β-1,3 Glucan as a Test for Central Venous Catheter Biofilm ...€¦ · β-1,3 Glucan as a Test for...
9
β-1,3 Glucan as a Test for Central Venous Catheter Biofilm Infection Author(s): Jeniel Nett, Leslie Lincoln, Karen Marchillo and David Andes Source: The Journal of Infectious Diseases, Vol. 195, No. 11 (Jun. 1, 2007), pp. 1705-1712 Published by: Oxford University Press Stable URL: http://www.jstor.org/stable/30086160 . Accessed: 28/01/2015 18:04 Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at . http://www.jstor.org/page/info/about/policies/terms.jsp . JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. . Oxford University Press is collaborating with JSTOR to digitize, preserve and extend access to The Journal of Infectious Diseases. http://www.jstor.org This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PM All use subject to JSTOR Terms and Conditions
Transcript of β-1,3 Glucan as a Test for Central Venous Catheter Biofilm ...€¦ · β-1,3 Glucan as a Test for...

β-1,3 Glucan as a Test for Central Venous Catheter Biofilm InfectionAuthor(s): Jeniel Nett, Leslie Lincoln, Karen Marchillo and David AndesSource: The Journal of Infectious Diseases, Vol. 195, No. 11 (Jun. 1, 2007), pp. 1705-1712Published by: Oxford University PressStable URL: http://www.jstor.org/stable/30086160 .
Accessed: 28/01/2015 18:04
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
Oxford University Press is collaborating with JSTOR to digitize, preserve and extend access to The Journal ofInfectious Diseases.
http://www.jstor.org
This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PMAll use subject to JSTOR Terms and Conditions

MAJOR ARTICLE
0-1,3 Glucan as a Test for Central Venous Catheter
Biofilm Infection
Jeniel Nett, Leslie Lincoln, Karen Marchillo, and David Andes
Departments of Medicine and of Medical Microbiology and Immunology, University of Wisconsin, Madison
Biofilms are microbial communities that are associated with solid surfaces such as intravascular catheters. Candida species are a major cause of medical device-associated infections. Twenty percent to 70% of all candidemias are associated with this biofilm process. Diagnosis and effective treatment of Candida device- associated infections requires removal of the involved device. The ability to identify a biofilm device infection before catheter removal may obviate removal of a substantial number of devices. Prior studies in our laboratory identified cell wall changes (specifically, increased fl-1,3 glucan) associated with biofilm, compared with plank- tonic C. albicans. Both in vitro and in vivo (catheter) biofilm models were used to determine whether biofilm cells secreted more f-1,3 glucan and whether these differences could be used to discern the presence of a Candida biofilm infection with 3 species (C. albicans, C. glabrata, and C. parapsilosis). A limulus lysate assay was used to quantify (-1,3 glucan in supernatants from planktonic or biofilm cultures and in the serum of rats with an intravascular catheter biofilm infection or disseminated candidiasis. fl-1,3 glucan was detected from both in vitro and in vivo models from each condition. However, the concentrations of #-1,3 glucan from the biofilm conditions were 4-10-fold greater in vitro (P<.001) and were 10-fold greater in vivo (P<.001), despite equal or fewer numbers of cells in the biofilm conditions. These results suggest the secreted polysac- charide fl-1,3 glucan may serve as a useful tool for the diagnosis of Candida biofilm and device-associated infections.
Vascular catheter infections are common and are as-
sociated with high mortality and morbidity [1-3].
Nearly 5 million vascular catheters are used annually in the United States, and it is estimated that 2%-12%
of these result in sepsis [4-7]. Among central venous
catheter (CVC)-related infections, those due to Can-
dida species are associated with an attributable mor-
tality approaching 40% [8-10]. C. albicans device in-
fections are difficult to treat and often require removal
of the device for cure. Current treatment guidelines recommend device removal for treatment of candide-
mia, although removal may be technically difficult and associated with significant risk [7].
The majority of hospital-acquired infections, includ-
ing C. albicans infections, are associated with biofilms
[11]. A biofilm is a sessile microbial community em- bedded in polymeric matrix, with organisms irrevers-
ibly attached to a substratum or to each other [ 11, 12]. The cells in this environment exhibit an altered phe- notype with respect to antimicrobial resistance [12-16]. Candida biofilms can be up to 1000-fold more resistant to conventional antifungal agents, making the infec- tions very difficult to control in the medical setting.
