neuroradiology.rad.jhmi.edu · 2006-11-21 · Created Date: 11/21/2006 4:01:44 PM
9
Suprahyoid Spacesof the Head and Neck DavidM. Yousem If,/HEN ONE refers to the deep spaces of the Y Y neck. one includes all of the tissue outside the aerodigestivesystem mucosal and submucosal structures.The major lesions of the aerodigestive mucosal space(AMS) are surface epithelium neo- plasms. Squamous cell carcinomas (SQCCA) ac- count for most AMS neoplasms, and in conceft with minor salivary gland neoplasms and lym- phoma of Waldeyer's ring, they comprise over 957o of the neoplasms of the AMS. Thus, there is a reasonably limited differential diagnosisfor masses of the AMS. In contrast, the variety of lesions found in the deep spaces of the head and neck is astounding, and one is required to include spread of AMS lesionsto the deep spaces with one's differen- tial diagnoses. The classification ofregions ofthe deepspaces is not wholly arbitrary, yet engenderssome contro- versy amongst head and neck radiologists. For the radiologist who is not reading head and neck cases on a daily basis, the model derived from the works of Harnsberger, Osborne, and Smokerl-4seryesas the most practical approach. This model divides the nonmucosalspaces ofthe neck into regions defined by layers of the deep cervical fascia. The deep cervical fascia has superficial, middle, and deep layers, and these layers, in effect, form the bound- aries for different spaces of the head and neck. One separates the neck into the suprahyoid and infrahyoid compartments becauseof the termina- tion of some of the spaces at the hyoid level. In the suprahyoid region, the spaces of the neck include the masticatorspace, the prestyloid parapharyngeal space(PPS),the post-styloid parapharyngeal space or carotid space, the parotid space, the retropharyn- geal space, and the perivertebral space. In the infrahyoid region, the visceral space (encompass- ing the trachea,esophagus, thyroid and parathyroid glands) comes into play, whereas the masticator space, the PPS, and the parotid space are no longer present.The carotid space,reffopharyngeal space, and the perivertebral space spanthe suprahyoidand infrahyoid compartments. Before analyzing these spaces,it is helpful to understand how to localize a lesion to a particular space. Central to the suprahyoid spaces is the prestyloid parapharyngeal space, which is rela- tively unique among the spaces because its major component is fat. It is also the most mobile of the spacesof the head and neck becauseit is incom- pletely ensheathed by the deep cervical fascia. Most head and neck radiologists use the displace- ment of the PPS to help decide in which space a lesion resides.5,6 Thus if the PPS fat is pushed posteromedially by a mass, the assumptionis that the lesion arosein the masticator space. If the fat is pushedposterolaterally, an AMS massis suspected. If the mass is pushed anteriorly or anteromedially with predominantly an anterior direction, a carotid spacelesion is the likely culprit. (Distinguishing a pre-styloid process mass from a post-styloid ca- rotid space mass requires visualization of the styloid process by computed tomography (CT) and the styloid musculature by magnetic resonance imaging IMRII). If there is predominantly a medial displacement with some anterior component, a deep lobe parotid mass is the likely source. A retropharyngeal lesion will usually push the PPSfat anterolaterally. A perivertebral lesion may not af- fect the fat at all, but if it does,there will usually be an anterior componentof displacement. The second imporlant structure in the neck for localizing lesions is the longus colli musculature complex. When thesemusclesare displacedposte- riorly, the lesion is usually arising from the AMS or the retropharyngeal space. If displacedanteriorly, a perivertebralsource is indicated.The muscles them- selves are part of the perivertebral space so an intrinsic longus colli mass is within the periverte' bral space. At this point, an analysisof each space may help to gain confidence in diagnosing deep space le- sions. MASTICATOR SPACE The masticator space encloses the muscles of mastication (medial and lateral pterygoids, masse- ter, and temporalis), the neck and condyle of the mandible, and for simplicity's sake, the buccal From the Department of Radiology, Johns Hopkins Hospital, Baltimore, MD. Address reprint requests to David M. Yousem, MD, Depart- ment of Radiology, Johns Hopkins Hospital, 600 N. Wolfe St, Houck B-112, Baltimore, MD 21287. Copyright o 2000 by WB. SaundersCompany 003 7 - I 98X/00/3 s 0t - 000 8$ I 0.00/0 Seminarsin Roentgenology, Vol XXXV No 1 (January),2000: pp 63-71
Transcript of neuroradiology.rad.jhmi.edu · 2006-11-21 · Created Date: 11/21/2006 4:01:44 PM

Suprahyoid Spaces of the Head and Neck
David M. Yousem
If,/HEN ONE refers to the deep spaces of theY Y neck. one includes all of the tissue outside
the aerodigestive system mucosal and submucosalstructures. The major lesions of the aerodigestivemucosal space (AMS) are surface epithelium neo-plasms. Squamous cell carcinomas (SQCCA) ac-count for most AMS neoplasms, and in conceftwith minor salivary gland neoplasms and lym-phoma of Waldeyer's ring, they comprise over 957oof the neoplasms of the AMS. Thus, there is areasonably limited differential diagnosis for massesof the AMS. In contrast, the variety of lesionsfound in the deep spaces of the head and neck isastounding, and one is required to include spread ofAMS lesions to the deep spaces with one's differen-tial diagnoses.
