gum
- Second dressing against outside lip
• Bleeding tongue:
- Put dressing on wound and apply pressure
- Do not repeatedly rinse mouth or let patient swallow blood

© 2011 National Safety Council 17-79
Tooth Knocked Out
• Control bleeding with rolled gauze over socket
• Save tooth
May be reimplanted if patient sees dentist
Touch only tooth’s crown
Do not clean or scrub tooth
Place in container of milk or clean water
• Get patient and tooth to dentist

© 2011 National Safety Council 17-80
Burns
© 2011 National Safety Council 17-81
Burns
• Major cause of death and injury
• Caused by sun, heat, chemicals, electricity

© 2011 National Safety Council 17-82
Assessing a Heat Burn
• Perform the standard assessment
• Consider:
- Burn depth
- Burn size or extent
- Respiratory involvement
- Specific body areas burned
- Patient’s age and health status

© 2011 National Safety Council 17-83
Classification of Burns
• Superficial
• Partial-thickness
• Full-thickness
© 2011 National Safety Council 17-84
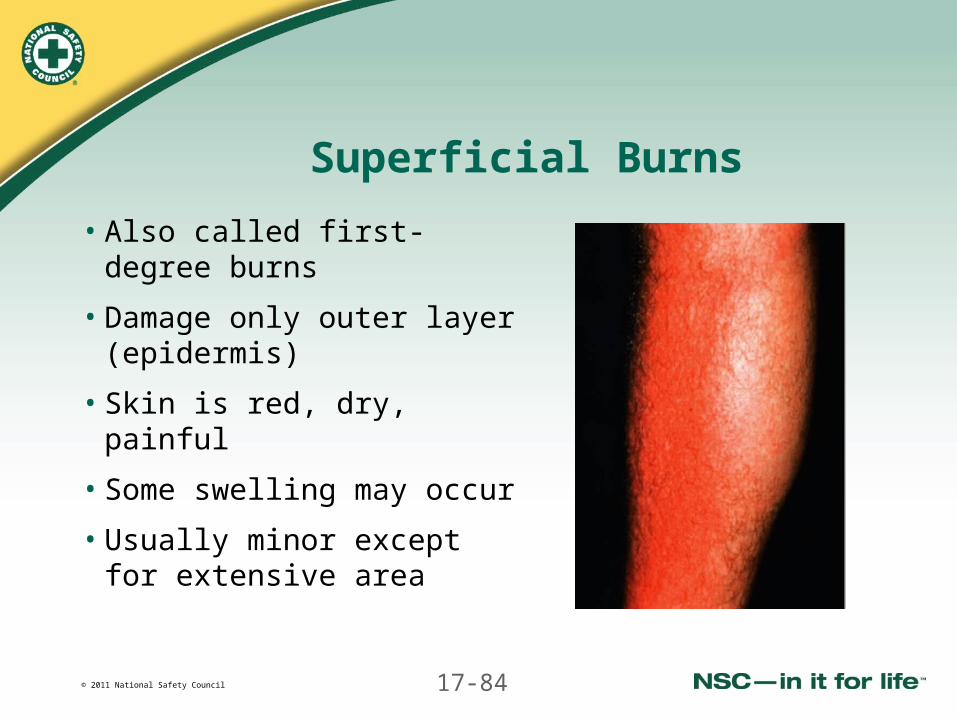
Superficial Burns
• Also called first-degree burns
• Damage only outer layer (epidermis)
• Skin is red, dry, painful
• Some swelling may occur
• Usually minor except for extensive area
© 2011 National Safety Council 17-85
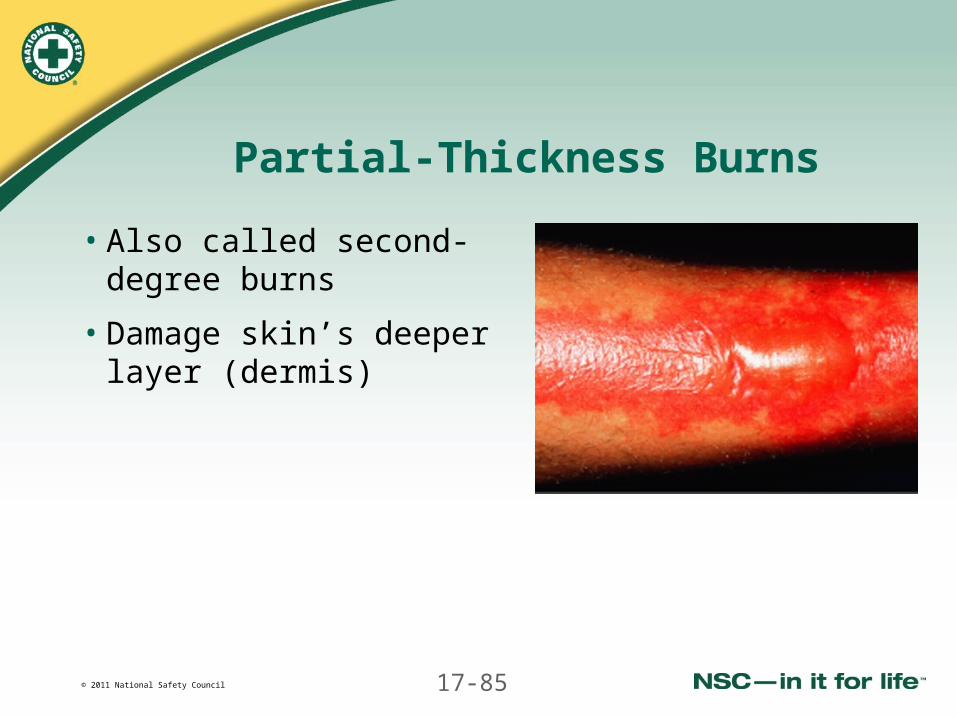
Partial-Thickness Burns
• Also called second-degree burns
• Damage skin’s deeper layer (dermis)