No laboratory methods exist to rapidly detect biofilm infections in vivo. Blood cultures require several days for incubation, are only positive in 50%-70% of pa- tients with disseminated candidiasis, and do not dif- ferentiate between biofilm and nonbiofilm infection. Both semiquantitative and quantitative catheter cul-
tures have been used for diagnosis of bloodstream in-
fections, with greater specificity for catheter infection
Received 30 October 2006; accepted 21 December 2006; electronically published 17 April 2007.
Potential conflicts of interest: none reported. Reprints or correspondence: Dr. David Andes, 600 Highland Ave., Rm. H4.572,
Madison, WI 53792 ([email protected]).
The Journal of Infectious Diseases 2007;195:1705-12 a 2007 by the Infectious Diseases Society of America. All rights reserved. 0022-1899/2007/19511-0020$15.00 DO: 10.1086/517522
3-1,3 Glucan Test for Biofilm Infection * JID 2007:195 (1 June) * 1705
This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PMAll use subject to JSTOR Terms and Conditions

than blood culture alone [17-19]. Both methods involve await-
ing culture results. However, quantitative cultures do not re-
quire removal of the catheter. To avoid having to remove a
catheter for diagnosis of infection, the differential time to pos-
itivity of catheter and peripheral blood cultures has also been
used [19]. This method utilizes the higher burden of organisms in a blood culture obtained from an infected catheter and mea-
sures the earlier time to positivity, compared with that of a
peripheral culture. Although this method could circumvent the
need for catheter removal to diagnose infection, 24-72 h may be spent awaiting culture results. The only Food and Drug
Administration-approved, non-culture-based test for diagnosis of invasive candidiasis is an assay for 3-1,3 glucan [20, 21].
Both in vitro and CVC in vivo C. albicans models have been
used to examine drug susceptibility and pathogenesis [12-16,
22]. Using these models, the current studies identified differ-
ences in carbohydrates surrounding biofilm cells. Findings sug-
gest a dramatic increase in secreted carbohydrates, including
3-1,3 glucan. We have demonstrated the ability to differentiate between biofilm and planktonic cells in vitro and in vivo using an assay for this material.
MATERIALS AND METHODS
Organisms and culture conditions. Four clinical Candida strains obtained from patients with bloodstream infection were
chosen for these investigations. C. albicans strains K1 and 98-
17, C. glabrata 5376, and C. parapsilosis 5986 were stored in
15% (vol/vol) glycerol stock at -800C. Before experiments, strains were maintained on yeast extract-peptone-dextrose me-
dium (YPD;1% yeast extract, 2% peptone, and 2% dextrose). Fresh colonies were used for inoculation of YPD or RPMI 1640 with morpholine propanesulfonic acid (MOPS), and cultures
were allowed to incubate for 16 h at 370C with orbital shaking at 250 rpm before inoculation.
In vitro biofilm formation. Flat, sterile medical-grade sil- icone disks were utilized as the biofilm substrate. Before in-
fection, the disks were coated with mouse serum and incubated at 370C for 30 min. C. albicans K1 was grown in YPD at 370C on an orbital shaker to late logarithmic phase. After the con-
ditioning period, 150 ,TL of culture (106 cells/mL) was inocu- lated on the disk and spread evenly. The disks were then in- cubated with 1 mL of RPMI/MOPS for 45 min at 370C. After
the adherence period, disks were rinsed in sterile water and
then placed in 10 mL of RPMI/MOPS and incubated at 370C
with gentle shaking for varying periods of time (detailed below). Planktonic culture conditions. C. albicans K1 was grown
overnight in YPD at 370C on an orbital shaker at 250 rpm and
used for inoculation of planktonic culture. Planktonic cultures were grown in 10 mL RPMI/MOPS in a glass flask at 370C on
an orbital shaker at 250 rpm until late logarithmic phase (106
cfu/mL).
In vitro glucan determination and microbiologic enumeration.