The classification ofregions ofthe deep spaces isnot wholly arbitrary, yet engenders some contro-versy amongst head and neck radiologists. For theradiologist who is not reading head and neck caseson a daily basis, the model derived from the worksof Harnsberger, Osborne, and Smokerl-4 seryes asthe most practical approach. This model divides thenonmucosal spaces ofthe neck into regions definedby layers of the deep cervical fascia. The deepcervical fascia has superficial, middle, and deeplayers, and these layers, in effect, form the bound-aries for different spaces of the head and neck.
One separates the neck into the suprahyoid andinfrahyoid compartments because of the termina-tion of some of the spaces at the hyoid level. In thesuprahyoid region, the spaces of the neck includethe masticator space, the prestyloid parapharyngealspace (PPS), the post-styloid parapharyngeal spaceor carotid space, the parotid space, the retropharyn-geal space, and the perivertebral space. In theinfrahyoid region, the visceral space (encompass-ing the trachea, esophagus, thyroid and parathyroidglands) comes into play, whereas the masticatorspace, the PPS, and the parotid space are no longerpresent. The carotid space, reffopharyngeal space,and the perivertebral space span the suprahyoid andinfrahyoid compartments.
Before analyzing these spaces, it is helpful tounderstand how to localize a lesion to a particularspace. Central to the suprahyoid spaces is theprestyloid parapharyngeal space, which is rela-tively unique among the spaces because its major
component is fat. It is also the most mobile of thespaces of the head and neck because it is incom-pletely ensheathed by the deep cervical fascia.Most head and neck radiologists use the displace-ment of the PPS to help decide in which space alesion resides.5,6 Thus if the PPS fat is pushedposteromedially by a mass, the assumption is thatthe lesion arose in the masticator space. If the fat ispushed posterolaterally, an AMS mass is suspected.If the mass is pushed anteriorly or anteromediallywith predominantly an anterior direction, a carotidspace lesion is the likely culprit. (Distinguishing apre-styloid process mass from a post-styloid ca-rotid space mass requires visualization of thestyloid process by computed tomography (CT) andthe styloid musculature by magnetic resonanceimaging IMRII). If there is predominantly a medialdisplacement with some anterior component, adeep lobe parotid mass is the likely source. Aretropharyngeal lesion will usually push the PPS fatanterolaterally. A perivertebral lesion may not af-fect the fat at all, but if it does, there will usually bean anterior component of displacement.
The second imporlant structure in the neck forlocalizing lesions is the longus colli musculaturecomplex. When these muscles are displaced poste-riorly, the lesion is usually arising from the AMS orthe retropharyngeal space. If displaced anteriorly, aperivertebral source is indicated. The muscles them-selves are part of the perivertebral space so anintrinsic longus colli mass is within the periverte'bral space.
At this point, an analysis of each space may helpto gain confidence in diagnosing deep space le-sions.
MASTICATOR SPACE
The masticator space encloses the muscles ofmastication (medial and lateral pterygoids, masse-ter, and temporalis), the neck and condyle of themandible, and for simplicity's sake, the buccal
From the Department of Radiology, Johns Hopkins Hospital,Baltimore, MD.
Address reprint requests to David M. Yousem, MD, Depart-ment of Radiology, Johns Hopkins Hospital, 600 N. Wolfe St,Houck B-112, Baltimore, MD 21287.
Copyright o 2000 by WB. Saunders Company00 3 7 - I 9 8X/00/3 s 0 t - 000 8 $ I 0. 00/0
Seminars in Roentgenology, Vol XXXV No 1 (January),2000: pp 63-71

64
region. Many of these structures are innervated bybranches of the trigeminal nerve and are suppliedby external carotid artery branches. The proximityof the pterygoid muscles to the AMS and themandible to the retromolar trigone and floor ofmouth predisposes this space to infiltration by AMSSQCCA.
A lesion of the masticator space will displacePPS fat posteromedially and the longus muscula-ture will be unaffected or displaced posteriorly. Ifthe lesion is primarily located in the masseter ortemporalis muscle, the PPS fat may be unaffected.