© 2011 National Safety Council 17-86
Partial-Thickness Burns (continued)
• Skin is red, mottled, very painful
• Blisters and weeping clear fluid may be present
• Often need medical attention

© 2011 National Safety Council 17-87
Full-Thickness Burns
• Also called third-degree burns
• Damage through subcutaneous layer and may include muscle and other tissues

© 2011 National Safety Council 17-88
Full-Thickness Burns (continued)
• Skin is charred and blackened or white, yellow, tab
• Burn feels leathery
• Pain is not present but likely in adjacent areas
• Medical emergency
© 2011 National Safety Council 17-89
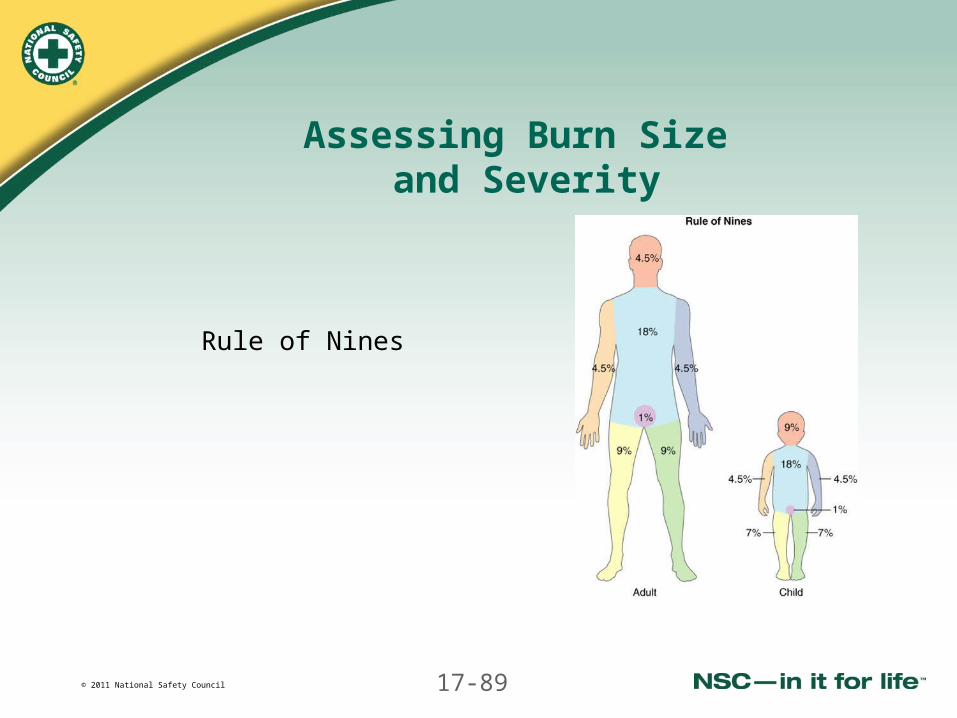
Assessing Burn Size and Severity
Rule of Nines

© 2011 National Safety Council 17-90
Emergency Burns by Size
• Burn size influences whether shock and complications develop
• Emergencies:
- Any full-thickness burn >50-cent piece
- Partial-thickness burn >10% of adult body (5% of child or older adult)
- Superficial burn over >50% of body
© 2011 National Safety Council 17-91
Assess Burn Location
• Partial- or full-thickness burns on face, genitals, hands or feet need immediate medical care
• Circumferential burns should receive immediate medical attention
• Burns around nose and mouth may affect breathing and are medical emergencies
© 2011 National Safety Council 17-92
Assess Burned Patient’sAge and Health
• Burns in those <5 or >55 are more serious
• Chronic health disorders make burns more serious