Supernatants from C. albicans in vitro biofilm cultures and
planktonic cultures were collected for determination of 0-1,3 glucan concentration. Viable cell number was used as a nor- malization factor for both the in vitro planktonic and biofilm
systems. Viable cell burdens were measured using plate counts to ensure the cultures contained a similar number of cells and were in a similar phase of growth. Both adherent and non- adherent cells were included in microbiologic enumeration of biofilm culture. Culture supernatants were collected from both the planktonic and biofilm systems at 4, 8, and 12 h. The cultures were centrifuged at 3000 g for 20 min, and the cell- free supernatant (confirmed by light microscopy) was removed and stored at -200C until glucan analysis. Biofilm formation was confirmed by visual inspection and by confocal microscopy. Glucan concentration was determined using a limulus lysate assay, the Glucatell (1,3)-3-D-Glucan Detection Reagent Kit
(Associates of Cape Cod), in accordance with the manufac-
turer's directions. The culture experiments were repeated on 2 occasions. Three glucan assay replicates were performed for each experiment per time point.
In vivo venous catheter biofilm model. A C. albicans CVC biofilm model was used for in vivo experiments as described elsewhere [22]. Briefly, animals were anesthetized, placed in
supine position, and prepped in a sterile fashion. A vertical incision was made in skin of the anterior neck just right of midline. The external jugular vein was identified and exposed with blunt surgical dissection, and a longitudinal incision was made in the vein wall. A sterile, heparinized (100 U/mL) poly- ethylene catheter (PE 100 [inner diameter, 0.76 mm; outer diameter, 1.52 mm]; Intramedic catalog no. 427430; Becton
Dickinson) was placed in the opening and advanced to a site above the right atrium (-2 cm). The catheter was secured with 3-0 silk ties. The proximal end of the catheter was then tunneled
subcutaneously and secured on the subscapular skin via a but- ton. The anterior neck site was closed with surgical staples (Ethicon Endo-Surgery), and the midscapular button was se- cured with a 2-0 Ti-Cron suture. Recovery of the animal after the catheter surgery was assessed according to a standard pro- tocol approved by the Veterans Administration Animal Com- mittee. After 24 h, 106 cells/mL of C. albicans strains K1 or 98-
17, C. glabrata 5376, or C. parapsilosis 5986, in late logarithmic phase and suspended in normal saline, were instilled in the catheter lumen for 4 h and then flushed with heparin. After a 12-, 24-, or 48-h incubation, blood samples were obtained from tail vein and catheter.
Tail-vein candidasis model. A tail-vein candidiasis model
was used to represent disseminated candidiasis in the absence of biofilm growth on an infected medical device [23, 24]. An- imals without catheters in place were infected by tail vein with 106 cells/mL of C. albicans strains K1 or 98-17, C. glabrata
1706 * JID 2007:195 (1 June) * Nett et al.
This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PMAll use subject to JSTOR Terms and Conditions

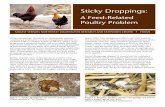
Figure 1. Confocal micrographs of an in vitro Candida albicans biofilm. C. albicans biofilms were grown on silicon disks and stained with FUN-1 and concanavalin A (ConA) fluorescent dyes. Metabolically active yeast cells are stained red by FUN-1, a fluorescent viability stain. ConA binds carbohydrates and results in green fluorescence of the cell walls of both yeast and hyphae. Extracellular green fluorescence is due to ConA binding to carbohydrate components of the matrix.
5376, or C. parapsilosis 5986, in late logarithmic phase and
suspended in normal saline. After 12, 24, or 48 h, serum sam-
ples were obtained for determination of 3-1,3 glucan content. To exclude the possibility of the catheter material alone causing an elevation of serum 0-1,3 glucan, several animals with cath- eters in place were infected by the tail-vein route. These animals had a nonbiofilm infection and a catheter in place.
In vivo glucan assay and microbiologic enumeration. Serum samples (1 mL) were frozen at -200C until analyzed for 0-1,3 glucan content using a limulus lysate assay, according
to the manufacturer's instructions (Fungitell (1,3)-f-D-Glucan Detection Reagent Kit; Associates of Cape Cod). Assays were
performed in triplicate. Kidneys were harvested and collected
at various time points (detailed above) from animals with CVC
infections and tail-vein infections for microbiologic viable bur-
den counts as an estimate of total-body organ burden [24]. Statistical analysis. Two biological replicates and 3 assay
replicates were performed at each time point for in vitro glucan
assay experiments. Three assay replicates were performed for
in vivo glucan determination. Analysis of variance and Stu-
/3-1,3 Glucan Test for Biofilm Infection - JID 2007:195 (1 June) - 1707
This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PMAll use subject to JSTOR Terms and Conditions

dent's t test were used to statistically compare glucan concen- trations. Viable burden counts from both in vitro and in vivo studies were performed in duplicate. Viable counts from plank- tonic and biofilm conditions were compared using a Student's t test to determine significance.