The most common non-neoplastic lesions of themasticator space are odontogenic in origin.T-e Infil-tration of the muscles by infectious spread fromdental caries or as a complication of tooth extrac-tions is not infrequently seen. An abscess, a massdefined by peripheral contrast enhancement, maybe present on either side of the mandible or maxillaor may straddle the bone (Fig 1). The presence ofedematous linear stranding into the subcutaneoustissue or the PPS (if not the clinical symptoms) willsuggest the inflammatory nature of the lesion. Ofthe noninflammatory non-neoplastic odontogeniclesions, dentigerous cysts, aneurysmal bone cysts,and simple unicameral cysts may lead to evaluationof masticator space lesions.T The muscles are alsonot immune from pathology. One may see atrophy
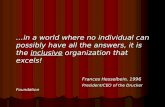
Fig 1. Masticator infection. This contrast-enhanced CTscan shows low density within the right masseter muscle(arrowheadl as well as enlargement of the right pterygoidmuscle. The parenchymal fat on the right side is displacedposteriorly and medially (arrowl. The CT scan also showsinfiltration of the subcutaneous tissue superficial to the rightmasseter muscle, suggestive of an inflammatory process.
DAVID M. YOUSEM
of the muscle after denervation injuries, or bilateralor unilateral enlargement of the muscles in cases ofbruxism or storage disease infiltrations.
Of benign neoplasms, hemangiomas (eg, venousvascular malformations) in the pediatric age groupand schwannomas and mandibular bony neoplasmsin the older population will predominate. Thehemangiomas may spread across spaces of the neck(transspatial) disrespecting the deep cervical fascia.The schwannomas are usually of mandibular nerveorigin and may be located anywhere from theinferior alveolar canal, the soft tissue of the masti-cator space, or the foramen ovale. Denervation ofthe muscle or abnormal T2-weighted intensity andgadolinium enhancement of the masticator musclesmay be seen in conjunction with the neurogenictumor. Of benign mandibular tumors, ameloblasto-mas are most common.
The most common malignancy to affect themasticator space is an AMS SQCCA. This is mostcommonly manifest as infiltration of the pterygoidmuscles from tonsillar or retromolar trigone can-cers leading to clinical complaints of trismus.roAlternatively, mandibular invasion may occur fromcancers of these sites. Metastases to the mandibleand direct secondary invasion by AMS malignan-cies are more common that primary malignanciesof the masticator space. The most common primarymalignant masticator space histologies are rhabdo-myosarcomas (Fig 2), lymphomas, and bony sarco-mas. Tumors may spread to or from the masticatorspace via perineural spread along the mandibularnerve."
PRESTYLOID PARAPHARYNGEAL SPACE
The PPS contains fat, vessels, nerves, and onoccasion, ectopic minor salivary gland tissue. The"styloid" of "prestyloid" refers to the styloidprocess and is a useful demarcation of the PPS fromthe carotid space. Although the styloid process iseasily identified on Cl the signal void associatedwith it on MRI may simulate a vessel. Thereforeone must identify the "styloid musculature," whichincludes the styloglossus, stylopharyngeus, andstylohyoid muscles on MRI to determine if a lesionis pre- or post-styloid. If the styloid musculature isdisplaced anteriorly, one should consider a carotidspace lesion.
It is rare to see a primary PPS lesion. Theinflammatory lesions of this space ale usuallyarising from theAMS, the tonsillar crypts, the deep

SUPRAHYOID SPACES
Fig 2. Rhabdomyosarcoma of the masticator space. Unen-hanced CT shows an infiltrative mass (asterisks) involving thepterygoid musculature, which demonstrates the characteris-tic displacement of the parapharyngeal fat in a posterior andmedial direction (arrowl. Compare right PPS fat with that onthe left {arrowhead}.
portion ofthe parotid gland, or the retropharyngealspace with secondary edema of the PPS. Branchialcleft cysts may occur in this space from either cleftI or II origin.
The most common benign neoplasm of the PPSis the pleomorphic adenoma, which takes originfrom the ectopic minor salivary gland tissue that ispresent in the PPS.5,12-15 This lesion is characterizedby high signal intensity on T2-weighted scans andhomogeneous enhancement (this distinguishes itfrom the branchial cleft cysts that will not enhanceor will only show rim enhancement). Rarely onemay find hemangiomas, schwannomas, and para-gangliomas in the PPS,12 though the latter two aremuch more frequent in the carotid space. Benignlymphadenopathy secondary to tonsillitis and phar-yngitis may also be seen in the PPS.
SQCCA of AMS origin is the most commonsource of malignancy in the PPS (Fig 3). Ininfiltrating the PPS, SQCCAs from the AMS willusually push the PPS fat posterolaterally. Othermucosal-based malignancies may also spread to thePPS. Malignant lymphadenopathy may reside inthe PPS. As for primary malignancies, these arederived from the ectopic minor salivary glands(adenoid cystic carcinoma being most commonfollowed by adenocarcinoma) or from soft-tissuesarcomas (synovial sarcoma, hemangiopericytoma,neurofibrosarcoma). Lymphomatous nodes may pre-sent in the PPS.
65
To unequivocally identify a lesion of the PPS asarising in that space, one would like to see the massentirely surrounded by PPS fat. This is rarelydemonstrated and often the PPS fat is eithercompletely obliterated or displaced anteriorly, simu-lating a parotid space or carotid space lesion. Thelatter can be excluded if one can determine that thelesion is found anterior to the styloid musculatureand/or styloid process.