© 2011 National Safety Council 17-93
Principles of Care for Heat Burns
• Cool with cold water except for burn over 20% of body or 10% in child
- Cool as long patient feels pain
- Continually add fresh water
• Protect burned area from additional trauma and pathogens
• Provide supportive care

© 2011 National Safety Council 17-94
Emergency Care for Heat Burns
• Perform standard patient care
• Follow general principles of wound care
• Remove the heat source and smoldering clothing
• Cool burn with sterile or clean room-temperature water or cold running tap water (except large, full-thickness burns)

© 2011 National Safety Council 17-95
Emergency Care for Heat Burns (continued)
• Remove constricting clothing and jewelry
• If clothing sticks cut around it
• Treat for shock
• Cover burn with non-stick dressing use sheet over large area
• Follow local protocol for oxygen
• Don’t apply cream or ointment
• Don’t break blisters
© 2011 National Safety Council 17-96
Emergency Care for Heat Burns (continued)
• Don’t give patient anything to drink
• Monitor breathing and give BLS if needed
• For large burns in children:
- Keep environment warm
- With suspicious pattern of burn marks, consider possibility of child abuse

© 2011 National Safety Council 17-97
Smoke Inhalation
© 2011 National Safety Council 17-98
Smoke Inhalation
• Airway may swell and make breathing difficult
• Damage to alveoli may affect ability to receive oxygen
• Carbon monoxide poisoning may also have occurred

© 2011 National Safety Council 17-99
Signs and Symptoms of Smoke Inhalation
• Coughing, wheezing, hoarse voice
• Possible burned area
• Blackening on face or chest
• Difficulty breathing

© 2011 National Safety Council 17-100
Care for Smoke Inhalation
• Perform standard patient care
• Get patient to fresh air, or fresh air to patient
• Follow local protocol for oxygen
• Help position into easy breathing
• Put unresponsive patient in recovery position
• Monitor breathing
• Be ready to give BLS if needed

© 2011 National Safety Council 17-101
Chemical Burns
© 2011 National Safety Council 17-102
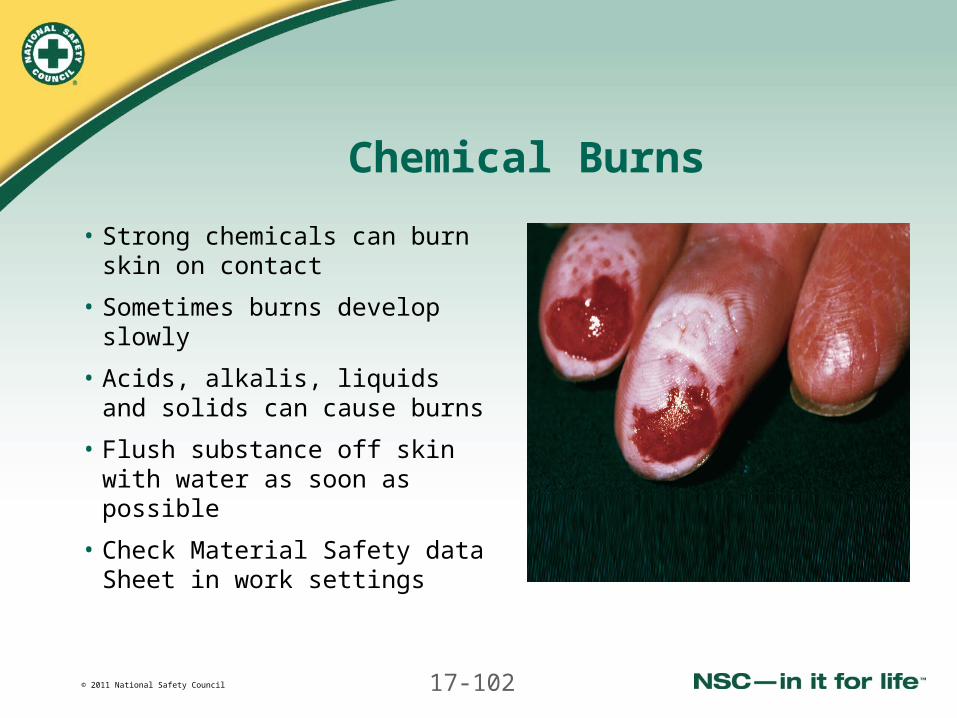
Chemical Burns
• Strong chemicals can burn skin on contact
• Sometimes burns develop slowly
• Acids, alkalis, liquids and solids can cause burns
• Flush substance off skin with water as soon as possible
• Check Material Safety data Sheet in work settings
© 2011 National Safety Council 17-103
Signs and Symptomsof Chemical Burns
• Pain or burning sensation
• Chemical on patient’s skin or clothing
• Spilled substance on or around unresponsive patient
• Smell of fumes
© 2011 National Safety Council 17-104
Emergency Care for Chemical Burns
• Perform standard patient care
• Send someone for the Material Safety Data Sheet
• Wear gloves and eye protection
• Move patient or ventilate area
• With dry chemicals, brush off skin