Biofilm scanning electron microscopy (SEM). SEM was used to image catheters of animals with CVC infections to confirm biofilm formation and assess the extent of biofilm on the catheter luminal surface [22]. Animals with CVC infections were killed at 12, 24, or 48 h, and catheters were collected for SEM. Catheters were harvested and transected perpendicular to catheter length. Segments were then placed in fixative (4% formaldehyde and 1% glutaraldehyde in PBS) for 20 h, washed for 5 min in PBS, and placed in 1% osmium tetroxide for 30 min. After a series alcohol washes, final drying was performed by critical point drying. Catheter segments were mounted on stubs and gold coated. Samples were imaged in a scanning electron microscope (JEOL JSM-6100) in the high-vacuum mode at 10 kV. The images were assembled using Adobe Pho-
toshop (version 7.0). Confocal microscopy. Confocal microscopy was used to
confirm in vitro Candida biofilm formation. Biofilms were
grown on silicone disks as described above. Disks were cut into small sections and placed in PBS with fluorescent dyes (the FUN-1 [50 /imol/L] component of the LIVE/DEAD yeast vi-
ability kit [Molecular Probes] and concanavalin A [ConA] con-
jugate [200 mmol/L; Alexa Fluor 488 conjugate]) and processed according to the manufacturer's instructions, as described else- where [22]. Imaging of FUN- 1-stained cells was accomplished by using a protocol with an excitation wavelength of 488 nm and an emission band at 617 nm for red. The ConA protocol included excitation and emission wavelengths of 490 and 528 nm, respectively. Biofilms were observed with a Nipkow disk- based confocal microscope (Axiovert 200; Zeiss) equipped with a mercury arc lamp. The objectives used included X20 and X40 differential interference contrast oil immersion objectives. Confocal images of green (ConA) and red (FUN-1) fluores- cence were conceived simultaneously using the Z-stack mode.
Images were processed for display by using Axiovision software (version 3.x; Zeiss).
RESULTS
In vitro biofilm confocal microscopy. We used confocal mi- croscopy to confirm and characterize the presence of biofilm on the silicone disks in our in vitro biofilm model (figure 1). We selected FUN-1 and ConA fluorescent dyes to stain yeast cells, hyphae, and matrix. At 24 h, yeast cells, hyphae, and matrix components were present on the silicone disk. Live, metabolically active yeast cells processed the FUN-1 viability stain, resulting in red fluorescence within intravacuolar struc- tures. Glucose and mannose residues of cell wall polysaccha-
rides were visualized as a green fluorescence due to ConA bind-
ing. The cell walls of both yeast and hyphae were visualized by this dye. The carbohydrate component of the matrix was also visualized by ConA dye and was seen as an extracellular green fluorescence. Because of colocalization of both fluorescent dyes, the metabolically active cells appeared yellow to orange during multichannel image capture.
In vitro biofilm glucan assay. We collected supernatants from the planktonic culture and the in vitro biofilm model described above to compare concentrations of /3-1,3 glucan. Glucan was detected in supernatants from both cultures and
temporally increased with rising cell numbers (figure 2). Using
microbiologic viable counts, we confirmed that cultures con-
tained the same number of viable cells. Although microbiologic
A
-J E
2 o
-,- O
7
6
5
4
3
2
Biofilm * Planktonic
2 4 6 8 10 12 14 16 18 20
Time (h)
B
E
r-
C!
250
200
150
100 -
50 i
0-
Biofilm Planktonic
4 8 12
Time (h)
Figure 2. In vitro biofilm and planktonic supernatant 0-1,3 glucan. Candida albicans biofilms were grown on medical-grade silicone disks. Supernatants were collected from planktonic and biofilm culture condi- tions, and p-1,3 glucan content (picograms per milliliter) was determined using limulus lysate assay (B). The black bars represent 0-1,3 glucan concentration from biofilm culture supernatant in picograms per milliliter, and the gray bars represent 0-1,3 glucan concentration from planktonic conditions. The viable burden of cells (colony-forming units per milliliter) from both conditions was determined by microbiologic enumeration (A). Error bars represent SDs.
1708 * JID 2007:195 (1 June) * Nett et al.
This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PMAll use subject to JSTOR Terms and Conditions

A. C. albicans K1 B. C. albicans 98-17 E. C. glabrata 5376
C. C. glabrata 5376 D. C. parapsilosis 5986
........ ........ ......