CAROTID SPACE (POST-STYLOID
PARAPHARYNGEAL SPACE)
The carotid space is a colloquialism used for thecarotid sheath and adjacent structures. Some headand neck radiologists disdain the term "carotidspace" because the fascia around the sheath ap-pears to be incomplete above the angle of themandible and the vessels lie within the greaterparapharyngeal space. Nevertheless, because thepathology of the post-styloid parapharyngeal spaceis different than that of the pre-styloid compartmentit is useful to separate these regions. The carotidaftery jugular vein, sympathetic nervous systemplexus, jugular chain lymph nodes, and cranialnerves IX. X. XI. and XII are all included in thecontents of the suprahyoid carotid space. Lesionsofthe carotid sheath push the PPS fat in an anteriordirection, with or without a medial component. Thestyloid musculature or process will also be dis-placed anteriorly.
Second branchial cleft cysts are often associatedwith the carotid bifurcation and are the most
Fig 3. Tonsilparapharyngealcinoma (T).
carcinoma. Note the displacement of thefat (arrow) laterally by this tonsil car-

common congenital lesion of the carotid space.16Inflammatory mas$es of the carotid space are oftenassociated with pharyngitis and tonsillitis. Usuallythese affect the venous side, manifesting as jugularthrombosis or thrombophlebitis. Rarely one maysee carotid arterial narrowing, spasm, pseudoaneu-
rysm formation, or thrombosis secondary to anadenitis, pharyngitis, or retropharyngeal infec-1i6n.17,18 Carotid artery dissection may be seen as adirect result of penetrating or blunt trauma or inassociation with predisposing systemic disorders(eg, fibromuscular dysplasia, Marfan's syndrome,cystic medial necrosis, Ehler's Danlos syndrome).
The two most common benign neoplasms toaffect the carotid sheath structures are schwanno-mas and paragangliomas.l6'18,1e The former may bederived from cranial nerves IX to XII in thesuprahyoid compartment (ust X in the infrahyoidcompartment) or from the sympathetic nervoussystem plexus (SNSP). Clinical symptoms mayinclude difficulty swallowing, a sensory deficit inthe gag reflex, palatal paresis, vocal cord paralysis,atrophy of the sternocleidomastoid and trapeziusmusculature, or lingual deviation. A lesion of theSNSP (and a carotid dissection) may present as aHorner's syndrome. In general, vagus nerve lesionsdisplace the carotid artery and jugular vein apartand anteriorly.
Paragangliomas that affect the carotid space maybe classified as glomus jugulare, glomus vagale,and carotid body tumors. Glomus jugulare tumorsmay grow into the jugular veins from the jugularforamen, whereas the glomus vagale tumors oftenwill displace carotid sheath structures anteriorly.The carotid body tumors, arising in the crotch ofthe carotid bifurcation, tend to splay the internaland external carotid arteries apart, rather thananteriorly as the vagus schwannoma will (Fig 4).
Paragangliomas and schwannomas may appearsimilarly on CT and MRI scans and can best bedistinguished based on dynamic imaging character-istics. Paragangliomas have a characteristic rapiduptake of contrast and an early dip (simulatingjugular venous dynamic characteristics), followedby persistent enhancement, whereas the dynamiccurve of a schwannoma shows a slower sustaineduptake curve, no eaily dip, and persistent enhance-msn1.20-23 On angiography, paragangliomas aremarkedly hypervascular and can receive feedingvessels from numerous exterrral carotid aftery
DAVID M. YOUSEM
Fig 4. Carotid bodytumor. This axial CT scan image showsthe characteristic location of a carotid body tumor (asterisksldisplacing the internal (straight arrow) from external (curvedarrowl carotid artery. lt avidly enhances.
branches, most notably the ascending pharyngealbranches.
Primary malignant lesions are exceedingly un-common in the carotid sheath. More often, thecarotid sheath may be encased by aggressive hypo-pharyngeal or nasopharyngeal AMS carcinomas orby extracapsular extension of malignant lymphad-enopathy. If tumor involves less than 270" of thecarotid arlery's circumference, there is a very goodchance that the tumor can be peeled from thevessel, sparing the need for carotid sacrifice. Withover 270" circumferential involvement, the carotidwill have to be resected and temporary balloonocclusion studies will be reouired to assess the needfor rev as cular ization.za
PAROTID SPACE
Besides the parotid gland, branches of cranialneryes VII and V. lymph nodes, and blood vesselsare enclosed in the parotid space. Nonetheless, with

SUPRAHYOID SPACES
the exception of the occasional schwannoma, it isglandular masses that are most commonly evalu-ated in this space. Although lesions of the superfi-cial portion of the parotid gland will not affect thePPS fat, those that arise in or extend to the deepportion of the gland (defined by the plane of cranialnerve VII or the stylomandibular tunnel) willdisplace the PPS fat in an anteromedial direction(Fig 5). These lesions are always anterior to thestyloid muscles and process.