© 2011 National Safety Council 17-105
Emergency Care for Chemical Burns (continued)
• Flush area as soon as possible with copious running water until additional EMS personnel arrive
© 2011 National Safety Council 17-106
Emergency Care for Chemical Burns (continued)
• Don’t try to neutralize an acid with an alkaline or vice versa
• Remove clothing and jewelry while flushing
• With a splash injury, consider possibility of an eye burn
• With chemical in the eye, flush with running water until additional EMS personnel arrive

© 2011 National Safety Council 17-107
Electrical Burns and Shocks
© 2011 National Safety Council 17-108
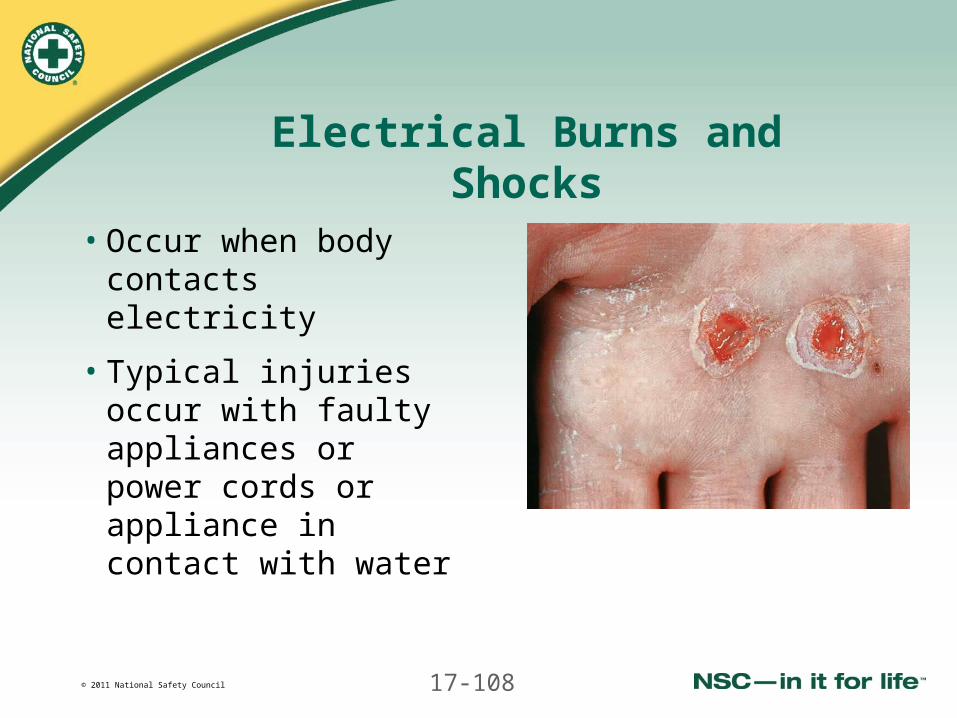
Electrical Burns and Shocks
• Occur when body contacts electricity
• Typical injuries occur with faulty appliances or power cords or appliance in contact with water

© 2011 National Safety Council 17-109
Injuries From Electricity
• External burns caused by heat of electricity
• Electrical injuries caused by electricity flowing inside body
• High-voltage electricity in body can cause heart rhythm irregularities that threaten circulation or cause heart to stop
• Patient may be in cardiac arrest on your arrival
© 2011 National Safety Council 17-110
Signs and Symptoms ofElectrical Injury
• Source of electricity nearby
• External entrance and exit wounds
• Unresponsiveness, seizures, changing levels of responsiveness
• Breathing abnormalities
• Weak or irregular pulse
• Can cause unseen severe internal injuries

© 2011 National Safety Council 17-111
Emergency Care for Electrical Burns
• Perform standard patient care
• Don’t touch patient until area is safe
• Stop burning and cool area
• Remove clothing and jewelry
• Cover burn with a sterile dressing
• Treat for shock
• Maintain normal body temperature
© 2011 National Safety Council 17-112
Emergency Care for Electrical Burns (continued)
• Keep unresponsive patient in recovery position
• Monitor breathing and vital signs
• Assume patient with lightning strike or high-voltage shock has spinal injury stabilize head and neck
• Care for shock and give BLS as needed


