Figure 3. Scanning electron micrographs (SEMs) of in vivo Candida species biofilms. Catheter segments from the rat venous catheter model were prepared for SEM. Panels A-D show biofilm on the luminal surface of the catheter segments from C. albicans K1, C. albicans 98-17, C. glabrata 5376, and C. parapsilosis 5686 at x50 magnification. Panel E shows the C. glabrata biofilm at x1000 magnification.
viable counts demonstrated similar numbers of cells in each
culture, biofilm culture supernatants were found to contain
significantly higher concentrations of 0-1,3 glucan (P<.001). At each of the time points, the supernatant from the biofilm
system contained 2-10-fold more glucan. The difference was
most pronounced at the 8-h time point, when biofilm super- natant contained >150 pg/mL 0-1,3 glucan and the planktonic
supernatant content was <25 pg/mL (P<.001).
In vivo biofilm SEM. Our next experiments were intended
to determine whether the enhanced release of /3-1,3 glucan from
biofilm cells observed in vitro occurs in vivo as well. We used
our in vivo CVC model to mimic device-associated infection
involving formation of a biofilm. We utilized SEM to verify biofilm formation and extent on the infected CVCs. We cap- tured images of the luminal surface of multiple catheter seg- ments 24 h after inoculation (figure 3). C. albicans strains KI
01
A
6
5.
4.
3.
2
1-
0-
Biofilm Disseminated
12 h 24 h 48 h
-J E c3, CL
cm
co 03
")" e3.
300
250
200
150
100
50
0
B Biofilm catheter Biofilm peripheral Disseminated
12 h 48 h
Figure 4. Serum 0-1,3 glucan concentrations (picograms per milliliter) in Candida albicans biofilm and disseminated (nonbiofilm) infections. Central venous catheters were surgically implanted in rats and infected with C. albicans. The viable burden of cells (log,,0 colony-forming units/organ) from the kidneys of animals with disseminated and biofilm infections were determined at various time points to estimate systemic burden of infection (A). Serum samples were obtained at 12 and 48 h, and 0-1,3 glucan content was determined using a limulus lysate assay (B). Black vertical bars represent 0-1,3 glucan content in picograms per milliliter in serum samples obtained from the catheter. Light gray bars represent 0-1,3 glucan content in the peripheral serum sample (tail vein) obtained from an animal with a biofilm catheter infection. Dark gray bars represent /3-1,3 glucan content of a serum sample from an animal with a disseminated infection. Error bars represent 1 SD.
03-1,3 Glucan Test for Biofilm Infection e JID 2007:195 (1 June) * 1709
This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PMAll use subject to JSTOR Terms and Conditions

and 98-17 formed extensive biofilms consisting of a network
of hyphae and yeast cells embedded in a heterogeneous matrix.
C. glabrata and C. parapsilosis, however, formed biofilms con-
sisting primarily of yeast cells. Like C. albicans, these biofilms also were heterogeneous and contained abundant matrix
material.
In vivo biofilm glucan assay. To determine whether biofilm formation is associated with elevated concentrations of 0-1,3
glucan in vivo, we compared the CVC (biofilm) rat model to
a traditional disseminated candidiasis (nonbiofilm) model. An-
imal catheters were inoculated with C. albicans K1, and biofilm
formation was confirmed using SEM at 24 h (figure 3A). After
catheter inoculation, serum samples were collected both directly from the catheter and the tail vein at 12 and 48 h. In a second
group of rats, infection was produced by injection of identical
inoculum via the tail vein. Blood samples were collected at the
various time points. We measured serum glucan content as well
as the viable cell burden in kidneys. As anticipated, the viable
burden in the kidneys, as an estimate of the systemic burden
of cells, was greater in the disseminated model (figure 4). De-
spite the in vivo presence of more cells, the serum from the
biofilm catheter infection contained nearly 10-fold more 0-1,3
glucan (P< .01) (figure 4). Also, tail-vein serum samples taken from animals with a biofilm infection contained high concen-
trations of 0-1,3 glucan, indicating a systemic release of glucan
during biofilm infection. Animals with catheters were also in-
fected by tail-vein route. Serum samples from these animals did not have elevation of 03-1,3 glucan, indicating that the cath- eter material does not result in the elevated serum glucan levels
without the presence of a biofilm (data not shown). Next, we extended our investigated of 3-1,3 glucan secretion
to other Candida species. We used clinical isolates of C. glabrata, C. parapsilosis, and an additional C. albicans isolate for infection of the biofilm CVC model. SEM confirmed the presence of biofilm on the luminal surface at 24 h (figure 3B-3E). Similar to our previous results, animals infected by biofilm route had 2-10-fold higher serum 0-1,3 glucan concentrations (figure 5). However, the magnitude of the difference varied by species. Biofilm infection with C. glabrata was associated with the high- est serum 0-1,3 glucan content. The disseminated model pro- duced >10-fold less glucan using this same strain. Interestingly, a serum sample taken from a site distant from the biofilm
infection contained only low levels of glucan. The C. parapsilosis and C. albicans biofilm infections produced 2-8-fold higher serum 1-1,3 glucan concentrations, compared with the re-
spective disseminated models.