Inflammatory conditions of the parotid glandmay be diffuse and bilateral (mumps paroti-tis, Sjogren's syndrome, Mikulicz's diseases, radia-tion-induced sialadenitis), diffuse and unilateral(peripartal parotitis, Stensen's duct sialolithiasiswith sialadenitis, viral parotitis, post-traumatic par-otitis), focal and bilateral (lymphoepithelial lesionsassociated with HIV positivity, cat scratch fever),and focal and unilateral (abscess, sialocele, pseudo-cyst).25 With the exception of the chronic sialadeniti-des, most of the inflammatory conditions of theparotid gland are characterized by bright signal ona T2-weighted series. Edema in the subcutaneousfat or adjacent PPS fat may suggest an inflamma-tory cause.
When one finds a cyst in the parotid gland, onemust consider a broad differential diagnosis thatincludes a first branchial cleft cyst, a pseudocyst, asialocele, a retention cyst, a lymphoepithelial cyst(HIV), or a cystic neoplasm.2s'26 The patient'shistory and risk factors may help distinguish theseentities. Usually the cystic neoplasms (Warthin's
Fig 5. Superficial and deep lobe parotid mass. This infil-trated parotid adenocarcinoma (straight arrow) affects thesuperficial and deep portion of the gland. The displacement ofthe parapharyngeal fat is both medial and anterior in direction{curved arrow).
o l
tumors and pleomorphic adenomas for the mostpart) have a solid, enhancing nodule associatedwith them.
Pleomorphic adenomas, a.k.a. benign mixed tu-mors, are the most common parotid neoplasm,account for over 707o of all parotid neoplasms andover 857o of all benign parotid tumors. Theircharacteristic high intensity on T2-weighted scanssuggest their diagnosis, often prompting the needfor contrast-enhanced studies to confirm they arenot cysts. A recent publication has found that theyhave delayed and sometimes heterogeneous en-hancement pattern on CT,27 but on enhanced MRIthey appear to take up the contrast agent promptlyand homogeneously (unless they have a cystic orfatty component).28,2e Whether assessing a deep orsuperficial parotid mass, pleomorphic adenoma isthe most common tumor.
Other benign parotid neoplasms include theWarthin's tumor. This is most often seen in elderlymen in the tail of the parotid and is usually ofheterogeneous T2-weighted intensity. It is the tu-mor most likely to be bilateral and multiple.3oOncocytomas, monomo{phic adenomas, and myo-epitheliomas are other benign parotid-based masses.Hemangiomas may infiltrate the parotid gland aadlipomas may occur within or outside the gland inthe parotid space. Schwannomas, as mentionedbefore, may arise from the facial nerve or theauriculotemporal branch of the mandibular nerve.
Malignant parotid masses are usually due tomucoepidermoid carcinoma, adenoid cystic carci-noma, adenocarcinoma, or acinic cell carcinoma, inthat order.31,32 The malignancies are usually interme-diate in signal intensity on T2-weighted scans,especially if hypercellular and of higher grade.Their margins may be irregular and infiltrative,though margination has not been as reliable inevaluating parotid masses as elsewhere.
Because the parotid gland encapsulates later infetal development, it has lymphoid tissue within it.Therefore one may see lymphadenopathy fromsystemic diseases (eg, sarcoid, lymphoma, tubercu-losis, HIV), regional lymphatic spread of tumors(squamous cell carcinoma and melanomas of theskin), and primary parotid lymphomas affecting thegland.
RETROPHARYYNGEAL SPACE
The retropharyngeal space contains fat and lymphnodes in its suprahyoid compartment. This space

68
may extend inferiorly into the upper thorax or as apotential space (the danger space) to the dia-phragm. Situated as it is between the AMS and thelongus colli-longus capitis muscle complex, it ispredominantly affected by diseases of theAMS andwill displace the longus musculature posteriorly. Ifthe retropharyngeal pathology is large enough, itwill push the PPS fat anterolaterally, while it staysposterior to the styloid musculature. Owing to itslimited contents, the retropharyngeal space, like thePPS, is more commonly secondarily inflltrated thanaffected by intrinsic lesions.33,3a
Of benign conditions that affect the retropharyn-geal space, tortuous carotid arteries that coursemedially though incompetent layers of the deepcervical fascia may present as a retropharyngealpseudomass. Benign lymphadenopathy as a re-sponse to pharyngitis also account for many lesionsin this region. Pharyngitis may give rise to lymph-adenitis, which may suppurate and lead to retropha-
ryngeal inflammatory masses. Although most "ret-ropharyngeal abscesses" are actually necroticsuppurative lymph nodes (and usually seen adja-
DAVID M, YOUSEM
cent to the carotid arteries), occasionally a trueabscess in the more medial midline location willoccur (Fig 6). Altematively, the retropharyngeal fatmay appear "dirIy" without a ring-enhancing orwater density collection. This is usually due toedema in this space. No true collection is present-just inflamed edematous fat.