DISCUSSION
Candida infections are common in hospitalized patients, par- ticularly those with implanted medical devices [4, 6, 7]. CVCs
become infected at an estimated rate of 1.2-4.5/1000 patient- catheter days [25, 26]. The diagnosis of a Candida CVC infec- tion is problematic, and the decision to remove a catheter is difficult. Replacement of a CVC is costly, associated with patient discomfort, and carries a mechanical complication rate of
6.3%-19.4% [25]. The Candida cells growing as biofilms are different from their
free-floating counterparts [11]. Sessile and embedded in a ma-
a, C
0
0T -J
5 -
4-
3-
2-
1-
0-
A
Biofilm kidney Disseminated kidney
CA-98-17 CG-5376 CP-5986
B
-J,
0a
C~ U,
400
300
200
100
0
I Biofilm catheter I Biofilm peripheral IDisseminated
CA-98-17 CG-5376 CP-5986
Figure 5. Serum 0-1,3 glucan concentrations (picograms per milliliter) from Candida albicans (CA-98-17), C. glabrata (CG-5376), and C. para- psilosis (CP-5986) biofilm and disseminated infections. Central venous catheters were surgically implanted in rats and infected with various Candida species. Serum samples were obtained at 24 h, and 3-1,3 glucan content was determined using limulus lysate assay (B). Black vertical bars represent 0-1,3 glucan content in picograms per milliliter in serum samples obtained from the catheter. Light gray bars represent 0-1,3 glucan content in the peripheral serum sample obtained from an animal with a biofilm catheter infection. Dark gray bars represent 3-1,3 glucan content of a serum sample from an animal with a disseminated infection. The viable burden of cells from the kidneys of animals with disseminated and biofilm infections were determined at various time points to estimate systemic burden of infection (A). Error bars represent 1 SD.
1710 * JID 2007:195 (1 June) * Nett et al.
This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PMAll use subject to JSTOR Terms and Conditions

trix, they exhibit a drug-resistant phenotype, making removal
of an infected catheter often necessary for cure [7, 10-12, 15]. The ability to detect a Candida biofilm could have a great
impact on the treatment on candidemia. Of patients diagnosed with candidemia, 30%-70% are reported to have a catheter-
related bloodstream infection [9, 10, 27]. However, studies in-
cluding high numbers of patients with neutropenia have dem-
onstrated lower incidence of CVC-associated candidemia and,
thus, biofilm infection (18%-47%) [6, 28]. Many devices in
these patients are surgically implanted, making removal and
replacement more difficult. Current guidelines recommend de-
vice removal for all patients with candidemia [7]. A test allow-
ing detection of a biofilm device-associated infection would
identify patients who would benefit most from device removal.
Those with candidemia and a negative biofilm test would be
able to avoid device removal.
In these investigations, we have proposed 0-1,3 glucan as a
biofilm marker for Candida. Previous studies have dem-
onstrated differences in secreted carbohydrate composition be-
tween C. albicans biofilm and planktonic cultures [29, 30]. Our
recent laboratory study has demonstrated a greater concentra-
tion of 0-1,3 glucan in the cell wall of Candida biofilm cells
[30]. We reasoned that the unidentified matrix carbohydrate could be a 0-glucan molecule. To test this hypothesis, we com-
pared the C. albicans biofilm conditions to planktonic condi-
tions and demonstrated increased 10-1,3 glucan concentrations
surrounding Candida biofilms both in vitro and in vivo. Using an in vivo model, which closely mimics a patient CVC infection, we identified significantly higher serum levels of 0-1,3 glucan,
compared with animals with disseminated infections. Our find-
ings suggest that serum 10-1,3 glucan may be a potential target to differentiate biofilm and nonbiofilm infections in patients.
The limulus lysate assay used in the present studies is ap-
proved for diagnosis of invasive fungal infection including Can-
dida [20, 31-34]. A cutoff of 60 pg/mL glucan has been used
for diagnosis of an invasive fungal infection [20, 34]. However, in one study, the serum 10-1,3 glucan concentration in patients with candidemia ranged from 60 to >2000 pg/mL [20]. Although a difference in systemic viable burden may account for variation
in serum glucan concentrations in these patients, it is also possible that patients with higher values had a biofilm catheter infection.
In the present experiments, 1-1,3 glucan served as a useful marker
for in vitro and in vivo biofilm formation. Using the glucan assay as an indicator of biofilm infection may markedly improve the
specificity of this test. Further investigation of the 1-1,3 glucan
assay in patients with Candida biofilm infections would be im-
portant to determine whether this assay, or a modified glucan
assay, may be able to diagnose a biofilm or device-associated
infection in a heterogeneous patient population.
References
1. Kojic EM, Darouiche RO. Candida infections of medical devices. Clin Microbiol Rev 2004; 17:255-67.
2. Crnich CJ, Maki DG. The role of intravascular devices in sepsis. Curr Infect Dis Rep 2001; 3:496-506.
3. National Nosocomial Infection Surveillance System. NNIS data sum- mary from Jan 1992-Jun 2001. Am J Infect Control 2001; 29:404-20.
4. Beck-Saugue C, Jarvis WR. Secular trends in the epidemiology of nos- ocomial fungal infections in the United States, 1980-1990. J Infect Dis 1993; 167:1247-51.
5. Maki DG, Tambyah PA. Engineering out the risk of infection with
urinary catheters. Emerg Infect Dis 2001; 7:1-6. 6. Nguyen MH, Peacock JE Jr, Tanner DC, et al. Therapeutic approaches
in patients with candidemia: evaluation in a multicenter, prospective, observational study. Arch Intern Med 1995; 155:2429-35.
7. Pappas PG, Rex JH, Sobel JD, et al. Guidelines for treatment of can- didiasis. Clin Infect Dis 2003; 38:161-89.
8. Wey SB, Mori M, Pfaller MA, Woolson RF, Wenzel RP. Hospital-ac- quired candidemia: the attributable mortality and excess length of stay. Arch Intern Med 1988; 148:2642-5.
9. Rex JH, Bennett JE, Sugar AM, et al. A randomized trial comparing fluconazole with amphotericin B for the treatment of candidemia in
patients without neutropenia. N Engl J Med 1994; 331:1325-30. 10. Rex JH, Bennett JE, Sugar AM, et al. Intravascular catheter exchange
and duration of candidemia. Clin Infect Dis 1995; 21:994-6. 11. Donlan RM. Biofilm formation: a clinically relevant microbiological
process. Clin Infect Dis 2001; 33:1387-92. 12. Chandra J, Kuhn DM, Mukherjee PK, Hoyer LL, McCormick T, Ghan-
noum MA. Biofilm formation by the fungal pathogen Candida albicans:
development, architecture, and drug resistance. J Bacteriol 2001; 183: 5385-94.
13. Bachmann SP, Vande Walle K, Ramage G, et al. In vitro activity of
caspofungin against Candida albicans biofilms. Antimicrob Agents Che- mother 2002; 46:3591-6.
14. Hawser SP, Douglas LJ. Biofilm formation by Candida species on the surface of catheter materials in vitro. Infect Immun 1994; 62:915-21.
15. Lewis RE, Kontoyiannis DP, Darouiche RO, Raad II, Prince RA. An-
tifungal activity of amphotericin B, fluconazole, and voriconazole in an in vitro model of Candida catheter-related bloodstream infection. Antimicrob Agents Chemother 2002; 46:3499-505.
16. Ramage G, Vande Walle K, Bachmann SP, Wickes BL, Lopez-Ribot JL. In vitro pharmacodynamic properties of three antifungal agents against preformed Candida albicans biofilms determined by time-kill studies. Antimicrob Agents Chemother 2002; 46:3634-6.
17. Maki DG, Weise CE, Sarafin HW. A semiquantitative method for iden-
tifying intravenous-catheter-related infection. N Engl J Med 1977; 296: 1305-9.