Lipomas may arise in the retropharyngeal space.Besides the occasional hemangioma, no other be-nign neoplasms populate this area.
AMS pharyngeal SQCCA is the most commonmalignancy to invade the retropharyngeal space.Nasopharyngeal carcinoma or its lymph nodesinfiltrate the RPS in 45Vo of cases at presentation.3sThe rate is slightly less for oropharyngeal andhypopharyngeal primary malignancies. Minor sali-vary gland malignancies of theAMS, rhabdomysar-comas (in children), and lymphomas may alsospread posteriorly. 10 Malignant lymphadenopathyfrom these primary tumors may present in the RPS.Parotid and thyroid malignancies also appear tohave a propensity for lymphatic spread to retropha-
ryngeal lymph nodes.36
Fig 6. Retropharyngeal abscess extending into thorax. (AlThis patient had perforation of the esophagus with extension ofa retropharyngeal abscess into the upper neck. This contlast-enhanced CT scan shows a low density retropharyngeal mass(arrowsl in front of the longest colli muscles (cl. Note the gas inthe abscess. (B) The collection (arrow) is seen posterior to theesophagus (e). (Cl Note that at the level of the manubrium theabscess collection (arrow) is still quite large.

SUPRAHYOID SPACES
PERIVERTEBRAL SPACE
The perivertebral space includes the vertebralcolumns, the paraspinal musculature, the posteriortriangles of the neck, and the neurovascular bundlesemanating from the spinal canal. As such it encom-passes all of the structures posterior to and includ-ing the longus colli-longus capitis muscular com-plex. When lesions of the perivertebral space are inproximity to the longus musculature, they willdisplace the muscles anteriorly, thereby distinguish-ing these masses from retropharyngeal masses orinvasive AMS masses.37
The variety of lesions that are located in this"grab-bag" space is quite wide because the lesionsmay be of bony, musculature, neurogenic, vascular,or lymphatic origin.
Of congenital lesions, lymphangiomas and ve-nous vascular malformations are commonly seen inthis region. The classic location of a cystic hy-groma is in the posterior triangle of the neck orextending to the axilla. The lesion is usuallymultiloculated and of various densities and intensi-ties owing to hemorrhage, lymph, or high proteincontent.
Developmental lesions of the spine includingvarious cysts, fibrous dysplasia, Paget's disease,renal osteodytrophy, degenerative spurs (especiallyanterior ones that push the longus musculatureanteriorly), diffuse idiopathic skeletal hyperostosis,anterior longitudinal ligament hypertrophy, andtraumatic injuries or hematomas associated withthe cervical spine are all considered lesions of the"perivertebral" space.
The infections that affect the perivertebral spaceare usually those that are associated with the spineas well. Discitis, osteomyelitis, epidural abscesses,paraspinal collections, and phlegmons may occurde novo, particularly in the population that abusesintravenous drugs, is exposed to tuberculosis, orundergoes spinal surgery. Staphylococcus, strepto-coccus, and mycobacteia are the usual pathogens.
Tumors of neurogenic origin are some of themore frequently seen benign neoplasms of theperivertebral space. Although some may emanatefrom the neural canal, thereby widening the fora-men, still others may derive from the branchesbeyond the foramen and present as true soft-tissuemasses in the neck. In this way, they may presentbehind the carotid sheath structures, simulatingvaqal schwannomas.
69
Other benign neoplasms in this region includethose of bony origin.16 The chordoma is the classiclesion of this space because it may be centered inthe upper cervical spine, will displace the longusmusculature anteriorly, and may appear quite ag-gressive. However, other benign bony lesions, suchas osteoblastomas, giant cell tumors (isolated orwith aneurysmal bone cysts), hemangiomas, andosteochondromas may populate this space.
Of malignancies, the bony varieties includeplasmacytomas, osteogenic sarcomas, Ewing's sar-coma, and lymphoma. Nonetheless, metastatic dis-ease to bone will be the most common malignantlesion of the perivertebral space.37 In the softtissues of the space, one may find lymphoma and avariety of sarcomas (neurofibrosarcoma, hemangio-pericytoma, rhabdomyosarcoma, and synovial sar-coma) (Fig 7). Malignant lymphadenopathy in thespinal accessory chain, usually from an AMSSQCCA but, in the young adult population may befrom Hodgkin's and non-Hodgkin's lymphomas,will account for many lateral perivertebral masses.In the lower neck the adenopathy may representspread from lung, breast, or thyroid primary tumors.
TRANSSPATIAL AN D M U LTISPATIAL LESIONS
Obviously, from the discussion above, one notesthat certain lesions seem to ignore the fascial layersthat encompass the suprahyoid spaces ofthe neck.38These transspatial lesions include, first and fore-most, squamous cell carcinoma, which will spreadthrough fascial planes in a very aggressive manner.Other carcinomas and sarcomas may act similarly.Of benign masses, hemangiomas and lymphangio-mas seem to be particularly infiltrative. One infec-tious entity that favors crossing the fascial planes isnecrotizing fasciitis, a very aggressive disease thatcan cause sloughing of soft-tissue layers.3e
By multispatial, one refers to lesions that can befound in a variety of spaces concurrently. Theclassic multispatial process is lymphadenopathy,which can be found in retropharyngeal, carotid,perivertebral, PPS, and parotid spaces. Generalizedlymphadenopathy like that is usually ascribed tolymphoma, HIV or AIDS infection, mononucleo-sis, metastatic disease, or occasionally, mycobacte-rium infection. Schwannomas, neurofibromas, andhemangiomas may also be located in many spacesparticularly in such syndromes as neurofibromato-sis, Mafucci's syndrome, and Klippel Trenaunay

DAVID M. YOUSEM
Fig 7. Hemangiopericytoma in the perivertebral space. (A) This hemangiopericytoma (hl infiltrated the perispinal musculature aswell as extended in to the right neural foramina, seen to be enlarged on T1-weighted scan, (Bl A T2-weighted scan shows therelatively low signal intensity of the perispinal component of the hemangiopericytoma {h}.
Weber syndrome. Metastatic disease to bone mayaffect the mandible of the masticator space and thespine in the perivertebral space.
CONCLUSION
Although the previous discussion may seemsimplistic at fi.rst glance, the principles governingthe analysis of deep-space masses of the head andneck will serve to help localize the lesion and limit
the usually broad differential diagnoses given tomasses in this area. By observing the patterns ofdisplacement of the PPS fat, the styloid process ormusculature, and the longus musculature complex,one should be able to identify the space in which amass resides. Although there is some overlap in theentities that populate each space, there are certainfavored diagnoses for each region that should beconsidered first (Table 1).
Table 1. Leading Diagnoses by Space and Type
Congenital Inflammatory Benign NeoplasmMalignantNeoplasm
Mast icator
PPS
Fibrous dysplasia
Branchial cleft cyst
Odontogenicabscess
Schwannoma AMS SOCCA, sar-coma
AMS SOCCA,adenoid cysticcarctnoma
Mucoepidermoidcarcinoma
Lymphadenopathy
AMS SOCCA,Nodes
Metastases tobones, lymphnooes
Pharyngi t isspread Pleomorphic
aoenoma
Parot id Branchial c lef t cyst Sia ladeni t is , HIV Pleomorphiccvsrs aoenoma
Carot id space Branchial c lef t cyst Thrombophlebi t is Schwannoma,paragangi loma
Retropharyngeal Medial carot id Adeni t is , abscess Lipoma, heman-space deviat ion gioma
Perivertebralspace Lymphangioma Disci t is ,osteomy- Schwannoma,el i t is chordoma
Cranial nerve Vl l
schwannomaCarotid dissection,
pseuooaneurysm
Sarcomas

SUPRAHYOID SPACES 7 1
REFERENCES
1. Hamsberger HR, Mancuso AA, Muraki AS, et al: Theupper aerodigestive tract and neck: CT evaluation of recurrenttumors. Radiology 149:503-509, 1983
2. Hamsberger HR, Osbom AG: Differential diagnosis ofhead and neck lesions based on their space of origin. 1. Thesuprahyoid part of the neck. AJR Am J Roentgenol 751:147-t54, l99l
3. Smoker WR, Hamsberger HR: Differential diagnosis ofhead and neck lesions based on their space of origin. 2. Theinfrahyoid portion of the neck. AJR Am J Roentgenol 157:155-159,1991
4. Smoker WR: Normal anatomy of the infrahyoid neck: Anoverview. Semin Ultrasound CT MRI 12:192-203,1991
5. Babbel R[ Harnsberger HR: The parapharyngeal space:The key to unlocking the suprahyoid neck. Semin UltrasoundCTMRI 11:444-459.1990
6. Cross RR, Shapiro MD, Som PM: MRI of the parapharyn-geal space. Radiol Clin North Am27:353-378,1989
7. Chong VF, Fan YF: Pictorial review: Radiology of themasticator space. Clin Radiol 5 1 : 457 -465, 1996
8. Hardin C[ Hamsberger HR, Osbom AG, et al: Infectronand tumor in the masticator space: CT evaluation. Radiology157:413-417, 1985