18. Brun-Buisson C, Abrouk F, Legrand P, Huet Y, Larabi S, Rapin M.
Diagnosis of central venous catheter-related sepsis: critical level of
quantitative tip cultures. Arch Intern Med 1987; 147:873-7. 19. Safdar N, Fine JP, Maki DG. Meta-analysis: methods for diagnosing
intravascular device-related bloodstream infection. Ann Intern Med 2005; 142:451-66.
20. Ostrosky-Zeichner L, Alexander BD, Kett DH, et al. Multicenter clinical evaluation of the
(1--3) 1-D-glucan assay as an aid to diagnosis of fungal infections in humans. Clin Infect Dis 2005; 41:654-9.
21. Miyazaki T, Kohno S, Koga H, et al. G test, a new direct method for diagnosis of Candida infection: comparison with assays for beta-glucan and mannan antigen in the rabbit model of systemic candidiasis. J Clin Lab Anal 1992; 6:315-8.
22. Andes D, Nett J, Oshel P, Albrecht R, Marchillo K, Pitula A. Devel- opment and characterization of an in vivo central venous catheter Candida albicans biofilm model. Infect Immun 2004; 72:6023-31.
23. O'Reilly T, Andes D, Ostergaard C, Frimodt-Moller N. Evaluation of antimicrobials in experimental animal infections. In: Lorian V, ed.
0-1,3 Glucan Test for Biofilm Infection e JID 2007:195 (1 June) e 1711
This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PMAll use subject to JSTOR Terms and Conditions

Antibiotics in laboratory medicine. Baltimore, MD: Williams & Wil- kins, 2005:654-701.
24. Andes, D. Antifungal drug evaluation-candidemia animal models. In: Ernst EJ, Rogers PD, eds. Methods in molecular medicine-antifungal agents. Totowa, NJ: Humana Press, 2005:111-28.
25. McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med 2003; 348:1123-33.
26. Centers for Disease Control and Prevention. National Nosocomial In- fections Surveillance (NNIS) system report, data summary from Jan- uary 1992 to June 2002, issued August 2002. Am J Infect Control 2002; 30:458.
27. Abi-Said D, Anaissie E, Uzun O, Raad I, Pinzcowski H, Vartivarian S. The epidemiology of hematogenous candidiasis caused by different Candida species. Clin Infect Dis 1997; 24:1122-8.
28. Abi-Said D, Anaissie E, Uzun O, Raad I, Pinzcowski H, Vartivarian S. The epidemiology of hematogenous candidiasis caused by different Candida species. Clin Infect Dis 1997; 24:1122-8.
29. Baillie GS, Douglas LJ. Matrix polymers of Candida biofilms and their
possible role in biofilm resistance to antifungal drugs. J Antimicrob Chemother 2000; 46:397-403.
30. Nett J, Lincoln L, Marchillo K, VanHandel M, Andes D. Comparison
of cell wall of biofilm and planktonic C. albicans [abstract C117]. In:
Program and abstracts of the 8th ASM Conference on Candida and Candidiasis (Denver). Washington, DC: American Society for Micro-
biology, 2006:75. 31. Obadasi Z, Paetznick VL, Rodriguez JR, Chen E, McGinnis MR, Os-
trosky-Zeichner L. Difference in beta-glucan levels in culture super- natants of a variety of fungi. Med Mycol 2006; 44:267-72.
32. Pazos C, Pont6 J, Del Palacio A. Contribution of (1-+3) f-D-glucan chromogenic assay to diagnosis and therapeutic monitoring of invasive
aspergillosis in neutropenic adult patients: a comparison and serial
screening for circulating galactomannan. J Clin Microbiol 2005; 43: 299-305.
33. Kawazu M, Kanda Y, Nannya T, et al. Prospective comparison of the
diagnostic potential of real-time PCR, double-sandwich enzyme-linked immunosorbent assay screening for invasive aspergillus in patients with
hematological disorders. J Clin Microbiol 2004; 42:2733-41. 34. Odabasi Z, Mattiuzzi G, Estey E, et al. 3-D-glucan as a diagnostic
adjunct for invasive fungal infections: validation, cutoff development, and performance in patients with acute myelogenous leukemia and
myelodysplastic syndrome. Clin Infect Dis 2004; 39:199-205.
1712 , JID 2007:195 (1 June) * Nett et al.
This content downloaded from 128.104.46.196 on Wed, 28 Jan 2015 18:04:38 PMAll use subject to JSTOR Terms and Conditions