9. Tryhus MR, Smoker WR, Harnsberger HR: The normaland diseased masticator space. Semin Ultrasound CT MRI17:4"16-485. l99O
10. Yousem DM, Chalian AA: Oral cavity and pharynx.Radiol Clin NorthAm 36:967-981, 1998
11. Laine FJ, Braun I4 Jensen ME, et al: Perineural tumorextension through the foramen ovale: Evaluation with MRimaging. Radiology I7 4:65-7 1, 1990
12. Hughes KVr, Olsen KD, McCaffrey TV: Parapharyngealspace neoplasms. Head Neck l7:124-730,1995
13. Som PM, Braun IF, Shapiro MD, et al: Tumors of theparapharyngeal space and upper neck: MR imaging charactens-tics. Radiology 1 64:823 -829, 1987
14. Som PM, Sacher M, StollmanAl, et al: Common tumorsofthe parapharyngeal space: Refined imaging diagnosis. Radiol-ogy 169:81-85, 1988
15. Yousem DM, Sack MJ, Scanlan KA: Biopsy of parapha-ryngeal space lesions. Radiolo gy 193:619-622, 1994
16. Parker GD, Harnsberger HR: Radiologic evaluation ofthe normal and diseased posterior cervical space. AJR Am JRoentgenol I57 :16l-165, 1991
17. Chong VR Fan YF: Pictorial review: Radiology of thecarotid space. Clin Radiol 5l:762-768,1996
18. Fruin ME, Smoker WR, Harnsberger HR: The carotidspace in the suprahyoid neck. Semin Ultrasound CT MRI11:504-519, 1990
19. Fruin ME, Smoker WR, Hamsberger HR: The carotidspace of the infrahyoid neck. Semin Ultrasound CT MRI12:224-24O,1997
20. Vogl TJ, Juergens M, Balzer JO, et al: Glomus tumors ofthe skull base: Combined use ofMR angiography and spin-echoimaging. Radiology 192:103-110, 1994
21. Vogl TJ, Balzer JO: Base of skull, nasopharynx, andparapharyngeal space. Neuroimaging Clin NorthAm 6:351 -37 8,1996
22. YoglTI, Mack MG, Juergens M, et al: Skull base tumors:
Gadodiamide injection----enhanced MR imaging-drop-out ef-fect in the early enhancement pattern of paragangliomas versus
different tumors. Radiology 188:339-346, 1993
23. Yousem DM: Dynamic MR imaging in the head and
neck: An idea whose time has come . . . and gone. Radiology
I 89:659-660, 1993 (editorial)
24. Yousem DM, Hatabu H, Hurst RW, et aI: Carotid arteryinvasion by head and neck masses: Prediction with MR imaging.Radiology 195:'7 15 -"7 20, 1995
25. Holliday RA, Cohen WA, Schinella RA, et al: Benignlymphoepithelial parotid cysts and hyperplastic cervical adenopa-thy in AIDS-risk patients: A new CT appearance. Radiology168:439-441, 1988
26. Som PM, Brandwein MS, Silvers A: Nodal inclusion
cysts of the parotid gland and parapharyngeal space: A discus-sion of lymphoepithelial, AlDS-related parotid, and branchial
cysts, cystic Warthin's tumors, and cysts in Sjogren's syndrome.Laryngoscope 105:1122-1128, 1995
2'7. Lev MH, Khanduja K, Morris PP, et al: Parotid pleomor-
phic adenoma: Delayed CT enhancement. AJNRAm J Neurora-dio l 19:1835-1839. 1998
28. Teresi LM, Lufkin RB, Wortham DG, et al: Parotid
masses: MR imaging. Radiology 163:4O5-4O9, 198129. Schlakman BN, Yousem DM: MR of intraparotid masses.
AJNR Am J Neuroradiol 14: 1173-1 180, 1993
30. Shugar JM, Som PM, Biller HF: Warthin's tumor, amultifocal disease. Ann Otol Rhinol Laryngol 91:246-249, 1982
31. Som PM, Shugar JM, Sacher M, et al: Benign andmalignant parotid pleomorphic adenomas: CT and MR studies. JComputAssist Tomogr 12:65-69, 1988
32. Som PM, Biller IIF: High-grade malignancies of theparotid gland: Identification with MR imaging. Radiologyr73:823-826, 1989
33. Davis WL, Hamsberger HR, Smoker WRK, et al: Retro-pharyngeal space: Evaluation of normal anatomy and diseaseswith CT and MR imaging. Radiology 174:59-64,1990
34. Davis WL, Smoker WR, Harnsberger HR: The normaland diseased retropharyngeal and prevertebral spaces. SeminUltrasound CT MRI I 1:520-533, 1990
35. Chong Vfl Fan YF, Khoo JB: Retropharyngeal lymphad-enopathy in nasopharyngeal carcinoma. Eur J Radiol 21:100-105, 1995
36. Mclaughlin MP, Mendenhall WM, Mancuso AA, et al:Retropharyngeal adenopatby as a predictor of outcome insquamous cell carcinoma of the head and neck. Head Neck17 :190 -198 ,1995
37. Davis WL, Hamsberger HR: CT and MRI of the normaland diseased perivertebral space. Neuroradiology 37:388-394,7995
38. Vogelzang P, Hamsberger HR, Smoker WR: Multispatialand transpatial diseases of the extracranial head and neck. SeminUltrasound CT MRI 12:274-287 , l99l
39. Becker M, Zbarcn P, Hermans R, et al: Necrotizingfasciitis of the head and neck: Role of CT in diagnosis andmanagement. Radiology 202:4'7 1-47 6, 199'7